

Abstract
Objectives
Internet-based STI testing programmes may overcome barriers posed by in-clinic testing, though uptake could reflect social gradients. The role these services play in comparison to clinical testing services is unknown. We compared experiences of testing barriers between STI clinic clients to clients of GetCheckedOnline.com (GCO; where clients take a printed lab form to a lab).
Methods
Our 10-month cross-sectional study was conducted after GCO was promoted to STI clinic clients and men who have sex with men (MSM). Clinic and GCO clients completed an online survey assessing testing barriers and facilitators; responses were compared using bivariate analysis (level of significance P<0.01; significant results below).
Results
Compared with 321 clinic clients, the 73 GCO clients were more likely to be older (median 35 vs 30 years), MSM (45% vs 16%), be testing routinely (67% vs 39%), have delayed testing for any reason (76% vs 54%) and due to clinic distance (28% vs 9%), report delays due to wait times (50% vs 17%), embarrassment with testing (16% vs 6%), discomfort discussing sexual health where they usually go for testing (39% vs 22%), as well as discomfort discussing sexual history with (19% vs 5%) and fearing judgement from (30% vs 15%) any healthcare provider. GCO clients were less likely to have found clinic hours convenient (59% vs 77%) and clinic appointments easy to make (49% vs 66%), and more likely to report long wait times (50% vs 17%). We found no differences in technology skills/use.
Conclusions
In this urban setting, an internet-based testing service effectively engaged individuals experiencing testing barriers, with few social gradients in uptake. While some testing barriers could be addressed through increasing access to clinical services, others require social and structural changes, highlighting the importance of internet-based STI testing services to increasing test uptake.
Keywords: gay men, testing, intervention studies, public health
Introduction
The increasing adoption of internet-based sexual health interventions speaks both to inevitable shifts in health service delivery and the continued appeal of reaching individuals with barriers to appropriate care who are at higher risk of sexually transmitted and bloodborne infections (STBBI).1 2 One such example are publicly funded internet-based diagnostic STBBI testing programmes, which typically reduce interactions with healthcare providers to post-test discussions for positive results, with or without a visit to a lab for submitting specimens (eg, where clients visit a website to either print a lab form to take to a lab or request a home self-sampling kit to mail to a lab for testing, with results accessed online, by phone or text).3–6 Developers of such programmes are motivated by the potential of internet-based services to reach individuals at greatest risk of infection and to reduce testing barriers through improving convenience and confidentiality.3 7–9 Their appeal to policy makers may also lie in assumptions regarding cost savings by reducing clinic-based testing expenditures.10 Perceived benefits of internet-based STBBI testing by patients are typically related to privacy and confidentiality (eg, avoiding anxiety or embarrassment associated with seeing a healthcare provider for testing, or being seen attending an STI clinic) and convenience (eg, no wait time for appointments, no need to travel to a clinic).11–14 While providing a means to overcome these barriers would improve equitable access to testing services, internet-based STBBI testing programmes could unintentionally perpetuate existing inequities if their uptake is patterned on existing social gradients, such as use by individuals with higher education or income. Existing inequities would be further exacerbated if use of these services was higher among individuals already having sufficient access to face-to-face testing services or who have higher levels of online health literacy (eg, more ‘tech-savvy’).15
In British Columbia, Canada, all residents are enrolled in the provincial medical services plan which provides universal healthcare, including STBBI testing and treatment. STBBI testing is available in settings ranging from specialised STI clinics to primary care settings. The BC Centre for Disease Control (BCCDC) implemented an internet-based STBBI testing programme called GetCheckedOnline.com (GCO) in 2014, where clients interact with the healthcare system when they submit specimens at a private lab or discuss positive or indeterminate lab results with a nurse by phone (negative results viewed online). GCO was initially promoted at STI clinics operated by BCCDC and to gay, bisexual and other men who have sex with men (GBMSM). This service offers testing for chlamydia and gonorrhoea through urine, throat and rectal swabs, and serological testing for HIV, hepatitis C and syphilis. As reduction of testing barriers and inequities in testing access is a primary objective of GCO, the objective of our study was to determine whether clients testing through GCO differed from clients testing through a low-threshold provincial STI clinic operated by BCCDC (where clients can test using pseudonyms). Based on our prior formative research,11 16 17 we hypothesised that GCO clients would more frequently report experiencing barriers accessing face-to-face STBBI testing, including clinic barriers (eg, long clinic wait times, inability to get to clinic during business hours, distance), provider-related barriers (eg, embarrassment talking to a provider about sex, privacy concerns, need to disclose sexual orientation) and societal or structural factors (eg, stigma or perceived judgement associated with seeking testing). We also hypothesised that GCO clients as early adopters of a new technology would be more likely to have higher technological access and skills.15 18
Methods
We used the CHERRIES checklist for reporting results of internet surveys to inform our description of study methods.19
Description of GetCheckedOnline.com and clinic testing pathways
We have previously published detailed descriptions of the GCO testing pathway as well as an evaluation of the GCO pilot phase during which this study took place.7 20 In brief, clients visit the GCO website to create an account and provide a first and last name, gender and sex, and birthdate (not verified). Clients then complete a risk assessment, generating tailored testing recommendations and specific educational messages. Clients who indicate being symptomatic or a contact of a partner with an STI are recommended to present to a clinic for testing instead of proceeding with GCO. Clients then print a lab form (with a code in place of their name for anonymity) and take it to an existing specimen submission site operated by a private general laboratory to submit specimens. These sites were initially chosen based on the distribution of known addresses of clients testing at the provincial STI clinic, as well as for locations with evening or weekend availability. At the lab, a phlebotomist collects blood for HIV, hepatitis C and syphilis testing. Chlamydia and gonorrhoea testing is done on client-provided urine samples, and if recommended, self-collected rectal and/or throat swabs. When test results are available, all clients are notified and receive test results online (if negative) or by phone (if positive; figure 1). The time to transition from account creation to specimen submission varies (days to months). This differs from the typical testing process at the STI clinic where recruitment for this study occurred, where clients present for pre-test counselling and specimen collection, and notification only occurs for positive results (figure 1).
Figure 1.

Comparison of testing and recruitment processes for GetCheckedOnline and clinic clients. Stars indicate events used to trigger subsequent recruitment emails at 2 and 3 weeks later for GetCheckedOnline and provincial STI clinic clients, respectively. aGetCheckedOnline clients take their printed lab form to a local private general laboratory where specimens are submitted (a phlebotomist collects blood specimens; client provides urine and self-collected throat and rectal swabs). Clinic clients have blood specimens collected by a clinic nurse who typically collects rectal and throat swabs, if not self-collected by the patient (client provides urine). +ve, positive result; –ve, negative result; BCCDC, BC Centre for Disease Control.
Study design
We recruited a sample of GCO and clinic clients who had consented to be contacted for research purposes and who had tested for STBBI in Vancouver, British Columbia, over a 10-month period (15 June 2015 to 12 April 2016). Clinic clients were recruited from a low-threshold provincial STI clinic operated by BCCDC and where GCO had been promoted to clients. In addition to the six private laboratory specimen submission sites being selected based on client addresses at this clinic, it is also located among other STI testing clinics in the Vancouver area (see online supplementary figure).
sextrans-2017-053325supp001.jpg (1.2MB, jpg)
{kind=link}
For GCO clients and provincial STI clinic clients, we used the email address provided during account creation or testing visit, respectively, to send an email invitation 2 weeks following the dates test results would be available to clients. This corresponded to 2 weeks following the receipt of a test result for GCO clients (date of reporting known for this study) and 3 weeks following pre-test visit for STI clinic clients, accounting for an approximate 1-week turnaround time for lab results (date of reporting not known for this study; figure 1).
The initial recruitment email invited clients to participate in a survey about their recent testing experience, included a link to the web survey and described the eligibility criteria for our study: (i) recently tested for an STI or HIV and (ii) at least 15 years of age. Reminder invitations were sent 2, 5 and 8 days later. The survey landing page included necessary information for informed consent, with proceeding to the survey taken as indication of consent. A $20 gift card was provided as an honorarium on completion of the survey. As surveys were sent to email addresses specific to each participant, duplicate participation was prevented.
Survey instrument
We reviewed the literature to summarise known barriers to and facilitators of STBBI testing and identified those potentially mitigated by a web-based testing service. From this work, and in consideration of health equity-based and socioecological approaches to sexual health and prior research by our team,11 13 15 21–23 we developed a multilevel framework for testing barriers and facilitators to inform our survey. This framework was centred on (i) the individual, (ii) the interaction between individuals and testing providers, (iii) the testing clinic and (iv) social and structural factors (including socio-demographics). For each level, we identified variables of interest and found suitable validated questions or developed new questions.
The initial baseline survey was developed using a secure installation of FluidSurveys (http://www.fluidsurveys.com), and was tested for usability and functionality by members of the study team. The resulting survey was piloted with 16 individuals, including 13 provincial STI clinic clients and 3 individuals who had participated in usability testing of the GCO programmes, and revised accordingly. The survey was available in English only. The final survey included 105 items in total (one per page) and used adaptive questioning to reduce the number of items for completion by each participant based on responses to previous questions. The survey was divided into five sections used to indicate progression through the survey, and participants had the ability to go backwards and forwards in the survey to review or edit answers, and could save answers and continue the survey at a later date. With the exception of questions using Likert scale responses, questions included options such as ‘I don’t know’ or ‘prefer not to say’ to minimise missing responses.
Analysis
We first determined potential recruitment biases among STI clinic and GCO clients. For the provincial STI clinic client sample, we extracted key demographic and sexual behaviour data for all clients receiving an STBBI test during the recruitment period from the common electronic medical record of this clinic. We compared characteristics of those consenting and not consenting to be contacted for research, and, among those consenting and invited, characteristics of participants and non-participants in the survey. A similar analysis was conducted for the GCO client sample, using data that were collected through use of the GCO programme. Bivariate comparisons were conducted using χ2, Fisher’s exact or t-test as appropriate (level of significance set at P<0.05). All available data for each comparison were used. Analyses were conducted in R V.3.2.2.24
Survey data were extracted from FluidSurveys and imported into SPSS V.14 for analysis. We conducted descriptive and bivariate analyses using χ2 analysis for categorical or ordinal variables, and t-tests for continuous variables. Due to the number of comparisons conducted, we set the level of significance at P<0.01.
Results
During the study period, 100/381 (26%) of the GCO clients who were tested also consented to be contacted for research, and all were invited to participate in the survey (figure 2). A greater proportion of GCO clients consenting to be contacted for research were men who have sex with men (MSM; table 1); however, the 73/100 (73%) GCO clinic clients participating in the survey included proportionately fewer MSM than non-participants. For provincial STI clinic clients, 811/3955 (21%) who were tested for STBBI consented to research, all of whom were invited; consenting clients were younger, included more homosexual or bisexual-identified persons, included fewer men and non-indigenous non-Caucasian persons and had a higher proportion that had tested for HIV. The 321/811 (40%) provincial STI clinic clients participating in the survey included proportionately fewer men than non-participants. The final clinic sample contained 321 participants.
Figure 2.
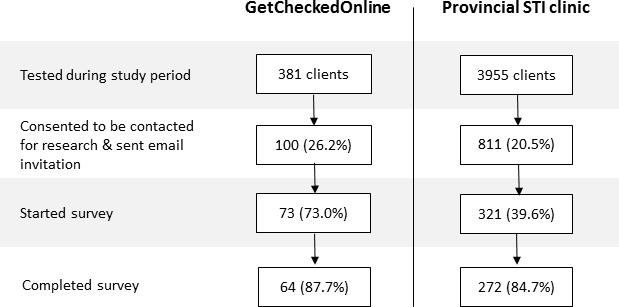
Recruitment outcomes for GetCheckedOnline.com (GCO) and clinic clients. Percentages calculated using denominator from previous step.
Table 1.
Comparison of client characteristics by two-stage recruitment for the provincial STI clinic and GetCheckedOnline samples
| Client characteristics† | Consented to be contacted for research‡ | Not consented to be contacted for research‡ | Participated | Did not participate |
| GetCheckedOnline sample (n) | 100 | 281 | 73 | 27 |
| Age: median (range) | 35 (19–58) | 32 (17–72) | 35 (19–58) | 36 (23–55) |
| Male gender | 67/100 (67%) | 203/281 (72%) | 45/73 (62%) | 22/27 (81%) |
| Indigenous | 2/98 (2%) | 3/269 (1%) | 2/71 (3%) | 0/27 (0%) |
| Non-indigenous, non-Caucasian | 25/98 (26%) | 70/269 (26%) | 18/71 (25%) | 7/27 (26%) |
| Man who has sex with men | 48/100 (48%) | 81/281 (29%)* | 29/73 (40%) | 19/27 (70%)* |
| Woman who has sex with women | 4/100 (4%) | 12/281 (4%) | 2/73 (3%) | 2/27 (7%) |
| 4+ partners (3 months) | 29/93 (31%) | 67/268 (25%) | 19/68 (28%) | 10/25 (40%) |
| Tested for HIV | 94/100 (94%) | 266/281 (95%) | 68/73 (93%) | 26/27 (96%) |
| Symptoms of an STI | 11/97 (11%) | 54/275 (20%) | 8/71 (11%) | 3/26 (12%) |
| Contact of partner with STI | 8/94 (9%) | 25/276 (9%) | 5/68 (7%) | 3/26 (12%) |
| No previous STI/HIV test | 4/100 (4%) | 31/281 (11%) | 3/73 (4%) | 1/27 (4%) |
| Positive result (any STBBI) | 3/100 (3%) | 8/281 (3%) | – | – |
| Provincial STI clinic sample (n) | 811 | 3144 | 321 | 490 |
| Age: median (range) | 30 (17–77) | 32 (13–92)* | 30 (18–74) | 30 (17–77) |
| Male gender | 469/811 (58%) | 2175/3144 (69%)* | 159/321 (50%) | 310/490 (63%)* |
| Indigenous | 5/506 (1%) | 34/2177 (2%) | 4/222 (2%) | 1/284 (0.4%) |
| Non-indigenous, non-Caucasian | 129/506 (25%) | 831/2177 (35%)* | 47/222 (21%) | 87/284 (29%) |
| Homosexual or bisexual | 130/573 (23%) | 431/2380 (18%)* | 63/242 (26%) | 67/331 (20%) |
| Number partners (6 months): median (range) | 2 (0–100) | 2 (0–300) | 2 (0–30) | 2 (0–100) |
| Tested for HIV | 698/811 (86%) | 2594/3144 (83%)* | 286/321 (89%) | 412/490 (84%) |
| Positive result (any STBBI) | 63/811 (8%) | 249/3144 (8%) | – | – |
* P<0.05, statistical comparisons between invited versus not invited, and participants versus non-participants.
†Data extracted from two administrative data systems, with varying patient-level variables available for analysis in each dataset meaning direct comparisons between datasets not always possible.
‡All clients who consented to be contacted for research were invited to participate.
STBBI, sexually transmitted and bloodborne infections.
Based on survey data, a considerable proportion of clients were aware of or had used both services. Almost half of the clinic clients were aware of GCO prior to taking the survey (133/321, 41%) with 22 (7%) participants having previously created an account or tested through GCO. A smaller proportion of GCO clients (22/73, 30%) were known to have previously tested at the provincial STI clinic. GCO clients were less likely to still be waiting for a test result at the time of the survey (1/73 (1%) vs 38/308 (12%) clinic clients, P=0.005).
We found few differences in individual-level barriers and facilitators of testing (see online supplementary table). Only 1 of 14 questions related to technological skills and access differed between groups, with GCO clients more commonly valuing being able to access online health resources (48/58 (83%) vs 136/231 (59%), P=0.001). We observed no differences in testing history or pattern, although more GCO clients reported their reason for last test as a routine test than clinic clients (48/72 (67%) vs 125/321 (39%), P<0.0001). A greater proportion of clinic clients reported testing due to symptoms or being a contact of a person with an STI (8/72 (11%) vs 99/321 (31%), P=0.001).
sextrans-2017-053325supp002.pdf (126.2KB, pdf)
Overall, more GCO clients reported delays in testing in the past year for any reason compared with clinic clients (54/71 (76%) vs 159/294 (54%), P=0.001). We found that more GCO clients reported barriers related to interactions with testing providers, including feeling uncomfortable discussing their sexual history where they usually go for healthcare (27/70 (39%) vs 57/258 (22%), P=0.005) and with healthcare providers in general (13/70 (19%) vs 15/290 (5%), P<0.0001) as well as worrying about being judged by a healthcare provider when providing a sexual history (21/70 (30%) vs 42/289 (15%), P=0.002). At a clinic level, we found more GCO clients reported delaying testing in the past year due to distance to a clinic (20/71 (28%) vs 26/294 (9%), P<0.0001) and fewer GCO clients agreed that the last time they tested at a clinic they found the clinic hours convenient (41/70 (59%) vs 221/286 (77%), P=0.001) or that they found it easy to make an appointment (33/67 (49%) vs 189/285 (66%), P=0.009). A greater proportion of GCO clients agreed that they had to wait a long time to see a doctor or nurse (35/70 (50%) vs 48/286 (17%), P<0.0001).
At the social and structural level, GCO clients were older (median 35 vs 30 years, P=0.001) and a greater proportion were GBMSM (31/69 (45%) vs 48/295 (16%), P<0.0001). More GCO clients agreed that it was embarrassing to test for an STI or HIV (11/68 (16%) vs 18/286 (6%), P=0.008).
Discussion
We found that a greater proportion of clients testing through GCO reported delays in testing over the past year and reported barriers related to accessing clinic-based services and to interactions with healthcare providers, as expected.11 17 However, although we had anticipated that users of GCO would be more likely to be technologically skilled and greater adopters of technology, this was not the case in our study. Youth are popularly perceived to be ‘digital natives’ and more accepting of new health technologies; our findings support others’ challenging of this assumption, given that GCO clients were significantly older than STI clinic clients.25
Given the potential for internet-based sexual health interventions such as GCO to exacerbate existing health inequities if used preferentially by individuals with sufficient resources to access existing health services,26 we were encouraged to see few differences in socio-demographics between GCO and clinic clients. We did find a significantly higher proportion of GBMSM among GCO clients. GBMSM have been demonstrated to be highly accepting of internet-based sexual health interventions,27 and we previously found high intention to use a hypothetical internet-based testing service among a large national sample of GBMSM.16 However, it is also possible that the higher proportion of GBMSM observed may reflect the targeting of social marketing efforts to this population during the recruitment period. We did not see significant differences in testing history, including proportion of first-time testers. GCO users were more likely to identify routine testing as their reason for testing, which may be related to convenience, often considered to be one of the biggest benefits of internet-based testing programmes. However, these results may also be a function of the GCO programme itself as individuals with symptoms or sexual contacts of a person with an STBBI are recommended to present to a clinic for testing (which may explain the higher frequency of these reasons for testing in the clinic group and higher diagnosis rate).
Our natural experiment study unfolded during the pilot phase of GCO implementation (a period when small but increasing uptake occurred). This limited our sample size of GCO users, and in combination with the characteristics of the internet-based service (eg, no verification of client identifiers used, promotion to hard-to-reach populations), precluded using conventional experimental methodologies or sampling techniques (eg, cohort studies, registry-based or population-based sampling). However, by using a concurrently recruited sample from an STI clinic where GCO had been promoted, we aimed to improve the comparability of these samples. We did find differences in recruitment outcomes between GCO and clinic client samples that may have affected our findings in unknown ways. Volunteer bias may have influenced the findings as GCO clients might have been more motivated than clinic testers to respond to the survey after experiencing satisfaction with the reduction of testing barriers. Experiencing a positive or negative STBBI test result could also influence survey participation; however, while GCO and clinic clients consenting and not consenting to be contacted by research did not differ by positivity rate, we were unable to compare positivity rates between participants and non-participants. Furthermore, the STI clinic clients were recruited from a low-threshold service where clients can test without using their real name, which may have conservatively minimised differences in experiences of testing barriers between the two groups (in this same survey, 80% of clinic clients were very satisfied with their testing experience (data not shown)). We also acknowledge that of necessity to survey GCO clients, our study involved a web-based survey which required sufficient digital literacy to complete; this may have limited our ability to detect differences in technological skills and access.26 As others have noted, the rigorous evaluation of digital health interventions is difficult and multimethod, interdisciplinary research approaches are recommended. This study is one part of our larger multimethod programme of research to evaluate the impact of GCO, including conducting interviews with GCO users, and community surveys of GBMSM in Vancouver that may help to further validate these findings.7
As client characteristics, test outcomes and follow-up may differ between testing settings, this study fills an identified critical gap—the lack of comparison between users of internet-based STBBI testing programmes and users of existing face-to-face testing services.28 Few comparative studies of users and non-users of internet-based testing programmes have been performed. Studies of a registry-based online chlamydia screening programme in the Netherlands compared users with non-users, finding non-users to have different demographic characteristics, to be less sexually active, have lower perceived risk of infection and lack privacy to check results at home.29 30 A Swedish study surveyed users of an online testing service and users of other web portals, finding similar rates of internet use.31 Finally, a US study found higher chlamydia positivity among women accessing self-collection kits online compared with women visiting family planning clinics.32
Overall, our findings suggest that internet-based STBBI testing services such as GCO may be of benefit to individuals experiencing barriers to accessing STBBI testing, without exacerbating existing inequities in testing access. Our findings are likely generalisable to internet-based testing programmes involving specimen submission at a laboratory in urban areas with accessible, low-threshold clinic-based testing services. The clinic-based testing barriers reported by GCO clients in our study could be addressed by expanded availability of testing services. However, other reported barriers such as discomfort discussing sexual history, fear of judgement and embarrassment with testing reflect broader system issues such as stigma or the appropriateness and safety of clinical services. These barriers are not easily addressed and require long-term societal and structural changes, demonstrating the potential importance of internet-based STBBI testing programmes on increasing test uptake. These findings provide the initial steps towards understanding the potential contribution of internet-based STBBI testing services as part of a spectrum of testing services needed to provide quality sexual healthcare across diverse client groups.33 Further comparative research in different settings, populations and with different types of internet-based testing programmes such as home self-collection or self-testing kits is needed.
Key messages.
The role of internet-based STI testing services on reducing inequities in testing access in comparison to clinic-based services has not been well understood to date.
GetCheckedOnline.com (GCO) is a comprehensive internet-based STI testing service where clients print a lab form and submit specimens at a private laboratory, getting results online or by phone.
Clients of GCO were more likely than STI clinic clients to report past difficulties in testing access (eg, long wait times) and interactions with providers (eg, discomfort with discussing sexual history).
In an urban setting, use of internet-based testing services may not be patterned on social gradients, technological access or literacy.
Further research on the role played by internet-based STI testing services is needed, particularly in suburban, rural and remote areas where clinical testing services may be less accessible.
Acknowledgments
The authors acknowledge the contributions of Dr Robert Balshaw and Mark Bondyra at BCCDC for their advice on statistical analysis and implementation of recruitment strategies, respectively. They also like to acknowledge the contributions of Cathy Chabot and Anna Carson, Youth Sexual Health Team, University of British Columbia in developing the survey instrument.
Footnotes
Handling editor: Jackie A Cassell
Contributors: MG led all aspects of this study and manuscript preparation. MG, KT, TS, DH, CKF, GO and JS contributed to overall study design, analysis and interpretation of study findings. PK, MK and CB are knowledge users and contributed to interpretation of study findings. All authors have reviewed and contributed to the submitted manuscript.
Funding: Funding for this study was provided by the Canadian Institutes of Health Research (grants PHE-114129, PHE-318068) which played no other role in this study.
Competing interests: MK has received contract or grant funding to his institution from Roche, Merck, Hologic, Boehringer Ingelheim, and Siemens that was unrelated to this work.
Ethics approval: University of British Columbia Research Ethics Board (number H11-01168).
Provenance and peer review: Not commissioned; externally peer reviewed.
Correction notice: This paper has been amended since it was published Online First. There was an error in Figure 2 and this has been replaced with an updated version.
References
- 1. Rietmeijer CA, McFarlane M. STI prevention services online: moving beyond the proof of concept. Sex Transm Dis 2008;35:770–1. 10.1097/OLQ.0b013e318180280d [DOI] [PubMed] [Google Scholar]
- 2. McFarlane M, Bull SS. Use of the internet in STD/HIV prevention Behavioral Interventions for Prevention and Control of Sexually Transmitted Diseases. US: Springer, 2007:214–31. [Google Scholar]
- 3. Gaydos CA, Dwyer K, Barnes M, et al. Internet-based screening for Chlamydia trachomatis to reach non-clinic populations with mailed self-administered vaginal swabs. Sex Transm Dis 2006;33:451–7. 10.1097/01.olq.0000200497.14326.fb [DOI] [PubMed] [Google Scholar]
- 4. Mann TA, Uddin Z, Hendriks AM, et al. Get Tested Why Not? A novel approach to internet-based chlamydia and gonorrhea testing in Canada. Can J Public Health 2013;104:205–9. 10.17269/cjph.104.3684 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Estcourt CS, Gibbs J, Sutcliffe LJ, et al. The eSexual Health Clinic system for management, prevention, and control of sexually transmitted infections: exploratory studies in people testing for Chlamydia trachomatis. Lancet Public Health 2017;2:e182–e190. 10.1016/S2468-2667(17)30034-8 [DOI] [PubMed] [Google Scholar]
- 6. Rotblatt H, Montoya JA, Plant A, et al. There’s no place like home: first-year use of the ‘I Know’ home testing program for chlamydia and gonorrhea. Am J Public Health 2013;103:1376–80. 10.2105/AJPH.2012.301010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Gilbert M, Haag D, Hottes TS, et al. Get Checked… Where? The Development of a Comprehensive, Integrated Internet-Based Testing Program for Sexually Transmitted and Blood-Borne Infections in British Columbia, Canada. JMIR Res Protoc 2016;5:e186 10.2196/resprot.6293 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Levine DK, Scott KC, Klausner JD. Online syphilis testing--confidential and convenient. Sex Transm Dis 2005;32:139–41. 10.1097/01.olq.0000149783.67826.4d [DOI] [PubMed] [Google Scholar]
- 9. Koekenbier RH, Davidovich U, van Leent EJ, et al. Online-mediated syphilis testing: feasibility, efficacy, and usage. Sex Transm Dis 2008;35:764–9. 10.1097/OLQ.0b013e31816fcb0a [DOI] [PubMed] [Google Scholar]
- 10. Tate DF, Finkelstein EA, Khavjou O, et al. Cost effectiveness of internet interventions: review and recommendations. Ann Behav Med 2009;38:40–5. 10.1007/s12160-009-9131-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Hottes TS, Farrell J, Bondyra M, et al. Internet-based HIV and sexually transmitted infection testing in British Columbia, Canada: opinions and expectations of prospective clients. J Med Internet Res 2012;14:e41 10.2196/jmir.1948 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Lorimer K, McDaid L. Young men’s views toward the barriers and facilitators of Internet-based Chlamydia trachomatis screening: qualitative study. J Med Internet Res 2013;15:e265 10.2196/jmir.2628 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Shoveller J, Knight R, Davis W, et al. Online sexual health services: examining youth’s perspectives. Can J Public Health 2012;103:14–18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Tomnay JE, Bourke L, Fairley CK. Exploring the acceptability of online sexually transmissible infection testing for rural young people in Victoria. Aust J Rural Health 2014;22:40–4. 10.1111/ajr.12077 [DOI] [PubMed] [Google Scholar]
- 15. Farrell J, Hottes TS, Haag D, et al. , 2015. Health equity and BritishColumbia’s GetCheckedOnline program: How can we make an online testing servicefor sexually transmitted infections that works for everyone? Gay and Lesbian Medical Association 33rd Annual Conference, Portland, Oregon. [Google Scholar]
- 16. Gilbert M, Hottes TS, Kerr T, et al. Factors associated with intention to use internet-based testing for sexually transmitted infections among men who have sex with men. J Med Internet Res 2013;15:e254 10.2196/jmir.2888 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Gilbert M, Hottes TS, Chabot C, et al. , 2013. "There are a million scenarios to consider": Health care provider perspectives on internet-based testing for sexually transmitted infections, HIV and hepatitis C in British Columbia. STI & AIDS World Congress, Vienna, Austria [Google Scholar]
- 18. Rogers E, Singhal A, Quinlan M. Diffusion of innovations: an integrated approach to communication theory and research. 2 ed New York, London: Routledge, 2008. [Google Scholar]
- 19. Eysenbach G. Improving the quality of Web surveys: the Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J Med Internet Res 2004;6:e34 10.2196/jmir.6.3.e34 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Gilbert M, Salway T, Haag D, et al. Use of GetCheckedOnline, a comprehensive web-based testing service for sexually transmitted and blood-borne infections. J Med Internet Res 2017;19:e81 10.2196/jmir.7097 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Shoveller J, Johnson J, Rosenberg M, et al. Youth’s experiences with STI testing in four communities in British Columbia, Canada. Sex Transm Infect 2009;85:397–401. 10.1136/sti.2008.035568 [DOI] [PubMed] [Google Scholar]
- 22. Rusch M, Shoveller J, Burgess S, et al. Association of sexually transmitted disease-related stigma with sexual health care among women attending a community clinic program. Sex Transm Dis 2008;35:553–7. 10.1097/OLQ.0b013e3181685855 [DOI] [PubMed] [Google Scholar]
- 23. Goldenberg S, Shoveller J, Koehoorn M, et al. Barriers to STI testing among youth in a Canadian oil and gas community. Health Place 2008;14:718–29. 10.1016/j.healthplace.2007.11.005 [DOI] [PubMed] [Google Scholar]
- 24. R: A language and environment for statistical computing.R Foundation for Statistical Computing; 2017. [Google Scholar]
- 25. Neil S. The digital native – myth and reality. Aslib Proceedings 2009;61:364–79. [Google Scholar]
- 26. Phelan JC, Link BG, Tehranifar P. Social conditions as fundamental causes of health inequalities: theory, evidence, and policy implications. J Health Soc Behav 2010;51 (Suppl):S28–S40. 10.1177/0022146510383498 [DOI] [PubMed] [Google Scholar]
- 27. Mimiaga MJ, Fair AD, Tetu AM, et al. Acceptability of an internet-based partner notification system for sexually transmitted infection exposure among men who have sex with men. Am J Public Health 2008;98:1009–11. 10.2105/AJPH.2006.098467 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Wilson E, Free C, Morris TP, et al. Can Internet-Based Sexual Health Services Increase Diagnoses of Sexually Transmitted Infections (STI)? Protocol for a Randomized Evaluation of an Internet-Based STI Testing and Results Service. JMIR Res Protoc 2016;5:e9 10.2196/resprot.4094 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Op de Coul EL, Götz HM, van Bergen JE, et al. Who participates in the Dutch Chlamydia screening? A study on demographic and behavioral correlates of participation and positivity. Sex Transm Dis 2012;39:97–103. 10.1097/OLQ.0b013e3182383097 [DOI] [PubMed] [Google Scholar]
- 30. Greenland KE, Op de Coul EL, van Bergen JE, et al. Acceptability of the internet-based Chlamydia screening implementation in the Netherlands and insights into nonresponse. Sex Transm Dis 2011;38:1–74. 10.1097/OLQ.0b013e318204546e [DOI] [PubMed] [Google Scholar]
- 31. Novak D, Novak M. Use of the Internet for home testing for Chlamydia trachomatis in Sweden: who are the users? Int J STD AIDS 2012;23:83–7. 10.1258/ijsa.2011.011030 [DOI] [PubMed] [Google Scholar]
- 32. Gaydos CA, Barnes M, Aumakhan B, et al. Chlamydia trachomatis age-specific prevalence in women who used an internet-based self-screening program compared to women who were screened in family planning clinics. Sex Transm Dis 2011;38:74–8. 10.1097/OLQ.0b013e3182039d7f [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Wellings K, Mehl GL, Free CJ. eSexual health interventions: promising, but more evidence needed. Lancet Public Health 2017;2:e162–e163. 10.1016/S2468-2667(17)30051-8 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
sextrans-2017-053325supp001.jpg (1.2MB, jpg)
sextrans-2017-053325supp002.pdf (126.2KB, pdf)