

Abstract
Background:
Preconception care is an interventions aim to identify and modify biomedical, behavioral and social risks to pregnancy through prevention and management, emphasizing factors that must be acted upon before conception or in early pregnancy to have maximal impact.
Objective:
The aim of the study is to assess awareness and perception of preconception care among women.
Method:
A cross-sectional study conducted at UDUTH Sokoto, Nigeria, from 5 February to 1 March, 2018. A total of 131 women were recruited by simple random sampling technique via the ante-natal care clinic, using semi-structured interviewer questionnaires. Data were analyzed using SPSS version 24 and the results were presented in tables and charts. A P value of <0.05 was considered statistically significant.
Results:
There ages ranged between 16 years to 46 years and 32.8% (43/131) were within 26-30 years with a mean of 28.10 ± 6.064. Only 20.61% of them were aware of preconception care. There was significant association between awareness and the patient's tribe as well as employment status at P value 0.004 and 0.017 respectively. Among those who were unaware, 88.46% will accept if offered while, about 45.75% of those who declined believed it was not necessary.
Conclusion:
There was poor awareness but good perception and acceptability of preconception care. Therefore, there is a need to create awareness and incorporate it into routine maternal healthcare services to achieve better feto-maternal outcome.
Keywords: Antenatal care clinic, awareness, perception, preconception care, women
Introduction
Preconception care is related to women perception and acceptability of preconception outcomes.[1] It includes reducing risk in preparation for pregnancy, managing pre-existing medical conditions and preventive interventions.[1] It is, therefore, defined as a set of interventions that aim to identify and modify biomedical, behavioral and social risks to a woman's health or pregnancy outcome through prevention and management. It emphasizes on those factors which must be acted upon before conception or in early pregnancy to have maximal impact.[2]
In 2005, Centre for Disease Control set out recommendations for improving women's health preconceptionally. Actions to address awareness include to conduct consumer focused research necessary to develop messages and terminology to promote prry to develohealth care (PCHC) and awareness, design and conduct social marketing campaign necessary to develop messages for promotion of PCHC knowledge, attitude and behavior among men and women of child bearing age.[2,3,4]
Evidence had shown that, unintended and unwanted pregnancies have been associated with increased risk of adverse pregnancy outcomes, and almost half of all pregnancies in the developed world are unintended and about 52% of these women have at-least one risk factor that could have negative impact on pregnancy outcome. These factors include obesity, diabetes mellitus, smoking and alcohol consumption.[5,6] Moreover, interventions provided during the inter-conception period may reduce risks during subsequent pregnancies.[7,8]
While primary healthcare providers have the opportunity to assist women in preventing unwanted pregnancies and improve their health prior to conception.[9] In Nigeria, the service is almost non-existing. A significant number of the population concerned is unaware of such services and their benefits.[10] Studies in this environment had shown that only about 43.1%[10] of women were aware of preconception care in the Southern part of the country, with just 6% in the North.[11] This difference is as a result of the differences in the literacy level, and therefore, health seeking behavior among the groups.
Despite facts on the untoward effects on unplanned pregnancies and positive impact on preconception care, only about 32% of women were reported to have utilized it.[12]
Materials and Method
It was a cross-sectional study carried out between 5 February and 1 March in 2018 at the Obstetrics and Gynecological department of the Usmanu Danfodiyo University Teaching Hospital (UDUTH) Sokoto. A total of 131 women were recruited after informed consent was obtained. Recruitment was by simple random sampling technique of balloting using a semi-structured interviewer administered questionnaire. Information on socio-demographic characteristics, obstetric, medical, surgical and social history was obtained. In addition, awareness of preconception care was assessed using a modified Likert's chart, where six parameters related to preconception care were used. The questions included; (1) Preconception care is a care given to couples before pregnancy, (2) It prevent unintended pregnancies, (3) It prevent birth defects, (4) It prevent complications of pregnancy, labour and delivery, (5) It prevent neonatal infection, (6) It prevents maternal and child mortalities. Where a participant answered “yes” to 1 to 2 questions, then she was scored poor. if “yes” to 3 to 4 then scored good; and “yes” to 5 to 6 implied excellent levels of awareness. The questionnaire was pretested prior to commencement of the study and the data obtained were analyzed using the Statistical Software Package for Social Sciences version 24. The interpretation of the result was by both descriptive and inferential statistical methods, where P value <0.05 was considered statistically significant.
Ethical clearance was obtained from the institution's Ethics and Research and Committee.
Result
The women's ages ranged between 16-46 years with modal age of 26-30 years and a mean of 28.10 ±6.064. Majority of the respondents, 81.7% (107/131) were of Hausa/Fulani ethnic group. Among them, 55.7% (73/131) had tertiary level of education and 52.7% (69/131) were unemployed. More than half (52.7%: 69/131) were multiparous women as shown in Table 1.
Table 1.
Socio-demographic characteristics of respondents
| Characteristics | Frequency | Percentage |
|---|---|---|
| Age | ||
| 16-20 years | 11 | 8.4 |
| 21-25 years | 39 | 29.8 |
| 26-30 years | 43 | 32.8 |
| 31-35 years | 23 | 17.6 |
| 36-40 years | 11 | 8.4 |
| 41-45 years | 3 | 2.3 |
| 46 and above | 1 | 0.7 |
| Total | 131 | 100 |
| Ethnicity | ||
| Hausa | 107 | 81.7 |
| Igbo | 5 | 3.8 |
| Yoruba | 4 | 3.1 |
| Others | 15 | 11.5 |
| Total | 131 | 100 |
| Occupation | ||
| Unemployed | 69 | 52.7 |
| Business | 19 | 14.5 |
| Civil servant | 43 | 32.8 |
| Total | 131 | 100 |
| Educational status | ||
| Primary | 11 | 8.4 |
| Secondary | 36 | 27.5 |
| Tertiary | 73 | 55.7 |
| Qur’an | 11 | 8.4 |
| Total | 131 | 100 |
| Parity | ||
| Para 1-2 | 33 | 25.2 |
| Para 3-4 | 69 | 52.7 |
| Para 5 above | 29 | 22.1 |
| Total | 131 | 100 |
Only 20.61%(27/131) of the respondents ever heard of preconception care, while 79.38% (104/131) never heard of it. The main source of information was healthcare providers in 70.4% (19/27) of them, whereas 18.5% (5/27) was through the media and 11.1% (3/27) was by community members as depicted in Figure 1.
Figure 1.

Awareness of preconception care by the respondents
There was significant association between awareness and the patient's tribe (Igbos: 3.82% [5/131]) and employment status (civil servants: 32.82% [43/131]) at P values 0.004 and 0.017, respectively, as summarized in Table 2.
Table 2.
Factors associated with awareness of preconception care
| Characteristics | Aware of preconception caren (%) | Not aware of preconception caren (%) | χ2 | P |
|---|---|---|---|---|
| Age | ||||
| 15-30 years | 18 (19.4) | 75 (80.6) | 0.309 | 0.578 |
| ≥31 years | 9 (23.7) | 29 (76.3) | ||
| Ethnicity | ||||
| Hausa | 17 (15.9) | 90 (84.1) | 9.79 | 0.004* |
| Igbo | 3 (60.0) | 2 (40.0) | ||
| Yoruba | 2 (50.0) | 2 (50.0) | ||
| Others | 5 (33.3) | 10 (66.7) | ||
| Occupation | ||||
| Unemployed | 11 (15.9) | 58 (84.1) | 9.008 | 0.017* |
| Business | 1 (5.30) | 18 (94.7) | ||
| Civil servant | 15 (34.9) | 28 (65.1) | ||
| Educational status | ||||
| Informal | 2 (9.1) | 20 (90.9) | 2.14 | 0.164 |
| Formal | 36 | 27.5 | ||
| Parity | ||||
| Para 1-2 | 8 (24.2) | 25 (75.8) | 4.28 | 0.117 |
| Para 3-4 | 17 (24.6) | 52 (75.4) | ||
| Para 5 above | 2 (6.9) | 27 (93.1) |
Among the respondents, 11.50% (15/131) utilized preconception care services prior to their previous or index pregnancies due to various indications, among whom only 7/23 (30.43%) knew the exact indications. Of them, who were not aware of preconception care, 88.46% (92/104) will accept if offered because they believed it is beneficial for their health, while 11.54% (12/104) will not [Figure 2].
Figure 2.
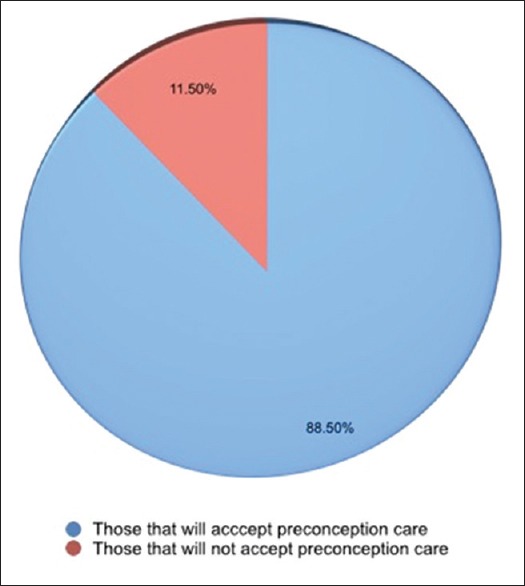
Acceptance of preconception care
Among 75% (9/12) of them, who declined believed it was not necessary, 8.33% (1/12) thought she had no risk factor and 16.67% (2/12) spouses do not accept (as presented in Figure 3).
Figure 3.
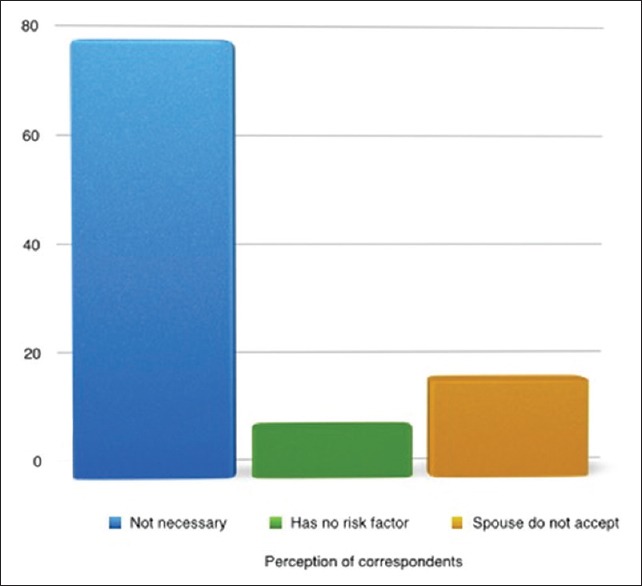
Perception of preconception care
Majority of the respondents, 72.5% (95/131) prefer to conceive after 2 years from their last child birth, while 17.6% (23/131) would want to conceive within 2 years and 5.34% (7/131) were not planning to get pregnant at all. Among them, 85.71% (6/7) had completed their family size, while 14.29% (1/7) had difficulty during index pregnancy.
Discussion
This study assessed the awareness and perception of preconception care among women. The level of awareness was 20.6% among the study participants. This is lower then what was reported from Ethiopia (27.5%) and Saudi (37.9%).[12,13] It is also lower than (76%) among Mexican-American populace and a study conducted in Enugu, South-Eastern Nigeria revealed 43.1% awareness, and 63.5% in Ife, South west[10,14,15] among study participants. The high level of awareness in the studies above could probably be due to level of education and background medical knowledge among their respondents However, our finding is higher than what was reported from Nepal (15.6%),[16] Iran (11%),[17] Sudan (11%)[18] and 6% in Zaria, North-Western Nigeria.[11] Among them, who are aware of preconception care, majority got their information from healthcare providers, which is similar to what was reported by most studies. Moreover, it is contrary to media reported from Nepal.[16] Among the study participants who were aware of preconception, 70.4% had very good understanding of preconception care based on ability to recognise the benefits derived from such services. This is higher than what was reported from Nepal (15.4%), Sudan (47%) and Ethiopia (27.7%).[12] Nepal (15.4%), Sudan (47%) and Ethiopia (27.7%).[12] In this study, the preconception care awareness is associated with employment status, as civil servants have higher tendency as well as being of Igbo ethnicity. These could be explained by the socio-cultural background and the positive health seeking behavior in the group compared to the dominant community who are usually conserved. This is contrary to educational status and age reported from Ethiopia[12] and Saudi.[13] It is also associated with education and parity in a study from Nigeria,[10] while that of Nepal[16] found no association with demographics. Of them, who were not aware of preconception care, 88% will accept if offered because they believed it is beneficial to their health. About two-third (75%) of them, who declined the offer, felt preconception care is not necessary, and this is mainly as a result of lack of awareness that such services exist.
Majority of the respondents, 72.5% prefer to conceive after 2 years from their last child birth and believed that pregnancy planning improves feto-maternal outcome. Similar findings of positive perception of benefits of preconception care and high acceptability was also reported by other researchers.
Conclusion
There is poor awareness but good perception and high acceptability of preconception care in our environment. There is prompt need to create awareness to improve perception of preconception care among the populace. The services should be readily available and incorporate it into routine maternal healthcare services to achieve better feto-maternal outcome. These can be achieved by offering it at every opportunity when women access healthcare units including other disciplines until it becomes fully incorporated into the maternal and child healthcare services.
Author contributions
Dr Amina Gambo Umar: Contributed in design, analysis, interpretation, drafting of research manuscript and final approval of the revised manuscript for publication.
Sadiya Nasir: Contributed in design of the research manuscript and final approval of the revised manuscript for publication.
Dr Karima Tunau: Contributed in design and drafting of the manuscript and final approval of the revised manuscript for publication.
Dr Swati Singh: Contributed in design, analysis, interpretation, drafting of a research manuscript and final approval of the revised manuscript for publication.
Dr Umar Ibrahim Augie: Contributed in analysis, interpretation, drafting of a research manuscript and final approval of the revised manuscript for publication.
Dr Miaro Hassan: Contributed in design, drafting of a research manuscript and final approval of the revised manuscript for publication.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgements
We acknowledge the Hospital management that offered ethical approval and the women participated in the research.
References
- 1.Fugin L. Reproductive health policy in China. Int J Womency f inte Reprod Sci. 2015;1:13–20. [Google Scholar]
- 2.Johnson K, Posner SF, Biermann J, Cordero JF, Atrash HK, Parker CS, et al. Recommendations to improve preconception health and health care-United States: A report of the CDC/ATSDR preconception care work group and the selected panel on preconception care. MMWR Recomm Rep. 2006;55:1–23. [PubMed] [Google Scholar]
- 3.Boulet SL, Parker C, Altrash H. Preconception care in international setting. Matern Child Health J. 2006;10:29–35. doi: 10.1007/s10995-006-0091-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Squier L, MitchelL EW, Lewis MD, Lynch M, Dolina S, Margolis M, et al. Consumeroliperception of preconception health. Am J Health Promotion. 2013;27:10–9. doi: 10.4278/ajhp.120217-QUAL-95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Sharp PS, Balkhair T, Olison A. Intention to become pregnant, low birth weight and preterm birth: A Systematic review. Maten Child Health J. 2011:15205–16. doi: 10.1007/s10995-009-0546-2. [DOI] [PubMed] [Google Scholar]
- 6.Baduna M, Johnson K, Hench K, Reyes M. Healthy start lessons learned on interconnection care: Women's Health Issues. 2008;18:61–6. doi: 10.1016/j.whi.2008.07.010. [DOI] [PubMed] [Google Scholar]
- 7.Finer LB, Zolina MR. Unintended pregnancy in United States: Incidence and disparities, 2006. Contraception. 2011;84:478–85. doi: 10.1016/j.contraception.2011.07.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Williams L, Morrow B, Shulman H, Stephen R, DH, Step D, Fowler C. PRAMS 2002 surveillance report: Pregnancy Risk Basement Monitoring System. 2006 [Google Scholar]
- 9.Denny CH, Floyd RL, Green PP, Hayles DK. Racial and ethnic disparities in preconception risk factors and preconception. J Obstet Gynecol Neonatal Nurse. 2011;40:109–19. [Google Scholar]
- 10.Ezegwu HU, Dim C, Dim N, Ikema AC. Preconception care in South-Eastern Nigeria. J Obst Gynecol. 2008;28:765–8. doi: 10.1080/01443610802462647. [DOI] [PubMed] [Google Scholar]
- 11.Idris SH, Gambo MN, Ibrahim MS, Muhammed SI. Barriers to utilization of maternal services in a semi-urban community in Northern Nigeria: The clients perspective. Nig Med J. 2013;54:27–32. doi: 10.4103/0300-1652.108890. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Ayalew Y, Mulat A, Dile M, Simegn A. Women’omknowledge and associated factors in preconception care in adet, West Gojjam, Northwest Ethiopia: A community based cross sectional study. Reproduct Health. 2017;14:15. doi: 10.1186/s12978-017-0279-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Madanat AY, Sheshah EA. Preconception care in Saudi women with diabetes mellitus. J Fam Comm Med. 2016;23:109–14. doi: 10.4103/2230-8229.181012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Coonrod DV, Bruce NC, Malcolm TD, Drachman D, Frey KA. Knowledge and attitudes regarding preconception care in a predominantly low-income Mexican American population. Am J Obstet Gynecol. 2009;200:686.e1–7. doi: 10.1016/j.ajog.2009.02.036. [DOI] [PubMed] [Google Scholar]
- 15.Olowokere AE, Komolafe A, Owofadeju C. Awareness, knowledge and uptake of preconception care among women in Ife central local government area of Osun State, Nigeria. J Community Med Prim Health Care. 2015;27:83–92. [Google Scholar]
- 16.Prashansa G, Rojana D. Knowledge on preconception care among reproductive age women. Saudi J Med Pharm Sci. 2016;2:1–6. [Google Scholar]
- 17.Ghaffari F, Jahani Shourab N, Jafarnejad F, Esmaily H. Application of Donabedian quality of care framework to assess the outcomes of preconception care in urban health centers, Mashhad, Iran. J Midw Reprod Health. 2014;2:50–9. [Google Scholar]
- 18.Ahmed KM, Elbashir IM, Mohamed SI, Saeed AM, Alawad AM. Knowledge, attitude and practice of preconception care among Sudanese women in reproductive age about rheumatic heart disease at Alshaab and Ahmad Gassim hospitals in Sudan. Basic Res J Med Clin Sci. 2015;4:199–203. [Google Scholar]