

Abstract
Objective
The objective of this study is to evaluate the results and effectiveness of the technique of meniscal repair type all-inside using Fast-Fix device.
Methods
A retrospective cohort study evaluating 22 patients with meniscal surgery between January 2004 and December 2010 underwent meniscal repair technique for all-inside with the Fast-Fix device with or without ACL reconstruction. Function and quality of life outcomes were chosen by the IKDC and Lysholm score, before and postoperatively, and reoperation rates, relying to the time of final follow-up. Statistical analysis was performed using the Student's t test.
Results
The mean follow-up was 59 months (16–84). The Lysholm score showed 72% (16 patients) of excellent and good results (84–100 points), 27% (6 patients) fair (65–83 points) and no cases classified as poor (<64 points). According to the IKDC: 81% (18 patients) of excellent and good results (75–100 points), 18% of cases regular (50–75 points) and no patient had poor results (<50 points). There were no failures or complications.
Conclusion
The technique of meniscal repair type all-inside using the Fast-Fix device is safe and effective for the treatment of meniscal lesions in the red zone or red-white with or without simultaneous ACL reconstruction, with good and excellent results in most patients Level 4 Study.
Keywords: Arthroscopy, Menisci tibial, Suture techniques
Resumo
Objetivo
Avaliar os resultados e a eficácia da técnica de reparo meniscal tipo all-inside com o uso do dispositivo FasT-Fix.
Métodos
Estudo de coorte retrospectivo com avaliação de 22 pacientes com lesão meniscal operados entre janeiro de 2004 e dezembro de 2010, submetidos ao reparo meniscal pela técnica all-inside com o dispositivo FasT-Fix e associados ou não à reconstrução do LCA. Função e qualidade de vida foram os desfechos escolhidos por meio dos questionários de Lysholm e IKDC, pré e pós-operatoriamente, além das taxas de reoperação, relevando-se o tempo de seguimento final. A análise estatística foi feita com o uso do teste t de Student.
Resultados
O tempo médio de seguimento foi de 59 meses (16–84). O escore de Lysholm apresentou 73% (16 pacientes) de excelentes e bons resultados (84–100 pontos), 27% (seis pacientes) regulares (65–83 pontos) e nenhum caso classificado como ruim (<64 pontos). Segundo o IKDC: 82% (18 pacientes) de excelentes e bons resultados (75–100 pontos); 18% de casos regulares (50–75 pontos) e nenhum paciente obteve resultados ruins (<50 pontos). Não ocorreram falhas ou complicações.
Conclusão
A técnica de reparo meniscal tipo all-inside com o uso do dispositivo FasT-Fix, nos pacientes avaliados, se mostrou eficaz e segura para o tratamento das lesões de menisco na zona vermelha ou zona vermelho-branca associada ou não à reconstrução simultânea do LCA e apresentou resultados bons e excelentes na maioria dos pacientes.
Palavras-chave: Artroscopia, Meniscos tibiais, Técnicas de sutura
Introduction
The menisci are fibrocartilaginous structure in the knee that perform important functions such as load absorption1 and transmission,2 synovial fluid distribution and lubrication,3 improvement of femorotibial joint congruence,4 stabilization5 and protection of the joint cartilage when subjected to axial loads.1, 4, 5 Absence of the menisci is associated with joint instability and to increased cartilage degeneration.6, 7 Therefore, meniscal repair should be preferable to meniscectomy, whenever feasible.5, 8
Meniscal sutures have already been performed for more than a century. They were first described and performed as open procedures by Annandale, in 1883, and Katzenstein, in 1908. Since then, a variety of techniques for performing meniscal sutures have been put forward, and these have evolved from sutures performed as open procedures to arthroscopic repair techniques of inside-out, outside-in and all-inside types.
Since the classic study on vascularization of the menisci conducted by Arnoczky and Warren9 in 1982, which demonstrated the possibility of achieving meniscal healing, arthroscopic techniques and particularly those of all-inside type have gained widespread use among physicians.
The all-inside arthroscopic suturing technique presents the advantage of not requiring secondary safety incisions for performing meniscal sutures, which diminishes the morbidity of the procedure.10, 11 This technique presents less difficulty, a low complication rate and results similar to those from the classical suturing techniques.11, 12, 13
The objective of this study was to evaluate the results and effectiveness of the all-inside meniscal repair technique, using the Fast-Fix device (Smith & Nephew, Andover, MA, USA), which was the precursor of the fourth generation of meniscal suturing.
Material and method
In a retrospective cohort study, 22 patients with meniscal injuries who underwent meniscal repair using the all-inside technique with the Fast-Fix device with or without anterior cruciate ligament (ACL) reconstruction (using the flexor tendons) between January 2004 and December 2010 were evaluated. All the procedures were performed by the same surgeon (LJBA). Out of the 22 patients, 16 underwent simultaneous reconstruction of the ACL and six underwent arthroscopic suturing of a meniscal injury alone.
The patients were evaluated through applying the Lysholm questionnaire14 and that of the International Knee Documentation Committee (IKDC).15 Evaluations were made before and after the operation, with a minimum of 16 months of postoperative evaluation until the time of the final follow-up.
The inclusion criteria were that the injuries should be unstable longitudinal peripheral injuries of the meniscus, located in the red-red or red-white zones,9 which were 10 mm or more in length, and that the patients should answer the assessment questionnaires completely. Patients with concomitant ACL injury or failure underwent reconstruction of this ligament using flexor tendons, during the same surgical procedure.
The exclusion criteria were that there should not be an Outerbridge grade 3 or 4 chondral lesion in the same compartment; meniscal injuries with hybrid treatment, i.e. in which the meniscus was partially sutured and partially resected; and meniscal injuries that were sutured using repair techniques other than all-inside with the Fast-Fix device. In addition, patients who did not answer the questionnaires completely or who were lost from the follow-up were excluded, as were those whose meniscal injuries were “unrepairable” (in the white zone, complex, radial or horizontal), osteoarthritic patients and those with inflammatory diseases.
The surgical technique consisted firstly of stimulating the borders of the meniscal injury by abrading them with a shaver or specific rasps, and subsequently drilling the most external portion of the meniscus using a Jelco no. 14, with the aim of creating channels for the vascular access. These two procedures are very important, because they facilitate and stimulate healing of the menisci. The meniscal suture in the true sense began with introduction of the Fast-Fix device into the knee within its protective sleeve. For sutures of the body of the meniscus, the anterior portal of the compartment opposite to that of the injured meniscus was used. On the other hand, for suturing injuries to the posterior cornu of the meniscus, the anterior portal of the same compartment was used. The Fast-Fix device was introduced into the meniscus twice, so as to cross meniscal injury horizontally, vertically or obliquely, according to the morphology of the injury. In this manner, the meniscus was advanced as far as the joint capsule such that two anchors could grip the meniscus around the capsule, thus stabilizing it. The device was then removed from the knee and the knot, which had been pre-assembled, was tensioned by means of a “knot-pulling” device, which also served for cutting the excess thread (Fig. 1, Fig. 2, Fig. 3, Fig. 4).
Fig. 1.
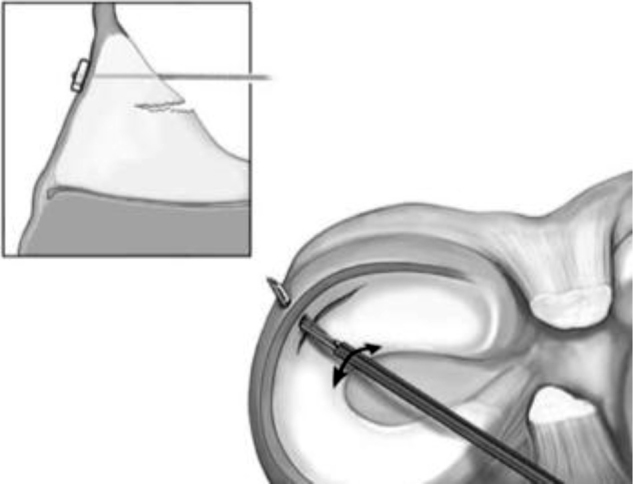
Insertion of the first implant, with the needle starting in the external portion of the meniscus and crossing the capsule.
Fig. 2.
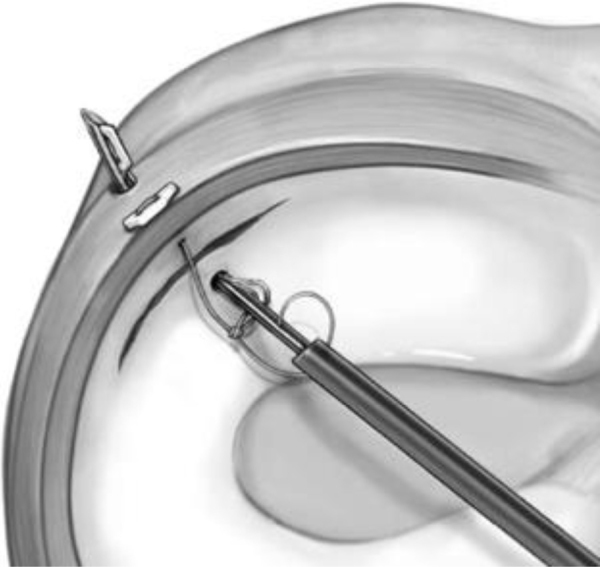
Insertion of the second implant, with the needle entering the internal portion of the meniscus and crossing the capsule.
Fig. 3.
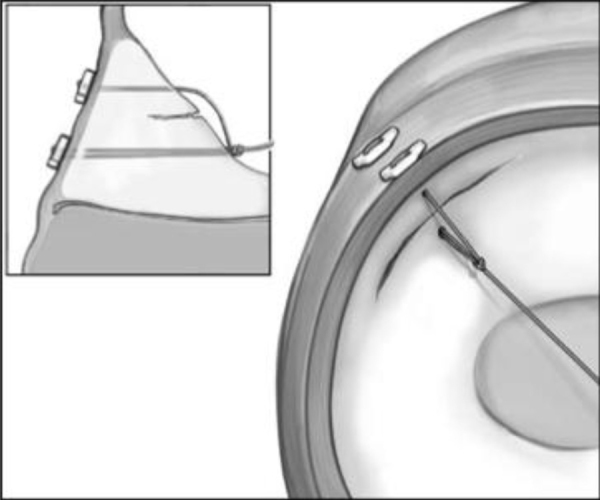
The two implants now positioned after the capsule and the knot pre-assembled on the thread, with the needle already withdrawn from the joint.
Fig. 4.

Tensioning of the suture, using a “knot pusher”, which served for cutting the thread later on.
After the operation, the patients remained without weight-bearing for six weeks, followed by another two weeks of partial weight-bearing. Thus, they were released from using crutches after eight weeks. Flexion was restricted to 90 degrees during the first four weeks and was then progressively allowed to increase. The same protocol was used for the patients with both ACL reconstruction and meniscal repair. The patients were allowed to return to sports activity when the operated limb had recovered at least 70% of its extensor mechanism strength, in relation to the contralateral limb. However, this was never less than six months after the operation.
Failure of the procedure was defined as the need for a new surgical procedure (partial meniscectomy), the presence of mechanical symptoms (such as joint blockage) or poor results according to the questionnaires (Lysholm score < 64 or IKDC score < 50).
The statistical analysis was done using Student's t test, irrespective of statistical significance. A relationship between age and/or time elapsed after the operation and the functional result was sought.
Results
The data resulting from the individual questionnaires answered by each patient are shown in Table 1.
Table 1.
Full sample.
| Patient | Sex | Age | Time elapsed since operation (months) | Lysholm before operation | Lysholm after operation | IKDC before operation | IKDC after operation |
|---|---|---|---|---|---|---|---|
| ABF | ♂ | 21 | 26 | 60 | 100 | 49.4 | 92 |
| AM | ♂ | 39 | 55 | 48 | 76 | 46 | 78.2 |
| AMA | ♀ | 39 | 52 | 55 | 79 | 50.6 | 62.1 |
| AN | ♂ | 28 | 77 | 50 | 72 | 44.8 | 73.6 |
| BG | ♀ | 21 | 69 | 33 | 91 | 26.4 | 87 |
| CSC | ♂ | 50 | 75 | 48 | 95 | 36.8 | 80.5 |
| ED | ♂ | 44 | 47 | 82 | 100 | 69 | 97.7 |
| FF | ♂ | 32 | 74 | 50 | 100 | 42.5 | 100 |
| FFS | ♂ | 40 | 54 | 43 | 90 | 28.7 | 73.6 |
| FKIM | ♂ | 28 | 65 | 63 | 95 | 59.8 | 81.6 |
| GL | ♂ | 32 | 53 | 40 | 94 | 35.6 | 90.8 |
| GR | ♂ | 24 | 53 | 70 | 100 | 58.6 | 100 |
| LF | ♀ | 19 | 16 | 48 | 81 | 49.4 | 78.2 |
| LHSL | ♂ | 41 | 63 | 62 | 70 | 57.5 | 78.2 |
| RC | ♂ | 35 | 55 | 11 | 91 | 5.7 | 89.7 |
| RCR | ♂ | 30 | 84 | 100 | 100 | 100 | 100 |
| RLJL | ♂ | 21 | 72 | 86 | 84 | 87.4 | 71.3 |
| RN | ♂ | 38 | 52 | 42 | 100 | 28.7 | 94.3 |
| RV | ♂ | 28 | 66 | 45 | 75 | 29.9 | 93.1 |
| SJS | ♂ | 39 | 62 | 56 | 86 | 37.9 | 94.3 |
| TSM | ♂ | 29 | 60 | 52 | 100 | 48.3 | 100 |
| TW | ♂ | 25 | 69 | 84 | 100 | 70.1 | 98.9 |
Twenty-two patients who underwent all-inside meniscal suturing were evaluated with regard to the results from the Lysholm and IKDC scales and reoperation rate, as presented in the table for the total sample. The mean length of follow-up was 59 months (16–84).
In the Lysholm scale, the results are considered to be excellent/good when the score is between 84 and 100 points; fair results have scores between 65 and 83; and poor results are those with scores of 64 or less. Among our results, 73% (16 patients) had excellent or good Lysholm scores, 27% (six patients) had fair scores and none of the patients had poor results (score < 64).
In turn, in the IKDC, results are considered to be excellent/good when the score is 75 points or over; fair results have scores between 50 and 74; and the results are taken to be poor when the scores do not reach 50 points. According to this scale, 82% of the cases (18 patients) were considered to have excellent results, 18% were fair and none were poor.
The Kolmogorov–Smirnov test was used to determine whether the scale scores presented normal distribution. This assumption was satisfied for both scales (p > 0.05). The paired Student's t test was used to compare the scales from before to after the operation, as shown in Table 2.
Table 2.
Evaluation of the questionnaires before and after the operation.
| Variable | Mean | SD | N | p |
|---|---|---|---|---|
| Lysholm before | 55.82 | 19.72 | 22 | <0.001 |
| Lysholm after | 89.95 | 10.39 | 22 | |
| IKDC before | 48.32 | 21.03 | 22 | <0.001 |
| IKDC after | 87.05 | 11.24 | 22 |
SD, standard deviation; N, sample; p, statistical significance.
There was a statistically significant improvement in the scale scores in comparing function from before to after the operation (p < 0.05).
Neither age nor time elapsed since the operation showed any statistically significant correlation with improvement on the functional scales (p > 0.05). There was only a statistically significant correlation between the improvements on the scales, i.e. the greater the improvement observed on the Lysholm scale was, the greater the improvement on the IKDC scale also was (r = 0.877 and p < 0.001), as shown in Table 3.
Table 3.
Correlation between the questionnaires, age and time elapsed after operation.
| Correlation | Age | Time elapsed after operation (months) | Change on Lysholm |
|---|---|---|---|
| Time elapsed after operation (months) | |||
| r | 0.178 | ||
| p | 0.428 | ||
| N | 22 | ||
| Lysholm score | |||
| r | 0.108 | −0.232 | |
| p | 0.631 | 0.298 | |
| N | 22 | 22 | |
| IKDC score | |||
| r | 0.142 | −0.155 | 0.877 |
| p | 0.530 | 0.490 | <0.001 |
| N | 22 | 22 | 22 |
r, relational strength; N, number of patients in the sample; p, statistical significance.
The absolute and relative changes in the Lysholm and IKDC scales were compared between the group that underwent simultaneous reconstruction of the ACL (73%) and the group that only underwent meniscal suturing (27%). The results suggested that there was a greater change between the pre and postoperative assessments in the group with simultaneous ACL reconstruction, but without statistical significance (Table 4).
Table 4.
Evaluation of meniscal suturing performed simultaneously with ACL reconstruction.
| Variable | ACL |
||||||
|---|---|---|---|---|---|---|---|
| Without reconstruction |
With reconstruction |
p |
|||||
| Mean | SD | N | Mean | SD | N | ||
| Lysholm before | 67.7 | 21.6 | 6 | 51.4 | 17.7 | 16 | |
| Lysholm after | 93.3 | 10.6 | 6 | 88.7 | 10.4 | 16 | |
| Change in Lysholm (after-before) | 25.7 | 22.5 | 6 | 37.3 | 19.0 | 16 | 0.236 |
| Change in Lysholm % (after-before)/before | 48.5 | 43.9 | 6 | 114.5 | 169.9 | 16 | 0.366 |
| IKDC before | 63.8 | 24.1 | 6 | 42.5 | 17.1 | 16 | |
| IKDC after | 91.6 | 13.2 | 6 | 85.4 | 10.4 | 16 | |
| Change in IKDC (after-before) | 27.8 | 29.5 | 6 | 42.8 | 20.0 | 16 | 0.182 |
| Change in IKDC % (after-before/before | 60.8 | 59.7 | 6 | 194.3 | 348.7 | 16 | 0.369 |
The mean change on both scales was statistically equal for patients with and without ACL reconstruction (p > 0.05).
SD, standard deviation; N, sample; p, statistical significance.
No need for new surgery (for partial meniscectomy), or any presence of mechanical symptoms such as joint blockage, was observed in any of the patients evaluated, after the operation.
There were no neurovascular complications or any implant migration in any of the patients evaluated.
Discussion
Suturing of the meniscus was introduced with the aim of preserving this tissue, so as to prevent the deleterious alterations resulting from its resection, even if done only partially. Such alterations have an effect in relation both to degeneration and to instability of the knee. Although meniscal repair presents a higher reoperation rate, it has better long-term results than partial meniscectomy.6, 7, 16
At the beginning of the development of meniscal suturing techniques, the first generation was based on the inside-out procedure of Henning.17 This was followed by the second generation of outside-in procedures, which was introduced by Warren18 with the aim of diminishing the risk of fibular nerve injury in lateral meniscal repairs. Also focusing on preventing neurovascular injury, the all-inside meniscal repair technique was introduced. This type of suturing initially consisted of using bioabsorbable devices such as arrows, darts or staples, and became the third generation of meniscal suturing. It presented potential benefits such as ease of use, adaptability to different types of injury, reduced duration of operations and diminished morbidity. However, it was not free from complications, such as early failure (due to breakage of the implant) and repair resistance that was inferior to that of the previous techniques (inside-out and outside-in), which presented more than twice the resistance to suture tear forces.19, 20 To surmount these deficiencies of the initial implants of the all-inside third generation, the Fast-Fix device was developed as a modification of the Smith & Nephew T-Fix device, with the main aim of achieving suture resistance equal to that provided by the inside-out technique.12 These inside-out suturing devices using resistant thread have become known as the fourth generation, among which the Fast-Fix device is the precursor. Today, the all-inside technique performed using fourth-generation implants and the inside-out technique present similar success and complication rates.21
With better comprehension of the importance of meniscal suturing, there has been rapid development of the repair techniques over the last 25 years. These improvements have been aimed mainly toward making surgery easier, and have led to increased use of this procedure.12, 22 Unfortunately, in Brazil the popularity of meniscal repair still seems to be far behind what has been reached in other regions, such as the United States and Europe. This can be demonstrated partly by the relative scarcity of studies published in the Brazilian literature on this topic and partly by the difficulty of having these devices released for use through healthcare service agreements and within the Brazilian National Health System (SUS), given that they make the final cost of surgery higher. Auditors and managers do not understand the real benefit that this increased expenditure brings for patients and consequently deny requests to use these devices.23, 24, 25 The technological gap that exists between Brazil and more developed countries should also be mentioned, considering that approval for devices developed outside of Brazil that are more advanced ends up being delayed by controlling bodies. Furthermore, the Brazilian materials are often well below what is desired, and are sometimes even improper for use.
In considering treatment failure to be the need for a new surgical procedure, the presence of mechanical symptoms or a Lysholm score less than 64 or IKDC less than 50, we were able to conclude that in our study there were no cases of failure and that no complications were diagnosed. However, it needs to be borne in mind that in the present study, the sample was relatively small and that this may have influenced the result. In addition, the mean duration of postoperative assessment was 59 months (medium term). If we were to evaluate these patients again, over a longer term, we would probably find cases of failure with the need for a new surgical procedure. In stratifying the results according to the scores obtained, the Lysholm scale showed that 73% of the results were excellent and good and 27% were fair. None of the patients were classified as poor. According to the IKDC, 82% of the results were excellent and good and 18% were fair. Once again, none of the results were classified as poor.
In the literature, the clinical success rates for meniscal sutures are between 83% and 96.4%, when done together with ACL reconstruction,26, 27, 28 and 84% when the procedures are done at different times.29 On the other hand, the rate of good results from conservative treatment for meniscal injuries in association with ACL reconstruction has been found to be 50–61%.30 When the meniscal repair is done separately, without association with ACL reconstruction, a failure rate of 17–19% has been reported.21
The greater success rate presented here can be partly explained by a less rigorous assessment criterion, given that in some of the studies presented, the sutured meniscus was evaluated by means of a second arthroscopy procedure and, in certain cases, meniscal injuries were seen to be present in clinically symptomless patients, which increased the rigor of the results. Other potential factors were the small sample size and the greater rigor in choosing the sutured injuries. In the present study, also differing from the literature, the success rate from meniscal repair when associated with ACL reconstruction was not seen to be greater than in the same procedure done separately. The explanation for this is probably related to the small number of patients, given that despite the lack of statistical significance, there was a tendency for patients with simultaneous ACL reconstruction to present better pre and postoperative evaluations.
Conclusion
Among the patients studied, the all-inside meniscal repair technique using the Fast-Fix device was effective and safe for treating meniscal injuries in the red zone or red-white zone, with or without simultaneous ACL reconstruction, and presented good or excellent results in the majority of the patients.
Conflicts of interest
Dr. Leonardo José Bernardes Albertoni is a consultant for Pró-Cirurgia Especializada (PCE), the distributor for Smith & Nephew in Brazil, but he declares that he did not receive any incentive to carrying out this study. The authors declare that there were no conflicts of interest.
Footnotes
Study conducted at the Department of Orthopedics and Traumatology, Escola Paulista de Medicina, Universidade Federal de São Paulo, São Paulo, SP, Brazil.
References
- 1.Voloshin A.S., Wosk J. Shock absorption of meniscectomized and painful knees: a comparative in vivo study. J Biomed Eng. 1983;5:157–161. doi: 10.1016/0141-5425(83)90036-5. [DOI] [PubMed] [Google Scholar]
- 2.Kurosawa H., Fukubayashi T., Nakajima H. Load-bearing mode of the knee joint: physical behavior of the knee joint with or without menisci. Clin Orthop Relat Res. 1980:283–290. [PubMed] [Google Scholar]
- 3.MacConaill M.A. The movements of bones and joints; the synovial fluid and its assistants. J Bone Joint Surg Br. 1950;32:244–252. doi: 10.1302/0301-620X.32B2.244. [DOI] [PubMed] [Google Scholar]
- 4.Hsieh H.H., Walker P.S. Stabilizing mechanisms of the loaded and unloaded knee joint. J Bone Joint Surg Am. 1976;58:87–93. [PubMed] [Google Scholar]
- 5.Barber F.A., Stone R.G. Meniscal repair. An arthroscopic technique. J Bone Joint Surg Br. 1985;67:39–41. doi: 10.1302/0301-620X.67B1.3881452. [DOI] [PubMed] [Google Scholar]
- 6.Fairbank T.J. Knee joint changes after meniscectomy. J Bone Joint Surg Br. 1948;30:664–670. [PubMed] [Google Scholar]
- 7.Baratz M.E., Fu F.H., Mengato R. Meniscal tears: the effect of meniscectomy and of repair on intraarticular contact areas and stress in the human knee. A preliminary report. Am J Sports Med. 1986;14:270–275. doi: 10.1177/036354658601400405. [DOI] [PubMed] [Google Scholar]
- 8.Pujol N., Barbier O., Boisrenoult P., Beaufils P. Amount of meniscal resection after failed meniscal repair. Am J Sports Med. 2011;39:1648–1652. doi: 10.1177/0363546511402661. [DOI] [PubMed] [Google Scholar]
- 9.Arnoczky S.P., Warren R.F. Microvasculature of the human meniscus. Am J Sports Med. 1982;10:90–95. doi: 10.1177/036354658201000205. [DOI] [PubMed] [Google Scholar]
- 10.Morgan C.D. The “all-inside” meniscus repair. Arthroscopy. 1991;7:120–125. doi: 10.1016/0749-8063(91)90093-d. [DOI] [PubMed] [Google Scholar]
- 11.Choi N.H., Kim T.H., Victoroff B.N. Comparison of arthroscopic medial meniscal suture repair techniques: inside-out versus all-inside repair. Am J Sports Med. 2009;37:2144–2150. doi: 10.1177/0363546509339010. [DOI] [PubMed] [Google Scholar]
- 12.Haas A.L., Schepsis A.A., Hornstein J., Edgar C.M. Meniscal repair using the FasT-Fix all-inside meniscal repair device. Arthroscopy. 2005;21:167–175. doi: 10.1016/j.arthro.2004.10.012. [DOI] [PubMed] [Google Scholar]
- 13.Stärke C., Kopf S., Petersen W., Becker R. Meniscal repair. Arthroscopy. 2009;25:1033–1044. doi: 10.1016/j.arthro.2008.12.010. [DOI] [PubMed] [Google Scholar]
- 14.Peccini M.S., Ciconelli R., Cohen M. Questionário específico para sintomas do joelho “lysholm knee scoring scale” – tradução e validação para a língua portuguesa. Acta Ortop Bras. 2006;14:268–272. [Google Scholar]
- 15.Irrgang J.J., Anderson A.F., Boland A.L., Harner C.D., Kurosaka M., Neyret P. Development and validation of the international knee documentation committee subjective knee form. Am J Sports Med. 2001;29:600–613. doi: 10.1177/03635465010290051301. [DOI] [PubMed] [Google Scholar]
- 16.Paxton E.S., Stock M.V., Brophy R.H. Meniscal repair versus partial meniscectomy: a systematic review comparing reoperation rates and clinical outcomes. Arthroscopy. 2011;27:1275–1288. doi: 10.1016/j.arthro.2011.03.088. [DOI] [PubMed] [Google Scholar]
- 17.Henning C.E. Arthroscopic repair of meniscus tears. Orthopedics. 1983;6:1130–1132. doi: 10.3928/0147-7447-19830901-08. [DOI] [PubMed] [Google Scholar]
- 18.Warren R.F. Arthroscopic meniscus repair. Arthroscopy. 1985;1:170–172. doi: 10.1016/s0749-8063(85)80005-0. [DOI] [PubMed] [Google Scholar]
- 19.Barber F.A., Herbert M.A. Meniscal repair devices. Arthroscopy. 2000;16:613–618. doi: 10.1053/jars.2000.4819. [DOI] [PubMed] [Google Scholar]
- 20.Jones H.P., Lemos M.J., Wilk R.M., Smiley P.M., Gutierrez R., Schepsis A.A. Two-year follow-up of meniscal repair using a bioabsorbable arrow. Arthroscopy. 2002;18:64–69. doi: 10.1053/jars.2002.25343. [DOI] [PubMed] [Google Scholar]
- 21.Grant J.A., Wilde J., Miller B.S., Bedi A. Comparison of inside-out and all-inside techniques for the repair of isolated meniscal tears: a systematic review. Am J Sports Med. 2012;40:459–468. doi: 10.1177/0363546511411701. [DOI] [PubMed] [Google Scholar]
- 22.Musahl V., Jordan S.S., Colvin A.C., Tranovich M.J., Irrgang J.J., Harner C.D. Practice patterns for combined anterior cruciate ligament and meniscal surgery in the United States. Am J Sports Med. 2010;38:918–923. doi: 10.1177/0363546509357900. [DOI] [PubMed] [Google Scholar]
- 23.Silva J.L., Namba M.M., Pereira Filho F.A., Barbosa M.A., Albano M., Martins R.O. Sutura meniscal inside-out com agulha de anestesia peridural. Rev Bras Ortop. 2004;39:264–269. [Google Scholar]
- 24.Hernandez A.J., Camanho G.L., Laraya M.H.F., Favaro E. Sutura de menisco com implantes absorvíveis. Acta Ortop Bras. 2006;14:217–219. [Google Scholar]
- 25.Lino Júnior W. Evolução funcional da reparação do menisco por implante absorvível. Rev Bras Ortop. 2009;44:112–119. doi: 10.1016/S2255-4971(15)30057-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Ahn J.H., Lee Y.S., Yoo J.C., Chang M.J., Koh K.H., Kim M.H. Clinical and second-look arthroscopic evaluation of repaired medial meniscus in anterior cruciate ligament-reconstructed knees. Am J Sports Med. 2010;38:472–477. doi: 10.1177/0363546509348102. [DOI] [PubMed] [Google Scholar]
- 27.Tachibana Y., Sakaguchi K., Goto T., Oda H., Yamazaki K., Iida S. Repair integrity evaluated by second-look arthroscopy after arthroscopic meniscal repair with the FasT-Fix during anterior cruciate ligament reconstruction. Am J Sports Med. 2010;38:965–971. doi: 10.1177/0363546509356977. [DOI] [PubMed] [Google Scholar]
- 28.Popescu D., Sastre S., Caballero M., Lee J.W., Claret I., Nuñez M. Meniscal repair using the FasT-Fix device in patients with chronic meniscal lesions. Knee Surg Sports Traumatol Arthrosc. 2010;18:546–550. doi: 10.1007/s00167-009-0926-6. [DOI] [PubMed] [Google Scholar]
- 29.Kubiak G., Fabiś J. Clinical results of meniscus repair. Ortop Traumatol Rehabil. 2010;12:28–40. [PubMed] [Google Scholar]
- 30.Pujol N., Beaufils P. Healing results of meniscal tears left in situ during anterior cruciate ligament reconstruction: a review of clinical studies. Knee Surg Sports Traumatol Arthrosc. 2009;17:396–401. doi: 10.1007/s00167-008-0711-y. [DOI] [PubMed] [Google Scholar]