

Abstract
Objective
To minimize the occurrence of missed injuries, the tertiary evaluation was introduced consisting of reassessment of the patient, 24 hours after admission, with: complete history, physical examination, review of exams and diagnostic testing if necessary.
Methods
Observational study evaluating trauma patients admitted to a teaching hospital in São Paulo, according to a protocol for tertiary evaluation.
Results
Between February and May 2012, for 12 weeks, 182 patients were submitted to tertiary evaluation, 100 (55%) polytraumatized and 82 (45%) were victims of low-energy trauma. Neglected lesions were observed in 21 (11.5%) patients, who had 28 missed injuries. Of these 28 lesions, seven (25%) required surgical treatment.
Conclusion
Strategies including formal tertiary evaluation, the protocol applied for assessing trauma victims, seem to be beneficial in these patients, regardless of the mechanism of trauma. The method is easily applied, effective and has low cost in identifying missed injuries in the victims of trauma.
Keywords: Evaluation, Multiple trauma, Trauma severity indices
Resumo
Objetivo
Com o intuito de minimizar a ocorrência de lesões despercebidas, foi introduzida a avaliação terciária, que consiste na reavaliação do paciente, 24 horas após sua internação, com: anamnese completa, exame físico detalhado, revisão dos exames subsidiários e complementação diagnóstica se houver necessidade.
Métodos
Estudo observacional que avaliou pacientes vítimas de trauma internados em hospital escola na cidade de São Paulo, guiado por protocolo para avaliação terciária.
Resultados
Entre fevereiro e maio de 2012, durante 12 semanas, foram submetidos à avaliação terciária 182 pacientes vítimas de trauma, 100 (55%) politraumatizados e 82 (45%) vítimas de trauma de baixa energia. As lesões negligenciadas foram observadas em 21 (11,5%) pacientes, que apresentavam 28 lesões despercebidas. Dessas 28 lesões, sete (25%) necessitaram de tratamento cirúrgico.
Conclusão
Estratégias que incluem avaliação terciária formal, aplicada nas vítimas de trauma, sugerem ser benéficas aos pacientes, independentemente do mecanismo de trauma. É método de execução fácil, custo financeiro barato e efetivo na identificação de lesões negligenciadas nas vítimas de trauma.
Palavras-chave: Avaliação, Índices de gravidade do trauma, Traumatismo múltiplo
1. Introduction
In attending trauma patients, regardless of whether a high or low- energy mechanism was involved, the initial approach can follow the steps recommended in the Advanced Trauma Life Support (ATLS) protocol, which was drawn up by the American College of Surgeons. This covers both primary and secondary assessments.1, 2 However, another group of patients who are brought to emergency services end up undergoing physical examination guided only by their own complaints. The initial attendance may neglect secondary information that patients themselves describe or possibly fail to comment about. Thus, injuries may go unnoticed and aggregate morbidity that determines these patients’ prognosis.
With the aim of minimizing the occurrences of these unnoticed injuries, tertiary assessment was introduced.3 This consists of reassessing the patient, 24 hours after hospitalization, with the following purposes: taking a complete history, performing a detailed physical examination, reviewing the subsidiary tests and doing additional diagnostic testing, if necessary. Thus, the attendance for trauma victims reaches a higher level of complexity, such that the initial phase consists of primary assessment in either a pre-hospital or a hospital environment, the secondary assessment is in the emergency room and the tertiary assessment takes place with the patient hospitalized in the ward.
Because of the impossibility of obtaining data of greater precision regarding the conditions and other situations at the time of the trauma and the impossibility of achieving greater collaboration from the patient in the initial assessment that would enable complete diagnosis of traumatic injuries, we proposed to use a protocol for tertiary assessment based on detailed history-taking and complete physical examination, following the logical sequence. This proposal for tertiary assessment improves patients’ prognoses through identifying visceral, neurological and tendon injuries, fractures and bruising that remain unnoticed in the primary and/or secondary assessments.
2. Methods
An observational study assessing trauma patients in a teaching hospital in the city of São Paulo, 24 hours after hospitalization, was conducted in accordance with the protocol proposed for tertiary assessment. Patients who were unconscious or under sedation were reassessed after regaining consciousness.
Over the 12-week period between February and May 2012, 182 patients hospitalized in the Central Hospital with a diagnosis of at least injury to the musculoskeletal system requiring surgical treatment were evaluated. Individuals with pathological factures of any etiology were excluded, and it was stipulated that the patients needed to have been hospitalized for less than 24 hours.
The assessments were made by one of the three third-year resident physicians under training at the service, who are authors of this study. The resident physician indicated had not participated in the initial assessment and/or the secondary assessment at the time of the patient's hospitalization. The protocol devised for carrying out the study (Annex 1) included obtaining identification data, history-taking, standardized and systematized physical examination, the date and time of the reassessment and the need for complementary examinations and additional clinical evaluations, in cases of unconscious or intubated patients. Seeking reasons for possible diagnostic failures was mandatory.
Upon applying the protocol, we also obtained the following parameters: sex, age, schooling level, body mass index, trauma mechanism, time of hospital admission, initial diagnosis and the date and time of reassessment. After diagnosing any injuries that had been ignored, the need for additional intervention was assessed and the reasons why the injury had been neglected were identified.
The categorical variables were expressed as absolute and percentage values, and the continuous variable were expressed as means and standard deviations.
3. Results
Over the 12-week period between February and May 2012, 182 consecutive trauma patients underwent tertiary assessment, among whom 100 (55%) had suffered multiple trauma and 82 (45%) were victims of trauma that was considered to be low-energy. For 51 patients (30.2%), an emergency surgical approach was needed; 64 (35.2%) presented associated head- brain trauma; and one (0.5%) died.
The patients baseline demographic characteristics are expressed in Table 1. Among the patients studied, 124 (68.1%) were male; the mean age was 41.2 ± 19.2 years; 86 (48.3%) were of mixed skin color, 69 (38%) were white, 24 (13.2%) were black and three (1.6%) were oriental; the mean body mass index (BMI) was 25.5 ± 4.4 kg/m2; the mean number of years of schooling was 8.5 ± 4 years; 88 patients (48.4%) presented upper-limb injuries; 99 (54.4%) presented lower-limb injuries); three (1.6%) had facial fractures; eight (4.4%) had spinal fractures; five (2.7%) had pelvic ring fractures; and 109 patients (65.5%) were admitted between the hours of 6:00 and 18:00, and were thus considered to be daytime patients. The unconscious or sedated patients were reassessed after they regained consciousness. All the patients were hospitalized under the care of the orthopedics team alone or in conjunction with other teams of the hospital.
Table 1.
Demographic characteristics of the patients hospitalized.
| Observational data | Value | Percentage of total number of patients | Interval |
|---|---|---|---|
| Patients | 182 | 100 | |
| Male | 124 | 68 | |
| Age in years | 41.2 | ± 19.2 | |
| BMI in kg/m2 | 25.5 | ± 4.4 | |
| Schooling in years | 8.5 | ± 4 | |
| Upper-limb injuries | 88 | 48.3 | |
| Lower-limb injuries | 99 | 54.4 | |
| Spinal injuries | 8 | 4.4 | |
| Pelvic ring injuries | 5 | 2.7 | |
| Facial fractures | 3 | 1.6 | |
| Time of admission between 6:00 and 18:00 | 119 | 65.5 |
BMI, body mass index; kg, kilogram; m2, square meter, min, minutes; n, number of patients studied.
Neglected injuries were observed in 21 patients (11.5%), who presented 28 unnoticed injuries, as described in Table 2 and identified in the protocol. Upper-limb neglected injuries (Fig. 1) were identified in three patients (14.3%) patients, which corresponded to four injuries (14.3%). Eight patients (38.1%) presented lower-limb injuries corresponding to 14 injuries (50%). Six patients (28.6%) had chest injuries, two (9.5%) had facial injuries and three (14.3%) had spinal injuries. Among these 28 injuries, seven patients (25%) received nonsurgical treatment consisting of immobilization, oral medication for the symptoms and local care.
Table 2.
Distribution of undiagnosed injuries according to body segment.
| Segment | Patients = 21 | Injuries = 28 |
|---|---|---|
| Upper limbs | 3 | 4 – acromioclavicular dislocation Clavicle fracture (2) |
| Fracture of distal third of radius | ||
| Lower limbs | 8 | 13 – Fracture of femoral condyle 4 fractures of right metatarsal and 5 fractures of left toes |
| Fracture of fibular neck (2) | ||
| Fracture of lateral tibial plateau | ||
| Knee instability (2) | ||
| Fracture of calcaneus (2) | ||
| Fracture of intermediate wedge | ||
| Injury of common fibular nerve | ||
| Fracture of ischiopubic ramus | ||
| Chest | 5 | 6 – Fractures of costal arches |
| Face | 2 | 2 – Fracture of mandible |
| Fracture of orbit | ||
| Spine | 3 | 3 – Fracture of L2, L4 and L5 |
Frat, fratura; L2, segunda vértebra lombar; L4, quarta vértebra lombar; L5, quinta vértebra lombar; LAC, luxação acromioclavicular; MMII, membros inferiores; MMSS, membros superiores; MTTD, metatarso direito; n, nervo; PDE, pododáctilo esquerdo.
Figure 1.
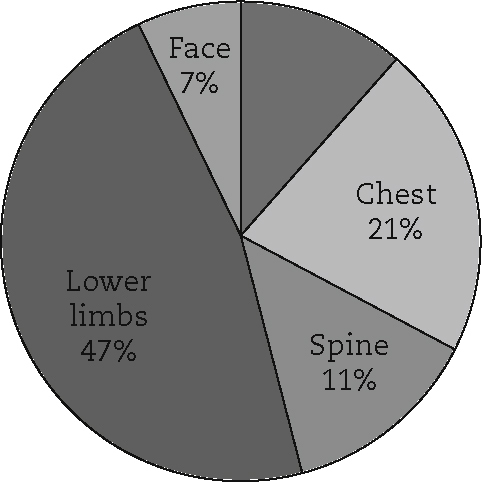
Graphical expression of the undiagnosed injuries according to body segment (UL, upper limbs; LL, lower limbs).
For 16 (76.2%) of the patients with diagnostic failure, this was correlated with inadequate initial assessment, and for five (23.8%) with failure of communication with the patient.
4. Discussion
This assessment method was shown to be safe and effective for aiding in diagnosing neglected injuries. In addition, evidence suggests that in centers characterized by high demand from trauma patients, this action would minimize the negative impact caused by injuries that remain undiagnosed when attending to these patients.4 Undiagnosed injuries that are clinically significant may culminate in complications, increased morbidity and even death.
Studies on undiagnosed injuries have reported incidences of between 0.6% and 65%, depending on the method used.5, 6 The lack of standardized prospective studies makes it difficult to identify the real incidence of these lesions in trauma patients.7 We observed that the neglected injuries included diagnoses that were missed both in clinical examinations and in radiographic imaging. This observation suggests that the practice of tertiary assessment is valuable for achieving early diagnosis of neglected injuries. This makes it possible to infer that improvement of the quality of clinical examinations in the assessments that these patients undergo and evaluation of the imaging examinations by specialists would give rise to a higher rate of clinical suspicion of neglected injuries.
Our study demonstrated that undiagnosed injuries occurred in patients who were victims of both high and low-lowenergy trauma, i.e. going from those who suffered twisted ankle injuries to those who suffered motorcycle accidents. Although such injuries occurred in greater numbers in patients presenting higher-energy mechanisms, the results were not statistically significant. In our sample, victims of high-energy accidents predominated, which was coherent with the data in the literature researched.2, 3, 4, 5, 6, 7, 8, 9 We can affirm that the relevance of our results lies in the number of neglected injuries encountered, of which one third required surgical treatment.
The initial attendance, through the primary assessment (either before hospitalization or at the hospital) and the secondary assessment, has the fundamental aim of treating injuries that threaten the patient's life. In seeking to make a complete clinical assessment in order to establish the diagnoses for trauma victims, it needs to be borne in mind that systematical reviews for these patients will be required, and that the first appropriate time for this to take place is during the hospitalization. The importance of searching for neglected injuries at services attending trauma patients needs to be highlighted.
It has been suggested that, regardless of the trauma mechanism, such patients would benefit from strategies that include formal tertiary assessment applied to trauma victims, with standardized and systematized clinical examinations and reviewing of the subsidiary tests.3, 4, 5, 8 In our sample, we were able to diagnose neglected injuries in 21 patients (11.5%), without added morbidity. This is an easily applied, inexpensive and effective method. It was not possible to define the degree of accuracy of the method.
5. Limitations of the study
This study had the following limitations: its observational nature; the small number of patients included; the fact that it was conducted in a single center; and the lack of patient follow-up later on, when it would have been possible to check on whether any injuries had been neglected in the tertiary assessment.
6. Conclusions
The protocol for tertiary assessment was shown to be effective for identifying neglected injuries among trauma victims.
Conflicts of interest
The authors declare no conflicts of interest.
Footnotes
Work performed in the Department of Orthopedics and Traumatology, Irmandade da Santa Casa de Misericórdia de São Paulo, São Paulo, SP, Brazil.
References
- 1.Alexander R.H., Proctor H.J. American College of Surgeons; Chicago: 1993. Advanced trauma life support student manual. [Google Scholar]
- 2.Soundappan S.V., Holland A.J., Cass D.T. Role of an extended tertiary survey in detecting missed injuries in children. J Trauma. 2004;57(1):114–118. doi: 10.1097/01.ta.0000108992.51091.f7. [DOI] [PubMed] [Google Scholar]
- 3.Enderson B.L., Reath D.B., Meadors J., Dallas W., DeBoo J.M., Maull K.I. The tertiary trauma survey: a prospective study of missed injury. J Trauma. 1990;30(6):666–669. [PubMed] [Google Scholar]
- 4.Hodgson N.F., Stewart T.C., Girotti M.J. Autopsies and death certification in deaths due to blunt trauma: what are we missing? Can J Surg. 2000;43(2):130–136. [PMC free article] [PubMed] [Google Scholar]
- 5.Janjua K.J., Sugrue M., Deane S.A. Prospective evaluation of early missed injuries and the role of tertiary trauma survey. J Trauma. 1998;44(6):1000–1006. doi: 10.1097/00005373-199806000-00012. [DOI] [PubMed] [Google Scholar]
- 6.Kremli M.K. Missed musculoskeletal injuries in a University Hospital in Riyadh: types of missed injuries and responsible factors. Injury. 1996;27(7):503–506. doi: 10.1016/0020-1383(96)00044-7. [DOI] [PubMed] [Google Scholar]
- 7.Buduhan G., McRitchie D.I. Missed injuries in patients with multiple trauma. J Trauma. 2000;49:600–605. doi: 10.1097/00005373-200010000-00005. [DOI] [PubMed] [Google Scholar]
- 8.Houshian S., Larsen M.S., Holm C. Missed injuries in a level I trauma center. J Trauma. 2002;52(4):715–719. doi: 10.1097/00005373-200204000-00018. [DOI] [PubMed] [Google Scholar]
- 9.Vles W.J., Veen E.J., Roukema J.A., Meeuwis J.D., Leenen L.P. Consequences of delayed diagnoses in trauma patients: a prospective study. J Am Coll Surg. 2003;197(4):596–602. doi: 10.1016/S1072-7515(03)00601-X. [DOI] [PubMed] [Google Scholar]