

Abstract
The osteochondritis dissecans (OCD) is a disease of unknown cause that classically affects the knee lateral border of the medial femoral condyle. We present a rare case of OCD in bilateral lateral femoral condyle.
Keywords: Osteochondritis dissecans, Knee, Cartilage articular
Resumo
A osteocondrite dissecante (OCD) é uma patologia de causa desconhecida, que classicamente acomete no joelho a borda lateral do côndilo femural medial. Apresentamos um raro caso de OCD no côndilo femural lateral bilateral.
Palavras-chave: Osteocondrite dissecante, Joelho, Cartilagem articular
Case report
The patient was a 28-year-old white female nurse of sedentary habits who presented a complaint of sudden pain in her left knee around 20 days earlier, without any history of trauma. The condition improved with non-steroidal anti-inflammatory drugs and worsened after physical exertion. She also reported that she had had a similar condition in her right knee three years earlier, but the right knee was asymptomatic at this time.
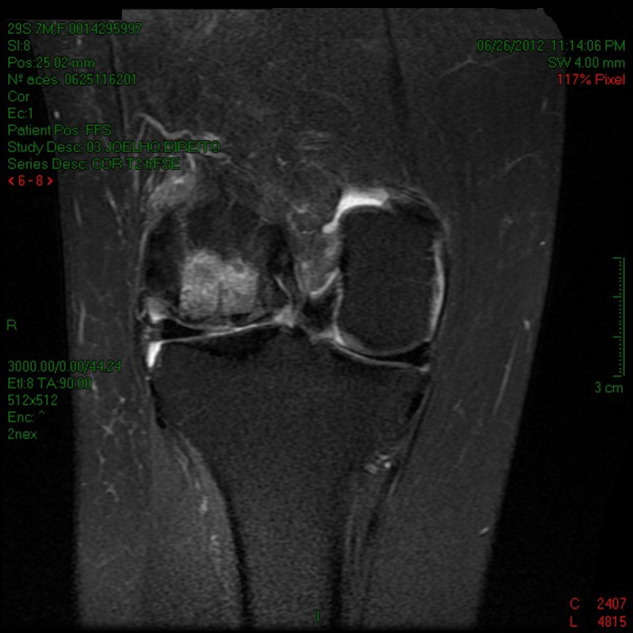
On physical examination, she presented bilateral genu valgum with crepitation on flexion–extension and pain on anterolateral palpation in both knees. The pain was more intense in the left knee, which also presented effusion (+/4+). Radiographs in AP, lateral and tunnel views were produced on the patient, and also bilateral magnetic resonance imaging (MRI). This revealed unstable osteochondral fragments measuring 30 mm × 20 mm in the lateral femoral condyle in the left knee and 30 mm × 28 mm in the right knee. According to the Insall classification for MRI on osteochondritis,1 the lesions were classified as stage V on the left side and stage IV on the right side (Figure 1, Figure 2).
Figure 1.
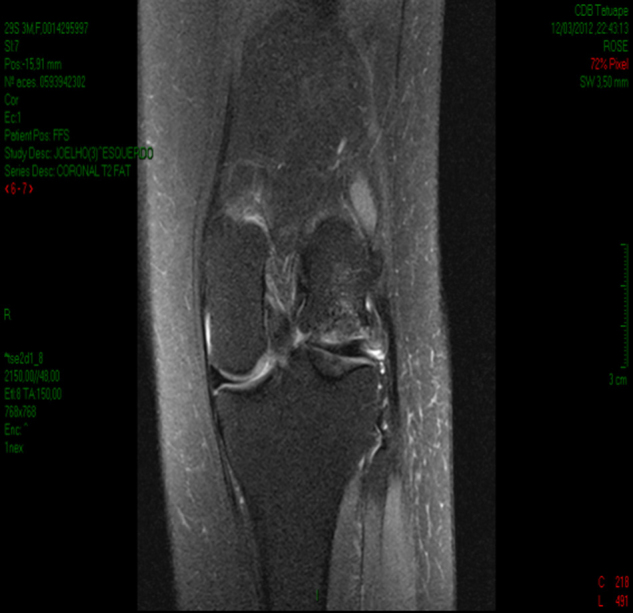
Preoperative MRI on the left knee.
Figure 2.

Preoperative MRI on the right knee.
We implemented surgical treatment initially on the left knee. The patient underwent arthroscopy with joint inspection, in which we observed a chondral lesion of around 30 mm × 20 mm in the lateral femoral condyle of the left knee, with a loose chondral fragment in the joint. This fragment did not present vitality and was of ivory appearance, and in situ fixation was contraindicated. We then performed arthrotomy, with exposure of the lateral condyle of the femur. We decided to perform mosaicplasty, using an autologous osteochondral graft. This was obtained by removing three osteochondral plugs from the lateral face of the trochlea of the lateral femoral condyle (donor zone), using trephines with an 8 mm Artrex® guide (Fig. 3), in order to fill the injured area (recipient zone). The patient was discharged from hospital one day after the surgery, without immobilization, but she continued to use crutches for 45 days, without weight-bearing, and with passive range-of-motion exercises. Her condition evolved satisfactorily, without pain or limitations.
Figure 3.

Postoperative MRI on the left knee.
One year after the surgery on the left knee, the patient started to complain of pain and joint locking in the right knee. She then underwent surgical treatment with arthroscopy, which showed the lesion in the lateral femoral condyle and the presence of a free intra-articular body measuring around 30 mm × 30 mm. We performed lateral arthrotomy, with removal of the loose fragment, and mosaicplasty on the lateral femoral condyle, in which three osteochondral plugs were removed from the donor zone on the lateral face of the trochlea, in the same way as done in the procedure on the left knee. However, this time, the plugs were of diameter 10 mm and we used trephines with a Johnson & Johnson® guide. We then used the same postoperative protocol, with satisfactory evolution (Fig. 4).
Figure 4.
Postoperative MRI on the right knee.
One year and six months has now passed since the operation on the left knee, and six months since the operation on the right knee, and the patient does not have any complaints or limitations.
Discussion
Osteochondritis dissecans (OCD) is a pathological condition of unknown cause that occurs in the subchondral bone.2, 3 It presents in a juvenile form, when the growth plate is open, or in an adult form, when it is present in the mature skeleton. The latter generally requires surgical treatment and has worse prognosis. Clinically, it presents several forms of manifestation.
It classically affects the lateral border of the medial femoral condyle.2 Bilateral occurrence and cases in the lateral femoral condyle have been little reported in the literature.4
It is classified in accordance with the anatomical location, stability of the fragment and alterations seen on MRI, scintigraphy and radiographs.2 Alterations seen in imaging aid in choosing the therapy and, when this is the case, in the evolution of conservative treatment.3
The surgical treatment comprises several techniques,4, 5, 6, 7, 8 such as resection of the fragment, arthroscopic drilling, mosaicplasty, in situ fixation of the fragment and microfracturing, among others, according to the location and viability of the fragment.9 However, initial arthroscopy has been shown to be important for evaluating the type and extent of the lesion and the mobility of the osteochondral fragment. It has a direct implication in the choice of appropriate therapy and in performing it arthroscopically when possible. Arthrotomy can also be chosen, when necessary.10 In the present case, after performing arthroscopy and assessing the vitality of the fragment and its size, we decided to use mosaicplasty.
In this manner, we have reported a rare bilateral case of osteochondritis dissecans of the lateral femoral condyle, which was treated by means of the mosaicplasty technique with good clinical results.
Conflicts of interest
The authors declare no conflicts of interest.
Footnotes
Work performed at the Tatuapé Orthopedics Clinic, Taubaté, SP, Brazil.
References
- 1.Hefti F., Berguiristian J., Krauspae R., Möller-Madsen B., Riccio V., Tschauner C. Osteochondritis dissecans: a multicenter study of the European Pediatric Orthopaedic Society. J Pediatr Orthop B. 1999;8(4):231–245. [PubMed] [Google Scholar]
- 2.Ganley T.J., Flynn J.M. Osteochondritis dissecans. In: Scott W.N., editor. Surgery of the knee. 4th ed. Churchill Livingstone; New York: 2006. pp. 1234–1241. [Google Scholar]
- 3.Anderson A.F., Lipscomb A.B., Coulan C. Antegrade curettement, bone grafting, and pinning of osteochondritis in the skeletally matureknee. Am J Sports Med. 1990;18(3):254–261. doi: 10.1177/036354659001800306. [DOI] [PubMed] [Google Scholar]
- 4.Cetik O., Turker M., Uslu M. Bilateral osteochondritis dissecans of lateral femoral condyle. Knee Surg Sports Traumatol Arthrosc. 2005;13(6):468–471. doi: 10.1007/s00167-004-0543-3. [DOI] [PubMed] [Google Scholar]
- 5.Green W.T., Banks H.H. Osteochondritis dissecans in children. Clin Orthop Relat Res. 1990;(255):3–12. [PubMed] [Google Scholar]
- 6.Havulinna J., Jokio P., Lindholm T.S., Viljanen V., Savilahti S. Long-term results of Smillie pin fixation of osteochondritis dissecans in the femoral condyles. Ann Chir Gynaecol. 1995;84(1):71–80. [PubMed] [Google Scholar]
- 7.Lindholm S., Pylkkänen P. Internal fixation of the fragment of osteochondritis dissecans in the knee by means of bone pins. A preliminary report on several cases. Acta Chir Scand. 1974;140(8):626–629. [PubMed] [Google Scholar]
- 8.Slough J.A., Noto A.M., Schmidt T.L. Tibial cortical bone peg fixation in osteochondritis dissecans of the knee. Clin Orthop Relat Res. 1991;(267):122–127. [PubMed] [Google Scholar]
- 9.Twyman R.S., Desai K., Aichroth P.M. Osteochondritis dissecans of the knee. A long-term study. J Bone Joint Surg Br. 1991;73(3):461–464. doi: 10.1302/0301-620X.73B3.1670450. [DOI] [PubMed] [Google Scholar]
- 10.Severino N.R., Camargo O.P.A., Aihara T., Cury R.P.L., Vaz C.E.S., Perez G.G. Osteocondrite dissecante do joelho: estudo restrospectivo de 52 pacientes. Rev Bras Ortop. 1996;31(4):309–314. [Google Scholar]