

Abstract
Restoration is one of the most important things in the field of dentistry, in restoration, there are two main things that must be considered, that was esthetic factors and functional factors. A tooth after endodontics treatment require more complex restoration than normal tooth, because lot of factors needed to be observed first, one of which is tissue residue, root canal anatomy, and even the economics condition of the patient. Post, cores, and crowns themselves have several contra indications in their use, therefore a dentist must be able to have other alternatives in the choice of restoration. Endocrown is an alternative that can be used by a dentist in performing postendodontics restoration.
KEYWORDS: Endocrown, endodontics, esthetic, postcore crown, restoration, vertucci type canal
INTRODUCTION
Endodontics is one of the most common treatments in the field of Dentistry. Endodontics is the treatment of the pulp or root canal, where teeth that have been treated with endodontic treatment have different characteristics with teeth that are not treated endodontic, one of which is endurance or fragility of the tooth structure. Other factors that must be considered are the position of the tooth, anatomy of the tooth itself and the root canal, the remaining healthy tissue structure, the functional activities in the area of dental occlusion, the age of the tooth and the patient itself, the supporting tissue of the tooth which is the periodontal includes alveolar and gingiva, even the financial aspects of the patient. Therefore, the choice of restoration must be exactly as indicated.
The selected restoration in postendodontic treatment must pay attention to various aspects, as mentioned above. Post, core, and crown are one of the main choices of various restoration options on tooth that have been carried out by endodontics. Post, core, and crown are the main choices because of the excellent esthetic, functional factors.[1,2,3,4] The use of composite post and cores, when used appropriately and according to indications, results in long-term satisfaction. Limitations on the use of postcore, including root anatomical variations, dilaceration or short roots, small diameter root shapes, and high costs. An alternative to the use of post and crown is the use of adhesive endodontic crown or also called endocrown.[5,6,7]
Endocrown is a partial crown made from ceramic material or composite resin which is applied with resin cement to the postendodontic teeth. This restoration is full occlusal coverage and takes advantage of the pulp chamber to increase the adhesive surface area. Materials used for the manufacture of endocrown are feldsphatic and glass-ceramic, hybrid composite resins, and computer-aided design and computer-aided manufacturing (CAD/CAM) ceramics and composite resins.[6,8] Endocrown indications include loss of extensive tooth structure, small intermaxillary spaces where rehabilitation using pegs and crowns is not possible because of insufficient thickness of ceramic material, and cases where postuse is contraindicated because there are anatomic variations of the roots.[7,9]
In this case, composite endocrown was the treatment of choice based on the loss of extensive tooth structure and orthodontic treatment has been planned after.
CASE REPORT
A 29-year-old female patient had reported to the Department of Conservative Dentistry and Endodontics FKG Unpad, with chief complaint that she wants to get a restoration after treated by endodontist last week, she told that she is going to use orthodontics [Figure 1].
Figure 1.

Odontogram
Patient had no history of hypertension, diabetes mellitus, allergic reaction, and blood abnormalities.
EXTRAORAL EXAMINATION
Symmetrical face, lip, and normal temporomandibular joint
Normal lymph node.
INTRAORAL EXAMINATION
Good oral hygiene
Temporary restoration was done on the occlusal extension to the buccal pit, proximal distal, and some lingual in good condition without any leakage seen
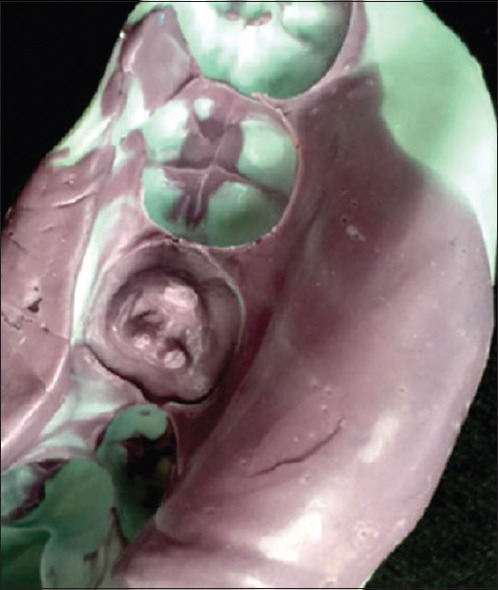
Biting test and percussion tests shown negative reaction, no sign of tooth movement, and normal periodontal [Figure 2].
Figure 2.

Clinical Appearance on tooth 36
Radiological examination results showed that there was a radiopaque appearance in enamel, dentin, up to the dental pulp chamber of tooth 36. There were three straight shape root canals, with distal roots branching into two, and visible radiopaque features resembling root canal fillers from orifice to apex. The alveolar crest is seen within normal height. The periodontal membrane is widened at the apical distal root. The lamina dura appears to disappear or seen diffuse at the apical distal root. Periapical tissue around the distal root shows diffuse radiopaque features [Figure 3].
Figure 3.

Periapical Radiograph on tooth 36
TREATMENT PLAN AND PROCEDURE
On the first visit (July 28, 2016), clinical and radiographic examination was done, and diagnosis and prognosis of tooth 36 was made. Patient was informed and inform consent was agreed about endocrown restoration according to resistance of the tooth structure, Vertucci Type V root canal form, and minimal invasive principal.
First, a wax up was made and impression by putty was done to get elastomer matrix for temporary restoration. Endocrown preparation was done by wheel diamond bur, taking the coronal part of tooth structure until the supragingival margin. Gutta-percha was taken by flat end tapered diamond bur 1 mm under orifice. Pulp chamber preparation was also made by tapered diamond bur shaping the pulp chamber divergent coronally 5°–10° of tooth axis [Figure 4]. Smart Dentin Replacement (SDR-Dentsply) was applied on the pulp chamber as a base.
Figure 4.

Before and after composite endocrown preparation
After preparation finished, impression was taken by double impression [Figure 5], meanwhile maxillary teeth were impressed by alginate and casted by dental stone. Temporary crown by Bis-Acrilyc Composite (Protemp 4 Temporization Material– 3M ESPE) was applied to elastomer matrix and placed to tooth 36, the excess materials were taken using excavator. Temporary crown can be seen in Figure 6.
Figure 5.
Double impression
Figure 6.
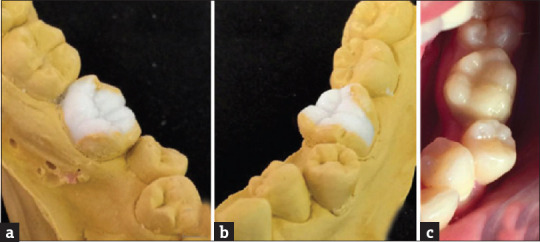
Wax up process (a) Lingual view of wax-up; (b) Buccal view of wax-up; (c) Oclusal view after insertion of temporary crown
Working model was prepared for indirect composite endocrown making [Figure 7a–h]. Application of separator was given to all surface of prepared tooth 36, and proximal surface of tooth 37 and 35 which has a proximal contact to 36, so were antagonist teeth, for several seconds. Application of (SDR-Dentsply) was made in tooth chamber until tooth preparation margin and light-cured.
Figure 7.
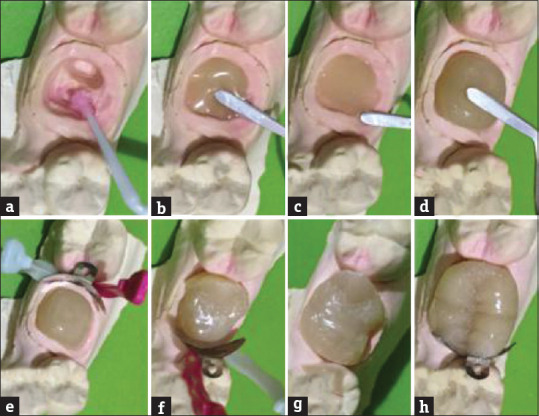
Indirect composite endocrown restoration process on tooth 36 (a) Separator application; (b-d) dentin shade application, layer by layer build the core; (e) application of sectional matrix on distal area of the tooth and application of composite enamel shade; (f) application of sectional matrix on mesial area of the tooth; (g) sculpting the buccal and the lingual wall; (h) sculpting the occlusal anatomy of the tooth
Resin composite application by layering technique was made on working model. Resin composite that was being used is Dual Shade resin composite (3M-FIltek Z350XT Universal Composite). First A3 dentin shade resin composite is applied to all tooth surface remaining ± 0, 5 mm space for enamel shade composite. The remaining ± 0, 5 mm space was measured by hand instrument missura (LM Arte) and by occlusion with antagonist teeth, and light-cured after.
Sectional matrix was used for ideal proximal contouring to tooth 35 and 37 [Figure 7e–f]. Application of A2 enamel shade was placed on proximal, buccal, and lingual surface by application of hand instrument (LM Arte) [Figure 7e–g]. Application of A2 enamel shade composite also placed on occlusal, pit and fissure, and then contoured by fissure hand instrument (LM Arte) [Figure 7h]. Each steps of composite placement, continued by light curing process. Stain color (Coltene) was also used on pit and fissure by composite brush, after that a thin layer of A2 enamel shade composite was placed on top and contoured. Oxygen barrier is applied on all surfaces of endocrown and light-cured [Figure 8].
Figure 8.
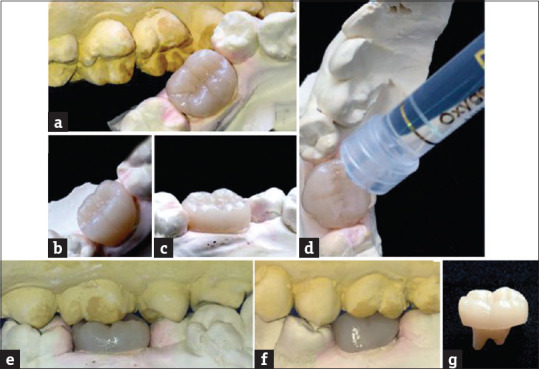
Result of composite endocrown restoration (a) occlusal view; (b) buccal view; (c) lingual view; (d) glycerine application (deox, Ultradent) as a oxygen-barrier gel; (e) relationship of crown height in occlusion with antagonist tooth (lingual view); (f) relationship of crown height in occlusion with antagonist toot (buccal view); (g) endocrown final restoration
Clinical examination on the second visit (7 days later) showed asymptomatic, insensitivity to percussion, no tooth mobility nor periodontal abnormalities, and temporary restoration was in a good condition.
Temporary restoration was removed using crown remover, and after that try in endocrown on tooth 36 was done. Restoration margin and tooth shoulder preparation was checked. Occlusion was also checked by articulating paper on centric occlusion position. Occlusal adjustment was done by flame fine finishing diamond bur, and polished by rubber polishing enhance (Dentsply), SofLex polishing disc (3M– ESPE), interdental strip (3M– ESPE), astro brush (Ivoclaire) and diamond polishing paste 0.5 μm (Ultradent).
Endocrown surface was etched on intaglio surface, rinsed, and silane was applied for several seconds, bonding, air-dried was used so that the bonding is only a thin layer, and then light-cured [Figure 9].
Figure 9.
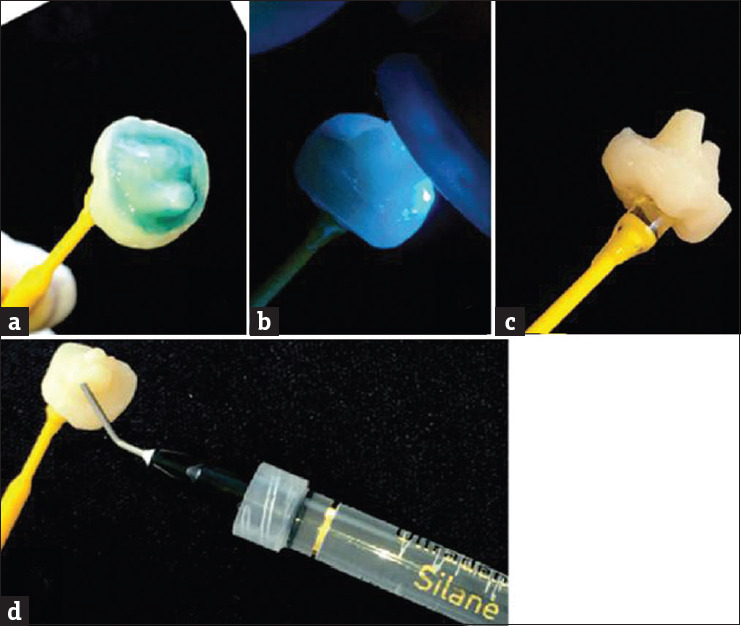
Adhesive step on endocrown (a) Acid-etching the intaglio surface of endocrown then washed off with water syringe and dried off; (b) Application of silane; (c) Application of bonding agent; (d) Light-curing of bonding agent
Adhesive step is also done on tooth surface, selective etch and bonding by the 5th generation bonding was done on all prepared tooth 36 surface [Figure 10]. Etched was done by 37% phosphoric acid for 15 s [Figure 10a], rinsed and dried with three-way syringe until moist [Figure 10b]. Bonding was applied on tooth surface after etching was done by a microbrush [Figure 10c], after waiting for several seconds, bonding was thinned by air-dried, and teflon tape was placed on tooth 35 and 37 [Figure 10d], and then light cured.
Figure 10.
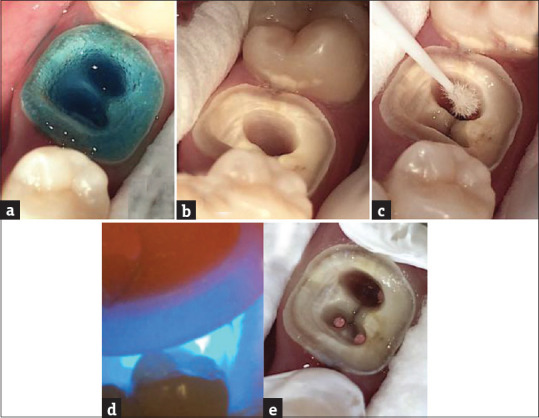
Adhesive step on tooth 36 (a) acid-etching the tooth; (b) acid-etch is washed off with water syringe and dried off to the moist state; (c) application of bonding agent; (d) light-curing the bonding agent; (e) application of seal tape to the proximal area of adjacent teeth
Resin cement (Relyx– 3M ESPE) applied to surface of prepared tooth 36 and to intaglio surface of restoration. Restoration was applied to tooth 36, light-cured for 1 s, excess resin on buccal and lingual surface was removed by sickle scaler interdental, meanwhile excess on interdental surface was removed by dental floss. 20 s light-curing was done on all surface of endocrown restoration.
Oxygen barrier (OxyGel– Ultradent) was applied on cementing surface so that the polymerization is not inhibited by oxygen inhibited layer. After that, light cure was done. Cementation result showed in Figure 11.
Figure 11.

Clinical examination after composite endocrown cementation (a) Oclusal view; (b) Buccal view
Patient was instructed to avoid hard textured food on region 36 for 24 h, and to maintain good oral hygiene. Patient was informed about long term evaluation, 1 week after endocrown insertion and after orthodontic treatment is finished.
Follow-up, 7 days after insertion showed that tooth 36 was asymptomatic, insensitive to percussion, and neither tooth mobility nor periodontal abnormalities. Restoration was under good condition and neither transformation nor discoloration of restoration observed [Figure 12].
Figure 12.
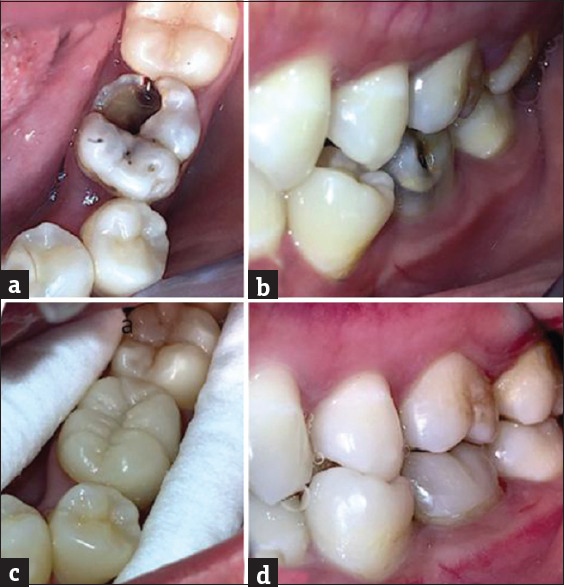
Clinical assessment (a) preoperative occlusal view; (b) preoperative buccal view; (c) occlusal view of 1 week followup after composite endocrown insertion on tooth 36; (d) buccal view of1week followup after composite endocrown insertion on tooth 36
Radiographic examination showed radiopaque crown on enamel, dentin, through pulp chamber on tooth 36. Three root canals showed straight form, with distal root has 2 branch, obturation was showed as radiopaque on orifice to apex. Alveolar crest showed normal condition. Periodontal membrane and lamina dura was also in normal condition. Periapical tissue surrounding distal root showed slight radiopaque appearance [Figure 13]. Polishing was done on this visit.
Figure 13.
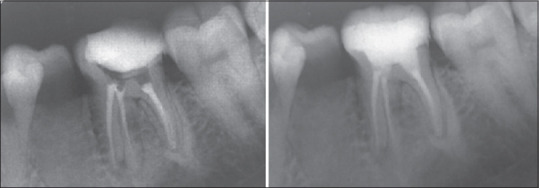
Radiographic examination before and after composite endocrown on tooth 36
DISCUSSION
Restorative design of teeth that have been treated with endodontics is a challenge for dentists and is still a contentious issue. Conventional crowns with metal pegs still widely used in the dentistry, but the principle of their invasive use has been widely criticized. New materials for restoration options using adhesive materials have been introduced at this time which can provide more conservative dental results also faster, and cost-effective treatment.[1,2,3,4]
The choice of postendodontic dental restoration is based on several factors. These factors include the healthy tissue structure of the remaining teeth, the teeth location in the mouth, and the esthetics that are important as a selection guide of adequate restorations. Other consideration factors include the function activity in the tooth occlusal area, tooth age, endodontic/periodontal prognosis, and patient financial aspects.
Assessment of teeth adhesion properties after endodontic treatment of remaining healthy coronal tissue of teeth is done at the preliminary stage when cavity removed and the pulp tissue is removed. This assessment includes the remaining wall tissue structure that must be healthy, no fissure, and a minimum thickness of 1 mm. Thin physical and cavity walls must be detected before reconstructing the preendodontic build-up with composite resin, because part of the resin will be used as the basis for definitive restoration.
The physiological and anatomical differences between anterior and posterior teeth are important when selecting restorations.[5] Relationship of molar, canine lateral guidance, incisors anterior guidance to Class I occlusion shows molar teeth receiving axial loads, anterior teeth (incisors and canines) receive shear load, while premolar teeth receive a more complex burden of axial and shear loads, and hence premolars have the potential for fracture compared to other teeth.[5,6,7] This indicates the use of postbased on the location of the teeth in the mouth and the load received by the tooth.
Classic treatments such as posts, cores, and crowns must remain a primary consideration for severely damaged premolars, until further clinical trials prove the possibility of restoring teeth adhesively with endocrown.[10] Several in vitro studies have proven the validity of molar endocrown and premolar, only a few in vivo studies have been conducted, and reported good clinical performance on molar.[9,11,12,13]
The use of post and composite cores, if used appropriately and according to indications, results in long-term satisfaction. Limitations on the use of post, including root anatomical variations, dilated or short roots, small diameter root shapes, and high costs. An alternative to the use of post and core is the use of adhesive endodontic crown or also called endocrown.[2,3]
Endocrown is a partial crown made from ceramic material or composite resin which is cemented with resin cement to the postendodontic teeth. This restoration is full occlusal coverage and takes advantage of the pulp chamber to increase the adhesive surface area. Materials used for making endocrown are feldsphatic and glass-ceramic, composite hybrid resin, and CAD/CAM ceramic and composite resin.[6,8]
Endocrown indications include extensive loss of tooth structure, small intermaxillary spaces where rehabilitation using pegs and crowns is not possible because of insufficient thickness of ceramic material, and cases where postuse is contraindicated because there are anatomic variations of the roots.[7,9]
In this study, the right maxillary first premolar had V-type root canal morphology according to the Vertucci classification [Figure 14].[8]
Figure 14.
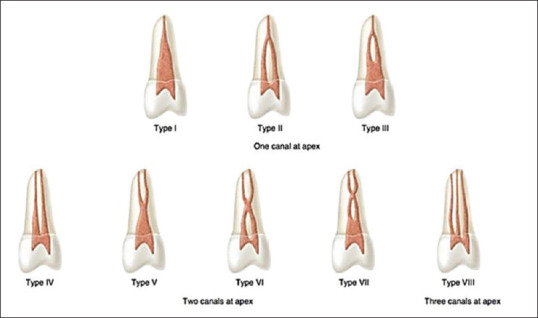
Vertucci classification7
Endocrown has the advantage that its procedures are easy and have better mechanical performance than conventional crowns, lower costs due to fewer procedure stages, less time, and good esthetics.[9,12,14]
The endocrown preparation principle follows the same pattern as the preparation principle for indirect inlay and onlay restorations. This restoration uses all depth, extension, and inclination of the pulp chamber wall to improve the stability and retention of the restoration, without removing filler material from inside root canal.[11]
The study states that composite resin overlays, related to their low modulus of elasticity, show better clinical performance than ceramics, including receiving and minimizing internal loads. The difference in modulus of elasticity between ceramics and dentine causes the risk of root fracture in teeth.[10,15]
The author chooses indirect nanocluster composite resin, taking into account the stress-absorbing properties and practical advantages including the possibility of modification and easily surface correction.[1]
Cavity preparation at the first visit and adhesive application when cementing has the same procedure for endocrown ceramic and composite resin restorations. The difference is only intaglio surface adhesive action of both materials when cemented. Occlusal portion cutback at least 2–3 mm with a butt-margin is recommended for ceramics and composite resin restorations. Buccal margins are placed on the ⅓ supragingival cervix or 0.5–1 mm subgingival for esthetic purposes.[16,17]
The use of dual shade composite nanocluster, Filtek Z350XT (3M– Espe) for endocrown restorations was chosen based on functional and esthetic considerations, and long-term temporary restoration because patients would use orthodontic braces afterward.
Filtek Z350XT (3M– Espe) contains nanocluster filler, which is a combination of 20 nm silica filler, 4–11 nm zirconia filler, and zirconia/silica filler cluster. The literature states that this system shows good results based on compressive and diametric tensile strength, flexural strength and modulus, fracture toughness, wear resistance, low volumetric shrinkage, and good esthetics.[18]
The superiority of the Z350XT compared to other composites are easily polished, colors that blend with the surrounding teeth, good handling, and good clinical performance [Table 1]. This system has four complete color opacity, including dentin, body, enamel, and translucent. The Filtek Z350XT Restoration is indicated for use as an anterior and posterior direct restoration, core build-up, splinting, and indirect restorations (inlay, onlay, and veneer).[18]
Table 1.
Comparison of physical and mechanical properties of Z350XT composite resin with other composite resin
| Level | Filtek™ Z350 XT Universal Restorative (DEB shades) | Filtek™ Z350 XT Universal Restorative (T shades) | Filtek™ Supreme XT Universal Restorative (DEB shades) | CeramX™ Mono | Durafill® VS | Estelite® Sigma Quick | EsthetX® HD | Gradia® Direct | Grandio® | Herculite ® XRV Ultra™ | Premise™ | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Compressive Strength | Mpa | 370.56 | 394.01 | 361.37 | 346.8 | 349.86 | 364.19 | 376.83 | 323.4 | 341.84 | 349.1 | 370.81 |
| StDev | 15.13 | 25.05 | 23.78 | 22.96 | 10.4 | 14.03 | 35.41 | 7.92 | 16.04 | 23.51 | 18.83 | |
| Diametral Tensile Strength | Mpa | 86.12 | 90.64 | 85.53 | 63.31 | 55.89 | 77.56 | 73.64 | 52.82 | 81.28 | 80.65 | 65.89 |
| StDev | 3.91 | 1.4 | 5.47 | 6.49 | 2.87 | 2.98 | 2.38 | 5.89 | 5.63 | 5.76 | 8.18 | |
| Flexural Strength | Mpa | 165.14 | 157.98 | 165.9 | 113.68 | 64.5 | 111.08 | 132.9 | 106.07 | 144.03 | 106.48 | 108.64 |
| StDev | 13.59 | 8.16 | 5.4 | 11.52 | 3.62 | 3.94 | 8.65 | 6.77 | 17.54 | 14.34 | 9.64 | |
| Flexural Modulus | Mpa | 11348.00 | 9180.00 | 11436.00 | 8830.00 | 2613.00 | 7552.00 | 10128.00 | 6299.00 | 19437.00 | 7679.00 | 7839.00 |
| StDev | 271.00 | 431.00 | 442.00 | 379.00 | 66.00 | 202.00 | 146.00 | 185.00 | 299.00 | 541.00 | 183.00 | |
| Fracture Toughness | K1c | 1.84 | 1.51 | 1.92 | 1.69 | 1.01 | - | 1.70 | 1.05 | 1.68 | - | 1.81 |
| StDev | 0.19 | 0.02 | 0.21 | 0.05 | 0.09 | - | 0.12 | 0.06 | 0.07 | - | 0.03 | |
| Shrinkage | % | 1.97 | 2.48 | 2.06 | 1.97 | 2.00 | 1.80 | 2.58 | 1.92 | 1.69 | 2.70 | 1.66 |
| StDev | 0.03 | 0.06 | 0.06 | 0.05 | 0.08 | 0.05 | 0.05 | 0.04 | 0.04 | 0.07 | 0.06 | |
| Polish Retention | ||||||||||||
| Initial | Mean | 94.83 | 93.83 | 92.81 | 72.9 | 86.33 | 93.93 | 92.45 | 76.17 | 67.27 | 89.67 | 91.6 |
| StDev | 1.03 | 1.39 | 2.35 | - | 0.15 | 0.68 | 2.33 | 0.32 | 1.71 | 2.17 | 0.96 | |
| 500 cycles | Mean | 86.82 | 88.04 | 83.09 | 36.03 | 74.82 | 67.62 | 54.75 | 37.98 | 43.47 | 69.63 | 70.36 |
| StDev | 5.77 | 6.01 | 6.08 | 7.27 | 4.85 | 7.45 | 3.86 | 10.27 | 4.82 | 9.21 | 5.97 | |
| 1000 cycles | Mean | 83.32 | 85.72 | 78.73 | 25.5 | 68.08 | 64.14 | 27.65 | 21.58 | 35.31 | 60.83 | 63.11 |
| StDev | 5.96 | 5.6 | 7.69 | 6.39 | 5.67 | 3.75 | 1.03 | 12.86 | 6.34 | 7.29 | 5.81 | |
| 2000 cycles | Mean | 76.55 | 82.83 | 69.74 | 23.18 | 59.03 | 63.55 | 25.05 | 13.53 | 20.79 | 54.89 | 49.35 |
| StDev | 6.43 | 5.12 | 8.57 | 2.74 | 6.15 | 3.88 | 2.64 | 5 | 3.29 | 6.85 | 8.48 | |
| 3000 cycles | Mean | 73.19 | 82.01 | 62.89 | 10.45 | 58.7 | 64.29 | 29.28 | 13 | 17.26 | 52.57 | 44.12 |
| StDev | 5.99 | 5.96 | 8.69 | 1.37 | 3.38 | 9.89 | 2.59 | 0.81 | 2.81 | 11.34 | 4.93 | |
| 4000 cycles | Mean | 70.33 | 81.23 | 56.63 | 9.8 | 55.67 | 62.35 | 26.78 | 10.47 | 13.13 | 53.71 | 39.29 |
| StDev | 5.52 | 4.15 | 7.28 | 1.23 | 6.57 | 3.66 | 6.12 | 0.89 | 1.33 | 5.48 | 6.97 | |
| 5000 cycles | Mean | 69.66 | 79.8 | 53.48 | 9.55 | 54.02 | 63.6 | 28.68 | 11.77 | 12.16 | 52.84 | 39.26 |
| StDev | 5.36 | 6.05 | 8.19 | 1 | 3.57 | 9.53 | 0.65 | 1.16 | 0.96 | 11.58 | 3.12 | |
| 6000 cycles | Mean | 68.62 | 79.72 | 54.73 | 7.98 | 53.21 | 65.01 | 27.65 | 10.55 | 11.48 | 54.88 | 37.18 |
| StDev | 4.77 | 4.42 | 7.75 | 0.71 | 6.32 | 3.33 | 1.01 | 1.22 | 0.98 | 4.57 | 5 | |
| 3-Body Wear Rate | um lost | 5.61 | 6.54 | 5.07 | 32.04 | 15.22 | 7.5 | 7.38 | 15.17 | 8.49 | 15.78 | 16.27 |
| StDev | 0.63 | 0.5 | 0.8 | 0.68 | 0.55 | 0.46 | 0.31 | 1.43 | 0.64 | 2.13 | 0.55 |
The endocrown restoration clinical success depends largely on the exact measurement of the material use at the restorative stage. Selection of temporary crown material with Protemp 4 (3M-ESPE) is an adequate technique for gum health preservation and preventing teeth movement during endocrown restorations procedure.[6] Protemp 4 (3M-ESPE) was chosen because its advantages than other material, such as fracture resistance for short-term or long-term use, good mechanical strength, decent appearance without polishing, easy to use, and available in six colors.[19]
Temporary crown making techniques were carried out using modified direct technique with elastomeric matrix which chosen because its easy manipulation, good anatomical and morphological shape, well convection for periodontium tissue protection, and great finishing and polishing results. This technique is recommended for one or more teeth because it provides a clinical advantage of the material and working time and can be relined several times.
Dual cure resin cement (RelyX U200 Self Adhesive Resin Cement-3M ESPE) was used in this case by considering the need for light-cured light to penetrate the thickness of the composite endocrown. Relyx U200 is permanent self-adhesive resin cement with dual cure, radiopaque and broad-spectrum polymerization for indirect restoration applications. Its clinical material performance compared to other ingredients shows high adhesion strength, low postoperative sensitivity, good mechanical properties, decent color stability, and long-term stability.[20]
The combination of two polymerization mechanisms, light and chemical, guarantees polymerization under no light conditions [Table 2]. This material has adequate mechanical and suffice adhesion properties, and is easily applied with double-bodied syringes with provided mixing tips, which prevent air bubbles formation.[20]
Table 2.
Composition of RelyX self-adhesive cement
| Base paste | Catalyst paste |
|---|---|
| Methacrylate monomers containing phosphoric acid group | Methacrylate monomers |
| Methacrylate monomers | Alkaline (basic) fillers |
| Silanated fillers | Silanated fillers |
| Initiator components | Initiator components |
| Stabilizers | Stabilizer |
| Rheological additives | Pigment |
| Rheological additives |
Prepolymerization of the cement may result in easy removal of excess material from the edges of the restoration and teeth. Mechanical reduction of excess cement can cause trauma to the marginal gingival tissue and cause gingival recession.
CONCLUSION
Restoration after endodontic treatment in 36 using endocrown composite in this case gave good results and could be considered as an option in restoring posterior teeth after endodontic treatment with consideration of long-term temporary restoration.
DECLARATION OF PATIENT CONSENT
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
SUGGESTION
Long-term evaluation of composite endocrown restorations is needed as long-term temporary restoration
FINANCIAL SUPPORT AND SPONSORSHIP
Nil.
CONFLICTS OF INTEREST
There are no conflicts of interest.
REFERENCES
- 1.Rocca GT, Bonnafous F, Rizcalla N, Krejci I. A technique to improve the esthetic aspects of CAD/CAM composite resin restorations. J Prosthet Dent. 2010;104:273–5. doi: 10.1016/S0022-3913(10)60138-2. [DOI] [PubMed] [Google Scholar]
- 2.Magne P, Knezevic A. Thickness of CAD-CAM composite resin overlays influences fatigue resistance of endodontically treated premolars. Dent Mater. 2009;25:1264–8. doi: 10.1016/j.dental.2009.05.007. [DOI] [PubMed] [Google Scholar]
- 3.Lin CL, Chang YH, Pa CA. Estimation of the risk of failure for an endodontically treated maxillary premolar with MODP preparation and CAD/CAM ceramic restorations. J Endod. 2009;35:1391–5. doi: 10.1016/j.joen.2009.06.020. [DOI] [PubMed] [Google Scholar]
- 4.Bindl A, Richter B, Mörmann WH. Survival of ceramic computer-aided design/manufacturing crowns bonded to preparations with reduced macroretention geometry. Int J Prosthodont. 2005;18:219–24. [PubMed] [Google Scholar]
- 5.Bindl A, Mörmann WH. Clinical evaluation of adhesively placed cerec endo-crowns after 2 years – preliminary results. J Adhes Dent. 1999;1:255–65. [PubMed] [Google Scholar]
- 6.Göhring TN, Peters OA. Restoration of endodontically treated teeth without posts. Am J Dent. 2003;16:313–7. [PubMed] [Google Scholar]
- 7.Hargreaves M, Berman L. Cohen's Pathways of the Pulp. 11th ed. St. Louis, Missouri: Mosby Elsevier; 2016. [Google Scholar]
- 8.Dietschi D, Duc O, Krejci I, Sadan A. Biomechanical considerations for the restoration of endodontically treated teeth: A systematic review of the literature - part 1. Composition and micro- and macrostructure alterations. Quintessence Int. 2007;38:733–43. [PubMed] [Google Scholar]
- 9.Biacchi GR, Basting RT. Comparison of fracture strength of endocrowns and glass fiber post-retained conventional crowns. Oper Dent. 2012;37:130–6. doi: 10.2341/11-105-L. [DOI] [PubMed] [Google Scholar]
- 10.Filser F, Kocher P, Weibel F, Lüthy H, Schärer P, Gauckler LJ, et al. Reliability and strength of all-ceramic dental restorations fabricated by direct ceramic machining (DCM) Int J Comput Dent. 2001;4:89–106. [PubMed] [Google Scholar]
- 11.Rocca GT, Krejci I. Crown and post-free adhesive restorations for endodontically treated posterior teeth: From direct composite to endocrowns. Eur J Esthet Dent. 2013;8:156–79. [PubMed] [Google Scholar]
- 12.Veselinović V, Todorović A, Lisjak D, Lazić V. Restoring endodontically treated teeth with all-ceramic endo-crowns: Case report. Stomatol Glas Srb. 2008;55:54–64. [Google Scholar]
- 13.Kohli A. Textbook of endodontics. J Conserv Dent. 2010;13:2. [Google Scholar]
- 14.Dietschi D, Duc O, Krejci I, Sadan A. Biomechanical considerations for the restoration of endodontically treated teeth: A systematic review of the literature, part II (Evaluation of fatigue behavior, interfaces, and in vivo studies) Quintessence Int. 2008;39:117–29. [PubMed] [Google Scholar]
- 15.Heymann HO, Swift EJ, Jr, Ritter AV. Missouri: Elsevier Health Sciences; 2014. Sturdevant's Art and Science of Operative Dentistry. [Google Scholar]
- 16.Asmussen E, Peutzfeldt A, Sahafi A. Finite element analysis of stresses in endodontically treated, dowel-restored teeth. J Prosthet Dent. 2005;94:321–9. doi: 10.1016/j.prosdent.2005.07.003. [DOI] [PubMed] [Google Scholar]
- 17.Zarow M, Devoto W, Saracinelli M. Reconstruction of endodontically treated posterior teeth – With or without post? Guidelines for the dental practitioner. Eur J Esthet Dent. 2009;4:312–27. [PubMed] [Google Scholar]
- 18.ESPE 3M. Filtek Z350XT. Technical Product Profile FILTEK. 2014. [Downloaded on 2018 Nov 26]. Available from: http://www.multimedia. 3m.com/mws/media/631547O/filtek-z350-xt-technical-product-profile.pdf .
- 19.ESPE 3M. Ideal Temporisation Solution. 2014. [Downloaded on 2018 Nov 26]. Available from: https://multimedia. 3m.com/mws/media/1010658O/protemp-4.pdf .
- 20.Posts F, Pack A. The Strong Bond you Can Rely on elyx U200 – Strength we Put Trust. 2012 [Google Scholar]