

Abstract
Introduction:
With the development of laparoscopic skills, the laparoscopic common bile duct exploration (LCBDE) and laparoscopic cholecystectomy (LC) has become the standard surgical procedure for choledocholithiasis. We usually use Hem-o-lok clips to control cystic duct and vessels, which is safe on most occasions and has few perioperative complications such as major bleeding, wound infection, bile leakage, and biliary and bowel injury. However, a rare complication of post-cholecystectomy clip migration (PCCM) increases year by year due to the advancement and development of LC, CBD exploration as well as the wide use of surgical ligation clips.
Materials and Methods:
Six patients whose clips are found dropping into CBD or forming T-tube sinus after laparoscopic surgery in our department.
Results:
Six patients whose clips are found dropping into CBD (clip-stone) (3/6) or forming T-tube sinus (T clip-sinus) (3/6) after LCBDE or LC.
Conclusions:
PCCM is a rare but severe complication of LCBDE. A pre-operative understanding of bile duct anatomy, the use of the minimum number of clips and the harmonic scalpel during the surgeries is necessary. Considering clip-stone or clip-sinus in the differential diagnosis of patients with biliary colics or cholangitis after LCBDE even years after surgery, the detailed medical history and pre-operative examination are inevitable, especially for these patients who had undergone LCBDE.
Keywords: Choledocholithiasis, clip-stone, laparoscopic common bile duct exploration, migration, post-cholecystectomy clip migration
INTRODUCTION
Gallstone disease is one of the most common benign diseases, and laparoscopic cholecystectomy (LC) and laparoscopic common bile duct exploration (LCBDE) have become the standard surgical procedure for it.[1] Various clips (Hem-o-lok clips in our department) are used to control vessels and the cystic duct, which is a safer and more efficient way when compared with conventional surgery. However, there is still a high possibility of complications, and the common complications include bile duct injury, bile leakage, infection, gastrointestinal injury, bleeding,[2] deep venous thrombosis of the lower extremity, air embolism, subcutaneous emphysema, etc. In addition, rare complications such as postcholecystectomy clip migration (PCCM), bile duct dysfunction, and bilirubin metabolism disorders have also been reported.[3] The first case of PCCM was reported in 1978 by Walker,[4] which resulted in the formation of CBD stone. Similar cases had been reported afterwards. However, rare clip migration after LCBDE whose clips dropping into CBD or forming T-tube sinus had been reported. Thus, we report six patients whose clips are found dropping into CBD (clip-stone) (3/6) or forming T-tube sinus (T clip-sinus) (3/6) after LCBDE or LC in our department to explore the reasons of it and find a more effective and safe way ligating cystic duct and gallbladder vessels. And also we review the literature from 1997 to 2017 to introduce the characteristics and treatment outcomes of these cases. (We did not search the articles earlier than 1997 considering the technology gap between these two epochs).
MATERIALS AND METHODS
The first three patients underwent LCBDE due to the gallbladder and CBD stones, and we found clips forming T-tube sinus. Patient one, female, 31-year-old, the diameter of the CBD of whom is about 1.2 cm and there are a lot of stones like fine sediments within it, was indwelled with 22#T. Cholangioscope was conducted after 4 months, and we saw a small stone whose diameter was about 8 mm. Much to our surprise, we found the clips had formed a part of the sinus. We removed the stone with the reticular basket. Reviewing the pre-operative computed tomography (CT), we could see a part of sinus was consisted of by Hem-o-lok clips [Figure 1]. During these 4 months, the patient did not have cholangioscope, she was still symptom-free.
Figure 1.

The Hem-o-lok clip near the T-sinus
Patient two, female, 60-year-old, the diameter of the CBD of whom is about 1.1 cm, and there are a lot of small stones within it, was indwelled with 20#T. Cholangioscope was carried out after 3 months, and we saw a small stone whose diameter was around 4 mm. We also found the clips had formed a part of the sinus. Accordingly, we removed the stone with the reticular basket. Reviewing pre-operative CT, we could see a part of sinus was made up of the Hem-o-lok clips. During the whole disease process, the patient was as well symptom-free.
Patient three, female, 83-year-old, the diameter of the CBD is about 1.0 cm, and there is about 1.2 cm stone within it, was indwelled with 20#T. Cholangioscope was implemented after 6 months and we saw two small stones whose diameter was both about 3 mm. We as well found the clips had formed a part of sinus. We removed the stones with the reticular basket. Reviewing the pre-operative CT, we could see a part of sinus was consisted of by the Hem-o-lok clips. During these 6 months, the patient was symptom-free.
Patient four, this 61-year-old woman presented with repeated episodes of jaundice and upper right quadrant abdominal pain with a history of LC for chronic cholecystitis. Laboratory indices were as follows: WBC 16300/mL and total bilirubin 2.7 mg/dL. Abdominal ultrasound indicated the diameter of the CBD of is 1.1 cm, and there is a about 2.8 cm stone within it. Roux-en-Y was performed, and a clip-stone (8 mm × 22 mm) was found in CBD.
Moreover, the following two patients underwent LCBDE due to the gallbladder and CBD stones, and we found clips dropping into CBD. Patient five, female, 72-year-old, the diameter of the CBD of whom is about 1.3 cm and there are a lot of stones ranging from 0.8 cm to 1.2 cm within it, was indwelled with 22#T. Cholangioscope was conducted after 4 months and we saw two small stones. We removed the stones with the reticular basket, and we also pulled out her T tube. However, she felt pain in her right upper quadrant as before after 1½ years. Her CT scan showed a stone about 1.3 cm in CBD. We then performed exploratory laparotomy, bile duct exploration and J tube drainage because her abdominal pain aggravated and she even appeared chills and fever. We cut the stone and saw a Hem-o-lok clip inside [Figure 2 and Video 1]. The J tube was removed under endoscope after 2 weeks, and she discharged without pain or fever.
Figure 2.

A stone in common bile duct and there is a Hem-o-lok clip within it
Patient six, female, 64-year-old, the diameter of the CBD of whom is about 1.5 cm, and there are two large stones (one about 1.2 cm and the other about 1.4 cm), was indwelled with 24#T. However, she appeared symptoms including fever, jaundice, skin itching and so on after 2 months. We performed T-tube cholangiography and we found that the CBD was thickened and the thickest diameter reached 1.4 cm while the lower end of the CBD became thinner and narrowed. The digital subtraction angiography of the biliary tract revealed the narrowing of the CBD and a clip drops into CBD [Figure 3 and Video 2]. As a result, percutaneous transhepatic biliary drainage and stent implantation was performed to relieve her symptoms.
Figure 3.
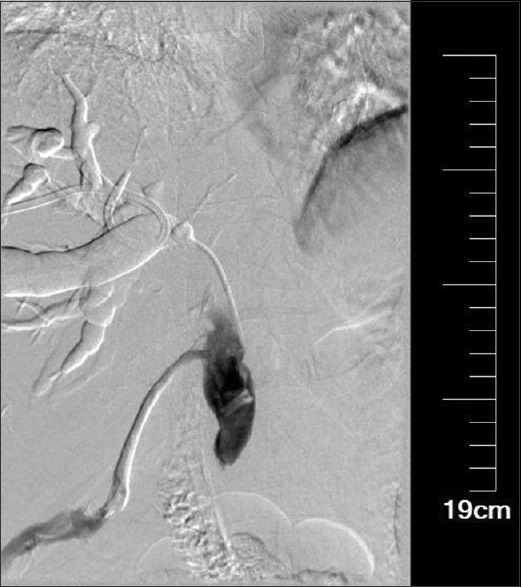
The clip in common bile duct and it has not yet formed a stone
Literature review
We searched through the PubMed, EMBASE, Cochrane, CNKI, Wangfang database using the keywords ‘clip migration’ and ‘bile duct stones’ from 1997 to 2017. We excluded the cases that could not provide adequate details or they were from the same institution. Finally, 53[5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57] publications reporting 64 cases were reviewed.
In these cases, the female was in the majority (n = 35, 54.6%) and the average age at presentations is 59.75-year-old (range 31–93 years). Most of the initial operations are LC (n = 43, 67.1%), some are LCBDE, OC and others. Types of operations are shown in Table 1. The median time of PCCM is 24 months (the average time of PCCM is 55.4 months) (range 1 day to 20 years). Some cases of PCCM caused the corresponding symptoms although hadn’t formed to stone, always in the early 3 months after the operation. The common clinical symptoms of PCCM were right upper abdominal pain, jaundice, fever and rare cases included pyaemia and shock [Table 2]. The median number of the migrated clip was one (range 1–4), and the common migration is to CBD and duodenum [Table 2]. Pre-operative imaging diagnosis varied from US, CT, magnetic resonance cholangiopancreatography to endoscopic retrograde cholangiopancreatography (MRCP to ERCP) [Table 3]. Moreover, the management of PCCM is also multiple. Based on current evidence, ERCP should be the modality of choice with surgery or PTC reserved as rescue procedures, especially in the presence of difficult biliary strictures or large stones [Table 3]. As for T clip-sinus, choledochoscope is the first non-invasive choice with satisfactory results.
Table 1.
Details of gender and initial operations
| n (%) | |
|---|---|
| Gender | |
| Female | 35 (54.7) |
| Male | 26 (40.6) |
| Not mentioned | 3 (4.7) |
| Initial operations | |
| LC | 43 (67.1) |
| LCBDE | 15 (23.4) |
| OC | 4 (6.2) |
| OC + OLT | 1 (1.6) |
| Not mentioned | 1 (1.6) |
LC: Laparoscopic cholecystectomy, LCBDE: Laparoscopic common bile duct exploration, OTP: Orthotopic liver transplantation, OC: Open cholecystectomy
Table 2.
The clinical presentations and migration position of post-cholecystectomy clip migration
| n (%) | |
|---|---|
| Clinical symptoms | |
| RUP | 46 (71.8) |
| Jaundice | 30 (46.9) |
| Fever | 19 (29.7) |
| Chill | 5 (7.8) |
| Nausea/vomiting | 18 (28.1) |
| No symptoms | 12 (18.8) |
| Others* | 5 (7.8) |
| Migration position of PCCM | |
| Common bile duct | 49 (76.6) |
| Duodenum | 4 (6.3) |
| T-tube sinus | 10 (15.6) |
| Gallbladder remnant | 1 (1.6) |
*Other symptoms: Include pancreatitis (n=2), shock (n=1), itch (n=1), pyemia (n=1). RUP: Right upper abdominal pain, PCCM: Post-cholecystectomy clip migration
Table 3.
The pre-operative imaging diagnosis and details of treatment and outcomes of post-cholecystectomy clip migration
| n (%) | |
|---|---|
| Pre-operative imaging diagnosis | |
| X-ray | 9 (14.1) |
| US | 18 (28.1) |
| CT | 19 (29.7) |
| MRCP | 10 (15.6) |
| ERCP | 18 (28.1) |
| T-tube cholangiography | 9 (14.1) |
| Choledochoscope test | 3 (4.7) |
| Details of treatment and outcomes | |
| ERCP | |
| ERCP successful clearance | 35 (54.7) |
| Unsuccessful attempts requiring surgery | 6 (9.4) |
| Surgery* | |
| Initial successful surgery | 7 (10.9) |
| Failed initial ERCP clearance | 6 (9.4) |
| Choledochoscope | 12 (18.8) |
| Others | |
| ERCP + LC | 1 (1.6) |
| Gastroscope | 1 (1.6) |
| PTC | 1 (1.6) |
| Untreated | 1 (1.6) |
*Surgery: Included Roux-en-Y, bile duct exploration, and et al. US: Ultrasound, ERCP: Endoscopic retrograde cholangiopancreatography, LC: Laparoscopic cholecystectomy, PTC: Percutaneous transhepatic cholangiography, CT: Computed tomography, MRCP: Magnetic resonance cholangiopancreatography
DISCUSSION
LCBDE is a relatively safe way to deal with stones in CBD. Overall, PCCM is rare. However, it is possible that the true incidence of PCCM with resultant biliary complications is underestimated.[58] In this paper, clips had migrated into the CBD or formed the T-tube sinus. Common symptoms varied from abdominal pain, obstructive jaundice to fever[58] while rare complications included acute pancreatitis, embolism of the clip and so on.[14,27,39] The etiology of clips migrating into the CBD or forming T-tube sinus remains unclear. As for clip migration, some authors held that the clips were applied improperly so that the cystic duct remained patent due to ineffective clipping resulting in biloma with bile leakage.[23,32,59] However, others deemed that it is inevitable in that even well-placed clips may migrate due to localised inflammatory.[23] In a nutshell, there are many factors that contribute to the migration process and the aforementioned factors include inaccurate clip placements with resultant bile duct injuries, local suppurative inflammatory processes, bile leak with resultant biloma formation, local infective processes as well as the number of clips.[37] Moreover, we found the clips near the T tube and they did not drop into CBD at first while they migrated to CBD once the T tube was removed. As for T-tube sinus, there was no related literature involved about the formation process. We speculated that the distance between the T-tube and the clips might be the main cause. A short distance between them allowed the clips to gradually from the fibrous tissue of T-tube sinus and it is because both of them are foreign matters simultaneously wrapped by fibrous capsule so that we could see the clip inside sinus through choledochoscope. The angle between the two, chronic inflammation and mechanical compression from the surrounding tissues may also prompt the clips to approach the T tube.
The diagnosis primarily relied on some non-invasive examinations, such as ultrasound, CT scan, MRCP and T-tube radiography.[45] Imaging will be required to distinguish between post-cholecystectomy primary CBD stones from PCCM-related biliary complications. Simple abdominal radiography may show abnormal positions of the metal clips.[58] In our cases, diagnosis was based on the abdominal CT scan and was further confirmed by choledochoscope. And with the development of endoscopic technology, ERCP (for clip-stone) and choledochoscope (for T clip-sinus) gradually become the preferential way to deal with clip migration because they are faster, more economic with fewer traumas and complications.[10,60] Performing an adequate EST is necessary and important as it may facilitate spontaneous passage to excrete stones even if the initial ERCP extraction had failed. Surgeries will be operated to handle the difficult clip-stones or acute, serious patients.[23,58] Based on our past experience, bile duct exploration and J tube (a kind of ureteral catheter) drainage (primary suture the CBD) is better than T-tube drainage when tackling a single clip-stone and avoiding the migration again. After 2 weeks, we could remove the J tube with an endoscope to prevent the patients from long-term pains in the T tube.
To prevent surgical clip migration, some put forward that the blind application of clips must be forbidden and it is better to use the minimum number of clips: (1) avoid blind application of clips to control bleeding; (2) limit the length of the residual cystic duct at 0.5 cm–1.0 cm; (3) keep clips away from T-tube as much as possible.[18,23,58] Others deemed that absorbable clips could be used and they emphasised that synthetic, absorbable sutures or other suture materials should be used for biliary surgery to reduce inflammatory reaction.[17,37,61]
CONCLUSIONS
PCCM is a rare but severe complication of LCBDE. A pre-operative understanding of bile duct anatomy, the use of the minimum number of clips and the harmonic scalpel[62] during the surgeries is necessary. Considering clip-stone or clip-sinus in the differential diagnosis of patients with biliary colics or cholangitis after LCBDE even years after surgery, the detailed medical history, and pre-operative examination are inevitable, especially for these patients who had undergone LCBDE. Moreover, we are bound to have a better understanding of the disease as time goes on.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Videos available on: www.journalofmas.com
REFERENCES
- 1.Ellison EC, Carey LC. Cholecystectomy, cholecystostomy and intraoperative evaluation of the biliary tree. In: Baker JR, Fishcer JE, editors. Mastery of Surgery. 4th ed. Philadelphia: Lippincott Williams & Wilkins; 2001. [Google Scholar]
- 2.Huang X, Feng Y, Huang Z. Complications of laparoscopic cholecystectomy in China: An analysis of 39,238 cases. Chin Med J (Engl) 1997;110:704–6. [PubMed] [Google Scholar]
- 3.Wolf AS, Nijsse BA, Sokal SM, Chang Y, Berger DL. Surgical outcomes of open cholecystectomy in the laparoscopic era. Am J Surg. 2009;197:781–4. doi: 10.1016/j.amjsurg.2008.05.010. [DOI] [PubMed] [Google Scholar]
- 4.Walker WE, Avant GR, Reynolds VH. Cholangitis with a silver lining. Arch Surg. 1979;114:214–5. doi: 10.1001/archsurg.1979.01370260104019. [DOI] [PubMed] [Google Scholar]
- 5.Bradfield H, Granke D. Surgical clip as a nidus for a common bile duct stone: Radiographic demonstration. Abdom Imaging. 1997;22:293–4. doi: 10.1007/s002619900192. [DOI] [PubMed] [Google Scholar]
- 6.Venu RP, Brown RD, Rosenthal G, Deutch SF, LoGuidice JA, Pastika B, et al. An impacted metallic clip at the ampulla causing ascending cholangitis. Gastrointest Endosc. 1997;45:435–6. doi: 10.1016/s0016-5107(97)70161-5. [DOI] [PubMed] [Google Scholar]
- 7.Yu SC, Yuan RH, Ho MC, Lee WJ. Duodenal endoclip migration after laparoscopic cholecystectomy: Report of a case. Endoscopy. 1997;29:339. doi: 10.1055/s-2007-1004212. [DOI] [PubMed] [Google Scholar]
- 8.Cetta F, Lombardo F, Baldi C, Cariati A. Clip migration within the common duct after laparoscopic cholecystectomy: A case of transient acute pancreatitis in the absence of associated stones. Endoscopy. 1997;29:S59–60. doi: 10.1055/s-2007-1004338. [DOI] [PubMed] [Google Scholar]
- 9.Herline AJ, Fisk JM, Debelak JP, Shull HJ, Jr, Chapman WC. Surgical clips: A cause of late recurrent gallstones. Am Surg. 1998;64:845–8. [PubMed] [Google Scholar]
- 10.Alberts MS, Fenoglio M, Ratzer E. Recurrent common bile duct stones containing metallic clips following laparoscopic common bile duct exploration. J Laparoendosc Adv Surg Tech A. 1999;9:441–4. doi: 10.1089/lap.1999.9.441. [DOI] [PubMed] [Google Scholar]
- 11.Ng WT, Kong CK, Lee WM. Migration of three endoclips following laparoscopic cholecystectomy. J R Coll Surg Edinb. 1999;44:200–2. [PubMed] [Google Scholar]
- 12.Mansoa A, Martins A, Brito E Melo M, Coito P. Surgical clips as a nidus for stone formation in the common bile duct. Surg Endosc. 2000;14:1189. doi: 10.1007/s004640040026. [DOI] [PubMed] [Google Scholar]
- 13.Matsumoto H, Ikeda E, Mitsunaga S, Naitoh M, Furutani S, Nawa S, et al. Choledochal stenosis and lithiasis caused by penetration and migration of surgical metal clips. J Hepatobiliary Pancreat Surg. 2000;7:603–5. doi: 10.1007/s005340070011. [DOI] [PubMed] [Google Scholar]
- 14.Ammann K, Kiesenebner J, Gadenstätter M, Mathis G, Stoss F. Embolism of a metallic clip: An unusual complication following laparoscopic cholecystectomy. Dig Surg. 2000;17:542–4. doi: 10.1159/000051959. [DOI] [PubMed] [Google Scholar]
- 15.Reis LD. Surgical clips incorporated into a duodenal ulcer: A rare complication after elective laparoscopic cholecystectomy. Endoscopy. 2000;32:S3. [PubMed] [Google Scholar]
- 16.Petersen JM. Surgical clip choledocholithiasis. Gastrointest Endosc. 2002;56:113. doi: 10.1067/mge.2002.123422. [DOI] [PubMed] [Google Scholar]
- 17.Dell’Abate P, Del Rio P, Soliani P, Colla G, Sianesi M. Choledocholithiasis caused by migration of a surgical clip after video laparoscopic cholecystectomy. J Laparoendosc Adv Surg Tech A. 2003;13:203–4. doi: 10.1089/109264203766207753. [DOI] [PubMed] [Google Scholar]
- 18.Hai S, Tanaka H, Kubo S, Takemura S, Kanazawa A, Tanaka S, et al. Choledocholithiasis caused by migration of a surgical clip into the biliary tract following laparoscopic cholecystectomy. Surg Endosc. 2003;17:2028–31. doi: 10.1007/s00464-003-4517-1. [DOI] [PubMed] [Google Scholar]
- 19.Angel R, Abisambra N, Marin JC. Clip choledocholithiasis after laparoscopic cholecystectomy. Endoscopy. 2004;36:251. doi: 10.1055/s-2004-814263. [DOI] [PubMed] [Google Scholar]
- 20.Chong VH, Yim HB, Lim CC. Clip-induced biliary stone. Singapore Med J. 2004;45:533–5. [PubMed] [Google Scholar]
- 21.Liu LF, He K, Liu JJ. A case of three titanium clips in the common bile duct after laparoscopic cholecystectomy. Chin J Hepatobiliary Surg. 2005;1:30. [Google Scholar]
- 22.Mouzas IA, Petrakis I, Vardas E, Kogerakis N, Skordilis P, Prassopoulos P, et al. Bile leakage presenting as acute abdomen due to a stone created around a migrated surgical clip. Med Sci Monit. 2005;11:CS16–8. [PubMed] [Google Scholar]
- 23.Ahn SI, Lee KY, Kim SJ, Cho EH, Choi SK, Hur YS, et al. Surgical clips found at the hepatic duct after laparoscopic cholecystectomy: A possible case of clip migration. Surg Laparosc Endosc Percutan Tech. 2005;15:279–82. doi: 10.1097/01.sle.0000183257.27303.4e. [DOI] [PubMed] [Google Scholar]
- 24.Khanna S, Vij JC. Endoclips as nidus for choledocholithiasis presenting 5 years after laproscopic cholecystectomy. Endoscopy. 2005;37:188. doi: 10.1055/s-2004-826191. [DOI] [PubMed] [Google Scholar]
- 25.Tan HY, Gen XQ. A case of a titanium clip in the formation of stones in the common bile duct. Peoples Mil Surg. 2005;48:616. [Google Scholar]
- 26.Alsulaiman R, Barkun J, Barkun A. Surgical clip migration into the common bile duct after orthotopic liver transplantation. Gastrointest Endosc. 2006;64:833–4. doi: 10.1016/j.gie.2006.04.016. [DOI] [PubMed] [Google Scholar]
- 27.Dolay K, Alis H, Soylu A, Altaca G, Aygun E. Migrated endoclip and stone formation after cholecystectomy: A new danger of acute pancreatitis. World J Gastroenterol. 2007;13:6446–8. doi: 10.3748/wjg.v13.i47.6446. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Attwell A, Hawes R. Surgical clip migration and choledocholithiasis: A late, abrupt complication of laparoscopic cholecystectomy. Dig Dis Sci. 2007;52:2254–6. doi: 10.1007/s10620-006-9101-9. [DOI] [PubMed] [Google Scholar]
- 29.Steffen M, Kronsbein H, Wesche L. Metal clip as a nidus for formation of common bile duct stone following laparascopic cholecystectomy. Z Gastroenterol. 2007;45:317–9. doi: 10.1055/s-2007-962982. [DOI] [PubMed] [Google Scholar]
- 30.Samim MM, Armstrong CP. Surgical clip found at duodenal ulcer after laparoscopic cholecystectomy: Report of a case. Int J Surg. 2008;6:473–4. doi: 10.1016/j.ijsu.2006.06.007. [DOI] [PubMed] [Google Scholar]
- 31.Li HL, Liu ZM. A case of biologic clips walking to common bile duct after laparoscopic cholecystectomy. Chin J Hepatobiliary Surg. 2009;15:577. [Google Scholar]
- 32.Wang YL, Zhang GY, Wang L, Hu SY. Metallic clip migration to T-tube sinus tract after laparoscopic choledochotomy. Acta Chir Belg. 2009;109:242–4. doi: 10.1080/00015458.2009.11680415. [DOI] [PubMed] [Google Scholar]
- 33.Brandt LJ. Surgical clip migration and stone formation in a gallbladder remnant after laparoscopic cholecystectomy. Gastrointest Endosc. 2009;70:780–1. doi: 10.1016/j.gie.2009.05.025. [DOI] [PubMed] [Google Scholar]
- 34.Goshi T, Okamura S, Takeuchi H, Kimura T, Kitamura S, Tamaki K, et al. Migrated endoclip and stone formation after cholecystectomy: A case treated by endoscopic sphincterotomy. Intern Med. 2009;48:2015–7. doi: 10.2169/internalmedicine.48.2634. [DOI] [PubMed] [Google Scholar]
- 35.Lee SL, Kim HK, Cho YS. Acute obstructive cholangitis due to foreign body in the common bile duct. Migrated endoclip. Gastroenterology. 2010;139:e3–4. doi: 10.1053/j.gastro.2009.10.065. [DOI] [PubMed] [Google Scholar]
- 36.Wang ZS, Zhang BY, Wu LQ, et al. A case of intra cholecystectomy after cholecystectomy with endoscopic cholecystectomy. Chin J Gen Surg. 2010;25:855. [Google Scholar]
- 37.Gonzalez FJ, Dominguez E, Lede A, Jose P, Miguel P. Migration of vessel clip into the common bile duct and late formation of choledocholithiasis after laparoscopic cholecystectomy. Am J Surg. 2011;202:e41–3. doi: 10.1016/j.amjsurg.2010.08.011. [DOI] [PubMed] [Google Scholar]
- 38.Molina-Infante J, Fernandez-Bermejo M, Mateos-Rodriguez JM. Migrated surgical clip-induced choledocholithiasis. Endoscopy. 2011;43(Suppl 2):E350–1. doi: 10.1055/s-0030-1256856. [DOI] [PubMed] [Google Scholar]
- 39.Ray S, Bavishi Y. Endoclip migration into the duodenum: An unusual complication after laparoscopic cholecystectomy. Am Surg. 2011;77:E216–7. [PubMed] [Google Scholar]
- 40.Tseng CW, Wei CK, Hsieh YH. Education and imaging. Hepatobiliary and pancreatic: Clip migration after laparoscopic cholecystectomy. J Gastroenterol Hepatol. 2011;26:1695. doi: 10.1111/j.1440-1746.2011.06906.x. [DOI] [PubMed] [Google Scholar]
- 41.Rowe D, Nikfarjam M. Cystic duct clip migration into the common bile duct. Indian J Gastroenterol. 2012;31:86. doi: 10.1007/s12664-011-0155-z. [DOI] [PubMed] [Google Scholar]
- 42.Sajith KG, Dutta AK, Joseph AJ, Simon EG, Chacko A. Tombstone of surgical clip in common bile duct. Trop Gastroenterol. 2012;33:67–9. doi: 10.7869/tg.2012.12. [DOI] [PubMed] [Google Scholar]
- 43.Song M, Kwek BE, Ang TL. Acute cholangitis secondary to a recently migrated cystic duct clip, 15 years after cholecystectomy. Endoscopy. 2012;44(Suppl 2):E294–5. doi: 10.1055/s-0032-1309914. [DOI] [PubMed] [Google Scholar]
- 44.Liu Y, Ji B, Wang Y, Wang G. Hem-o-lok clip found in common bile duct after laparoscopic cholecystectomy and common bile duct exploration: A clinical analysis of 8 cases. Int J Med Sci. 2012;9:225–7. doi: 10.7150/ijms.4023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Ray S, Bhattacharya SP. Endoclip migration into the common bile duct with stone formation: A rare complication after laparoscopic cholecystectomy. JSLS. 2013;17:330–2. doi: 10.4293/108680813X13654754534350. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Sharma M, Singh B, Varghese R. Surgical clips in the common bile duct suspected on endoscopic ultrasound and confirmed on endoscopic retrograde cholangiopancreatography. Endosc Ultrasound. 2013;2:157–8. doi: 10.7178/eus.06.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Photi ES, Partridge G, Rhodes M, Lewis MP. Surgical clip migration following laparoscopic cholecystectomy as a cause of cholangitis. J Surg Case Rep 2014. 2014 doi: 10.1093/jscr/rju026. pii: rju026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Hong T, Xu XQ, He XD, Qu Q, Li BL, Zheng CJ, et al. Choledochoduodenal fistula caused by migration of endoclip after laparoscopic cholecystectomy. World J Gastroenterol. 2014;20:4827–9. doi: 10.3748/wjg.v20.i16.4827. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Ghavidel A. Migration of clips after laparoscopic cholecystectomy; a case report and literature review. Middle East J Dig Dis. 2015;7:45–9. [PMC free article] [PubMed] [Google Scholar]
- 50.Sormaz IC, Keskin M, Sönmez RE, Soytaş Y, Tekant Y, Avtan L, et al. Obstructive jaundice secondary to endoclip migration into common bile duct after laparoscopic cholecystectomy. Minerva Chir. 2015;70:381–3. [PubMed] [Google Scholar]
- 51.Singh MK, Kinder KZ, Braverman SE. Transhepatic management of a migrated intraductal surgical clip after cholecystectomy and gastrectomy. J Vasc Interv Radiol. 2015;26:1866. doi: 10.1016/j.jvir.2015.08.025. [DOI] [PubMed] [Google Scholar]
- 52.Cookson NE, Mirnezami R, Ziprin P. Acute cholangitis following intraductal migration of surgical clips 10 years after laparoscopic cholecystectomy. Case Rep Gastrointest Med 2015. 2015 doi: 10.1155/2015/504295. 504295. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Tang XD, Liu SH, Chen S. Two cases of Hem-o-lock clips wandering in common bile duct after laparoscopic cholecystectomy and bile duct exploration and stone removal. Chin J Dig Endosc. 2015;32:565–6. [Google Scholar]
- 54.Nagorni EA, Kouklakis G, Tsaroucha A, Foutzitzi S, Courcoutsakis N, Romanidis K, et al. Post-laparoscopic cholecystectomy mirizzi syndrome induced by polymeric surgical clips: A case report and review of the literature. J Med Case Rep. 2016;10:135. doi: 10.1186/s13256-016-0932-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Rawal KK. Migration of surgical clips into the common bile duct after laparoscopic cholecystectomy. Case Rep Gastroenterol. 2016;10:787–92. doi: 10.1159/000453658. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Antunes AG, Peixe B, Guerreiro H. Pancreatitis and cholangitis following intraductal migration of a metal clip 5 years after laparoscopic cholecystectomy. Gastroenterol Hepatol. 2017;40:615–7. doi: 10.1016/j.gastrohep.2016.08.007. [DOI] [PubMed] [Google Scholar]
- 57.Qu JW, Wang GY, Yuan ZQ, Li KW. Hem-o-lok clips migration: An easily neglected complication after laparoscopic biliary surgery. Case Rep Surg 2017. 2017 doi: 10.1155/2017/7279129. 7279129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Chong VH, Chong CF. Biliary complications secondary to post-cholecystectomy clip migration: A review of 69 cases. J Gastrointest Surg. 2010;14:688–96. doi: 10.1007/s11605-009-1131-0. [DOI] [PubMed] [Google Scholar]
- 59.Tsumura H, Ichikawa T, Kagawa T, Nishihara M, Yoshikawa K, Yamamoto G, et al. Failure of endoscopic removal of common bile duct stones due to endo-clip migration following laparoscopic cholecystectomy. J Hepatobiliary Pancreat Surg. 2002;9:274–7. doi: 10.1007/s005340200032. [DOI] [PubMed] [Google Scholar]
- 60.Kager LM, Ponsioen CY. Unexpected bile duct stones formed around surgical clips 4 years after laparoscopic cholecystectomy. Can J Surg. 2009;52:E114–6. [PMC free article] [PubMed] [Google Scholar]
- 61.Leung KL, Kwong KH, Lau WY, Chung SC, Li AK. Absorbable clips for cystic duct ligation in laparoscopic cholecystectomy. Surg Endosc. 1996;10:49–51. doi: 10.1007/s004649910012. [DOI] [PubMed] [Google Scholar]
- 62.Catena F, Ansaloni L, Di Saverio S, Gazzotti F, Coccolini F, Pinna AD, et al. Prospective analysis of 101 consecutive cases of laparoscopic cholecystectomy for acute cholecystitis operated with harmonic scalpel. Surg Laparosc Endosc Percutan Tech. 2009;19:312–6. doi: 10.1097/SLE.0b013e3181b16662. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.