

Abstract
Though appendicitis is the most common cause of acute abdomen, the vermiform appendix as a cause of small bowel obstruction is a rarity. The inflamed appendix can cause obstruction by making a knot around the small bowel. There are only few case reports on Appendico-ileal knotting (AIK). We have not found any report on AIK causing small bowel obstruction during pregnancy. The diagnosis of acute abdomen in pregnancy is difficult due to the accompanying anatomic and physiologic changes. Because obstruction due to AIK present like any other cause of obstruction diagnosing the condition pre-operatively is uncommon. Here, we report 30 years old Gravida 9, Para 8 women who presented with cardinal symptoms of small bowel obstruction at term and found to have AIK intra-operatively. The challenge of difficulty in making the diagnosis and management options are discussed
INTRODUCTION
Intestinal obstruction is among the three most common surgical emergencies seen in pregnancy. The causes of small bowel obstruction (SBO) in pregnancy includes volvulus, adhesions, hernias, intestinal knots etc. [1]. The incidence of small bowel obstruction ranges from 1:1 500–1:16 000 pregnancies [1].
Intestinal knot are well-recognized causes of bowel obstruction. The most common form of intestinal knots is the ileo-sigmoid knotting (ISK) which causes closed loop obstruction of both the small bowel and the colon. Ileo-ileal knotting can occur too [2]. But, all forms of intestinal knots are extremely rare during pregnancy. In AIK the distal ileum is entrapped by knot of the appendix which encircles the distal ileum resulting closed-loop obstruction [1, 3–5]. The vermiform appendix or an inflamed appendix as a cause of intestinal obstruction in pregnancy is exceedingly rare that we didn’t find a report in literature.
Presentation of SBO from AIK is similar to other causes with no specific sign or symptoms. Due to this and rarity of the condition pre-operative diagnosis is uncommon and diagnosis is almost always intra-operative surprise. Here, we report 30 years old Gravida 9, Para 8 women who presented with cardinal symptoms of small bowel obstruction at term. AIK was identified as the cause of the obstruction during laparotomy. The challenge of difficulty in making the diagnosis and management options are discussed.
THE CASE
A 30-years old Gravida 9 (gestational age of 32 weeks), Para 8 mother presented with vomiting, abdominal pain and distension of 4 days. She failed to pass feces and flatus during those four days. She didn’t have pushing down pain, vaginal bleeding, and history of abdominal trauma or surgery.
On examination she was acutely sick looking. Blood pressure (180/120mmg), pulse rate (96 beat per minute) and respiratory rates (32breath per minute) were high but temperature (36.5°C) was normal. Abdomen was protuberant with a 30 weeks sized gravid uterus. Fetal heart beat was positive. She had mild epigastric and upper abdomen tenderness. Per vaginal examination revealed a closed cervix while rectum was empty on digital rectal examination. The rest of the physical examination was unremarkable.
On investigations she had Leucocytosis (15 400) with left shift, mild anemia (hemoglobin= 11 g/dl), hypokalemia (potassium = 2.2 mmol/l) and protein-uria (+3). Renal and liver function tests were normal. The abdominal Ultrasound and x-ray showed evidence of SBO.
Patient was admitted with a diagnosis of third trimester pregnancy with severe pre-eclamsia, SBO secondary to small bowel volvulus (SBV) and hypokalemia. In preparation for emergency laparotomy she was resuscitated and started on management.
A midline laparotomy was performed. The intra-operative findings were intact 30 weeks sized gravid uterus, an inflamed appendix encircling the distal ileum (30 cm from the ileo-cecal valve). The tip of the appendix was adherent to the posterior peritoneum medial to the cecum. (Fig. 1). A lower uterine segment cesarean section was done. An alive male neonate weighing 1.8 kg with an APGAR score of 7 and 8 at the first and fifth minutes delivered. After uterus was closed, the appendix tip was gently released from the peritoneum which freed the ileum (Fig. 2). Appendectomy completed the operation. The baby treated in neonatal intensive care unit. Post-operatively, patient had an uneventful recovery and discharged on the fifth day after operation. In the first three post operative months the patient and the infants were in good health.
Figure 1:
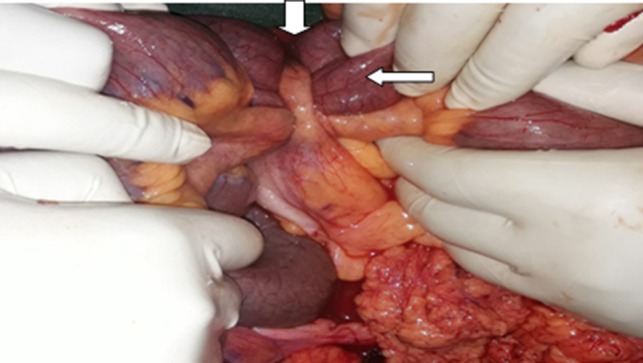
Intra-operative picture, Note the appendix (down arrow) making a knot around the distal ileum (side arrow).
Figure 2:
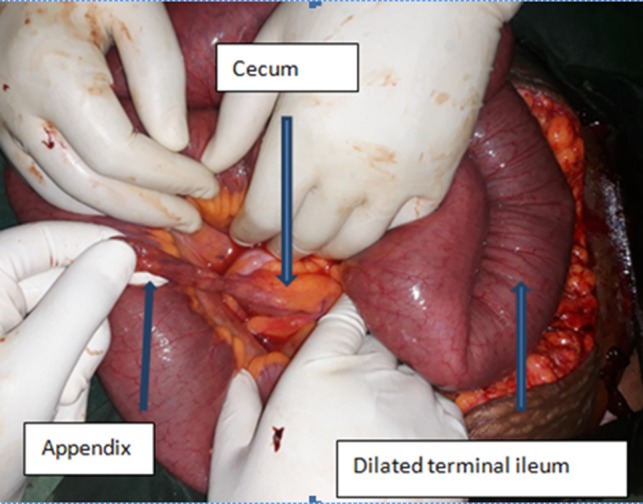
A display of loops of bowel and the vermiform appendix after release of obstruction.
DISCUSSION
Acute appendicitis, acute cholecystitis and SBO are the top three non obstetric causes of acute abdomen during pregnancy. SBO during pregnancy is uncommon and occurs usually in the second trimester of pregnancy and rarely in the third trimester [1]. The occurrence of both appendicitis and small bowel obstruction during pregnancy is an extremely rare phenomenon.
When the appendix causes obstruction, it mostly occurs as a result of complication of the acute appendicitis in the form of ileus (secondary to peri-appendiceal inflammation or as part of generalized peritonitis) or trapped in an appendiceal mass [6]. The appendix can also cause obstruction by forming a knot with the ileum(AIK) [5].
Pre-operative diagnosis of AIK is very difficult and quite challenging. Like in our patient, most cases of SBO secondary to AIK are intra-op diagnosis [5]. If there is no obvious cause of obstruction, small bowel volvulus (SBV) is the primary diagnosis in areas where it is common. This was also the consideration in our patient. The reason why misdiagnosis of AIK is common is related to the rarity of the condition and accompanied paucity of knowledge and experience. For this reason delay in diagnosis and intervention are not uncommon [4, 5, 7, 8].
Imaging studies including abdominal X-ray and ultrasound will confirm the presence of SBO but unlikely to diagnose AIK. Abdominal CT in a prepared mind might help in a pre-operative diagnosis of AIK by showing evidence of acute appendicitis and SBO signs [8]. CT should be avoided in pregnant mothers when obstruction is diagnosed and laparotomy decided.
Laparoscopy has been found to be a safe approach for acute appendicitis and acute cholecystitis during pregnancy but it applicability for obstruction is not clear [1]. In our opinion open surgery with long midline access is a better option, because it gives adequate access to the whole abdomen and pelvis. In the third trimester of pregnancy and there is indication to terminate the pregnancy open surgery is the only option. During surgery, priority should be for the cesarean section and intestinal surgery or appendectomy should be delayed until the uterus is closed.
Obstruction caused by AIK is relieved by releasing the appendix from the posterior peritoneum. If the bowel is viable appendectomy completes the operation. However, when there is gangrenous change, resection and anastomosis of the bowel or right hemi-colectomy need to need be done [4, 5, 7–9].
For all non obstetric acute abdomens in addition to meticulous clinical and imaging evaluation, a high index of suspicion is an important tool in early diagnosis and management of pregnant mothers. When there is no obvious cause, keeping AIK in the differential diagnosis of SBO in a pregnant mothers or the general public is a prudent idea. This avoids delay in intervention and potential morbidity and mortality.
CONFLICT OF INTEREST STATEMENT
None declared.
REFERENCES
- 1. Augustin G, Majerovic M. Non-obstetrical acute abdomen during pregnancy. Eur J Obstet Gynecol Reprod Biol 2007;131:4–12. 10.1016/j.ejogrb.2006.07.052. [DOI] [PubMed] [Google Scholar]
- 2. Cakir M, Tekin A, Kucukkartallar T, Kartal A. Ileosigmoidal knotting, an unusual form of acute intestinal obstruction. Acute Med Surg 2015;2:234–6. 10.1002/ams2.108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Thanapal M, Um MS, Ariffin Z, Ukm AMS. Rare complication of appendix: small bowel gangrene caused by the appendicular knot. Med J Malaysia 2017;72:370–1. [PubMed] [Google Scholar]
- 4. Report C, Report TAC. Clinics in surgery strangulated intestinal obstruction due to appendiceal. Clin Surg 2017;2:5–7. [Google Scholar]
- 5. Malý O, Páral J. Appendicitis as a rare cause of mechanical small-bowel obstruction: a literature review of case reports. Int J Surg Case Rep 2016;29:180–4. 10.1016/j.ijscr.2016.10.065. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Lj AH, Ea A. Intes Tinal Obs Truction Caused by Appendicitis: As Ys Tematic Review Occl Usion Intes Tinale Cause P Ar L’ Appendicite: Une Revue S Ys. J West African Coll Surg 2017;7:94–115. [Google Scholar]
- 7. Al-Qallaf A, Shuaib A, Al-Sharaf K, Behbehani A. Acute appendicitis as a rare cause of mechanical small bowel obstruction case report. Qatar Med J 2017;2017:2–5. 10.5339/qmj.2017.4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Small P, Harrison S, Boobis L, Mahawar K, Brown D. Acute appendicitis presenting as small bowel obstruction: two case reports. Cases J. 2009;2:4–7. 10.1186/1757-1626-2-9106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Soo CT, Tsegha LJ. Appendicular knot causing closed-loop obstruction, volvulus and strangulation of ileum in a 9-year-old: a case report. Ann Pediatr Surg 2016;12:111–4. 10.1097/01.XPS.0000481349.36594.66. [DOI] [Google Scholar]