

Abstract
Introduction:
Previous Canadian epidemiologic studies have identified associations between occupations and prostate cancer risk, though evidence is limited. However, there are no well-established preventable risk factors for prostate cancer, which warrants the need for further investigation into occupational factors to strengthen existing evidence. This study uses occupation and prostate cancer information from a large surveillance cohort in Ontario that linked workers’ compensation claim data to administrative health databases.
Methods:
Occupations were examined using the Occupational Disease Surveillance System (ODSS). ODSS included 1 231 177 male workers for the 1983 to 2015 period, whose records were linked to the Ontario Cancer Registry (OCR) in order to identify and follow up on prostate cancer diagnoses. Cox proportional hazard models were used to calculate age-adjusted hazard ratios and 95% CI to estimate the risk of prostate cancer by occupation group.
Results:
A total of 34 997 prostate cancer cases were diagnosed among workers in ODSS. Overall, elevated prostate cancer risk was observed for men employed in management/ administration (HR 2.17, 95% CI = 1.98–2.38), teaching (HR 1.99, 95% CI = 1.79–2.21), transportation (HR 1.20, 95% CI = 1.16–1.24), construction (HR 1.09, 95% CI = 1.06–1.12), firefighting (HR 1.62, 95% CI = 1.47–1.78), and police work (HR 1.20, 95% CI = 1.10–1.32). Inconsistent findings were observed for clerical and farming occupations.
Conclusion:
Associations observed in white collar, construction, transportation, and protective services occupations were consistent with previous Canadian studies. Findings emphasize the need to assess job-specific exposures, sedentary behaviour, psychological stress, and shift work. Understanding specific occupational risk factors can lead to better understanding of prostate cancer etiology and improve prevention strategies.
Keywords: occupation; prostate cancer; surveillance; Ontario, cohort; compensation claims
Highlights
This is the first large occupational surveillance study in Ontario that links workers’ compensation claims to administrative health data.
We found increased risks of prostate cancer in white collar, transportation, construction, and protective services workers and mixed findings in clerical and farming workers.
Findings are consistent with recent published Canadian studies on occupation and prostate cancer.
Future studies need to address jobspecific exposures and examine other factors of shift work, stress, sedentary behaviour, and screening patterns.
Introduction
In Canada, prostate cancer is the most commonly diagnosed cancer among men.1,2 Aside from the few established non-modifiable risk factors of age, family history of prostate cancer, and ethnicity, there are no well-established modifiable risk factors for prostate cancer.1,2 Prostate cancer risk increases with age, especially after the age of 50 years.1 African American men are known to have the highest rates of prostate cancer and are more likely to be diagnosed at advanced stages of prostate cancer than other men.3,4 Men with a family history of prostate cancer are also at an increased risk, and are more likely to seek out prostate cancer screening.5 There is also growing evidence that men who are obese or overweight have an increased risk of prostate cancer and this may be related to dietary factors and physical inactivity.6 There is also some evidence that consumption of processed or red meat may lead to an increased risk of prostate cancer.7 Prostate-specific antigen (PSA) screening behaviours among men may also contribute to differences observed in prostate cancer risk.8-10 As there continues to be limited understanding on modifiable risk factors for prostate cancer, there is a need to investigate other factors, like occupation.
Work-related risk factors for prostate cancer have been increasingly suggested as recent Canadian studies have shown consistent associations between employment in broad occupational groups and prostate cancer risk. Associations have been observed for management and administration, farming, construction, transportation, and protective services occupations.5,11-14 It has been hypothesized that prostate cancer risk in these occupations is linked to factors such as sedentary behaviour, stress, shift work, whole body vibrations, and chemical exposures (ex. pesticides and diesel exhaust).15-21 The International Agency for Research on Cancer (IARC) has reported that there is some limited evidence for associations between prostate cancer risk and rubber production industries, cadmium and arsenic metals, malathion, and x and gamma radiation exposures.22
Prostate cancer is expected to remain the most common cancer in Canadian men in the coming decades.2 As working adult men spend a substantial part of their lives at work, occupational risk factors may be important determinants of prostate cancer risk. Improved occupational prostate cancer surveillance is crucial to identifying and reducing work-related risks for prostate cancer. The Occupational Disease Surveillance System (ODSS) was developed as the first surveillance system of its kind in Ontario to link worker compensation claims to administrative health databases to identify and monitor trends in work-related disease.23,24 The ODSS linkage was developed for surveillance of multiple occupational diseases, including prostate cancer. Unlike previous population- level studies, ODSS narrows the focus to a large cohort of Ontario’s working population.
The purpose of this study was to identify associations between occupation and prostate cancer in Ontario using ODSS. This study aims to determine whether previous findings from epidemiologic population studies in Canada are also observed in this study and to explore new associations.
Methods
ODSS was created through the linkage of multiple administrative health databases in Ontario. The system can be used to detect risk of disease, including cancers, among Ontario workers, which provides valuable information on work-related diseases.
Specifically, a cohort of Ontario workers was derived from Workplace Safety and Insurance Board (WSIB) accepted losttime compensation claims data. The WSIB provides mandatory coverage to 70–76% of workers and provides workers’ compensation to those with accepted occupational- related injury/illness claims.25 The remaining workers who are not covered by WSIB are self-employed individuals not opting for coverage, financial and entertainment workers, and other groups.25WSIB records from 1983 to 2014 were eligible for linkage, and these records contained information specific to the claim (date of injury, occupation/industry at time of claim, nature of injury) and personal information (worker name, sex, date of birth, and death date (if applicable)). Occupation associated with the claim was coded by the WSIB according to the Canadian Classification Dictionary of Occupations (CCDO 1971).
WSIB records (n = 2 253 734 unique workers) were linked, through a series of deterministic and probabilistic linkages, to the Ontario Health Insurance Plan’s (OHIP) Registered Persons Database (RPDB) (1990– 2015) (n = 16 162 277), which contains information on sex, residence, birthdate, death date or emigration (if applicable), and health insurance number (HIN).23,24 Records were excluded if they were missing sex or date of birth, were under the age of 15 years, had an invalid claim date, or were missing valid occupation or industry codes, resulting in a total of 2 190 246 unique workers in the cohort.23,24 Workers were then deterministically linked to the Ontario Cancer Registry (OCR) using HINs where available (n = 1 796 731), but also probabilistically linked where no HIN was available, by use of name, sex, birthdate, and death date (n = 393 515).24 The OCR provides information on Ontario incident cancer cases (1964–2016) collected from hospital records, pathology reports, cancer center records, and death certificates. As a result, 214 821 unique workers were linked to cancer diagnoses in the OCR.23,24 Follow-up time commenced from the date of the first claim and for this analysis, ODSS cohort members were followed up in the OCR for diagnosis of prostate cancer (International Statistical Classification of Diseases and Related Health Problems, 10th revision, C61). Workers with a prostate cancer diagnosis in the OCR that preceded entry into the ODSS cohort were excluded to establish a prostate cancer free cohort. Workers were followed from cohort entry until prostate cancer diagnosis, emigration from Ontario, death, or the end of the study period (December 31, 2016).23,24 A full description of the linkage methods can be found elsewhere.24
Cox proportional hazard models were used to calculate age-adjusted hazard ratios and 95% confidence intervals (CI) to estimate the risk of prostate cancer for each occupation. Workers with more than one claim record could appear in multiple occupation groups. For each analysis, the occupation group of interest was compared to all other workers in the cohort. Previously, different reference groups were considered (e.g., white-collar jobs) and analyses were restricted to specific age groups with increased prostate cancer development (> 50 years), however no significant changes were observed in the results (results not shown). The occupation groups (CCDO 1971) are presented at division (2-digit), major (3-digit), and minor (4-digit) levels. We conducted the analyses using statistical package SAS version 9.4 (SAS institute Inc., Cary, NC, USA).
In this analysis, occupation groups were examined based on a priori or suspected groups of interest stemming from the IARC evaluation and previous Canadian studies. These groups include agriculture and farming, management/administrative and related, transportation, construction, and protective services.5,11-14 Since ODSS is a newly established system, testing its ability to detect consistent risks among the a priori or suspected groups supports its use as a reliable and valid surveillance system.
This study was approved by the University of Toronto Health Sciences Research Ethics Board (protocol reference #27513).
Results
The ODSS cohort consisted of 1 231 177 male workers with a mean age at cohort entry of 37.4 years. During the cohort time period, 70% had only one accepted timeloss claim. Prostate cancer was the most commonly diagnosed cancer in the ODSS cohort, with a total of 34 997 incident prostate cancer cases identified, as shown in Table 1. The average follow-up time for occupation by division, major, or minor levels was 261 person-months.
Table 1. ODSS cohort distribution by birth year.
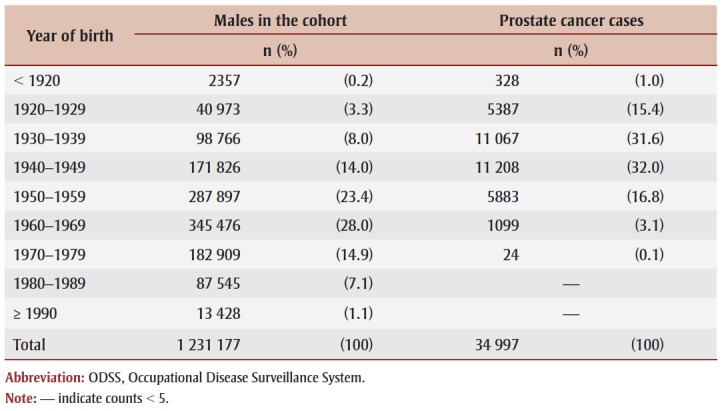 |
Table 2 presents the number of prostate cancer cases and risk estimates by occupation division. A priori and suspected occupation groups that showed elevated risks in the ODSS include management/ administrative, teaching, construction trades, and transportation equipment operating. Decreased risks were observed among two suspected at-risk a priori groups, namely, agriculture and forestry/ logging. Other associations were observed for natural sciences and engineering, medicine and health, service, mining and quarrying, processing, machining, product fabricating/assembling/repair, material handling, and other crafts/equipment operating occupation groups.
Table 2. Risk of prostate cancer by occupation division group in ODSS.
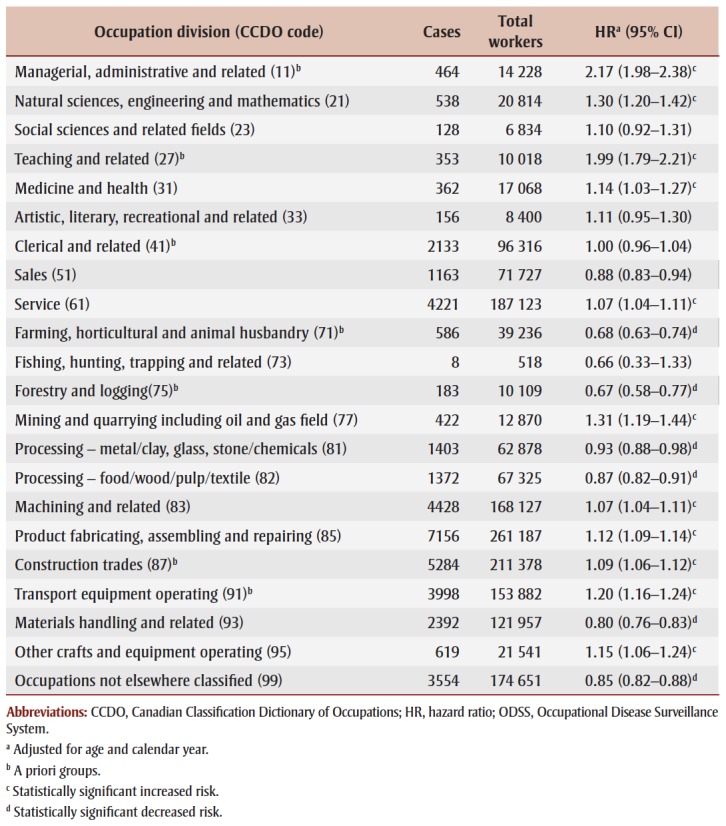 |
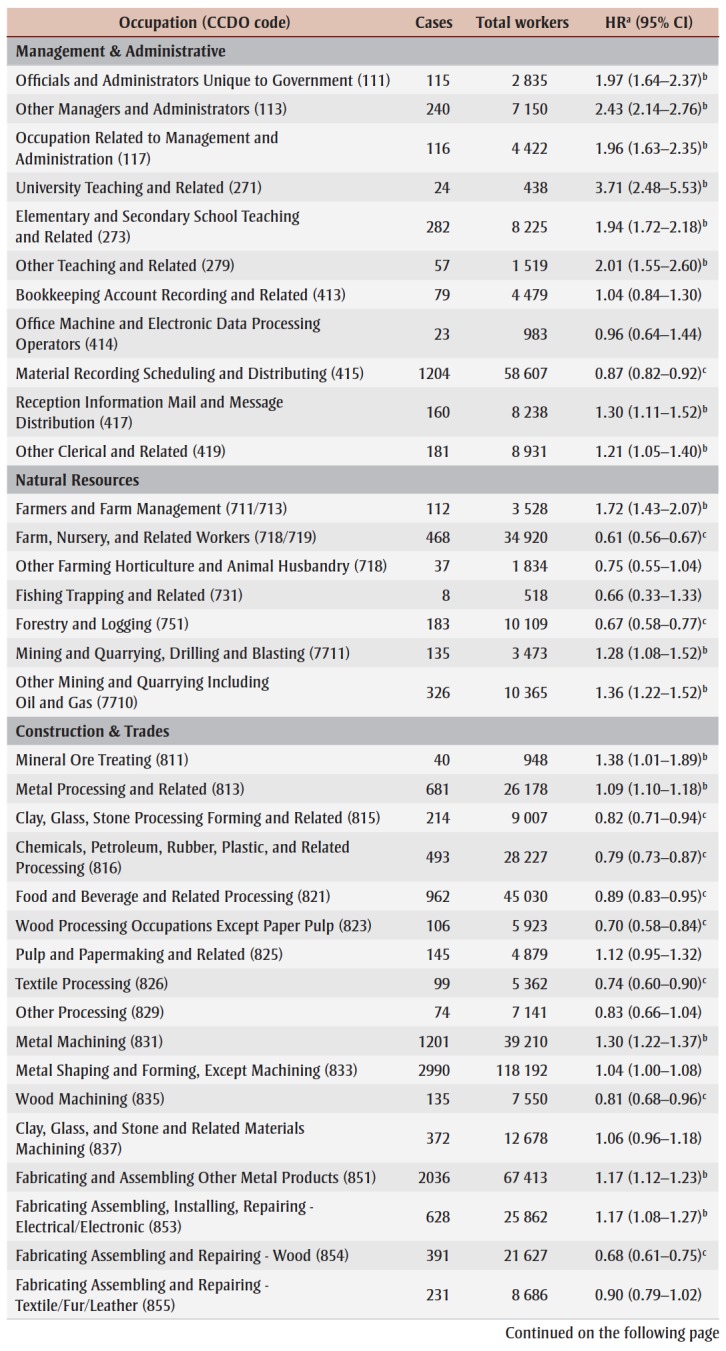
Table 3 reports the number of prostate cancer cases and risk estimates for major occupation groups (3-digit CCDO code) and some minor occupation groups (4-digit CCDO code) with a priori or suspected associations. Complete minor group-level results are presented in a supplementary Table (S1) available upon request from the authors.
Table 3. Risk of prostate cancer for selected a priori major occupation groups in ODSS.
|
Management and administration
Increased risks were observed across all major level management and administrative, teaching, and several non-managerial clerical occupation groups (Table 3). A more than 70% increased risk was observed for the major level teaching-related occupation, with the highest risk observed among university teachers at a minor level (S1).
Natural resources
An increased risk was observed in the overall major group of farmers and farm managers (Table 3), and at a minor level, this was specific to a small group of farmers (S1). However, a decreased risk was observed in the major group of farm, nursery, and related work (Table 3), and this was driven by farm workers (S1). Decreased risks in forestry and logging were primarily driven by workers employed in timber cutting and to a lesser degree, workers in laboring and elemental work (S1). Increased risks in mining and quarrying related occupations were observed across all minor level mining and quarrying occupations (S1).
Construction and trades
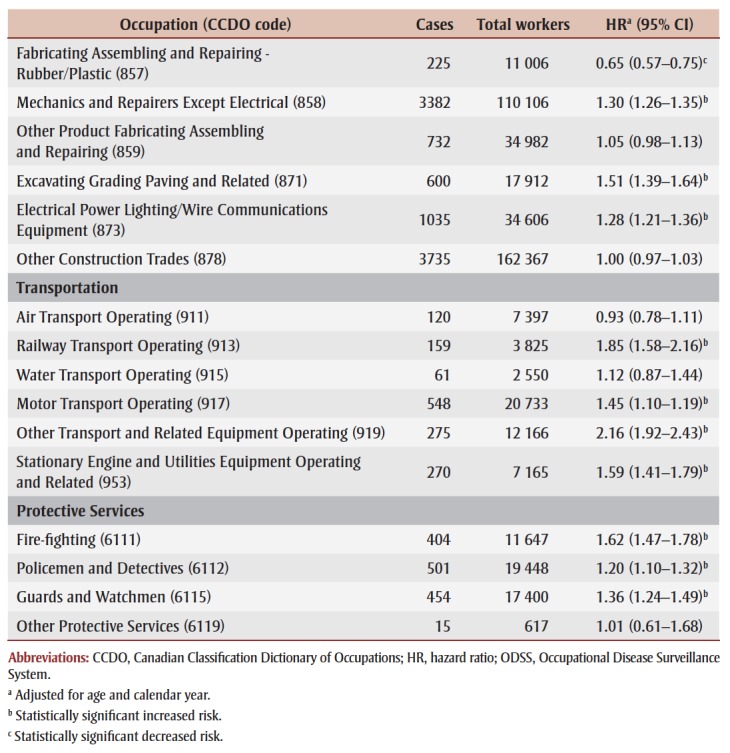
Increased risks were observed for metal related occupations such as metal processing, metal machining, metal shaping and forming, and fabricating and assembling other metal products; all groups which had large numbers of prostate cancer cases at a major level (Table 3). At a minor level, a number of these metal related occupations with many prostate cancer cases were also elevated: metal processing foremen, metal rolling, metal machining foremen, tool and die making, machinists, metal shaping and forming foreman, forging, boil-makers, and sheet metal workers (S1). An increased risk was also observed in the major group of mechanics and repairers which had one of the highest numbers of prostate cancer cases among the construction occupations (Table 3). Almost all minor groups under mechanics and repairers showed increased risks for prostate cancer, primarily driven by many prostate cancer cases in motor vehicle and industrial/farm/construction machinery occupations (S1). Several construction occupations at a major level were also observed as decreased risks: non-metal product processing, food and beverage processing, wood processing, textile processing, wood machining, and fabricating/assembling/repair of wood, rubber, and plastic (Table 3).
Transportation
Multiple transportation occupations at a major level were observed to be associated to prostate cancer, with increased risks across railway transport operating, motor transport operating, other transport and related operating, and stationary engine and utilities operating (Table 3). For railway transport, all minor level groups demonstrated increased risks, however these groups had small numbers of prostate cancer cases. All minor level motor transport occupations also showed increased risks, primarily driven by many cases in truck and bus driving (S1).
Protective services
Increased risks of prostate cancer were observed across firefighters, policemen and detectives, and guards and watchmen (Table 3).
Other occupations
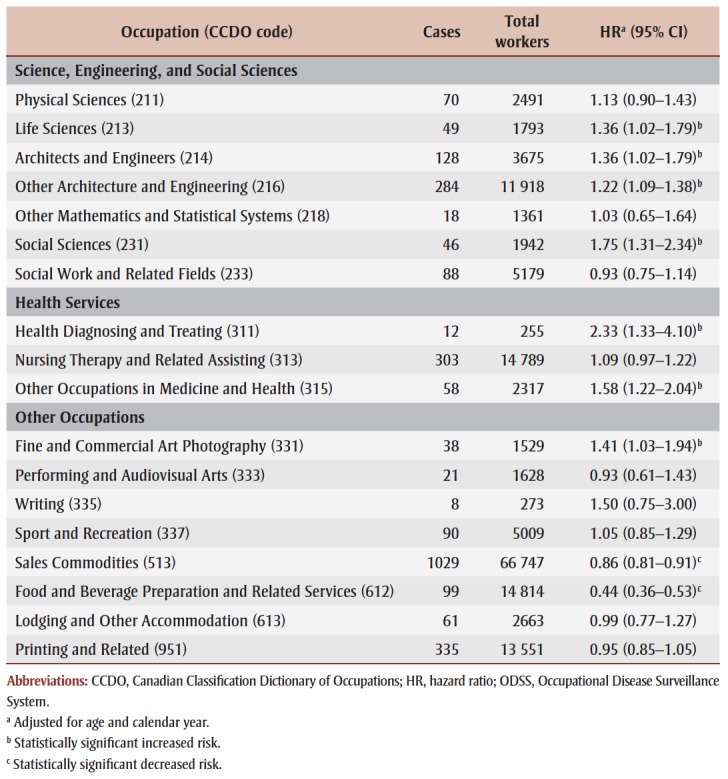
Table 4 presents risk estimates for other major occupation groups where excesses were observed at the division level (Table 2) and were not considered a priori or suspected groups of interest. Mainly, men employed in major occupational groups related to science/engineering/social sciences (life sciences, architecture and engineering) and health services (health diagnosing, nursing, other health occupations) were observed to have increased risks of prostate cancer (Table 4).
Table 4. Risk of prostate cancer for other major occupation groups in ODSS.
 |
Discussion
As in the general population, prostate cancer was the most common cancer diagnosed among men in the ODSS cohort. Consistent with a priori suspected associations and with recent published Canadian studies, this study observed an excess risk for prostate cancer among white collar, transportation, construction, and protective services occupations and for some clerical and farming occupations.5,11-13 Findings from this large study of more than 1.2 million male workers in Ontario strengthen previous findings. Occupational associations observed in this study may be driven by several work-related factors such as sedentary behaviour/low physical activity, psychological stress, shift-work, wholebody vibrations, and specific chemical exposures.
Previous studies have suggested that sedentary behaviour or low occupational physical activity may be linked to increased prostate cancer risk.26 A meta-analysis that included 19 cohort studies and 24 case-control studies observed a 19% reduction in prostate cancer risk related to occupational physical activity.27 Although the biological mechanism linking physical inactivity to prostate cancer is not clear, it is speculated that decreased physical activity may influence prostate cancer risk through changes in testosterone levels immune function, and insulin-like growth factors.27 Increased prostate cancer risks previously observed among white collar and administrative occupations have been commonly attributed to sedentary behavior, as there are few hazardous chemical exposures involved in these occupations.5,11-13 Our findings in managerial and administrative work may be explained by increased sedentary behaviour and low occupational physical activity. Men employed in managerial level positions are also likely to be older with higher education and experience, however we were able to adjust for age. Also, these workers tend to have a higher socioeconomic status (SES) when compared to blue collar workers, and a higher SES has been linked to increased use of health services and possible early diagnosis of prostate cancer (e.g., increased PSA screening), which may play a role in our findings.5,28 On the other hand, decreased risks identified in blue collar workers (e.g., farming, forestry and logging, and some construction trades) in our study may be linked to the increased occupational physical activity in these workers, compared to white collar workers. Transportation workers, specifically truck and bus drivers identified in our study, may also experience long periods of sitting or sedentary behaviour. Previous studies in Ontario saw no association with physical activity level in these workers.11,15 However, few studies in the literature have shown that increased occupational sedentary behaviour in transport drivers is also related to shift work, obesity, and low physical activity during nonwork hours.29,30
Psychological stress has been found to have an important impact on health conditions, with increased risks for cardiovascular disease and mental illness, but there is growing interest for its role in cancer etiology.31 Chronic stress may impact cancer development with activation of the sympathetic nervous system leading to downregulation of cellular immune response and promoting genomic instability. There is also some evidence that chronic stress can influence testosterone levels contributing to prostate cancer development.31The main source of stress in men is workplace stress, and few studies have been able to assess workplace stress and prostate cancer risk. Workplace stress is categorized by the balance of demand and control, with high stress environments involving high demand and low control.31
This is important in occupations identified in our study, such as firefighting and police work, which are recognized as high risk professions where workers are required to respond to a range of emergencies in consistent high stress environments. 32 But there is also the perception of stress, if the worker perceives their job to be of high stress compared to other workers. Some studies have reported that higher stress levels were often reported among white-collar workers when compared to blue collar workers.31,33 Workplace stress may be a contributor to increased risks identified in white collar workers in our study. Workplace stress has also been associated to increased unhealthy lifestyle factors such as physical inactivity, obesity, increased alcohol use, and smoking.7
Recent meta-analyses on shift work and prostate cancer suggest that night and rotating shift work is associated with prostate cancer risk.19,34,35 Shift work can lead to the suppression of melatonin synthesis which leads to the disruption of the circadian rhythm.35-37 Melatonin is recognized as an important contributor to preventing cancer development,19 but with the suppression of melatonin through increased shift work, there may be an increase in testosterone levels leading to increased prostate cancer risk.19 This is relevant across some occupations identified in this study that involve shift work, such as transportation, protective services, and health care occupations. Transportation drivers, specifically truck drivers identified in our study, may be likely to work night shifts or irregular hours.29,30 Shift work has also been shown among protective services occupations in firefighting and police work.38,39 Increased prostate cancer risks observed in health care occupations, specifically in nursing occupations, could be related to shift work as previous studies have established an association between nursing occupations, shift work, and breast cancer risk.36,37
Whole body vibration (WBV) is a common exposure in occupations involving repetitive vehicle or machine use, such as in transportation and construction jobs. Exposure to WBV occurs when mechanical energy from vibrating surfaces is passed to the body either in standing or sitting positions.40 Although the role of WBV in prostate cancer etiology remains unclear, other prostate conditions like prostatitis and increasing testosterone levels have been linked to WBV exposure.40Transportation workers in railway transportation, truck driving, motor transport operating, equipment operating, and stationary engine equipment operating had excess risks in our study similar to previous studies, which all involve WBV exposure.10,15-17,40-42 Construction workers involved in machinery related work requiring the use of hand tools may be exposed to whole body vibrations as well, however it is unclear which construction occupations involve WBV in our study.
Our study findings may also be related to specific chemical exposures. An increased risk in farmers and farm management may be linked to pesticide exposure, which has been consistently shown in the previous literature.43-45 Also, some agriculture studies have shown associations in men with a family history of prostate cancer and exposure to specific pesticides.46,47Farming workers may also be exposed to diesel exhaust, similar to workers in construction, transportation, mining, and protective services.11-13,43-45,48 These workers may be exposed through the use of diesel emitting vehicles or by working near them for long periods of time.43-45,48 Diesel exhaust exposure is also common in forestry and logging occupations, however decreased risks were observed for these groups in our study. There is evidence that cadmium and arsenic metal compounds are linked to prostate cancer risk based on IARC evaluations.25 However, in this study it was not possible to narrow down occupations by specific metal exposures, though we observed increased risks across different construction metal–related occupations. Increased risks were also observed among mechanics and repairmen, and these workers may be exposed to chemical agents such as solvents, iron and steel metals, and welding equipment.49
Screening behaviours may also contribute to prostate cancer risk differences observed in occupation groups in our study. It is well known that the PSA test is the only available screening test for prostate cancer. However, it is non-specific and can lead to false-positives and additional unnecessary testing.28,50 Routine prostate cancer screening is not recommended in Canada,50 but there are screening related factors that may influence screening behaviours in men. Previous evidence has shown that men of older age, with higher SES, family history of prostate cancer, and those who are married are more likely to get screened than other men.14,28,44 Also, men employed in white collar jobs have been shown to have better awareness, accessibility, and flexibility to seek out prostate cancer screening which may explain some of the increased risks identified in these occupations.10,28 Decreased risks identified in blue collar jobs of construction, farming, forestry, and logging may be related to decreased prostate cancer screening, based on lower SES, less flexible working hours, and less awareness of screening resources.10 Protective services workers, specifically firefighting, may have more frequent medical exams than other professions, given the nature of these occupations, resulting in increased screening behaviours.51,52 Excess risks observed in engineering and social sciences in our study have also been reported in the literature with the suggestion that these men are more likely to get screened for prostate cancer when compared to other men.5,10 Also, our findings in health care workers may indicate increased screening in these workers, as they are more likely to be informed on available medical tests.
There were limitations with this study. Although occupational information was collected at the time of claim, no lifetime work history was available. We also did not have the ability to examine occupation- related factors such as duration of employment. Only workers with a losttime compensation claim were included in this cohort, which over represents workers in physically hazardous occupations compared to the broader workforce since most accepted claims are for workplace injuries. Although this cohort includes many Ontario workers, it may not represent all individuals in the identified occupations and this could lead to selection bias, if risk factors associated with prostate cancer are correlated with physical hazards. All analyses were conducted within the cohort, such that both the target group and reference are formerly injured workers, which may offset this bias. Workers in particularly high hazard occupations, may also have an increased risk of death, which could remove them from follow-up prior to the age when they are at high risk of prostate cancer. While adjusting for age may address this, its impact could only be fully assessed using a competing risk model.
Due to the nature of how the cohort is constructed, people in senior level positions may have a higher level of risk attributed to them because of exposure under prior work duties, such as a manager who was a former worker. This may also occur simply because people had to be older in order to achieve that position, such as judges, and prostate cancer is a disease of old age. All analyses were age adjusted, which should at least partially mitigate potential bias, but caution should be used in interpreting excess risks in these groups. Also, the administrative databases used in this study did not capture information on socioeconomic (e.g., income, education), lifestyle, or known prostate cancer risk factors, aside from age, which could act as potential confounders and could help to alleviate some of the selection bias. This study also uses multiple testing which can lead to chance findings, a common issue with occupational studies looking at multiple groups. However, our study results were quite similar to previous publications, providing confidence in our findings. A major strength of this study is that it uses a linkage- based approach with accurate and updated administrative health data. Another major strength is the use of compensation claims data which provided vital and accurate employment information. The linkage-based approach is efficient for identifying a large sample of prostate cancer cases with occupational information prior to diagnosis. Also, comparisons were restricted to a cohort of workers rather than the general population which reduces the potential impact of the healthy worker effect.
Conclusion
This study identified associations between occupation and prostate cancer risk similar to a priori or suspected associations recognized in previous Canadian studies. Findings included associations in management/ administrative, construction, transportation, and protective services occupations and prostate cancer risk. There were also other associations that warrant further investigation. There is a continued need to examine potential job-specific exposures and other factors such as sedentary behaviour, stress, shift work, and screening patterns, among other non-occupational factors. Understanding specific work-related factors will help determine how the identified jobs are related to prostate cancer risk. This can lead to improved knowledge on prostate cancer risk factors and evidence-based prevention strategies.
Acknowledgements
This project was funded by the Ministry of Labour (No. 14-R-29) and the Public Health Agency of Canada (No. 1516-HQ- 000066). The Occupational Cancer Research Centre is supported from core funding from Cancer Care Ontario, the Canadian Cancer Society and the Ontario Ministry of Labour.
Conflicts of interest
None to declare.
Authors’ contributions and statement
JS, the primary author, contributed to the design and conceptualization of the work, data analysis, interpretation of the data, drafting and revising of the paper. JSM contributed to the acquisition of the data, design and conceptualization of the work, data analysis, and revising of the paper. CBM and AP contributed to the interpretation of the data and revising of the paper. PAD contributed to the acquisition of the data, design and conceptualization of the work, interpretation of the data, and revising of the paper.
The content and views expressed in this article are those of the authors and do not necessarily reflect those of the Government of Canada.
References
- GLOBOCAN 2018: estimated cancer incidence, mortality and prevalence worldwide in 2018 [Internet] IARC. 2018:estimated cancer incidence, mortality and prevalence worldwide in 2018 [Internet]. Available from: http://globocan.iarc.fr/Pages/fact_sheets_cancer.aspx. [Google Scholar]
- CCS. Toronto(ON): 2018. Prostate cancer statistics [Internet] Available from: http://www.cancer.ca/en/cancer-information/cancer-type/prostate/statistics/?region=on. [Google Scholar]
- Bashir MN, et al. Epidemiology of prostate cancer. Asian Pacific Journal of Cancer Prevention. 2015;16((13)):5137–41. doi: 10.7314/apjcp.2015.16.13.5137. [DOI] [PubMed] [Google Scholar]
- Mordukhovich I, Reiter PL, Backes DM, et al, et al. A review of African American-white differences in risk factors in cancer: prostate cancer. Cancer Causes Control. 2011;22((3)):341–57. doi: 10.1007/s10552-010-9712-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sauve JF, Lavoue J, Parent ME, et al. Occupation, industry and the risk of prostate cancer: a case-control in Montréal, Canada. Environmental Health. 2016;15((1)):100–57. doi: 10.1186/s12940-016-0185-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Diet, nutrition, physical activity, and prostate cancer [Internet] WCRF. 2014 Available from: https://www.wcrf.org/sites/default/files/Prostate-Cancer-2014-Report.pdf. [Google Scholar]
- Report of the advisory group to recommend priorities for IARC monographs during 2015-2019 [Internet] IARC. 2014 [Google Scholar]
- Pukkala E, Martinsen JI, Lynge E, et al, et al. Occupation and cancer – follow-up of 15 million people in five Nordic countries. Acta Oncologica. 2009;48((5)):646–790. doi: 10.1080/02841860902913546. [DOI] [PubMed] [Google Scholar]
- Rundle A, Neckerman KM, Sheehan D, et al, et al. A prospective study of socioeconomic status, prostate cancer screening and incidence among men at high risk for prostate cancer. Cancer Causes Control. 2014;24((2)):297–303. doi: 10.1007/s10552-012-0108-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Krstev S, Baris D, Stewart PA, et al, et al. Risk for prostate cancer by occupation and industry: a 24-state death certificate study. American Journal of Industrial Medicine. 1998:413–20. doi: 10.1002/(sici)1097-0274(199811)34:5<413::aid-ajim1>3.0.co;2-r. [DOI] [PubMed] [Google Scholar]
- Sritharan J, Demers PA, Harris SA, et al, et al. Natural resource-based industries and prostate cancer risk in Northeastern Ontario: a case-control study. Occupational and Environmental Medicine. 2016:506–11. doi: 10.1136/oemed-2016-103573. [DOI] [PubMed] [Google Scholar]
- Sritharan J, Demers PA, Harris SA, et al, et al. Occupation and risk of prostate cancer in Canadian men: a case-control study across eight Canadian provinces. Cancer Epidemiology. 2017:96–103. doi: 10.1016/j.canep.2017.04.006. [DOI] [PubMed] [Google Scholar]
- Sritharan J, MacLeod J, Harris S, et al, et al. Prostate cancer surveillance by occupation and industry: the Canadian census health and environment cohort (CanCHEC) Cancer Medicine. 2017;7((4)):1468–78. doi: 10.1002/cam4.1358. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zeegers MP, Friesema IH, Goldbohm R, et al, et al. A prospective study of occupation and prostate cancer risk. Zeegers MP, Friesema IH, Goldbohm R, et al. 2004;46((3)):271–9. doi: 10.1097/01.jom.0000116961.48464.6b. [DOI] [PubMed] [Google Scholar]
- Kortsak AM, Purdham JT, Kreiger N, et al, et al. Occupational risk factors for prostate cancer. American Journal of Industrial Medicine. 2007;50((8)):568–76. doi: 10.1002/ajim.20495. [DOI] [PubMed] [Google Scholar]
- Mayton AG, Jobes CC, Gallagher S, et al. Assessment of whole-body vibration exposures and influencing factors for quarry haul truck drivers and loader operators. International Journal of Heavy Vehicle Systems. 2014;21((3)):241–61. doi: 10.1504/IJHVS.2014.066080. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carex Canada. Vancouver(BC): 2016. Diesel engine exhaust [Internet] Available from: https://www.carexcanada.ca/en/diesel_engine_exhaust/ [Google Scholar]
- Lewis-Mikhael AM, Bueno-Cavanillas A, Guiron TO, et al, et al. Occupational exposure to pesticides and prostate cancer: a systematic review and meta-analysis. Occupational and Environmental Medicine. 2016:134–44. doi: 10.1136/oemed-2014-102692. [DOI] [PubMed] [Google Scholar]
- Rao D, Yu H, Bai Y, et al, et al. Does night-shift work increase the risk of prostate cancer. Onco Targets Ther. 2015 doi: 10.2147/OTT.S89769. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crompton S, et al. Statistics Canada. Ottawa(ON): 2011. What's stressing the stressed. [Google Scholar]
- John EH, Schwartz GG, Koo J, et al, et al. Sun exposure, vitamin D receptor gene polymorphisms, and risk of advanced prostate cancer. Cancer Research. 2005;65((12)):5470–9. doi: 10.1158/0008-5472.CAN-04-3134. [DOI] [PubMed] [Google Scholar]
- List of classifications by cancer sites with sufficient or limited evidence in humans, Volume 1 to 118*. IARC. 2017 Available from: https://monographs.iarc.fr/wp-content/uploads/2018/07/Table4.pdf. [Google Scholar]
- MacLeod J, McLeod C, Peter A, et al, et al. 033-5 Developing an occupational disease surveillance system: detecting work-related risks through the linkage of administrative databases. Occup Environ Med. 2016:A62–9. [Google Scholar]
- Feinstein SG, Lazgare LP, et al, et al. Examining lung cancer risks across different industries and occupations in Ontario, Canada: the establishment of the occupational disease surveillance system. Occupational and Environmental Medicine. 2018:543–4. doi: 10.1136/oemed-2017-104926. [DOI] [PubMed] [Google Scholar]
- AWCBC. Toronto(ON): 2017. Canadian workers' compensation system – year at a glance [Internet] Available from: http://awcbc.org/?page_id=11803. [Google Scholar]
- Dosemeci M, Hayes RB, Vetter R, et al, et al. Occupational physical activity, socioeconomic status, and risks of 15 cancer sites in Turkey. Cancer Causes Control. 1993 doi: 10.1007/BF00051333. [DOI] [PubMed] [Google Scholar]
- Liu Y, Hu F, Li D, et al, et al. Does physical activity reduce the risk of prostate cancer. European Urology. 2011:1029–44. doi: 10.1016/j.eururo.2011.07.007. [DOI] [PubMed] [Google Scholar]
- Wallner LP, Sarma AV, Lieber MM, et al, et al. Psychosocial factors associated with an increased frequency of prostate cancer screening in men ages 40-70: the Olmsted county study. Cancer Epidemiol Biomarkers Prev. 2008;17((12)):the Olmsted county study–44. doi: 10.1158/1055-9965.EPI-08-0050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Varela-Mato V, Yates T, Stensel DJ, et al, et al. Time spent sitting during and outside working hours in bus drivers: a pilot study. Preventative Medicine Reports. 2016 doi: 10.1016/j.pmedr.2015.11.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gilson ND, Bush RA, et al, et al. Patterns and perceptions of physical activity and sedentary time in male transport drivers working in regional Australia. Australian and New Zealand Journal of Public Health. 2014;38((4)):314–20. doi: 10.1111/1753-6405.12214. [DOI] [PubMed] [Google Scholar]
- Blanc-Lapierre A, Rousseau MC, Parent ME, et al. Perceived workplace stress is associated with an increased risk of prostate cancer before age 65. Perceived workplace stress is associated with an increased risk of prostate cancer before age 65. Frontiers in Oncology. 2017 doi: 10.3389/fonc.2017.00269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jahnke SA, Poston WS, Haddock CK, et al, et al. Firefighting and mental health: experiences of repeated exposure to trauma. Work. 2016;53((4)):737–44. doi: 10.3233/WOR-162255. [DOI] [PubMed] [Google Scholar]
- Aginsky KD, Constantinou D, Delport M, et al, et al. Cardiovascular disease risk profile and readiness to change in blue- and white-collar workers. Cardiovascular disease risk profile and readiness to change in blue- and white-collar workers. Family & Community Health. 2017;40((3)):236–44. doi: 10.1097/FCH.0000000000000148. [DOI] [PubMed] [Google Scholar]
- Gan Y, Li L, Zhang L, et al, et al. Association between shift work and risk of prostate cancer: a systematic review and meta-analysis of observational studies. Carcinogenesis. 2018;39((2)):87–97. doi: 10.1093/carcin/bgx129. [DOI] [PubMed] [Google Scholar]
- Parent ME, El-Zein M, Rousseau MC, et al, et al. Night work and risk of cancer among men. American Journal of Epidemiology. 2012;176((9)):751–9. doi: 10.1093/aje/kws318. [DOI] [PubMed] [Google Scholar]
- Brudnowska J, Peplonska B, et al. Night shift work and cancer risk: a literature review. Medycyna Pracy. 2011;62((3)):323–38. [PubMed] [Google Scholar]
- He C, Anand SJ, Ebell EH, et al, et al. Circadian disrupting exposures and breast cancer risk: a meta-analysis. International Archives of Occupational and Environmental Health. 2014;88((5)):533–47. doi: 10.1007/s00420-014-0986-x. [DOI] [PubMed] [Google Scholar]
- Wirth M, Vena JE, Smith EK, et al, et al. The epidemiology of cancer among police officers. American Journal of Industrial Medicine. 2013;56((4)):439–53. doi: 10.1002/ajim.22145. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pukkala E, Martinsen JI, Weiderpass E, et al, et al. Cancer incidence among firefighters: 45 years of follow-up in five Nordic countries. Occupational and Environmental Medicine. 2014:398–404. doi: 10.1136/oemed-2013-101803. [DOI] [PubMed] [Google Scholar]
- Nadalin V, Kreiger N, Parent ME, et al, et al. Prostate cancer and occupational whole-body vibration exposure. Annals of Occupational Hygiene. 2012;56((8)):968–74. doi: 10.1093/annhyg/mes010. [DOI] [PubMed] [Google Scholar]
- Aronson KJ, Siemiatycki J, Dewar R, et al, et al. Occupational risk factors for prostate cancer: results from a case-control study in Montreal, Quebec, Canada. American Journal of Epidemiology. 1996;143((4)):363–73. doi: 10.1093/oxfordjournals.aje.a008750. [DOI] [PubMed] [Google Scholar]
- Jones MK, Harris MA, Peters PA, et al, et al. Prostate cancer and occupational exposure to whole-body vibration in a national population-based cohort study. American Journal of Industrial Medicine. 2014;57((8)):896–905. doi: 10.1002/ajim.22354. [DOI] [PubMed] [Google Scholar]
- Ragin C, Davis-Reyes B, Tadesse H, et al, et al. Farming, reported pesticide use, and prostate cancer. Ragin C, Davis-Reyes B, Tadesse H, et al. 2013;7((2)):102–9. doi: 10.1177/1557988312458792. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Parent ME, Desy M, Siemiatycki J, et al. Does exposure to agriculture chemicals increase the risk of prostate cancer among farmers. McGill Journal of Medicine. 2009;12((1)):70–7. [PMC free article] [PubMed] [Google Scholar]
- Sharma-Wagner S, Chokkalingam AP, Malker HS, et al, et al. Occupation and prostate cancer risk in Sweden. Sharma-Wagner S, Chokkalingam AP, Malker HS, et al. 2000;42((5)):517–25. doi: 10.1097/00043764-200005000-00010. [DOI] [PubMed] [Google Scholar]
- Mahajan R, Blair A, Lynch CF, et al, et al. Fonofos exposure and cancer incidence in the agriculture health study. Environmental Health Perspectives. 2006;114((12)):1838–42. doi: 10.1289/ehp.9301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Christensen CH, Platz EA, Andreotti G, et al, et al. Coumaphos exposure and incident cancer among male participants in the agriculture health study (AHS) Christensen CH, Platz EA, Andreotti G, et al. 2010;118((1)):92–96. doi: 10.1289/ehp.0800446. [DOI] [PMC free article] [PubMed] [Google Scholar]
- LeMasters GK, Genaidy AM, Succop P, et al, et al. Cancer risk among firefighters: a review and meta-analysis of 32 studies. Journal of Occupational and Environmental Medicine. 2006;48((11)):1189–202. doi: 10.1097/01.jom.0000246229.68697.90. [DOI] [PubMed] [Google Scholar]
- Gulden JW, Kolk JJ, Verbeek AL, et al. Work environment and prostate cancer risk. Prostate. 1995;27((5)):250–7. doi: 10.1002/pros.2990270504. [DOI] [PubMed] [Google Scholar]
- Bell N, Gorber SC, Shane A, et al, et al. Recommendations on screening for prostate cancer with the prostate-specific antigen test. Canadian Medical Association Journal. 2014;186((16)):1225–34. doi: 10.1503/cmaj.140703. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ontario Fire Administration. Ajax(ON): 2014. Medical screening [Internet] Available from: http://www.ofai.ca/ofai-candidate-testing-services/medical-assessment. [Google Scholar]
- Tsai RJ, Luckhaupt SE, Schumacher P, et al, et al. Risk of cancer among firefighters in California, 1988-2007. Tsai RJ, Luckhaupt SE, Schumacher P, et al. 2015;58((7)):715–29. doi: 10.1002/ajim.22466. [DOI] [PMC free article] [PubMed] [Google Scholar]