

Summary:
Healthcare advocacy is an important tool in the plastic surgeon’s arsenal that stands the potential to improve both patient care and the profession. However, many physicians underestimate the importance and influence that healthcare advocacy has on the profession and feel that they lack the leverage and knowledge to advocate on behalf of themselves, their practices, their patients, and their profession, all of which are untrue. Plastic surgeons are uniquely positioned to advocate based on their clinical acumen, personal experiences with patient care, and their position in the healthcare ecosystem value chain. This article aims to equip plastic surgeons with a general framework of knowledge regarding policy and advocacy. Additionally, the article outlines and discusses recent advocacy efforts related to plastic surgery, and efforts that are on the horizon to provide some context to the relevance of advocacy related to plastic surgery. Finally, we aim to empower plastic surgeons to step into the policy advocacy arena for the betterment of our patients and the professional practice of plastic surgery.
INTRODUCTION
Healthcare advocacy is an integral tool for physicians to ensure that patients are treated to the best of their ability. Advocacy should be part of a physician’s armamentarium, regardless of specialty. In the ever-changing political climate of the United States, health policy and reform are turning into common hot-button issues, not only at the state level but also at the federal level of government. In contrast to politicians and other policy experts, plastic surgeons are uniquely positioned to advocate on behalf of their patients and their profession through their direct healthcare experience and clinical knowledge. A recent JAMA editorial by former Administrator of the Centers for Medicare and Medicaid Services, Dr. Donald Berwick said, “the work of a physician as a healer cannot stop at the door of an office, the threshold of an operating room, or the front gate of a hospital … To try to avoid the political fray through silence is impossible … Either engage, or assist in the harm.”1
The purpose of this special topics article is to provide plastic surgeons with a basic framework of knowledge regarding the importance of health policy advocacy and also to review recent successes in advocacy related to plastic surgery. We aim to empower plastic surgeons to be diligent advocates and to utilize their influence on policy.
POLICY AND ADVOCACY 101
Policy can be broadly defined as a set of rules, principles, or actions adopted by an institution for the benefit of its pertinent constituents or stakeholders, which are enforceable. Advocacy can be employed by a spectrum of individuals, ranging from local hospital personnel regarding implementation of institutional policy to government officials advocating for sweeping federal policies. On the one end of the policy spectrum, hospital systems can create policy that requires surgeons to double glove or wear a surgical cap versus a bouffant. On the other end of the spectrum, policy can be adopted by Congress that requires insurance companies to provide coverage for breast cancer patients who desire breast reconstruction as in the case of the Women’s Health and Cancer Rights Act.2 Advocacy is defined as taking action to support, oppose, or recommend policy or law, and in this current climate, physician advocacy is more important than ever before.3
Healthcare policy advocacy within plastic surgery stands the potential to impact education, training, practice of plastic surgery, and individual patient care.3 When considering policy and how it may impact the practice of plastic surgery, all key stakeholders who stand to benefit from or be impacted by a specific piece of policy should be considered. Key stakeholders in healthcare and health policy to be considered are often summarized into the 5 P’s: Patients, Providers, Purchasers, Payers, and the Public (Fig. 1). Healthcare policy has the potential to impact all aforementioned stakeholders, and taking each one into consideration is essential for meaningful advocacy.
Fig. 1.

Summary of the 5 P’s when considering relevant stakeholders for a given policy.
Although no two pieces of policy are implemented through precisely the same process, there is a general lifecycle of policy development that physician advocates should be familiar with, which can, in turn, shed light on where advocates can intervene through advocacy (Fig. 2). As advocates, plastic surgeons can identify problems and make them known to policy makers and healthcare administrators. By doing so, it will effectively influence both agenda setting and policy formulation to solve the identified issues through policy. For example, plastic surgeons have identified the need for insurance coverage of comprehensive pediatric congenital malformation. Because of this, it is hoped that the American Society of Plastic Surgeons (ASPS) continues to convey this issue to gain bipartisan support to draft new legislation. As a specific piece of policy is being considered for adoption, plastic surgeons can advocate support or opposition, depending on the policy’s impact on the 5 P’s. Lastly, plastic surgeons can evaluate policy through research to analyze how it impacts practice and patient care. These results can further influence agenda setting and subsequent policy formulation.
Fig. 2.
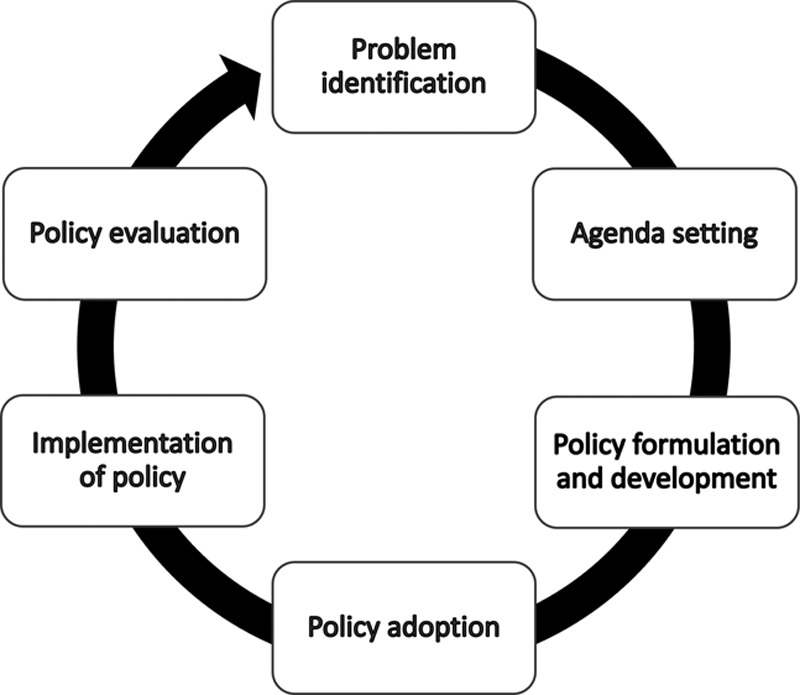
Summary depiction of the policy cycle, which is applicable to all levels of government.
AVENUES FOR ADVOCACY
The landscape of healthcare in the United States is uniquely complex and continuously evolving at the federal, state, and even institutional levels. Plastic surgeons are positioned to advocate at all levels for the betterment of patient care and the profession. Many physicians, including plastic surgeons, are unaware of the authority and expertise they stand to assist with changes.
There are numerous avenues through which plastic surgeons can advocate. Some examples include, state capitols, social media, blogging, community and institution education, and serving on committees and councils in professional organizations and at their own home institution.
The field of plastic surgery is fortunate to have a strong existing infrastructure for advocacy thanks to organizations such as the ASPS. One key cornerstone to the ASPS advocacy presence includes PlastyPAC.4 This is a political action committee (PAC) led by plastic surgeons who work in collaboration with fellow physicians, patients, and policy experts to advocate, educate, influence, and provide support for political campaigns and candidates that advance and reinforce key issues within the field of plastic surgery.
Despite this existing framework, contributions to PlastyPAC are limited. In fact, there are 9 states throughout the country without a single contributor to this specific PAC and 16 additional states with 3 or less contributors.4 This advocacy branch of the ASPS and its associated PAC could be even stronger and more representative of the entire profession with assistance and input from additional plastic surgeons throughout the country through engagement, or better understanding of the advantages of participating in political advocacy.
Participating in political advocacy can take many forms and include multiple levels of involvement.3 The simplest way to become engaged is through contacting the office of a Congressperson or executive through letter writing, phone calls, or email message. The format for letters and emails along with suggested rules of engagement of such messaging are simple. They are usually available within the Society’s advocacy representatives and are available as a supplement to this article. It is important to provide an introduction along with a description of expertise and experience in the field that qualifies and further buttresses the perspective provided in the message. Additionally, a brief description of rationale for contacting the individual should be incorporated early in the message to orient its recipient. In the body of the message, a concise but detailed perspective should be provided and contain evidence to support opinions related to the issue at hand. The message should conclude cordially and with an invitation to discuss the matter further at a later date with provided contact information. To summarize, the message should be collegial, brief, and inviting to explore the issue further collaboratively. Additionally, social media can play a role in advocacy. Platforms such as Twitter provide a platform, wherein plastic surgeons are able to share their perspective on a given issue and discuss with colleagues, policy makers, and other constituents/stakeholders interested in the topic.
Advocacy can also be much more involved and personable in the form of face-to-face meetings, which can be set up through contacting political figure’s office individually or on behalf of an association/organization (ie, ASPS). Similar to the aforementioned means of messaging, meetings are often brief, which requires professional and persuasive efforts in a concise timeframe focusing on a specific issue or piece of policy. More intimate forms of advocacy such as face-to-face meetings can lead to fruitful professional collaboration between plastic surgeons and policy makers/executives and can evolve into ad hoc/impromptu policy advising and communications as the healthcare landscape evolves.
The emphasis of health policy advocacy is to move the needle in the right direction for the betterment of patient care and the profession, specifically as it relates to plastic surgery. Letter writing, Tweets, and 20-min meetings may seem inconsequential, but this is untrue. These sorts of approaches can be effective and indeed are the sole means of amplifying the voice of plastic surgeons in the political arena. The effects of such efforts can be compounded further when a larger number of plastic surgery advocates step into the arena of policy.
As physicians, we are all engrossed in our practices endless hours a day and sometimes something as simple as emailing a congressperson seems to escape us. Over the years the responses for lack of engagement by our peers have included, “too busy,” “it doesn’t affect my practice,” “I won’t make a difference,” “someone else will do it,” “I don’t like my congressperson,” etc. The general apathy that exists remains the primary barrier to PAC contributions as well.
As will be discussed below, advocates in plastic surgery have already been successful in such efforts and should facilitate and inspire more plastic surgeons to become involved.
FEDERAL ADVOCACY
Key advocacy issues identified by the ASPS in the past undoubtedly have the potential to impact plastic surgeons, their practice, and their patients. In 2017 alone, the ASPS submitted 42 letters in support or opposition of different pieces of legislation relating to the field of plastic surgery. Advocacy on behalf of the ASPS played an integral role in the Breast Cancer Patient Education Act (BCPEA) of 2015.5 The BCPEA’s passage was a more recent success that came in the wake of the Women’s Health and Cancer Rights Act (WHCRA) of 1998, which required insurance coverage for breast cancer patients who desired breast reconstruction. Advocacy on behalf of the ASPS was instrumental in gaining support and eventually passing the Women’s Health and Cancer Rights Act.
The BCPEA aims to increase patient awareness and education of reconstructive options after mastectomy secondary to breast cancer. It also provides information pertaining to insurance companies and coverage options. Many patients, especially medically underserved populations, remain unaware of breast reconstruction and prostheses postmastectomy as an option that is covered by health insurance providers.6–8
Stakeholder engagement, not only including plastic surgeons, other physicians, and politicians but also patients themselves was instrumental in the passage of the BCPEA. Many patients accompanied plastic surgeons in advocating for this policy by sharing personal stories and experiences with federal legislators. This form of stakeholder engagement through sharing of firsthand experiences unquestionably also contributed to legislators’ support of the BCPEA. This underscores the importance of stakeholder engagement in policy advocacy.
The ASPS has identified this as a key issue and is continuously attempting to raise patient awareness of this surgical option for breast cancer patients in the wake of passage of the BCPEA. Support by plastic surgeons was instrumental in passing of the BCPEA, in part, due to their clinical knowledge, extensive experience with the specific patient population who stood to benefit from the bill’s passage, and insight regarding education, access, and shortcomings associated with insurance companies and costs related to breast reconstruction.
Additionally, the ASPS is diligently working to increase patient safety by supporting policy that ensures patients are seeking care from board-certified plastic surgeons. Numerous stories have emerged in the media regarding unethical care, unacceptable complications, and misleading advertisements involving uncertified physicians. This is an issue that is likely to persist unless plastic surgeons and other clinicians advocate for policy change at local, state, or federal levels.
The ASPS has also recognized the importance of increasing the number of plastic surgery staff and faculty positions available to medical school graduates and trainees, respectively. In past years, the number of plastic surgery services rendered has increased, and it is important to maintain an adequate workforce to meet those needs.9,10 By advocating for increased funding for Medicare-funded graduate medical education (GME) residency and fellowship positions, the ASPS continues to support this issue.
The ASPS is also working to increase health insurance coverage for additional types of reconstructive surgery. For example, ASPS recently endorsed the Ensuring Lasting Smiles Act, which would require health insurance coverage for reconstructive surgery of congenital craniofacial defects.11 Advocacy pertaining to this issue was the primary topic addressed and acted upon at the ASPS Advocacy Summit in June of 2018.
RESEARCH-RELATED ADVOCACY
Successful advocacy efforts through the Plastic Surgery Foundation have established research databases which tackle important clinical questions. Some of these databases include the National Breast Implant Registry (NBIR), Patient Registry and Outcomes For breast Implants and anaplastic large cell Lymphoma etiology and Epidemiology (PROFILE), and the General Registry of Autologous Fat Transfer. National Breast Implant Registry plans to be a collaborative effort in which patient safety will be monitored through post-market surveillance and device tracking information. The Patient Registry and Outcomes For breast Implants and anaplastic large cell Lymphoma etiology and Epidemiology registry is a centralized repository for important data regarding breast implant-associated anaplastic large cell lymphoma to obtain a better understanding of its etiology, epidemiology, and surveillance. Regulation related to fat grafting and regenerative medicine is of increasing interest, and the General Registry of Autologous Fat Transfer database will aim to contribute clinical practice guidelines through evidence-based data.
STATE-LEVEL ADVOCACY
Plastic surgeon advocacy has also contributed successful lobbying of numerous policy pieces at the state level of government as well, part of which included 155 letters submitted to state legislatures and regulatory bodies. In the state of Indiana, for example, plastic surgeons opposed legislation that would have permitted expansion of dental surgical scope to include the maxillofacial region. In Ohio, plastic surgeons implemented policy changes permitting mid-level providers and certified medical assistants to use and operate laser devices under the supervision of a qualified physician. Successful efforts in Louisiana culminated in approval of legislation for a breast reconstruction education. Plastic surgeons’ advocacy has not solely been limited to issues directly influencing the field of plastic surgery but also healthcare infrastructure and medical practice in general. In numerous states, plastic surgeons and PlastyPAC have actively opposed legislation that would permit advanced practice providers to practice independently and also have advocated against expansion of naturopaths’ scopes of practice.
LOCAL-LEVEL ADVOCACY
At more local levels of government, plastic surgeons have been active in promoting the field of plastic surgery and access to plastic surgery as well. Breast Reconstruction Awareness days are held annually in cities and municipalities throughout the country during breast cancer awareness month in October. Breast Reconstruction Awareness days take many forms, ranging from fundraising efforts through dine-out nights, to presence at local community and sporting events.
“NEGATIVE ADVOCACY”—PREVENTING ONEROUS POLICY
Sometimes, plastic surgeons may believe that nothing has been done to prevent certain practices. In those cases, the overall perception is that policy advocacy does not affect their practice, and part of why this misperception exists is by the nature of some forms of advocacy, which can entail the advocacy against enactment of onerous legislation. As mentioned, advocacy is a 2-way street that can work in both directions—both support and opposition of policy. For example, when the federal government was considering a national cosmetic surgery tax, practicing plastic surgeons in New Jersey had and were currently enduring a similar tax at a state level.12 Their advocacy from this experience with a similar policy within their own state rendered their input and perspectives immensely helpful in describing the possible downsides and detriments to enacting a similar policy at the federal level. Due, in part, to the onerous efforts of the ASPS advocacy team, a national cosmetic tax was never passed. Another example includes the current efforts to increase patient awareness of what is the scope of plastic surgery, prevent nonsurgeons from performing complex surgical procedures, prevent false or misleading advertisement of plastic surgery procedures to assure safety of plastic surgery patients.13 However, for plastic surgeons not engaged in advocacy, these worthwhile and noteworthy efforts are more likely to go unnoticed than supportive policy advocacy, which is much more likely to be more publicized and subject of discussion in the media.
RESIDENT AND MEDICAL STUDENT ENGAGEMENT
Medical students and residents are the future advocates for our patients and profession and the future leaders in the field of plastic surgery that will be responsible for changes. Recognizing this, resident and medical student involvement in advocacy is paramount to imprint the importance of healthcare literacy and advocacy. Attendance to the ASPS Advocacy Summit has been encouraged and marketed. Furthermore, there is a move to increase opportunities for resident representation on PlastyPAC’s Legislative Advocacy Committee and other leadership opportunities. One example of the importance of resident and medical student involvement in advocacy is the GME policy. The legislators engagement is noticeably more genuine when a future resident speaks of the proposed residency shortages than a plastic surgeon already in practice. On this case, residents and medical students are involved as stakeholders and advocates, similar to how patients were integral in advocating for passage of the BCPEA.
THE EVOLUTION OF ASPS ADVOCACY
The second annual ASPS Advocacy Summit took place June 26–28, 2018 in Washington, D.C.14 The meeting involved sessions and roundtable discussions for plastic surgeons, advocacy/policy experts, representatives from PlastyPAC, physician advocates, policymakers, and political analysts to collaborate on common interests. The summit allowed plastic surgeons to gain knowledge, experience, and tactics relating to advocacy, which could then be applied toward issues important to them and their institution. Moreover, ASPS selects policy priorities based on those roundtables and members’ input. The general membership is polled yearly and policy priority issues at both the federal and state levels are evaluated and prioritized.
Before the Advocacy Summit, in years prior multistate regional fly-ins were organized for plastic surgeons to meet with their respective legislators to advocate hot topic healthcare issues relevant to the practice of plastic surgery. These experiences, while effective, were less comprehensive and collaborative in contrast to the new annual summit that brings a larger number of participants to the table increasing the presence of stakeholders.
CONCLUSIONS
Some plastic surgeons have engaged in policy advocacy and those who have not, are poised to make beneficial contributions. Advocacy, in this way, stands to better the profession along with plastic surgery patients. It is important to engage and remain active in the arena of policy. A great framework for lobbying and advocacy has been developed and exists thanks to the work by the ASPS and other foundations, organizations, and societies, and it is time that plastic surgeons felt empowered to capitalize upon existing infrastructure.
ACKNOWLEDGMENTS
The authors would like to thank and acknowledge Jessica Frasco, ASPS—PlastyPAC staff liaison for providing information for the contents of this manuscript.
Footnotes
Published online 3 May 2019.
Disclosure: J.P.F. has received financial compensation in the past 12 months for consulting related to two products—Misonix and Integra.G.A.G. has received speakership financial compensation from Pacira Pharmaceuticals. The other authors have no financial interest to declare in relation to the content of this article.
REFERENCES
- 1.Berwick DM. Moral choices for today’s physician. JAMA. 2017;318:2081–2082. [DOI] [PubMed] [Google Scholar]
- 2.The Women’s Health and Cancer Rights Act. Available at https://www.cms.gov/CCIIO/Programs-and-Initiatives/Other-Insurance-Protections/whcra_factsheet.html. Accessed November 28, 2018.
- 3.Earnest MA, Wong SL, Federico SG. Perspective: physician advocacy: what is it and how do we do it? Acad Med. 2010;85:63–67. [DOI] [PubMed] [Google Scholar]
- 4.ASPS PlastyPAC. Available at https://plastypac.aristotle.com/SitePages/Homepage.aspx.
- 5.H.R.2540—Breast Cancer Patient Education Act of 2015. Available at https://www.congress.gov/bill/114th-congress/house-bill/2540/text. Accessed November 30, 2018.
- 6.Albornoz CR, Cohen WA, Razdan SN, et al. The impact of travel distance on breast reconstruction in the United States. Plast Reconstr Surg. 2016;137:12–18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Abdou SA, Daar DA, Robinson IS, et al. A systematic literature review on disparities in postmastectomy breast reconstruction. Plast Reconstr Surg Glob Open. 2018;6(9 Suppl):114–115. [Google Scholar]
- 8.Daar DA, Abdou SA, Robinson IS, et al. Disparities in postmastectomy breast reconstruction: a systematic review of the literature and modified framework for advancing research toward intervention. Ann Plast Surg. 2018;81:495–502. [DOI] [PubMed] [Google Scholar]
- 9.Janes L, Lanier ST, Evans GRD, et al. State of the plastic surgery workforce and the impact of graduate medical education reform on training of plastic surgeons. Plast Reconstr Surg. 2017;140:412–420. [DOI] [PubMed] [Google Scholar]
- 10.Siotos C, Payne RM, Cui D, et al. Evolution of the plastic surgery workforce. Plast Reconstr Surg Glob Open. 2017;5(9 Suppl):105–106. [Google Scholar]
- 11.H.R.6689—Ensuring Lasting Smiles Act. Available at https://www.congress.gov/bill/115th-congress/house-bill/6689/text. Accessed November 30, 2018.
- 12.ASPS. Costmetic Tax Advocacy Talking Points. Available at https://www.plasticsurgery.org/Documents/members-only/health-policy/key-issues/cosmetic-tax/Taxes-Talking-Points.doc. Accessed December 1, 2018.
- 13.ASPS. 2018 Federal Policy Priorities. Available at https://www.plasticsurgery.org/documents/Advocacy/ASPS-Policy-Priorities_Federal_2018.pdf. Accessed December 1, 2018.
- 14.ASPS Advocacy Summit. Available at https://www.plasticsurgery.org/for-medical-professionals/resources-and-education/events/advocacy-summit.