

Abstract
We report a case of injury of the medial bucket handle meniscal tears (BH), which resolved spontaneously, in association with anterior cruciate ligament (ACL) injury. The patient twisted his left knee during a fight in martial arts, progressing to pain and joint locking and a sense of distortion. In NMR it could be seen bucket-handle tear of the medial meniscus with displacement of the fragment to the intercondylar region, rupture of the lateral meniscus and ACL tear. After conservative treatment and physiotherapy, in an interval of one year, later examinations showed that there was spontaneous healing of AB.
Keywords: Anterior cruciate ligament injury bucket handle, Spontaneous resolution of bucket handle, Knee injury in trauma sports
Introduction
Meniscal lesions can occur separately or in association with bone or ligament injuries. One of the less frequent meniscal lesions is the bucket handle tear, which consists of a vertical or oblique tear that extends longitudinally, with medial displacement of the fragment, usually from the central part of the meniscus. The incidence of this condition ranges from 9% to 24% of the cases. Bucket handle tears have great clinical importance, since displacement of the fragment from the meniscus may cause joint locking, thus requiring surgical treatment. In the literature, there is only one description of a bucket handle tear with spontaneous resolution, but without any association with the anterior cruciate ligament (ACL). The diagnosis is made with the aid of NMR. The incidence of meniscal lesions in patients with ACL instability has been described in the literature as ranging from 35% to 97%. It is seen that 82% of the patients present associated meniscal lesions, and it is believed that the length of time between the initial injury and the reconstruction surgery is the main factor contributing towards this high rate of association.[1], [2], [3], [4]
The ACL acts as a mechanical stabilizer, thereby restricting anteriorization and rotation of the tibia in relation to the femur. Its main function is to prevent anterior displacement of the tibia in relation to the femur, in the mechanism for internal and external rotation, and to restrict valgus and varus stress. Functionally, the greatest vulnerability of the ACL occurs in rotational mechanisms, given that 70% of ACL tears are related to this mechanism. The incidence of ACL injury is 0.24 cases per 1,000 healthy individuals per year. Tearing of the ligament results from maximum overload, despite its resistance, especially during sports activities. It usually limits or impedes sports practice; nonetheless, depending on the patient's response to the injury, it may not have any influence on the patient's previous sports activites.[5], [6]
Case report
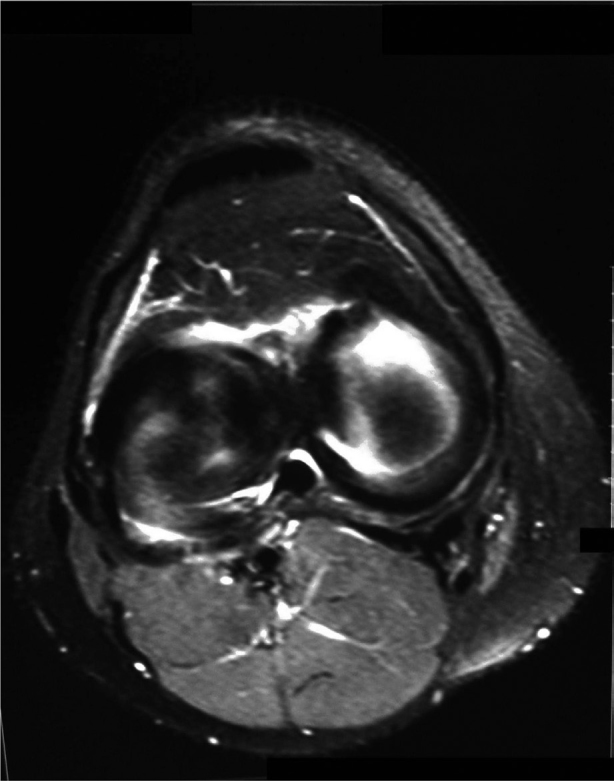
The patient (NNR) was a 17-year-old male (85 kg; 1.75 cm; mixed skin color). His complaint was that a year and a half earlier he had twisted his right knee when placing his leg on the floor during a karate match, without direct trauma. He developed pain and edema immediately after the trauma, with intensely incapacitating medial pain in the right knee. He used NSAIDs until the pain improved, with cold compresses on the site. One week later, he returned to karate training, doing only part of the activities, because he then presented joint instability, with uncertainty in flexing the joint on his own weight. He also presented difficulty in rotating the knee and in squatting, with a feeling that the joint had “gone out of its place”. He presented improvement of the pain after stretching the joint, whenever there was this sensation of pain followed by instability and subluxation of the joint. On clinical examination, the patient presented medial pain on mobilization, locking in extension at 45°, a positive anterior drawer sign (grade III), a positive Lachman test (grade III) and subluxation with crackling in the pivot shift test. NMR showed a bucket handle tear of the medial meniscus, with displacement of the fragment into the intercondylar region, tearing of the lateral meniscus, joint effusion, grade II femoropatellar chondropathy and ACL tearing (Fig. 1, Fig. 2).
Fig. 1.

NMR on the right knee, showing the bucket handle tear in a longitudinal slice.
Fig. 2.
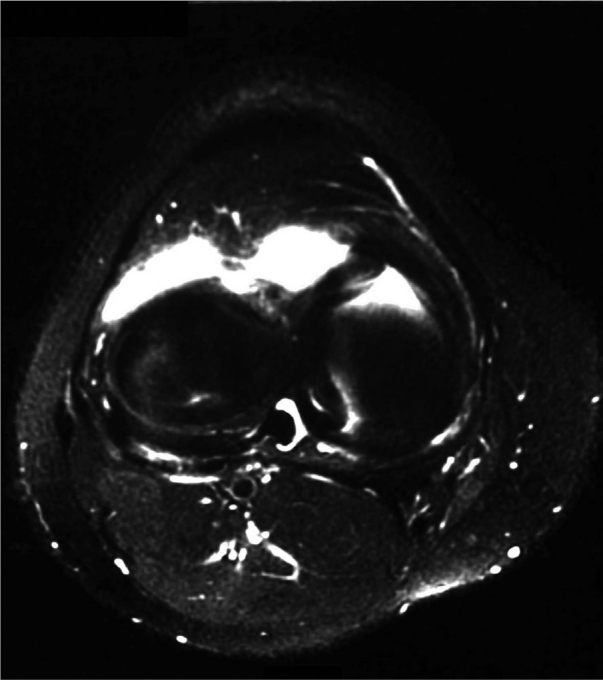
NMR on the right knee, showing the bucket handle tear in a transverse slice.
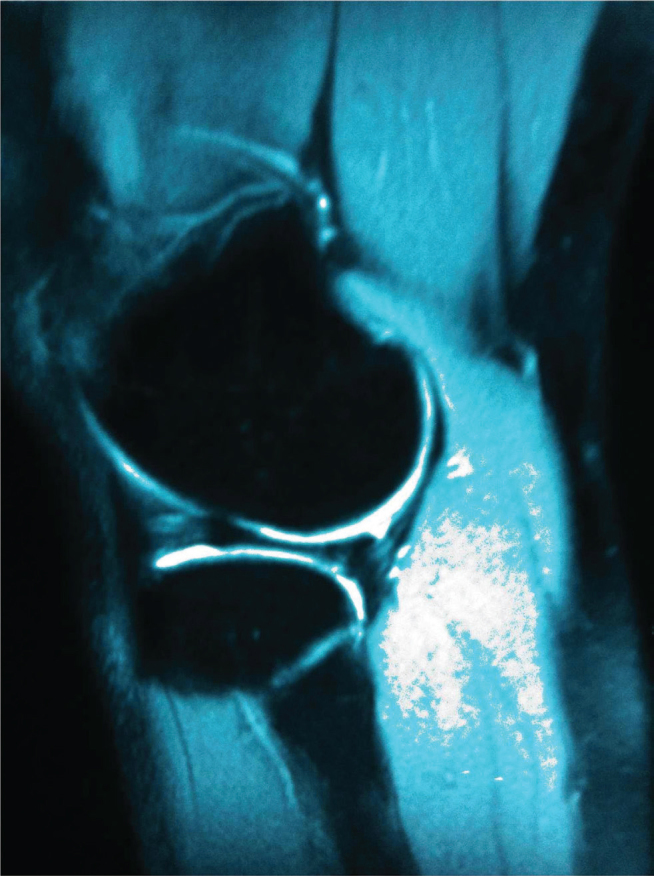
The orthopedic surgeon decided to perform ligament reconstruction by means of the tendon of the semitendinosus muscle, using arthroscopy, with restoration of the meniscus. However, the patient opted to undergo conservative treatment with regard to muscle strengthening through proprioceptive exercises, with strengthening of the extensor musculature and impact-free aerobic exercises such as swimming and cycling. Over one-year period, the patient gave up his karate training and dedicated himself solely to the rehabilitation and doing an educational course on sports habits. During this period, he repeated the NMR examination on his right knee, which presented slight signal abnormalities, with irregularity of the outlines of the lower surface of the lateral meniscus. This was thought to be related to an old tear, a radial tear at the root of the posterior body of the medial meniscus, complete tearing at the origin of the ACL and slight trochlear chondroplasty. Over this one-year period, the bucket handle tear completely regenerated, although a healed ACL tear remained, without impairing the patient's daily activities after restructuring of his sports habits. He did not present any joint pain or locking, but only some instability due to the old tearing of the ACL (Fig. 3, Fig. 4).
Fig. 3.
NMR on the right knee, one year after conservative treatment, with spontaneous resolution of the bucket handle tear seen in a longitudinal slice.
Fig. 4.
NMR on the right knee, one year after conservative treatment, with spontaneous resolution of the bucket handle tear seen in a transverse slice.
Discussion
Bucket handle tears of the medial meniscus are three to six times more common than similar tears in the lateral meniscus. These tears effectively reduce the width of the meniscus, and peripheral sagittal images do not demonstrate the normal bow-tie configuration of the meniscal body. The sensitivity of NMR for diagnosing bucket handle tears, if one or more of the four signs described is observed, is up to 97%, i.e. comparable with arthroscopy. It ranges from 27% to 44% for the posterior double cruciate sign, from 33% to 40% for the anterior double cornu sign, from 60% to 94% for the fragment displaced to the intercondylar incisure, and from 71% to 97% for absence of the bow-tie configuration. Identification of the displaced meniscal fragment is very important for surgical treatment, and this can be done via arthroscopy or conventional means. Bucket handle tears are often associated with ACL injuries (10% to 60%). Meniscal lesions are the biggest cause of knee locking in clinical practice. The differential diagnosis includes, among other conditions, cruciate ligament tears, cysts in the cruciate ligaments, intra-articular free bodies (osteochondritis dissecans, acute osteochondral lesions, synovial osteochondromatosis and penetrating injuries), pigmented nodular synovitis and plica syndrome.[1], [2], [7], [8], [9]
Functionally, two groups of individuals with ACL injuries can be identified. The first presents clinical symptoms such as edema, pain and instability during knee movements, with difficulty in performing some activities of daily living. For individuals in this group, surgical reconstruction of the ACL is often recommended. On the other hand, there is a group of individuals presenting ACL injuries but without reporting clinical symptoms such as edema and pain. The individuals in this group are able to perform motor tasks involving the knee joint, without any apparent functional deficit, and are considered to have adapted to the lesion.5
It is believed that a lack of proprioceptive information originating from the ACL causes static and dynamic alterations, along with two distinct responses. Firstly, there is an inhibitory reflex in the quadriceps, thereby diminishing the mass of this musculature, which is also observed clinically. This inhibition also diminishes the capacity of the quadriceps to generate extensor torque, which provokes excessive anteriorization of the tibia. Secondly, this facilitates activation of the hamstrings, which promotes strengthening of this musculature. Chronic ACL injury generates isometric weakness of the musculature, which performs internal rotation or strengthening of the external rotators, thereby increasing the activity of the vastus lateralis and biceps femoris during gait. Ligament injury in a knee may also interfere with the functionality of the contralateral limb, due to the complex circuitry, and activate a polysynaptic route in the contralateral neurons. In a general manner, individuals with ACL injuries present increased hip and knee flexion angles during gait.5
There is a need for proprioceptive reeducation of the knee, also known as sensory-motor reeducation. This aims to develop and/or improve the joint protection by means of conditioning and reflexive training. Exercises with special imbalance stimuli have been adapted to be performed in a closed kinetic chain, in which there is always a concentration on the quadriceps and hamstrings, thereby minimizing the anterior translation of the tibia and providing synchronism for hip, knee and ankle movements. We have also introduced exercises with variable resistance into the method, using rubber tubes and elastic bands, in order to seek a greater response regarding strength and muscle mass. The method also favors high-level sports players by adding special training with advanced proprioception and muscle explosion exercises, known as plyometric exercises. The length of time for applying the method is three months, with variation according to the patient's condition.10
In the present study, the case of a patient who had a bucket handle tear of the medial meniscus on NMR, with ACL tearing, is described. After the clinical treatment, a control examination showed that the tear had spontaneously resolved, since the meniscal fragment could no longer be seen and the meniscus was of normal volume, in relation to the previous examination. The patient only presented a slight signal irregularity in the posterior cornu. Therefore, this spontaneous resolution occurred without surgical intervention, even though an ACL lesion was still present, without impairing the patient's day-to-day joint movements and impact-free sports activities, and without flexing the knee for squat movements. As shown on the control NMR examination, we conclude that spontaneous resolution of the lesion occurred.
Conflicts of interest
The authors declare that there was no conflict of interests in conducting this study.
Footnotes
Work performed at the Orthopedics Service of Paracatu Atenas School, Paracatu, MG, Brazil.
References
- 1.Vianna E.M., Mattos A.C., Domingues R.C., Marchiori E. Resolução espontânea de lesão em alça de balde do menisco medial: relato de caso e revisão da literatura. Radiol Bras. 2004;37(3):219–221. [Google Scholar]
- 2.Helms C.A., Laorr A., Cannon W.D., Jr. The absent bow tie sign in bucket-handlle tears of the menisci in the knee. AJR Am J Roentgenol. 1998;170(1):57–61. doi: 10.2214/ajr.170.1.9423600. [DOI] [PubMed] [Google Scholar]
- 3.Wright D.H., De Smet A.A., Noris M. Bucket-handle tears of the medial and lateral me-nisci of the knee: value of MR imaging in detecting displaced fragments. AJR Am J Roentgenol. 1995;165(3):621–625. doi: 10.2214/ajr.165.3.7645481. [DOI] [PubMed] [Google Scholar]
- 4.Singson R.D., Feldman F., Staron R., Kierman H. MR imaging of displaced bucket-handle tear of the medial meniscus. AJR Am J Roentgenol. 1991;156(1):121–124. doi: 10.2214/ajr.156.1.1898544. [DOI] [PubMed] [Google Scholar]
- 5.Fatarelli I.F., Almeida G.L., Nascimento B.G. Lesão e reconstrução do LCA: uma revisão biomecânica e do controle motor. Rev Bras Fisioter. 2004;8(3):197–206. [Google Scholar]
- 6.Rezende U.M., Camanho G.L., Hernandez A.J. Alteração da atividade esportiva nas instabilidades crônicas do joelho. Rev Bras Ortop. 1993;28(10):725–730. [Google Scholar]
- 7.Karam F.C., Silva J.L.B., Fridman M.W., Abreu A., Arbo R.M., Abreu M. A ressonância magnética para o diagnóstico das lesões condrais, meniscais e dos ligamentos cruzados do joelho. Radiol Bras. 2007;40(3):179–182. [Google Scholar]
- 8.Brammer H., Sover E., Erickson S., Stone J. Simultaneous identification of medial and lateral buckethandle tears: the Jack and Jill lesion. AJR Am J Roentgenol. 1999;173(3):860–861. doi: 10.2214/ajr.173.3.10470967. [DOI] [PubMed] [Google Scholar]
- 9.McAllister D.R., Motamedi A.R. Spontaneous healing of a bucket-handle lateral meniscal tear in an anterior cruciate ligament-deficient knee. A case report. Am J Sports Med. 2001;29(5):660–662. doi: 10.1177/03635465010290052201. [DOI] [PubMed] [Google Scholar]
- 10.Sampaio T.C., Souza J.M.G. Reeducação proprioceptiva nas lesões do ligamento cruzado anterior do joelho. Rev Bras Ortop. 1994;29(5):303–309. [Google Scholar]