

Abstract
The doubling of the divorce rate among individuals over age 50 during the past 20 years underscores the urgency of studying the consequences of gray divorce and subsequent repartnering for adult well-being. We filled this gap by using the 1998–2014 Health and Retirement Study to evaluate how the levels of depressive symptoms changed following gray divorce versus widowhood. Individuals who divorced or became widowed already had experienced higher levels of depressive symptoms before dissolution relative to those who remained married. Compared with those who became widowed, those who transitioned to divorce experienced a lower elevation and a shorter time to recovery in depressive symptoms. When repartnering, both groups experienced similar magnitudes of initial reduction and subsequent rates of increase. Both the negative consequences of marital dissolution and the beneficial effects of repartnership for mental health persisted for several years, although ultimately they reverted to their pre-dissolution levels of depressive symptoms.
Keywords: crisis versus chronic strain, gray divorce, repartnering, selection, widowhood
Marital dissolution is stressful, often leading to poor health and lower well-being. For decades, gerontological research has focused on widowhood, overlooking divorce in later life. The divorce rate among persons aged 50 and older (gray divorce hereafter) has doubled over the past two decades (Brown and Lin 2012; Kennedy and Ruggles 2014). Roughly one in four divorces in 2010 occurred to persons aged 50 and older, in contrast to less than one in ten divorces in 1990 (Brown and Lin 2012). It is unclear whether the gray divorce rate will continue to rise or the upsurge simply reflects the experiences of a cohort who came of age during the dramatic increase in divorce during the 1970s. Even if the rate remains constant over the next 20 years, the number of older adults who will experience divorce in 2030 will rise by one third because of rapid population aging (Brown and Lin 2012).
Marital dissolution is not merely a discrete event, but rather a process that unfolds over time, shaping individual well-being while the marriage is still intact and after the dissolution has occurred (Amato 2000; Lee and DeMaris 2007). It may operate as either an acute or a chronic stressor. Becoming widowed is typically conceptualized as a temporary stressor that involves a decline in psychological well-being during a bereavement period (defined as six months in the Diagnostic and Statistical Manual of Mental Disorders, DSM) followed by recovery (Umberson, Thomeer, and Williams 2013). However, nearly all of the research on the linkages between widowhood and psychological well-being is either cross-sectional or relies on data measured at only two points in time (Sasson and Umberson 2014), making it difficult to discern whether the mental health of widow(er)s eventually returns to pre-widowhood levels and if so how long the recovery takes.
Prior research on divorce adjustment has differentiated between a temporary crisis period (about two years after divorce) from which individuals ultimately recover and a chronic strain that persists essentially indefinitely (Amato 2000; Hetherington and Kelly 2002; Wallerstein, Lewis, and Blakeslee 2000). Studies have lent empirical support to both the crisis model (Blekesaune 2008; Kalmijn 2017; Lorenz et al. 2006) and the chronic strain model (Johnson and Wu 2002), but they are based on divorce during younger adulthood. Whether gray divorce acts as an acute or chronic stressor for older adults’ mental health remains unknown. It is also unclear whether gray divorce is more (or less) detrimental relative to widowhood.
Repartnering following later-life marital dissolution is increasingly common, particularly among those who experienced a gray divorce (Brown et al. 2018). Repartnering after widowhood has been linked to fewer depressive symptoms relative to remaining single (Carr 2004; Hughes and Waite 2009). The potential mental health benefits of repartnering after gray divorce have not been investigated. Still, prior work on marital formation indicates that mental health benefits are temporary, reflecting a “honeymoon effect” (Kalmijn 2017:1612). Additionally, whether gray divorcé(e)s reap greater (or lesser) benefits from repartnering than widow(er)s and the extent to which repartnering could offset the negative consequences of later-life marital dissolution have not yet been examined.
Using the 1998–2014 Health and Retirement Study, this study fills gaps in the literature by answering three sets of questions. First, we ask whether marital dissolution, distinguishing between gray divorce and widowhood, has a positive effect on depressive symptoms and if so, whether these effects align with the crisis or chronic strain models. We also assess whether gray divorce is more (or less) detrimental than widowhood in later life. The second aim of this study is to examine whether repartnering after either gray divorce or widowhood has temporary negative effects on depressive symptoms consistent with the honeymoon effect. Last, we examine whether repartnering offsets the potentially negative consequences of later-life marital dissolution for mental health. We explore gender differences as marital dissolution often has different consequences for women and men (Amato 2010; Umberson et al. 2013) and the unbalanced sex ratio at older ages yields unique repartnering environments for women and men (Schimmele and Wu 2016). As more older adults experience gray divorce, it is important to understand how marital dissolution and subsequent repartnering are related to psychological well-being and how divorcé(e)s fare relative to widow(er)s.
BACKGROUND
The U.S. is an aging society. Currently, about 1 in 3 persons living in the U.S. is aged 50 or older. Scholars have focused on widowhood and extensively examined its consequences for older adult well-being. As recently as 2014, the Journals of Gerontology, Series B published a special issue on widowhood and bereavement. Few thought older people divorce in large numbers. Nevertheless, divorce after age 50 can no longer be ignored. The gray divorce rate has doubled, rising from 4.9 to 10.1 divorced persons per 1,000 married persons between 1990 and 2010 (Brown and Lin 2012). Over 600,000 people aged 50 and older got divorced in 2010. This rise came as a surprise to many scholars because the overall divorce rate in the U.S. remained stable during this period.
Many people form new unions following marital dissolution. Widowhood results in only one single person but divorce leaves two people available for repartnering. The rise of gray divorce suggests that in the future, more people will repartner in later life. The patterns of repartnering depend on dissolution type and gender. Repartnering following a gray divorce is more common than repartnering after widowhood (Brown et al. 2018). Although men are more likely than women to repartner (Brown, Bulanda, and Lee 2012; Vespa 2012), the gap between the divorced and the widowed is larger for women than men. Gray divorced women are about four times more likely to be repartnered than widowed women (24% versus 6%). By comparison, gray divorced men are only about 50% more likely than widowed men to be repartnered (43% versus 24%) (Brown et al. 2018). In short, contemporary patterns of later-life marital dissolution and subsequent repartnering underscore the need to address their ramifications for individual well-being.
Marital Dissolution and Depressive Symptoms
Marital dissolution is one of the most traumatic life transitions a person can experience (Carr and Pudrovska 2012). Both widowhood and divorce are linked to significant decreases in mental health. Individuals typically recover from the initial decline in psychological well-being after widowhood, leading some scholars to conclude that the detrimental effects of widowhood are largely due to the temporary stress of the event (i.e., bereavement) rather than an enduring effect that could result from the loss of resources (Umberson et al. 2013). Nevertheless, the vast majority of widowhood studies are cross-sectional or based on two waves of data. Thus, whether widow(er)s eventually return to the pre-widowhood level of well-being is unclear, although two recent studies suggest it may take up to eight years to recover to pre-widowhood levels of well-being (Lucas et al. 2003:535; Sasson and Umberson 2014:Figure 3), which does not align with the bereavement model.
Similarly, the evidence for the crisis versus chronic strain models is somewhat mixed. Some studies support the crisis model, showing that people gradually adjust to post-divorce life and their well-being returns to the pre-divorce level within a few years after divorce. Longitudinal studies of working-aged adults using U.S., British, and Switzerland data all documented significant increases in depressive feelings immediately after divorce that dissipated in two to five years (Blekesaune 2008; Kalmijn 2017; Lorenz et al. 2006). In contrast, the chronic strain model, which suggests that divorce has enduring negative effects on psychological well-being, has received support in other studies (Johnson and Wu 2002; Umberson et al. 2013).
Because the research to date has not differentiated divorce after age 50 and the U.S. studies relied on data that preceded the upsurge in gray divorce, it is unclear whether gray divorce acts as an acute or chronic stressor for older adults’ mental health. It may be that divorce operates similarly regardless of the age at which it occurs, and thus the negative consequences of gray divorce for mental health are temporary. Alternatively, the negative consequences of gray divorce may persist as a chronic strain because it is harder for older adults to recover from financial loss and reconstruct their social networks.
Moreover, it is unclear whether gray divorce is more (or less) detrimental for psychological well-being relative to widowhood. On the one hand, gray divorce may be more deleterious than widowhood because widow(er)s tend to receive more economic and social supports than divorcé(e)s (Kalmijn 2007; Lin, Brown, and Hammersmith 2017). On the other hand, gray divorce may be more benign than widowhood because the transition to divorce often involves a calculated decision-making process (at least for the initiator) whereas widowhood is involuntary (Bair 2007). Furthermore, emotional loneliness due to the death of a spouse is unlikely to be mitigated by other sources of social support (Stroebe et al. 1996). A British study (Wade and Pevalin 2004) showed that both divorcé(e)s and widow(er)s experienced the onset of poor mental health prior to marital dissolution and their mental health gradually improved after the transition. Relative to the widowed, the divorced experienced a flatter rate of mental health decline immediately before marital dissolution and a slower rate of recovery afterwards, but it took about the same amount of time for both divocé(e)s and widow(er)s to recover. This study, however, was based on divorce in the general adult population and was not specific to gray divorce. Additionally, although prior studies using more than two waves of panel data suggest no gender differences in mental health trajectories after widowhood (Sasson and Umberson 2014) or divorce (Blekesaune 2008; Kalmijn 2017; Strohschein et al. 2005), whether this applies to gray divorce remains unknown.
Repartnering after Marital Dissolution and Depressive Symptoms
Repartnering after marital dissolution, through either remarriage or cohabitation, presumably is beneficial for mental health, because couples can pool resources and provide emotional support to each other (Umberson and Montez 2010). Following widowhood, remarriage is associated with gains in psychological well-being (Wilcox et al. 2003). The pattern for divorced adults is similar with repartnered persons reporting fewer depressive symptoms compared with those who remained unpartnered after divorce (Johnson and Wu 2002; Strohschein et al. 2005). Yet, the benefit of repartnering, at least following divorce, seems to be temporary as distress returned to the pre-repartnering level in four years (Blekesaune 2008), likely reflecting the “honeymoon effect” (Kalmijn 2017). These studies focused on divorce during younger adulthood and were conducted before the rise of gray divorce. Whether the beneficial effects of repartnering after widowhood or gray divorce are temporary is unknown.
It is also unclear whether gray divorcé(e)s reap greater (or lesser) benefits from repartnering than widow(er)s. Because divorcé(e)s tend to face greater economic hardship and receive less social support than widow(er)s (Kalmijn 2007; Lin et al. 2017), repartnering may advantage divorcé(e)s more than widow(er)s. Conversely, divorcé(e)s often feel betrayed by their previous spouse and have difficulties establishing trust in the new relationship (Barrett 2000; Brimhall et al. 2008). Therefore, repartnering may bring fewer mental health benefits to divorcé(e)s than widow(er)s. Most research on remarriage centers on younger adulthood and studies on remarriage after widowhood are slim (Sweeney 2010). Two cross-sectional studies showed no difference in depressive symptoms between divorcé(e)s and widow(er)s who remarried (Barrett 2000; Hughes and Waite 2009) and the duration of remarriage was equally advantageous for both groups (Barrett 2000). Because these studies did not focus on gray divorce specifically, it is unclear whether the same finding holds in later life.
Prior studies have suggested that marital loss is harmful and marital gain is beneficial for mental health (Simon 2002), but the extent to which subsequent repartnering could offset the negative consequences of divorce or widowhood has not yet been examined. Strohschein and her colleagues (2005: 2299) claimed that the magnitude of the negative consequence of divorce was larger than the magnitude of the positive effect of repartnering for mental health, although the difference was not statistically tested. Kalmijn (2017:1625) found the effect of divorce on depressive feelings was 2.5 times stronger than the impact of marriage entry, but his measure of marriage entry mixed first marriages with remarriages. Because neither of the studies focused on gray divorce or widowhood, nor did they examine subsequent repartnering after marital dissolution (i.e., within-person change), the extent to which repartnering counteracts the negative consequences of later life marital dissolution, whether through gray divorce or widowhood, is unclear. Additionally, prior studies have demonstrated men tend to reap more mental health benefits from remarriage than women (Dykstra and de Jong Gierveld 2004; Umberson et al. 2013; Williams 2003). Whether there are similar gender differentials in the benefits of repartnering, particularly after gray divorce, has not been investigated.
Selection
Although marital dissolution tends to hurt mental health and repartnership protects it, one cannot rule out the social selection explanation. Marital dissolution can be selective of those with lower levels of mental health, probably reflecting the strain in marital quality that often precedes divorce or the stresses associated with spousal caregiving during a protracted illness (Amato 2000; Umberson et al. 2013). Likewise, people with better health are more likely to repartner, probably because they are more attractive as potential partners and they have the wherewithal to pursue repartnering (Brown et al. 2018). Instead of comparing continuously married persons with divorced (or widowed) persons or divorced (or widowed) persons who repartner with divorced (or widowed) persons who remain single, researchers need to take into account any selection effect by following individuals before marital dissolution and repartnership. A handful of studies that have adopted this prospective approach support both the social selection and social causation explanations. Individuals who got divorced or experienced widowhood already had experienced poorer mental health before marital dissolution. After controlling for mental health prior to a marital transition, divorce and widowhood have additional negative effects and repartnering has positive effects on mental health (Blekesaune 2008; Johnson and Wu 2002; Sasson and Umberson 2014; Wade and Pevalin 2004).
The Present Study
Patterns of later life marital dissolution are shifting. Despite the doubling of the gray divorce rate, little is known about how gray divorce influences older adults’ mental health and whether repartnering can offset the potential negative impact. The extent to which gray divorce is more detrimental than widowhood and whether repartnering offers differential benefits for divorcé(e)s versus widow(er)s also have not been studied. Our study is the first to examine the mental health consequences of marital dissolution, distinguishing between gray divorce and widowhood, along with subsequent repartnering.
We posit that marital dissolution, whether through widowhood or gray divorce, is a temporary life crisis in which depressive symptoms rise precipitously immediately following dissolution but gradually dissipate over time. Alternatively, if marital dissolution operates as a persistent chronic strain, we would observe an abrupt increase in depressive symptoms right after dissolution that then remain at this elevated level with no evidence of recovery. On the one hand, widowhood may be more benign than divorce because widow(er)s tend to receive more economic and social support than divorcé(e)s. On the other hand, divorce may be less detrimental to mental health than widowhood because widowhood is involuntary and emotional loneliness due to the death of a spouse is difficult to be mitigated by other sources of social support.
Likewise, we test whether repartnering has comparable benefits for those who were gray divorced or widowed since there is no basis from which to argue that one group should reap larger (or smaller) benefits from repartnering. If the benefits of repartnering are temporary as suggested by the honeymoon effect documented in Kalmijn’s (2017) analysis of marriage and well-being, we would anticipate that depressive symptoms drop precipitously right after repartnering but then gradually increase over time.
Additionally, we examine whether the gain from repartnering is greater or smaller than the loss from marital dissolution in later life. Based on prior studies (Kalmijn 2017; Strohschein et al. 2005), we expect that the benefits of repartnering will not entirely offset the losses from marital dissolution.
In this study, we also consider demographic characteristics that may confound the associations of depressive symptoms with marital dissolution and repartnership. People in a higher order marriage, younger people, minorities, and people with lower educational attainment or lower incomes are more likely to experience gray divorce compared with their respective counterparts (Brown and Lin 2012; Lin et al. 2018). Many of these factors are also tied to widowhood, with age and minority status positively related to spousal loss and education negatively associated with widowhood (Sullivan and Fenelon 2014). Among unmarried older adults, those who are younger, white, and have more socioeconomic resources more often repartner than their respective counterparts (Brown et al. 2012; Schimmele and Wu 2016; Vespa 2012). Age, being white, education, and income also negatively relate to depressive symptoms among older adults (Lee and DeMaris 2007; Sasson and Umberson 2014).
DATA AND METHODS
Data used in the analysis came from the 1998–2014 Health and Retirement Study (HRS), a longitudinal survey of a nationally representative, continuous cohort of individuals in the U.S. born before 1960. The HRS began interviewing in 1992 with a cohort of individuals born in 1931–1941 and re-interviews have been conducted every other year. In 1998, three additional cohorts were added to the study to make the sample representative of individuals aged 51 or older. Refresher samples aged 51–56 were added in 2004 and 2010 to maintain a nationally representative sample of the target population. The baseline interview response rates for various cohorts range from 70 to 82% and the re-interview response rates hover around 85 to 93%.
The HRS covers a range of topics, including respondents’ marital histories, demographic characteristics, household incomes, and depressive symptoms, making the data ideal for the purpose of this study. We created a marital history file to track the marriages formed and dissolved by all respondents. The HRS also includes information on cohabitation status at each interview which allows us to track cohabitation experiences among HRS respondents. In total, 33,492 respondents were interviewed in 1998 or later. Of them, 22,292 reported being married at any wave between 1998 and 2014. We further excluded respondents who were under age 50 (n = 637), who were in same-sex unions (n = 54), or who had a baseline weight equal to zero (n = 852). Finally, we removed 921 respondents who did not answer questions regarding depressive symptoms at any wave, yielding 19,828 respondents. Of these respondents, 15,320 were continuously married (77.3%), 3,646 became widowed (18.4%), and 862 separated or got divorced (divorced hereafter, 4.3%). Respondents were observed until they died or until the last interview in 2014.1
Measures
Depressive symptoms were measured using an abbreviated version of the Center for Epidemiologic Studies Depression Scale (CES-D, Radloff 1977). Respondents were asked whether they experienced the following symptoms much of the time during the week prior to the interview (yes versus no): feeling depressed, feeling that everything was an effort, having restless sleep, being unhappy, feeling lonely, feeling sad, being unable to get going, and not enjoying life. This abbreviated version, composed of the sum of these eight items, shares similar psychometric properties as the full CES-D scale (Turvey, Wallace, and Herzog 1999). The internal reliability coefficient for all eight items in the current study ranged from .75 to .80 across waves.
Marital dissolution was gauged by two time-invariant indicators of whether the respondent eventually got divorced (1 = Yes, 0 = No) or became widowed (1 = Yes, 0 = No). Marital status was a time-varying measure captured at each wave to distinguish among those who got divorced, became widowed, or remained married (reference category). Repartnering was also a time-varying variable measured at each wave to distinguish between repartnering through marriage or cohabitation versus remaining either divorced or widowed (reference category). Time since dissolution (repartnering) was a time-varying variable that clocked the number of years since the marital dissolution (repartnering) occurred. For respondents who were continuously married (remained divorced or widowed), this variable was coded 0 throughout the study. Additional details on these variables are in the Analytic Strategy section.
Several demographic characteristics were considered. Marriage order was a dichotomous variable indicating whether the current marriage was a first marriage (coded 0) or a higher-order marriage (coded 1). Respondent’s age at baseline was measured in years. Gender was coded 1 if woman and 0 if man. Racial and ethnic background was gauged by white (reference category), black, Hispanic, or other race. Education was captured by a set of four categorical variables: less than high school (reference category), high school, some college, and college or higher.
Household income was a time-varying measure of the logged value of real 1998 dollars, including earnings, capital income, pensions, annuities, social security income, unemployment or worker’s compensation, veterans’ benefits, welfare, food stamps, and other income from the year prior to the interview. Cohort consisted of three dichotomous variables indicating the year in which the respondent entered the HRS: the HRS cohort (1998 or earlier, reference category), the Early Baby Boomer cohort (2004), and the Mid Baby Boomer cohort (2010). Because less than 1% of covariates had missing values, we used the mode to impute missing data.
Analytic Strategy
We conducted three analyses. First, we compared the baseline characteristics of respondents who remained married, who became widowed, and who got divorced using means and percentages (as appropriate). Second, we estimated a multilevel model to capture pre-dissolution depressive symptoms and then followed the trajectory of depressive symptoms during and after marital dissolution to examine how individual depressive symptoms changed in response to divorce or widowhood. Because repeated measures of depressive symptoms were nested within individuals, a two-level model was estimated. This approach was used by Sasson and Umberson (2014) to examine depressive symptoms trajectories for the transition to widowhood (versus continuous marriage), but they did not consider subsequent repartnering, nor did they examine divorce. The model is specified as follows:
The level 1 equation describes how each person i’s depressive symptoms Y change over time t. Traditionally, the level 1 equation consists of only one intercept (π0i, depressive symptoms measured at time 0 for person i) and one slope (π1i, rate of change in individual i’s depressive symptoms trajectory after time 0). In this specification, we added six additional intercepts and slopes to create person-specific discontinuities in the trajectory after divorce or widowhood (Singer and Willett 2003). These intercepts and slopes allow respondents’ trajectories in Y to change at the point at which they transitioned to some state (divorce or widowhood). Both Divit and Widit are time-varying dichotomous variables for person i, where t is equal to year 0, 2, 4, etc. These two variables were coded 1 if the respondent got divorced (Divit) or became widowed (Widit) and 0 otherwise. Coefficients π2i and π3i capture the shift in elevation in response to divorce and widowhood, respectively. By comparing these two coefficients, we can evaluate whether divorce is more (or less) detrimental than widowhood immediately following a marital dissolution in later life.
Both PostDivit and PostWidit clock the time since marital dissolution. These two variables were coded 0 before respondents got divorced or became widowed and started counting the time (e.g., 1, 2, 3 years, etc.) once marital dissolution occurred. Coefficients π4i and π5i gauge the shift in the slope after divorce or widowhood occurred, respectively. We also added squared terms PostDivit2 and PostWidit2 to allow nonlinear changes in depressive symptoms after divorce or widowhood. By testing π4i + π6i = π5i + π7i, we can gauge whether divorce has more (or less) negative enduring effects than widowhood. Together, using estimates from these parameters, we are able to determine whether marital dissolution immediately elevates divorcé(e)s’ and widow(er)s’ depressive symptoms as well as how much time it takes for divorcé(e)s and widow(er)s to return to the pre-dissolution level of depressive symptoms. xit is a vector of time-varying covariates that may confound the association between marital dissolution and depressive symptoms (i.e., household income). εit is the error term for observation t for individual i.
The level 2 equations describe how the change in depressive symptoms varies between individuals. Coefficients γ00 and γ10 are population averages of the level-1 intercept and slope, respectively, for the continuously married. The coefficient vector γ0m is the population average difference in the level-1 intercept for a one-unit difference in the level-2 predictor vector xmi, whereas the coefficient vector γ1n is the population average difference in the level-1 slope for a one-unit difference in the level-2 predictor vector xni. The vectors xmi and xni are covariates (i.e., marriage order, age, gender, race and ethnic background, education, and cohort) that may account for the between-individual variation. In addition, we included two dichotomous measures—whether respondents got divorced or became widowed versus continuously married—to account for the possibility that those who got divorced or became widowed may already have had higher levels of depressive symptoms before marital dissolution occurred. The variances ζ0i and ζ1i are level-2 residual variances.
In the last analysis, we considered whether repartnering after marital dissolution offsets the negative effect of divorce or widowhood on depressive symptoms and whether the effect is temporary. The model is specified as follows:
Six additional variables RepartAfterDivit, RepartAfterWidit, PostRepartAfterDivit, PostRepartAfterWidit, PostRepartAfterDivit2, and PostRepartAfterWidit2 were added to the level 1 equation. Both RepartAfterDivit and RepartAfterWidit were coded 1 if respondents repartnered through remarriage or cohabitation after divorce (RepartAfterDivit) or widowhood (RepartAfterWidit) and 0 otherwise. A negative value of π8i (or π9i) suggests that divorcé(e)s (or widow(er)s) who repartnered experience a reduction in depressive symptoms compared to divorcé(e)s (or widow(er)s) who remained single. By comparing coefficients π8i and π9i, we can evaluate whether repartnering is more (or less) beneficial for divorcé(e)s than widow(er)s immediately after repartnership.
Both PostRepartAfterDivit and PostRepartAfterWidit clock the time since repartnering occurred. These two variables were coded 0 before respondents repartnered and started counting the time (e.g., 1, 2, 3 years, etc.) once repartnering occurred. A positive value of π10i (or π11i) indicates that divorcé(e)s (or widow(er)s) who entered repartnership have an accelerating rate of increase in depressive symptoms. A more positive value of π10i (or π11i) implies that divorcé(e)s (or widow(er)s) who repartnered have a steeper increase in depressive symptoms relative to divorcé(e)s who remained single. We also added squared terms PostRepartAfterDivit2 and PostRepartAfterWidit2 to allow nonlinear changes in depressive symptoms after repartnering. By testing π10i + π12i = π11i + π13i, we can examine whether repartnering after divorce has a more (or less) beneficial enduring effect than repartnering after widowhood. Additionally, we tested π2i = |π8i| and π3i = |π9i| to examine whether the gain from repartnering offsets the loss from divorce and widowhood, respectively. Finally, we repeated the second and third analyses for women and men separately to explore whether there are gender differences.
For the first analysis, baseline sample weights were used to adjust for the unequal probability of selection (for blacks, Hispanics, and respondents living in Florida) and nonresponse (Ofstedal et al. 2011). For the second and third analyses, we applied normalized wave-specific sample weights to the level 1 and baseline sample weights to the level 2 of the model (Heeringa, West, and Berglund 2017). We also computed robust standard errors to reflect the intra-clustering correlations arising from the HRS sampling strata for all three analyses. Because individuals with depression are more likely to drop out of the longitudinal study compared with those who are non-depressed, we included eight wave-specific indicators (1 = dropout at a given follow-up and 0 = remaining in the study) to take into account potential bias due to differential attrition (Muthén et al. 2011).
RESULTS
We compared individuals who transitioned to divorce or widowhood with those who remained married using baseline information, as shown in Table 1. On average, individuals who got divorced reported the highest level of depressive symptoms (1.80), followed by those who became widowed (1.53), and lastly those who remained married (1.23). More than three times as many who experienced divorce than widowhood subsequently repartnered (31.11% versus 8.66%). Those who got divorced were the youngest (56.22 years old) and most likely to be minorities (24.85% = 12.60% + 8.90% + 3.35%) or in a higher-order marriage (60.62%), whereas those who became widowed were the oldest (65.55 years old) and most likely to be whites (84.30%) or in a first marriage (70.84%). The continuously married were in the middle in terms of their age, race and ethnic background, and marriage order among the three groups. More than two thirds of the individuals who became widowed were women and one quarter of the individuals who became widowed did not have a high school degree, but the continuously married and those who got divorced were equally like to be women and shared similar educational attainment levels. The vast majority of individuals who transitioned to widowhood belonged to the HRS cohort (93.11%), while a substantial share of individuals who remained married (44.06% = 23.84% + 20.22%) or got divorced (45.80% = 25.74% + 20.06%) were Early or Mid Baby Boomers. Overall, individuals who became widowed had the lowest median household incomes of $35,900.00, followed by those who got divorced ($50,524.32), and then those who remained married ($57,081.71).
Table 1.
Weighted Mean (Standard Deviation) or Percentage for the Characteristics of the Sample by Later-Life Marital Transition
| Continuously Married (1) | Transition to Widowhood (2) | Transition to Divorce (3) | |
|---|---|---|---|
| Depressive symptoms at baseline12,13,23 | 1.23 (1.73) | 1.53 (2.18) | 1.80 (2.12) |
| Repartner after dissolution23 | |||
| No | - | 91.34 | 68.89 |
| Yes | - | 8.66 | 31.11 |
| Marriage order12,13,23 | |||
| First marriage | 66.83 | 70.84 | 39.38 |
| Higher-order marriage | 33.17 | 29.16 | 60.62 |
| Age at baseline12,13,23 | 58.45 (8.16) | 65.55 (11.56) | 56.22 (6.28) |
| Gender12,23 | |||
| Women | 44.45 | 68.95 | 46.62 |
| Men | 55.55 | 31.05 | 53.38 |
| Race and ethnicity12,13,23 | |||
| White | 80.49 | 84.30 | 75.15 |
| Black | 7.17 | 7.53 | 12.60 |
| Hispanic | 8.77 | 6.17 | 8.90 |
| Other race | 3.57 | 1.99 | 3.35 |
| Educational attainment12,23 | |||
| Less than high school | 15.89 | 25.09 | 17.39 |
| High school | 30.11 | 38.84 | 25.74 |
| Some college | 24.17 | 19.95 | 27.26 |
| College or higher | 29.83 | 16.13 | 29.60 |
| Median household income at baseline12,13,23 | 57,081.71 | 35,900.00 | 50,524.32 |
| Cohort12,23 | |||
| HRS | 55.94 | 93.11 | 54.20 |
| Early Baby Boomer | 23.84 | 5.38 | 25.74 |
| Mid Baby Boomer | 20.22 | 1.51 | 20.06 |
| Unweighted N | 15,320 | 3,646 | 862 |
Note. Column total may not equal 100% due to rounding error. Superscripts indicate that the two groups statistically differ at p < .05 (two-tailed tests)
Next, we estimated a multilevel model to examine the utility of the crisis versus chronic strain models for those who experienced gray divorce and the bereavement model for individuals who became widowed. Specifically, we tested the effect of elapsed time since divorce or widowhood on depressive symptoms and compared how the trajectories differed from those who remained married. The estimates are shown in Model 1 of Table 2. Individuals who got divorced or became widowed exhibited higher levels of depressive symptoms even before marital dissolution occurred, .642 and .263 points, respectively, higher than those who remained married. Moreover, individuals who got divorced reported higher levels of depressive symptoms than those who became widowed before their marital transition (.642 versus .263, p < .05, denoted by a superscript a in the table). Despite controlling for pre-dissolution differences, depressive symptoms still rose precipitously immediately following marital dissolution, more so for the transition to widowhood than divorce (1.080 versus .283, p < .05, denoted by a superscript b in the table). The detrimental effects of marital dissolution persisted for several years, although the level of depressive symptoms gradually dissipated and then leveled off, at a faster rate for those who became widowed than for those who got divorced (−.325 + .018 versus −.150 + .005, p < .05, denoted by a superscript c in the table).
Table 2.
Regression Coefficients from Discontinued Multilevel Models Predicting Depressive Symptoms
| Model 1 |
Model 2 |
|||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Initial Status | Rate of Change | Initial Status | Rate of Change | |||||||
| Intercept | 2.921 | *** | −.104 | *** | 2.892 | *** | −.100 | *** | ||
| Time-invariant covariates | ||||||||||
| Divorced group | .642 | *** | a | .025 | + | .640 | *** | d | .025 | + |
| Widowed group | .263 | *** | a | .019 | *** | .267 | *** | d | .019 | *** |
| Higher-order marriage | .169 | *** | .002 | .170 | *** | .002 | ||||
| Age at baseline | −.014 | *** | .002 | *** | −.014 | *** | .002 | *** | ||
| Women | .282 | *** | −.005 | + | .281 | *** | −.005 | * | ||
| Black | .336 | *** | −.020 | *** | .336 | *** | −.020 | *** | ||
| Hispanic | .329 | *** | −.014 | * | .330 | *** | −.014 | * | ||
| Other race | .489 | *** | −.019 | + | .494 | *** | −.020 | + | ||
| High school | −.464 | *** | .001 | −.465 | *** | .001 | ||||
| Some college | −.658 | *** | .007 | −.661 | *** | .007 | ||||
| College or higher | −.881 | *** | .004 | −.884 | *** | .004 | ||||
| Early Baby Boomer | −.128 | + | −.012 | + | −.126 | + | −.012 | + | ||
| Mid Baby Boomer | −.299 | *** | −.004 | −.298 | *** | −.005 | ||||
| Time-varying covariates | ||||||||||
| Transition to divorce | .283 | + | b | .352 | * | e | ||||
| Transition to widowhood | 1.080 | *** | b | 1.097 | *** | e | ||||
| Year since divorce | −.150 | *** | c | −.148 | ** | f | ||||
| Year since divorce2 | .005 | * | c | .005 | + | f | ||||
| Year since widowhood | −.325 | *** | c | −.320 | *** | f | ||||
| Year since widowhood2 | .018 | *** | c | .017 | *** | f | ||||
| Repartner after divorce | −.691 | *** | ||||||||
| Repartner after widowhood | −.918 | *** | ||||||||
| Year since repartner after divorce | .178 | * | ||||||||
| Year since repartner after divorce2 | −.011 | + | ||||||||
| Year since repartner after widowhood | .221 | *** | ||||||||
| Year since repartner after widowhood2 | −.016 | *** | ||||||||
| Household income | −.073 | *** | −.070 | *** | ||||||
| Variance components | ||||||||||
| Within-person | 1.538 | *** | 1.536 | *** | ||||||
| Initial status (1) | 1.654 | *** | 1.655 | *** | ||||||
| Rate of change (2) | .004 | *** | .004 | *** | ||||||
| Covariance between (1) and (2) | −.021 | *** | −.022 | *** | ||||||
| Log likelihood | −193246.061 | −193195.813 | ||||||||
p < .10
p < .05
p < .01
p < .001 (two-tailed tests)
The models also include eight dichotomous variables indicating at which wave the respondents were dropped out of the study.
Coefficients for the divorced and the widowed statistically differ at p < .05
The combined linear and the quadratic effects for the divorced and the widowed statistically differ at p < .05
To facilitate interpretation of the results, we also plotted the predicted depressive symptoms trajectories for the continuously married, those who got divorced, or became widowed by setting their transition to divorce or widowhood at year 6 and holding other covariates at their mean levels. As shown in Figure 1, it takes about 4 years (at year 10) for those who got divorced to recover to pre-dissolution levels of depressive symptoms. This pattern does not align with either the crisis or chronic strain models. Contrary to the crisis model, recovery takes a lot longer than a couple of years. But, individuals ultimately recover psychologically, which is at odds with the chronic strain model that stipulates persistent negative effects that do not diminish over time. For the widowed, it takes roughly 8 years (at year 14) for them to return to pre-dissolution levels of depressive symptoms. Again, this pattern is inconsistent with a temporary bereavement effect. It is important to note that even though the rate declined more quickly among the widowed than the divorced, it actually took the widowed longer than the divorced to achieve recovery to pre-dissolution levels of depressive symptoms.
Figure 1.
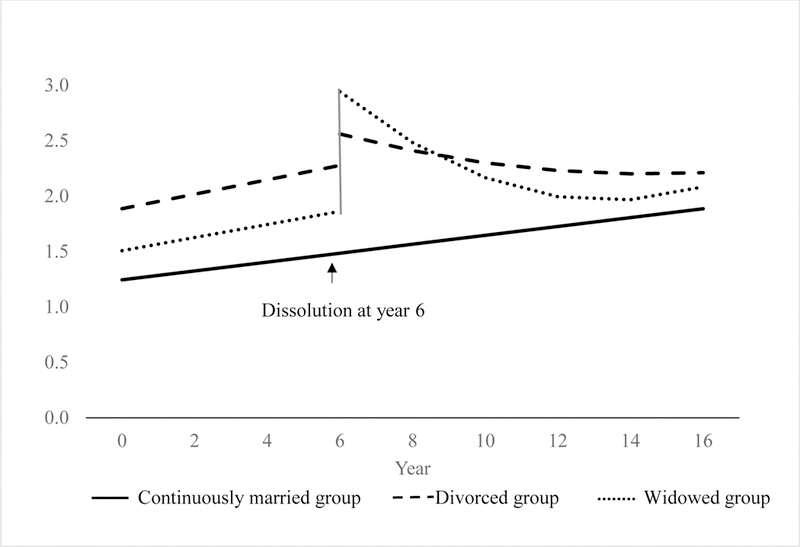
Predicted Depressive Symptoms Trajectories by Dissolution Type
Individuals who were in a higher-order marriage, younger, women, or minorities, those who had less education or lower incomes, and those who belonged to the HRS cohort reported higher depressive symptoms than their respective counterparts at baseline. The rate of increase in depressive symptoms was steeper for those who experienced a marital dissolution and who were older, men, or whites, relative to their respective counterparts.
In the last analysis, we considered whether the repartnering effect is a temporary honeymoon effect, whether gray divorcé(e)s reap greater (or lesser) benefits from repartnering than widow(er)s, and whether repartnering after marital dissolution offsets the negative consequences of divorce or widowhood for depressive symptoms. The estimates are presented in Model 2 of Table 2. The levels of depressive symptoms decreased abruptly immediately following repartnering for both those who got divorced and who became widowed by the same magnitude (−.691 versus −.918, p > .05). This beneficial effect of repartnering dissipated at the same rate for divorcé(e)s and widow(er)s as the level of depressive symptoms gradually increased over time after repartnering for both groups and then leveled off (.178 + [−.011] versus .221 + [−.016], p > .05). Together, these findings suggest that the beneficial effect of repartnering is also ultimately short-lived, consistent with the honeymoon effect.
Additionally, we found that the gain from repartnering is greater than the loss from divorce (|−.691| versus .352, p < .05), whereas the gain from repartnering and the loss from widowhood are similar in magnitude (|−.918| versus 1.097, p > .05). Finally, the associations of other covariates with depressive symptoms in Model 2 remained largely the same as those in Model 1.
We also plotted the predicted depressive symptoms trajectories for those who remained married, as well as those who got divorced or became widowed by fixing their transition to divorce or widowhood at year 6 and repartnering at year 10. As indicated in Figure 2, repartnering abruptly reduced divorcé(e)s’ depressive symptoms which converged to the level of the continuously-married, but their level of depressive symptoms gradually rose after repartnership. Likewise, repartnering swiftly decreased widow(er)s’ depressive symptoms to a level even lower than that of the continuously-married, but their level of depressive symptoms also steadily rose after repartnership. For both groups, the mental health benefits of repartnering attenuated in roughly six years.
Figure 2.
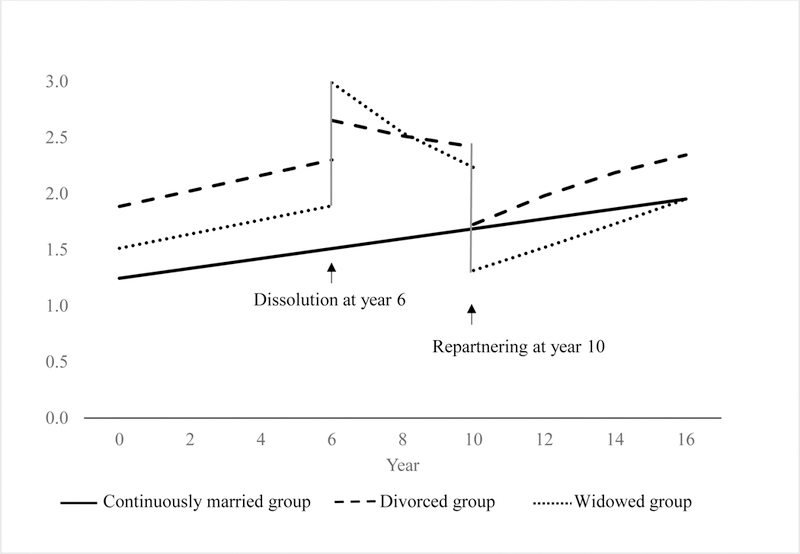
Predicted Depressive Symptoms Trajectories by Dissolution and Repartnering
We repeated the same procedure to estimate depressive symptoms trajectories for women and men separately and tested the magnitudes of elevations and slopes across gender. No significant gender differences were found (results not shown but available upon request).
DISCUSSION
For decades, scholars have retained their focus on widowhood and overlooked divorce in later life. The doubling of the gray divorce rate over the past 20 years underscores the urgency of studying the consequences of gray divorce and subsequent repartnering for older adult well-being. This study fills this critical gap by examining the depressive symptoms trajectories of a nationally representative sample of middle-aged and older adults who remained married, became widowed, or got divorced. We asked whether gray divorce is more (or less) detrimental than widowhood for mental health, whether repartnering is more (or less) beneficial for divorcé(e)s than for widow(er)s, and whether repartnering can offset the potentially negative consequences of later-life marital dissolution.
We found that those who got divorced or became widowed experienced higher levels of depressive symptoms leading up to the marital dissolution compared with those who remained married. This result mirrors earlier findings on depressive symptoms preceding earlier divorce or widowhood (Blekesaune 2008; Johnson and Wu 2002; Lee and DeMaris 2007; Wade and Pevalin 2004). It also suggests that prior studies that do not follow divorcé(e)s and widow(er)s before dissolution occurs likely overestimate the negative consequences of marital dissolution, because part of the association between marital dissolution and depressive symptoms is due to selection.
In contrast to conventional approaches to conceptualizing the effects of divorce on well-being, our findings do not align with either the crisis or the chronic strain models of divorce. According to the crisis model, the negative effects are temporary, with individual recovering to pre-divorce well-being levels within about two years after divorce. We found that individuals do recover after gray divorce, but it takes about four years, which is twice as long as expected based on the crisis model. This pattern also does not align with the chronic strain model, which posits indefinite negative effects from which there is no appreciable recovery. Although the negative effects of gray divorce persist for four years, ultimately individuals exhibit full recoveries. Thus, the pattern of findings we established satisfy only one of the two criteria of each of these divorce-adjustment models, suggesting that the pathway for older adults who experience gray divorce is unique.
We propose a new perspective for the gray divorce adjustment process: the convalescence model. Convalescence refers to a slow, gradual recovery from a weakened state which seems to accurately characterize the trajectories of psychological well-being following gray divorce. Kalmijn’s (2017) recent study of divorce and well-being showed it took individuals about five years to recover psychologically from divorce, a finding that is substantively similar to ours of four years. Nonetheless, it will be important for future research to consider this convalescence model to determine whether it applies to other domains of well-being for older adults who experience divorce.
The bereavement model was not supported by our findings either. Although individuals ultimately recovered from widowhood, the recovery was protracted, enduring for about eight years. This is considerably longer than the bereavement period of six months stated in the DSM but consistent with two prior studies using panel data that showed life satisfaction (Lucas et al. 2003) and depressive symptoms reverted to pre-widowhood levels in about eight years (Sasson and Umberson 2014). Arguably, the pattern we documented for widow(er)s aligns with the convalescence model we propose for gray divorce. It seems the convalescence model characterizes the adjustment process for adults in the second half of life regardless of whether marital dissolution occurs through gray divorce or widowhood.
Still, the depressive symptoms trajectories for older adults differed according to whether they experienced gray divorce or widowhood. Compared with those who became widowed, those who got divorced reported higher levels of depressive symptoms before their marital transition. Subsequently, they experienced a lower elevation immediately following divorce. Although the rate of recovery in depressive symptoms was slower for those who got divorced relative to those who became widowed, the length of time to recovery to the pre-dissolution level was shorter for the divorced than the widowed (4 versus 8 years according to Figure 1). This finding differs from the result in Wade and Pevalin’s study (2004) which showed that time to recovery was about the same for those who got divorced as those who became widowed. In short, our results suggest that the experience of gray divorce is less detrimental than the experience of widowhood for mental health.
Repartnering was equally beneficial for divorcé(e)s and widow(er)s as both groups experienced similar magnitudes of initial reduction and subsequent rates of increase in depressive symptoms, which is in concert with the finding from two cross-sectional studies (Barrett 2000; Hughes and Waite 2009). It took about six years for the initial gains from repartnering to diminish to pre-dissolution levels, reflecting the honeymoon effect documented in prior research (Kalmijn 2017). Repartnering after marital dissolution completely offsets the negative consequences of divorce or widowhood for depressive symptoms, contrary to our expectation. Consistent with several prior studies (Blekesaune 2008; Kalmijn 2017; Sasson and Umberson 2014; Strohschein et al. 2005), we did not find different depressive symptoms trajectories for women and men.
The study has some limitations. Depressive symptoms were measured at each interview, which occurred every two years in the HRS. Thus, we were unable to capture the immediate effect of dissolution for those who experienced it shortly after the interview. We combined remarriage and cohabitation as there are too few cohabitations to permit separate analyses for repartnering. Nevertheless, we expect remarriage and cohabitation to be equally beneficial for mental health as cohabitation operates as a substitute for remarriage among older adults (Brown et al. 2006; King and Scott 2005). A growing number of older adults are either dating or in a living-apart-together (LAT) arrangement that gives them the benefits of companionship without the hassle of sharing living quarters (Connidis, Borell, and Karlsson 2017; Langlais, Anderson, and Greene 2016). Unfortunately, the HRS does not collect any information on dating or LAT relationships. Whether these non-coresidential relationships offer the same mental health benefits as do remarriage and cohabitation is a topic that merits future study.
Despite these limitations, this study illustrates the importance of conceptualizing marital dissolution as a process (Amato 2000) and underscores the utility of using longitudinal data to follow individuals before, during, and after marital dissolution and repartnership. Using cross-sectional data or panel data of short duration cannot provide an accurate picture of how marital dissolution and repartnering relate to mental health nor can such an approach distinguish a crisis model and a chronic strain model. Our study spans a much longer time period (up to 16 years) than nearly all prior work on the consequences of marital dissolution and repartnering for individual well-being.
Notably, we uncover convincing evidence that existing models of adjustment to divorce and widowhood do not characterize the experiences of middle-aged and older adults. We reject both the crisis and chronic strain models of divorce, introducing a new model that we term the convalescence model, to describe the prolonged decline in depressive symptoms before eventual recovery to pre-dissolution levels. Likewise, we reject the bereavement model in favor of the convalescence model which more appropriately characterizes the extended adjustment process we documented for those who become widowed. The convalescence model offers a new perspective for understanding how adults in the second half of life respond following marital dissolution. Recent work using longitudinal data on divorce (Kalmijn 2017) and widowhood (Sasson and Umberson 2014) has documented nearly identical patterns of protracted decline followed by recovery, reinforcing our assertion that a new model is warranted. Of course, the convalescence model will require confirmation by other researchers and we hope future work will explicitly evaluate its applicability to the post-dissolution adjustment process particularly for adults aged 50 and older.
Our findings demonstrate the importance of widening the lens to encompass marital dissolutions that occur through either widowhood or gray divorce. Marital dissolution in middle age and older adulthood is a distinctive process that does not adhere to traditional models. Moreover, gray divorce has unique ramifications for psychological well-being that differ from widowhood. Even though both types of dissolution follow the novel convalescence model we advance, on balance, gray divorce is less detrimental than widowhood for mental health. The recovery time after gray divorce is about half as long as for widowhood. Following either gray divorce or widowhood, repartnering offers mental health benefits that attenuate after about six years. Future research should address how marital dissolution in the second half of life is related to other dimensions of well-being, such as economic security, physical health, and mortality, to assess whether the convalescence model we advanced for psychological well-being is more broadly applicable to post-dissolution adjustment across a range of outcomes for middle-aged and older adults.
Acknowledgements and Funding
An earlier version of this article was presented at the annual meeting of the Population Association of America, Denver, Colorado, April 2018. This research was supported by a grant to the first two authors from the National Institute on Aging (R15AG047588). Additional support was provided by the Center for Family and Demographic Research, Bowling Green State University, which has core funding from the Eunice Kennedy Shriver National Institute of Child Health and Human Development (P2CHD050959). Any opinions expressed here are solely those of the authors and not of the funding agency or center.
Author Bios
I-Fen Lin is professor of sociology at Bowling Green State University and a fellow of the Gerontological Society of America. Her research focuses on family change, dynamics, and functioning in later life, with attention to intergenerational transfer, caregiving, gray divorce, and reporting bias. She has published extensively in family and gerontology journals.
Susan L. Brown is distinguished research professor and chair of the Department of Sociology at Bowling Green State University. A family demographer, her research addresses the dynamics of intimate partnerships and their implications for well-being. She is the author of Families in America (University of California Press, 2017).
Matthew R. Wright is assistant professor of sociology at Arkansas State University. His research explores family change among older adults and its implications for well-being, with a focus on intimate partnerships, cohabitation, and gray divorce. He has published in family and gerontology journals.
Anna M. Hammermsith is assistant professor of sociology at Grand Valley State University. Her research explores union dissolution and repartnership in later life, paying close attention to aging parent’s relationships with their adult children. Her previous work can be found in other social science and gerontological journals.
Footnotes
Endnote
Of the 19,828 respondents, 27% died before the end of the study (2014), comprising 33% of the respondents who become widowed, 27% of the respondents who were continuously married, and 15% of the respondents who got divorced. Although the widowed were more likely to die than the other two groups, the widowed contributed more waves of information (6.8) to the study than the continuously married (5.0 waves) and the divorced (5.6 waves). After marital dissolution, the average number of follow-up wave was similar between divorcé(e)s (3.4 waves) and widow(er)s (3.3 waves). Additionally, the models included the effects of baseline age on both the initial status and the rate of change in depressive symptoms, as well as a study dropout indicator for each follow-up wave. Thus, the different patterns of depressive symptoms following divorce and widowhood observed in this study are unlikely attributable to the differential mortality rates of divorcé(e)s versus widow(er)s.
Contributor Information
I-Fen Lin, Department of Sociology, Bowling Green State University, Bowling Green, OH, USA.
Susan L. Brown, Department of Sociology, Bowling Green State University, Bowling Green, OH, USA
Matthew R. Wright, Department of Criminology, Sociology, & Geography, Arkansas State University, Jonesboro, AR, USA
Anna M. Hammersmith, Department of Sociology, Grand Valley State University, Allendale, MI, USA
References
- Amato Paul R. 2000. “The Consequences of Divorce for Adults and Children.” Journal of Marriage and the Family 62(4):1269–87. [Google Scholar]
- Amato Paul R. 2010. “Research on Divorce: Continuing Trends and New Developments.” Journal of Marriage and Family 72(3):650–66. [Google Scholar]
- Bair Deirdre. 2007. Calling It Quits: Late-Life Divorce and Starting Over New York: Random House. [Google Scholar]
- Barrett Anne E. 2000. “Marital Trajectories and Mental Health.” Journal of Health and Social Behavior 41(4):451–64. [PubMed] [Google Scholar]
- Blekesaune Morten. 2008. “Partnership Transitions and Mental Distress: Investigating Temporal Order.” Journal of Marriage and Family 70(4):879–90. [Google Scholar]
- Brimhall Andrew, Wampler Karen, and Kimball Thomas. 2008. “Learning from the Past, Altering the Future: A Tentative Theory of the Effect of Past Relationships on Couples Who Remarry.” Family Process 47(3):373–87. [DOI] [PubMed] [Google Scholar]
- Brown Susan L., Lee Gary R., and Bulanda Jennifer Roebuck. 2006. “Cohabitation Among Older Adults: A National Portrait.” The Journals of Gerontology, Series B: Psychological Sciences and Social Sciences 61(2):S71–S79. [DOI] [PubMed] [Google Scholar]
- Brown Susan L., Bulanda Jennifer Roebuck, and Lee Gary R.. 2012. “Transitions Into and Out of Cohabitation in Later Life.” Journal of Marriage and Family 74(4):774–93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brown Susan L. and Lin I-Fen. 2012. “The Gray Divorce Revolution: Rising Divorce Among Middle-Aged and Older Adults, 1990–2010.” The Journals of Gerontology, Series B: Psychological Sciences and Social Sciences 67(6):731–41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brown Susan L., Lin I-Fen, Hammersmith Anna M., and Wright Matthew R.. 2018. “Later Life Marital Dissolution and Repartnership Status: A National Portrait.” The Journals of Gerontology, Series B: Psychological Sciences and Social Sciences 73(6):1032–42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carr Deborah. 2004. “The Desire to Date and Remarry Among Older Widows and Widowers.” Journal of Marriage and Family 66(4):1051–68. [Google Scholar]
- Carr Deborah and Pudrovska Tetyana. 2012. “Divorce and Widowhood in Later Life.” Pp. 489–513 in Handbook of Families and Aging, 2nd ed., edited by Blieszner R and Bedford VH. Santa Barbara, CA: Praeger. [Google Scholar]
- Connidis Ingrid Arnet, Borell Klas, and Karlsson Sofie Ghazanfareeon. 2017. “Ambivalence and Living Apart Together in Later Life: A Critical Research Proposal.” Journal of Marriage and Family 79(5):1404–18. [Google Scholar]
- Dykstra Pearl A. and Gierveld Jenny de Jong. 2004. “Gender and Marital-History Differences in Emotional and Social Loneliness among Dutch Older Adults.” Canadian Journal on Aging 23(2):141–55. [DOI] [PubMed] [Google Scholar]
- Heeringa Steven G., West Brady T., and Berglund Patricia A.. 2017. Applied Survey Data Analysis 2nd ed. Boca Raton, FL: Chapman and Hall/CRC. [Google Scholar]
- Hetherington E. Mavis and Kelly John. 2002. For Better or For Worse: Divorce Reconsidered New York: W. W. Norton & Company. [Google Scholar]
- Hughes Mary Elizabeth and Waite Linda J.. 2009. “Marital Biography and Health at Mid-Life.” Journal of Health and Social Behavior 50(3):344–58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnson David R. and Wu Jian. 2002. “An Empirical Test of Crisis, Social Selection, and Role Explanations of the Relationship Between Marital Disruption and Psychological Distress: A Pooled Time-Series Analysis of Four-Wave Panel Data.” Journal of Marriage and Family 64(1):211–24. [Google Scholar]
- Kalmijn Matthijs. 2007. “Gender Differences in the Effects of Divorce, Widowhood and Remarriage on Intergenerational Support: Does Marriage Protect Fathers? Social Forces 85(3):1079–104. [Google Scholar]
- Kalmijn Matthijs. 2017. “The Ambiguous Link between Marriage and Health: A Dynamic Reanalysis of Loss and Gain Effects.” Social Forces 95(4):1607–36. [Google Scholar]
- Kennedy Sheela and Ruggles Steven. 2014. “Breaking Up Is Hard to Count: The Rise of Divorce in the United States, 1980–2010.” Demography 51(2):587–98. [DOI] [PMC free article] [PubMed] [Google Scholar]
- King Valarie and Scott Mindy E.. 2005. “A Comparison of Cohabiting Relationships Among Older and Younger Adults.” Journal of Marriage and Family 67(2):271–85. [Google Scholar]
- Langlais Michael R., Anderson Edward R., and Greene Shannon M.. 2016. “Consequences of Dating for Post-divorce Maternal Well-being.” Journal of Marriage and Family 78(4):1032–46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee Gary R. and DeMaris Alfred. 2007. “Widowhood, Gender, and Depression: A Longitudinal Analysis.” Research on Aging 29(1):56–72. [Google Scholar]
- Lin I-Fen, Brown Susan L., and Hammersmith Anna M.. 2017. “Marital Biography, Social Security Receipt, and Poverty.” Research on Aging 39(1):86–110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lin I-Fen, Brown Susan L., Wright Matthew R., and Hammersmith Anna M.. 2018. “Antecedents of Gray Divorce: A Life Course Perspective.” The Journals of Gerontology, Series B: Psychological Sciences and Social Sciences 73(6):1022–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lorenz Frederick O., Wickrama KAS, Conger Rand D., and Elder Glen H. Jr. 2006. “The Short-Term and Decade-Long Effects of Divorce on Women’s Midlife Health.” Journal of Health and Social Behavior 47(2):111–25. [DOI] [PubMed] [Google Scholar]
- Lucas Richard E., Clark Andrew E., Georgellis Yannis, and Diener Ed. 2003. “Reexamining Adaptation and the Set Point Model of Happiness: Reactions to Changes in Marital Status.” Journal of Personality and Social Psychology 84(3):527–39. [DOI] [PubMed] [Google Scholar]
- Muthén Bengt, Asparouhov Tihomir, Hunter Aimee M., and Leuchter Andrew F.. 2011. “Growth Modeling With Nonignorable Dropout: Alternative Analyses of the STAR*D Antidepressant Trial.” Psychological Methods 16(1):17–33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ofstedal Mary Beth, Weir David R., Chen Kuang-Tsung, and Wagner James. 2011. Updates to HRS Sample Weights (HRS Report No. DR-013). Retrieved April 10, 2018 (http://hrsonline.isr.umich.edu/sitedocs/userg/dr-013.pdf).
- Radloff Lenore Sawyer. 1977. “The CES-D Scale: A Self-Report Depression Scale for Research in the General Population.” Applied Psychological Measurement 1(3):385–401. [Google Scholar]
- Sasson Isaac and Umberson Debra J.. 2014. “Widowhood and Depression: New Light on Gender Differences, Selection, and Psychological Adjustment.” The Journals of Gerontology, Series B: Psychological Sciences and Social Sciences 69(1):135–45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schimmele Christoph M. and Wu Zheng. 2016. “Repartnering After Union Dissolution in Later Life.” Journal of Marriage and Family 78(4):1013–31. [Google Scholar]
- Simon Robin W. 2002. “Revisiting the Relationships among Gender, Marital Status, and Mental Health.” American Journal of Sociology 107(4):1065–96. [DOI] [PubMed] [Google Scholar]
- Singer Judith D. and Willett John B.. 2003. Applied Longitudinal Data Analysis: Modeling Change and Event Occurrence New York: Oxford University Press. [Google Scholar]
- Stroebe Wolfgang, Stroebe Margaret, Abakoumkin Georgios, and Schut Henk. 1996. “The Role of Loneliness and Social Support in Adjustment to Loss: A Test of Attachment Versus Stress Theory.” Journal of Personality and Social Psychology 70(6):1241–49. [DOI] [PubMed] [Google Scholar]
- Strohschein Lisa, Peggy McDonough Georges Monette, and Shao Qing. 2005. “Marital Transitions and Mental Health: Are There Gender Differences in The Short-Term Effects of Marital Status Change?” Social Science & Medicine 61(11):2293–303. [DOI] [PubMed] [Google Scholar]
- Sullivan Allison R. and Fenelon Andrew. 2014. “Patterns of Widowhood Mortality.” The Journals of Gerontology, Series B: Psychological Sciences and Social Sciences 69(1):53–62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sweeney Megan M. 2010. “Remarriage and Stepfamilies: Strategic Sites for Family Scholarship in the 21st Century.” Journal of Marriage and Family 72(3):667–84. [Google Scholar]
- Turvey Carolyn L., Wallace Robert B., and Herzog Regula. 1999. “A Revised CES-D Measure of Depressive Symptoms and a DSM-Based Measure of Major Depressive Episodes in the Elderly.” International Psychogeriatrics 11(2):139–48. [DOI] [PubMed] [Google Scholar]
- Umberson Debra, and Montez Jennifer Karas. 2010. “Social Relationships and Health: A Flashpoint for Health Policy.” Journal of Health and Social Behavior 51:S54–S66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Umberson Debra, Thomeer Mieke Beth, and Williams Kristi. 2013. “Family Status and Mental Health: Recent Advances and Future Directions.” Pp. 405–31 in Handbook of the Sociology of Mental Health, edited by Aneshensel CS, Phelan JC, and Bierman A. New York: Springer. [Google Scholar]
- Vespa Jonathan. 2012. “Union Formation in Later Life: Economic Determinants of Cohabitation and Remarriage Among Older Adults.” Demography 49(3):1103–25. [DOI] [PubMed] [Google Scholar]
- Wade Terrance J. and Pevalin David J.. 2004. “Marital Transitions and Mental Health.” Journal of Health and Social Behavior 45(2):155–70. [DOI] [PubMed] [Google Scholar]
- Wallerstein Judith S., Lewis Julia M., and Blakeslee Sandra. 2000. The Unexpected Legacy of Divorce: A 25 Year Landmark Study New York: Hyperion. [Google Scholar]
- Wilcox Sara, Evenson Kelly R., Aragaki Aaron, Sylvia Wassertheil-Smoller Charles P. Mouton, and Loevinger Barbara Lee. 2003. “The Effects of Widowhood on Physical and Mental Health, Health Behaviors, and Health Outcomes: The Women’s Health Initiative.” Health Psychology 22(5):513–22. [DOI] [PubMed] [Google Scholar]
- Williams Kristi. 2003. “Has the Future of Marriage Arrived? A Contemporary Examination of Gender, Marriage, and Psychological Well-Being.” Journal of Health and Social Behavior 44(4):470–87. [PMC free article] [PubMed] [Google Scholar]