

Abstract
Scant research has explored place-based correlates of achieving and maintaining HIV viral load suppression among heterosexuals living with HIV. We conducted multilevel analyses to examine associations between United Hospital Fund (UHF)-level characteristics and individual-level viral suppression and durable viral suppression among individuals with newly diagnosed HIV in New York City (NYC) who have heterosexual HIV transmission risk. Individual-level independent and dependent variables came from NYC’s HIV surveillance registry for individuals diagnosed with HIV in 2009-2013 (N=3,159; 57% virally suppressed; 36% durably virally suppressed). UHF-level covariates included measures of food distress, demographic composition, neighborhood disadvantage and affluence, healthcare access, alcohol outlet density, residential vacancy, and police stop and frisk rates. We found that living in neighborhoods where a larger percent of residents were food distressed was associated with not maintaining viral suppression. If future research should confirm this is a causal association, community-level interventions targeting food distress may improve the health of people living with HIV and reduce the risk of forward transmission.
Keywords: Food distress, HIV viral suppression, heterosexuals, New York City, Place-based predictors
Introduction
Compared to men who have sex with men, heterosexuals are less likely to achieve and maintain HIV viral suppression (Crepaz et al., 2016; Hall et al., 2013). For example, an analysis of National HIV Surveillance System data found that 58% of people who had heterosexual contact as their transmission risk achieved and maintained suppression compared to 68% of men with a history of same-sex sexual contact (Crepaz et al., 2016). Large racial/ethnic inequities exist in both the prevalence of HIV among heterosexuals and in whether heterosexuals achieve suppression (Crepaz et al., 2016; Stone, 2012). Whereas 73% of White people living with HIV (PLWH) achieved and maintained suppression nationally, only 53% of Black, and 61% of Latino and other PLWH achieved suppression (Crepaz et al., 2016).
Studies of determinants of HIV viral suppression have largely focused on individual-level and interpersonal factors, including substance use (Arnsten et al., 2002); food security (Aranka Anema, Vogenthaler, Frongillo, Kadiyala, & Weiser, 2009; S. D. Weiser et al., 2009; Sheri D Weiser et al., 2012; S. D. Weiser et al., 2011);; trust in and rapport with one’s medical providers (Beach, Keruly, & Moore, 2006; Blackstock, Addison, Brennan, & Alao, 2012) and social support (Burgoyne, 2005). Recently, however, an emerging line of research has begun to investigate whether features of PLWH’s environments might shape suppression (Beattie, 2015; Eberhart et al., 2014; Jefferson et al., 2017a; Shacham, Lian, Onen, Donovan, & Overton, 2013; Wiewel, 2014). For example, Beattie (2015) found that neighborhood poverty rates were associated with decreased likelihood of viral suppression, although Weiwel (2014) found that neighborhood poverty was unrelated to time to viral suppression. A better understanding of whether and how environmental features affect HIV viral suppression could inform community-level interventions and policies that target place characteristics to interrupt transmission dynamics.
Methods
Overview and Units of Analysis
The present multilevel study explored relationships between select place characteristics and viral suppression among HIV-diagnosed heterosexuals in New York City (NYC). Food access environments, for example, could affect wellbeing by determining access to nutritious food (Walker et al., 2010). Sociodemographic composition could affect survival through the effects of structural racism, which shapes the availability and nature of neighborhood resources (e.g., safe public spaces, fire stations, or police presence) (Wallace, 1990). Wealth and neighborhood economic disadvantage could affect access to safe and healthy housing, social support, and freedom from violence (Katz, Hsu, Lingo, Woelffer, & Schwarcz, 1998). We also explored police use of Terry stops (“stop and frisk”)(“Terry v. Ohio,” 1968) as an exposure, conceptualizing it as a form of community violence that might adversely affect health-care seeking and immune response (Liebschutz et al., 2010; Woods et al., 2005). Critical race theory and social geography scholarship both suggest that people’s experience of, access to, and meanings of neighborhoods and neighborhood characteristics are racialized (Cooper, Arriola, Haardörfer, & McBride, 2016; Ford & Airhihenbuwa, 2010; Sewell, Massey, & Denton, 2010). Given this, and given large racial/ethnic disparities in suppression (Hess K, 2016; Singh et al., 2014), we explored whether individual race/ethnicity moderates relationships between place-based exposures and suppression.
This cross-sectional multilevel study had two units of analysis: individuals diagnosed with HIV and NYC’s United Hospital Fund (UHF) districts. UHFs are aggregations of adjacent ZIP codes that are relatively homogenous (Goranson C, 2009) (Figure 1). The NYC Department of Health and Mental Hygiene (NYC DOHMH) uses UHFs for planning purposes. In 2010, there were 42 UHF districts in NYC, and the median UHF adult population size was 128,117 (25th percentile=83,451; 75th percentile=162,871) (United States Census Bureau, 2010).
Fig. 1.
New York City’s 42 United Hospital Fund (UHF) Areas. Contains north arrow, legend, scale bar, and map of UHFs.
Demographic and medical data on individuals were drawn from the NYC DOHMH’s HIV surveillance registry. NYC DOHMH is authorized by the New York State Department of Health to conduct population-based NYC HIV/AIDS surveillance. Since 2000, all NYC diagnostic and clinical providers have been required to report new diagnoses of HIV to NYC DOHMH. Laboratories performing HIV-related tests for NYC providers must report positive HIV diagnostic tests, HIV viral loads, and other clinical indicators (e.g., CD4 counts) to NYC DOHMH. New York State, including NYC, began comprehensive electronic HIV laboratory reporting in 2005. The surveillance registry includes demographic characteristics, residential ZIP code, place of birth, and transmission risk information for each individual; these data are primarily extracted from medical chart reviews. In 2016, the NYC surveillance registry contained a cumulative total of >230,000 cases and >8 million laboratory reports.
To be included in the analytic sample, individuals (≥13 years old) had to be newly diagnosed with HIV between January 1, 2009 and December 31, 2013 and: identify as Black, White, or Hispanic/Latino; report heterosexual contact prior to HIV diagnosis; and live in a NYC UHF district at diagnosis. Heterosexual contact included persons who had heterosexual sex with a person they knew to be HIV-infected, an injection drug user, or a person who had received blood products. For females only, this also included history of sex work, multiple sex partners, sexually transmitted disease, crack/cocaine use, sex with a bisexual male, probable heterosexual transmission as noted in medical chart, or sex with a male and negative history of injection drug use. People were linked to UHF districts via their ZIP code of residence at diagnosis. Thirty individuals otherwise eligible lacked a ZIP code and were excluded.
Measures
Individual-Level Outcomes
This analysis had two binary HIV-related outcomes, viral suppression and durable viral suppression, both assessed at the individual level using NYC DOHMH HIV surveillance data. In accordance with the standardized cut-off used by the Centers for Disease Control (Centers for Disease Control and Prevention, 2016), we classified individuals as “virally suppressed” if they had ≤200 copies of HIV per mL of blood at any point within 12 months after their diagnosis. Individuals were classified as “durably virally suppressed” if, within 12 months after their diagnosis, they (A) had at least two suppressed (≤200 cc/mL) viral load tests that were at least 90 days apart from one another with no intervening unsuppressed (>200 cc/mL) viral load tests, and (B) had no unsuppressed viral load tests after they had achieved durable viral suppression. Because we defined suppression and durable suppression as individual-level attributes observed in the year following each person’s diagnosis, these outcomes were time invariant.
UHF-Level Predictors
As evident in Table 1, we used administrative data to create measures of eight domains of UHF-level predictors: food access environment, sociodemographic composition, stability, wealth, economic disadvantage, healthcare access, social disorder, and police stop-and-frisk rates.
Table 1.
Sources and methods used to measure characteristics of United Hospital Fund districts.
| Construct | Sources & operationalization |
|---|---|
| Food Access Environment | The percent of food-distressed residents was calculated from 2010 U.S. Department of Agriculture Food Access Research Atlas data (Food Access Research Atlas, 2010) as the percent of residents who were both low-income (< 200% of federal poverty limit) and who lived in a food desert area (> 0.5 mile from a large grocery store or supermarket). |
| Racial/Ethnic Composition | The percent of residents who self-identified a; non Hispanic Black/African-American was calculated using 2007–2011 American Community Survey (AG) data (U.S. Census Bureau’s American Community Survey Office, 2011). This variable was skewed, and therefore three categories reflecting its multimodal distribution were created based upon review of the variable’s distribution: low (<5% of residents were Black), medium (5–29%), and high (>30%). |
| Age composition | The percent of residents who were 21–54 years old was calculated using 2007–2011 ACS data (U.S. Census Bureau’s American Community Survey Office, 2011). |
| Residential Stability | We used principal components analysis (PCA) to create a dimension of neighborhood stability (see Appendix A for component loadings). Constituent variables were: the percent of residents residing in the same home as one year ago, from 2007–2011 ACS data (U.S. Census Bureau’s American Community Survey Office, 2011); and the male:female sex ratio for 18–64 year old non-institutionalized residents from 2010 decennial census data (United States Census Bureau, 2010). |
| Affluence | We used PCA to create a dimension of neighborhood affluence using 2007–2011 ACS data (U.S. Census Bureau’s American Community Survey Office, 2011). Constituent variables were: the percent of residents ≥25 years old who were college educated; the percent of high income households (> 400% of 2009 U.S, median household income); and the percent of expensive homes (> 400% of 2009 U.S. median home value) (see Appendix A). |
| Economic disadvantage | We used PCA to create a dimension of UHF-level economic disadvantage using 2007–2011 ACS data (U.S. Census Bureau’s American Community Survey Office, 2011) (see Appendix A). Constituent variables were UHF-level median income and the percentages of people aged >16 years in the civilian workforce who were unemployed; of individuals living at or below the federal poverty level; of households that had received public assistance in the last 12 months; and of adults >25 years old who did not have a high school degree/GED. |
| Healthcare access | We used PCA to create a dimension of poor access to healthcare, using pooled 2009 and 2010 NYC DOHMH Community Health Survey data, weighted to adjust for selection in both years (see Appendix A). Constituent variables were the percent of UHF residents without health insurance and the percent of UHF residents who reported an unmet need for health care in the last 12 months (New York City Department of Health and Mental Hygiene, 2009–2010). |
| Social disorder | To assess dimensions of social disorder we created measures of the number of businesses licensed to sell alcohol for off-premises consumption per square mile in 2009 (Keen, Dyer, Whitehead, &; Latimer, 2014; United States Census Bureau, 2009), and the number of residences that had once been occupied and now were empty per square mile in 2009 (United States Postal Service/Department of Housing and Urban Development, 2009). |
| Police stop and frisk rates | We used 2009 NYC Police Department Stop, Question, and Frisk (SQF) data to measure the rate of stops per 100,000 adult residents and the rate of stops without an arrest per 100,000 adult residents (New York Police Department, 2009). Both rates were skewed and three categories reflecting multimodal distributions were created for each variable, based upon each variable’s distribution. Stops per 100,000 adult residents were categorized: low (<4,000 stops without anest per 100,000 residents), medium (4,000-<20,000), and high (>20,000). Stops without an arrest per 100,000 adult residents were categorized: low (<6,000 stops without arrest per 100,000 residents), medium (6,000-<22,000), and high (≥22,000). |
Keen, Dyer, Whitehead, & Latimer, (2014)
New York City Department of Health and Mental Hygiene. (2009–2010).
New York Police Department (2009).
United States Census Bureau’s American Community Survey Office. (2011).
United States Census Bureau. (2009).
United States Census Bureau. (2010).
United States Postal Service/Department of Housing and Urban Development (2009).
Individual-Level Covariates
Data on individual-level covariates came from NYC DOHMH HIV surveillance. Sex, race/ethnicity, nativity (born within vs. outside U.S. and territories), lifetime history of homelessness at diagnosis, year of HIV diagnosis, and age at HIV diagnosis were abstracted from patient medical records. These variables were all time invariant.
Analysis
Because individuals from the surveillance registry were nested in UHFs, multilevel logistic models were used to analyze the associations of UHF-level predictors to individual-level suppression and durable suppression. Level 2 consisted of the 42 UHF districts and Level 1 consisted of individuals in the surveillance registry living in those districts. All normally distributed continuous variables were mean-centered for analysis. Parameters were estimated in SAS 9.3 software’s (SAS Institute, 2011) PROC GLIMMIX using maximum likelihood with Laplace approximation, random intercepts, a binomial distribution, a log link, and an unstructured error covariance matrix.
Model building proceeded in stages for viral suppression. In Stage 1, we built bivariate multilevel models to examine relationships of each predictor to viral suppression. In Stage 2, we extended the model to examine whether individual race/ethnicity (comparing Latino and White to Black heterosexuals) might moderate relationships of UHF-level predictors to viral suppression. In Stage 3, we built a multivariable viral suppression model consisting of UHF-level variables that were significant at p≤.15. These models included the following theoretically relevant individual-level variables: individual race/ethnicity, nativity, age at HIV diagnosis, and year of HIV diagnosis. We also conducted post-hoc analyses to explore interactions of individual race/ethnicity with UHF-level variables when these interactions were statistically significant. In Stage 4, we calculated Exploratory Population Attributable Risk percentages (e-PAR%) to estimate the percentage of people reaching suppression or durable suppression attributable to each significant place-based variable (Northridge, 1995). We call these exploratory PAR%s because PAR%s assume causal relationships, an assumption that we cannot make with our cross-sectional data. Stage 5 was a sensitivity analysis. Five UHFs had <10 residents who met the eligibility criteria for this study. We dropped these UHFs from our analysis to determine if the magnitude of effect estimates changed.
We repeated this five-stage process for the durable viral suppression outcome with minor modifications. In the Stage 3 analysis for this outcome, we included the following UHF-level variables, which were not statistically significant in bivariate models but were of theoretical interest: residential vacancy, neighborhood disadvantage, poor access to healthcare, and stops without arrest per resident. We had initially included these four variables in the viral suppression multivariable model, but this theoretically informed model did not converge, even after utilizing Newton-Raphson optimization methods (Hughes & Kearney, 2003), and so we dropped these covariates from the viral suppression model.
As an analysis of surveillance data, this can be considered an analysis of a population (rather than a sample) that has no sampling error. In such cases, researchers studying similar populations have used p-values as heuristic devices to avoid over-interpreting model parameters (Friedman et al., 2006). We follow this tradition here. We use p-value <.05 to determine the significance of variables, and consider p-values above .05 and at or below .10 as indicative of borderline or marginal statistical significance. We also follow the suggestion of epidemiologists to report relative risks, rather than odds ratios, as a more accurate and intuitive estimate of likelihood (Davies, Crombie, & Tavakoli, 1998).
Results
Between 2009 and 2013, 3,159 Black, Latino, or White heterosexuals who lived in one of the 42 UHF districts were diagnosed with HIV in NYC (Table 2), representing 19% of all incident cases between 2009 and 2013. Thirty-one percent were Latino, 63.85% were Black, and 5.06% were White. Fifty-seven percent of all newly diagnosed individuals in this analysis achieved HIV viral suppression within 12 months of diagnosis, but only 36.15% were durably suppressed during that period. Across the 42 UHFs viral suppression percentages ranged from 33.33% to 100% (Q1: 50, Q2: 55.55, Q3: 63.63; Figure 2) and durable viral suppression percentages ranged from 20% to 70% (Q1: 30.46, Q2: 35.55, Q3: 42.22; Figure 3).
Table 2.
Descriptive statistics for characteristics of 3,159 Black, White, and Latino newly HIV-diagnosed heterosexuals in New York City, and of the United Hospital Fund districts (UHFs; N = 42) where they lived at HIV diagnosis between 2009–2013a
| Variable UHF-level variables | Mean (StdErr/Std) | Median | 25th and 75th percentiles |
|---|---|---|---|
| Food access environment | |||
| Percent of resident who were food distressed | 2.60 (4.82) | 0.32 | 0.0, 3.20 |
| Demographic composition | |||
| Percent of residents who were non-Hispanic Black | 20.83 (3.33) | 11.367 | 3.07, 29.25 |
| Percent of residents who were 21–54 years dd | 51.39 (0.89) | 49.42 | 47.71, 54.19 |
| Social disorder | |||
| Alcohol outlet density | 51.55 (37.95) | 46.83 | 20.39, 67.81 |
| Residential vacancy (vacancies per sq mi) | 40.96 (4.29) | 35.20 | 19.69, 55.52 |
| Police Stop and Frisk | |||
| Stops without arrest per 100,000 residents | 12116.11 (10917.43) | 9489.81 | 30007.8, 17163.63 |
| Stability | |||
| Percent of residents in same home as 1 yr ago | 88.11 (4.60) | 88.77 | 86.90, 91.62 |
| Male: Female sex ratio (18–64 non-institutionalized) | 0.994 (0.012) | 0.998 | 0.9946,0.9996 |
| UHF stability component | 0 (4.61) | 0.70 | −1.23,3.53 |
| Affluence | |||
| Percent college educated (≥25 yo) | 20.40 (9.18) | 17.83 | 14.63, 26.19 |
| Percent high income households (≥400% 2009 US median) | 6.86 (7.89) | 3.83 | 2.18, 6.86 |
| Percent expensive homes(≥400% 2009 US median) | 51.55 (20.28) | 52.55 | 36.68, 69.08 |
| UHF neighborhood affluence component | 0 (1.61) | −0.28 | −0.84, 0.73 |
| Economic disadvantage | |||
| Median income (US dollars) | 57714.10 (3748.18) | 54629.50 | 38087.50, 74518.00 |
| Percent unemployed | 9.44 (0.47) | 8.90 | 7.40, 11.61 |
| Percent in poverty | 19.00(1.45) | 16.53 | 12.46, 26.77 |
| Percent on public assistance | 4.35 (0.47) | 3.23 | 2.23, 5.88 |
| Percent without a high school education | 20.38 (1.64) | 19.28 | 12.46, 25.97 |
| UHF economic disadvantage component | 0(2.09) | −0.03 | −1.33, 1.69 |
| Poor access to healthcare | |||
| Percent uninsured | 16.16 (1.05) | 15.14 | 12.41, 21.89 |
| Percent went without needed care | 11.46 (0.59) | 10.93 | 8.73, 14.63 |
| Poor access to healthcare component | 0 (0.07) | −0.01 | −0.05, 0.07 |
| Individual-level variables | N (%) | ||
| Sex | |||
| Female | 2471 (78.22) | ||
| Male | 688 (21.78) | ||
| Race/ethnicity | |||
| Hispanic/Latino | 982 (31.09) | ||
| Non-Hispanic White | 160 (5.06) | ||
| Non-Hispanic Black | 2017 (63.85) | ||
| Nativity | |||
| Foreign-born | 1275 (40.36) | ||
| Not foreign-born | 1884 (59.64) | ||
| History of homelessness | |||
| Yes | 96 (3.04) | ||
| No or unknown | 3063 (96.96) | ||
| Age at HIV diagnosis | |||
| 13–19 | 145 (4.59) | ||
| 20–29 | 638 (20.20) | ||
| 30–39 | 727(23.01) | ||
| 40–49 | 862 (27.29) | ||
| 50–59 | 555 (17.57) | ||
| 60+ | 232 (7.34) | ||
| Year of HIV diagnosis | |||
| 2009 | 774 (24.5) | ||
| 2010 | 681 (21.56) | ||
| 2011 | 661 (20.92) | ||
| 2012 | 559 (17.7) | ||
| 2013 | 484 (15.32) | ||
| Suppression status | |||
| Suppressed | 1788 (56.6) | ||
| Durably suppressed | 1142 (36.15) |
Untransformed variables reported
Fig. 2.
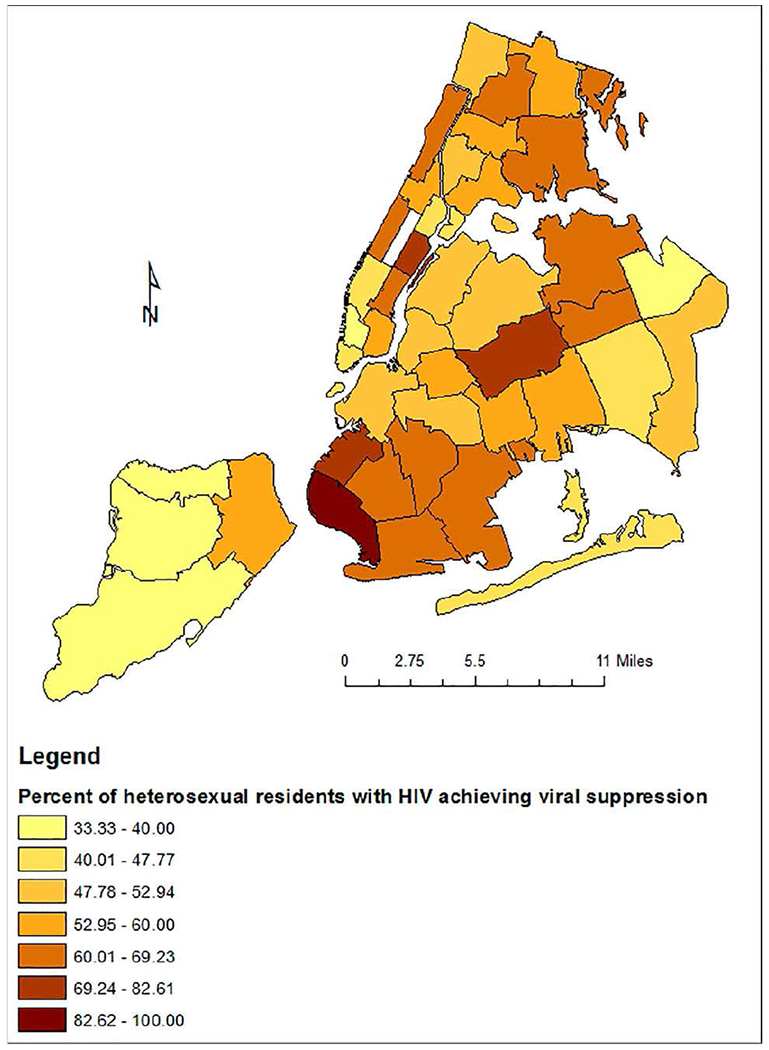
HIV Viral Suppression among Heterosexuals by UHF. Contains north arrow, legend, scale bar, and map of UHFs
Fig. 3.
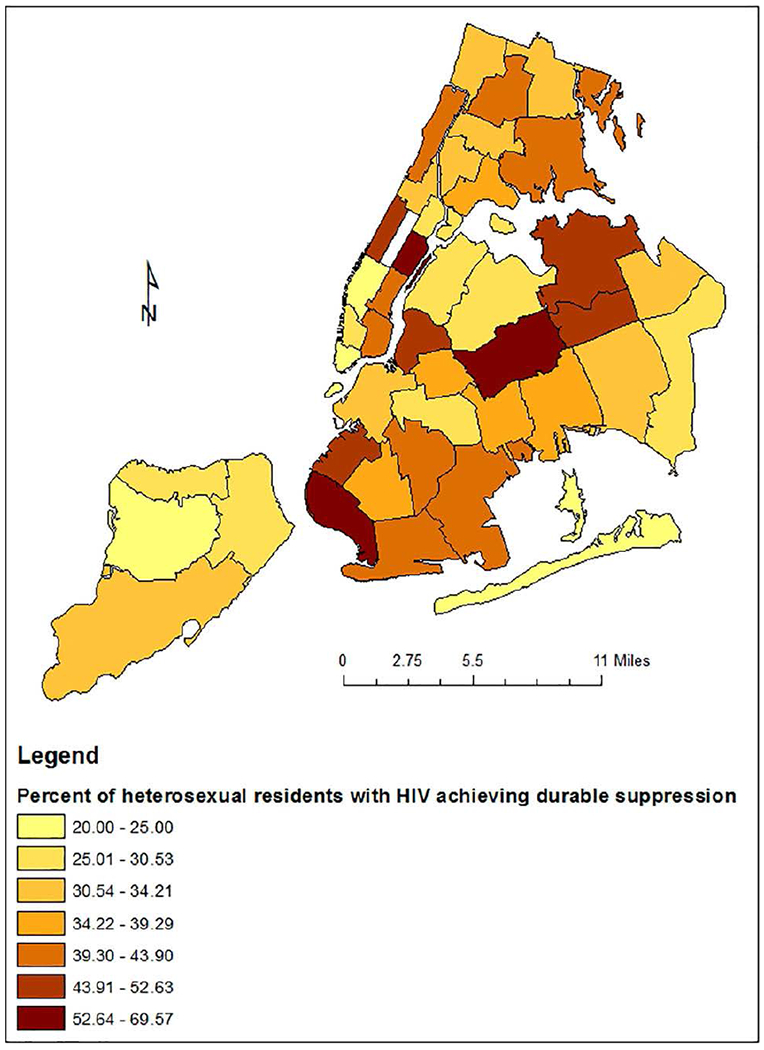
HIV Durable Suppression among Heterosexuals by UHF. Contains north arrow, legend, scale bar, and map of UHFs
In the 42 UHFs, the median percent of residents with low food access was 0.32% (25th percentile=0%; 75th percentile=3.20%). The median percent of residents who were Black was 11.37%, and varied substantially across UHFs (25th percentile=3.07%; 75th percentile=29.25%). See Table 2 for distributions of other UHF-level variables.
Viral Suppression
Multilevel models indicated that HIV-positive heterosexuals living in UHFs that had a larger percentage of food-distressed residents had a marginally significant lower likelihood of achieving viral suppression (Table 3). In the bivariate analysis, heterosexuals living in UHFs where less than 1% of residents were food distressed were 25% more likely to be suppressed than their counterparts living in UHFs where at least 5% of residents were food distressed (unadjusted relative risk [URR]=1.25, p=.04). The magnitude of this relationship was slightly attenuated in the multivariable analysis and was borderline statistically significant (adjusted relative risk [ARR]=1.18, p=.09). In the bivariate analysis, heterosexuals living in UHFs where less than 5% of residents were Black were 21% more likely to be suppressed than their counterparts living in UHFs where more than 30% of residents were Black (URR=1.21, p=.01). The magnitude of this relationship was slightly attenuated in the multivariable analysis and attained only borderline statistical significance (ARR=1.13, p=.09).
Table 3.
Bivariate and multivariate results of a multilevel regression of HIV viral suppression on individual- and United Hospital Fund- (UHF-) level covariates in a sample of heterosexuals (N = 3,159) in New York City diagnosed with HIV between 2009–2013
| Variable | Bivariates |
Multivariable model |
||
|---|---|---|---|---|
| Relative Risk | P-value | Adjusted Relative Risk | P-value | |
| UHF level variables | ||||
| % residents who were food distressed (ref = high) | ||||
| Low <1.00 | 1.25 | 0.04 | 1.18 | 0.09 |
| Medium 1.00–<5.00 | 1.18 | 0.13 | 1.12 | 0.23 |
| % residents who were non-Hispanic Black (ref = high) | ||||
| Low <5.00 | 1.21 | 0.01 | 1.13 | 0.09 |
| Medium 5.00-<30.00 | 1.04 | 0.44 | 1.02 | 0.72 |
| % residents who were 21–54 years old | 1.00 | 0.68 | ||
| Alcohol outlet density | 1.08 | 0.32 | ||
| Residential vacancy | 1.00 | 0.11 | 1.00 | 0.16 |
| Stops per resident (ref = high) | ||||
| Low <0.04 | 1.06 | 0.49 | ||
| Medium 0.04-<0.20 | 1.10 | 0.19 | ||
| Stops without arrest per resident (ref = high) | ||||
| Low <0.06 | 1.12 | 0.12 | 1.03 | 0.55 |
| Medium 0.06-<0.22 | 1.06 | 0.38 | 1.06 | 0.29 |
| UHF stabilityⱡ | 1.01 | 0.30 | ||
| UHF affluence₸ | 1.01 | 0.47 | ||
| Neighborhood disadvantage† | 0.99 | 0.26 | ||
| Poor access to healthcare | 0.94 | 0.87 | ||
| Individual-level variables | ||||
| Male (ref = Female) | 0.89 | 0.01 | 0.87 | 0.001 |
| Race/ethnicity (ref = Black) | ||||
| Hispanic | 1.14 | 0.0002 | 1.06 | 0.07 |
| White | 1.05 | 0.47 | 0.98 | 0.78 |
| Foreign-born | 1.30 | <.0001 | 1.23 | <.0001 |
| History of homelessness | 0.86 | 0.16 | ||
| Age at HIV diagnosis (ref = 40–49) | ||||
| 13–19 | 0.85 | 0.08 | 0.87 | 0.15 |
| 20–29 | 0.99 | 0.86 | 0.96 | 0.40 |
| 30–39 | 1.05 | 0.30 | 1.04 | 0.38 |
| 50-59 | 1.08 | 0.10 | 1.06 | 0.19 |
| 60+ | 1.12 | 0.05 | 1.05 | 0.35 |
| Year of HIV diagnosis (ref = 2009) | ||||
| 2010 | 1.15 | 0.01 | 1.14 | 0.01 |
| 2011 | 1.22 | <.0001 | 1.21 | 0.0001 |
| 2012 | 1.31 | <.0001 | 1.31 | <.0001 |
| 2013 | 1.43 | <.0001 | 1.36 | <.0001 |
Higher values mean more stability.
Higher values mean more affluence.
Higher values mean more disadvantage.
No other UHF-level exposures were significantly associated with suppression. Individual-level sex, race/ethnicity, nativity, and year of diagnosis were associated with achieving viral suppression in bivariate models and in the multivariable model (Table 3). No interactions between individual level race/ethnicity and significant UHF-level variables were found. In the sensitivity analysis that excluded UHFs with fewer than 10 individuals, the magnitude of the relationship between viral suppression and living in UHFs where less than 1% of residents were food distressed was further attenuated (ARR=1.14, p=.18).
Durable Viral Suppression
Heterosexuals living in UHFs that had a smaller percentage of food-distressed residents had a greater likelihood of achieving durable suppression (Table 4). In UHFs where <1% of residents were food distressed, heterosexuals were 70% more likely to be durably suppressed than their counterparts living in UHFs where at least 5% of residents were food distressed (ARR= 1.70, p=.01; URR= 1.48, p=.02). These models also suggest a possible dose-response relationship: heterosexuals living in UHFs where between 1 to <5% of residents were food distressed had a marginally significant greater likelihood of achieving durable suppression than their counterparts living in UHFs where at least 5% of residents were food distressed (ARR=1.36, p=.07; URR=1.35, p=.07). Considering the adjusted model, 27% of all durable viral suppression cases in the analysis were attributable to living in a neighborhood where less than 1% of residents were food distressed (e-PAR%=27.25, Confidence Interval [CI]= 16.91, 36.10). Residence in such a neighborhood varied by race/ethnicity (66% of Black vs 67% of Latino vs 57% of White heterosexuals), but confidence intervals for racial/ethnic-specific ePAR%s overlapped (Black e-PAR%=27.32, CI= 16.82, 36.42; Hispanic e-PAR%=27.76, CI=16.83, 37.49; White e-PAR%=23.42, CI= 12.63, 34.64). This suggests that there was no difference across racial/ethnic groups in the percentage of variance in the outcome attributable to this place-based exposure.
Table 4.
Bivariate and multivariate results of a multilevel regression of HIV durable viral suppression on individual- and United Hospital Fund- (UHF-) level covariates in a sample of heterosexuals (N = 3,159) in New York City diagnosed with HIV between 2009–2013.
| Variable | Bivariates |
Multivariable model |
||
|---|---|---|---|---|
| Relative Risk | P-value | Adjusted Relative Risk | P-value | |
| UHF-level variables | ||||
| % residents who were food distressed (ref = high) | ||||
| Low <1.00 | 1.48 | 0.02 | 1.70 | 0.01 |
| Medium 1.00-<5.00 | 1.35 | 0.07 | 1.36 | 0.07 |
| % residents who were non-Hispanic Black (ref = high) | ||||
| Low <5.00 | 1.36 | 0.002 | 1.05 | 0.65 |
| Medium 5.00-<30.00 | 1.07 | 0.26 | 1.04 | 0.50 |
| % residents who were 21–54 years old | 1.00 | 0.83 | ||
| Alcohol outlet density | 1.19 | 0.11 | 0.80 | 0.17 |
| Residential vacancy | 1.00 | 0.20 | 1.00 | 0.37 |
| Stops per resident (ref = high) | ||||
| Low <0.04 | 0.99 | 0.92 | ||
| Medium 0.04-<0.20 | 1.03 | 0.74 | ||
| Stops without arrest per resident (ref = high) | ||||
| Low <0.06 | 1.08 | 0.40 | 0.95 | 0.57 |
| Medium 0.06-<0.22 | 0.98 | 0.81 | 0.97 | 0.69 |
| UHF stabilityⱡ | 1.00 | 0.80 | ||
| UHF affluence₸ | 1.01 | 0.50 | ||
| Neighborhood disadvantage† | 0.98 | 0.28 | 0.98 | 0.23 |
| Poor access to healthcare | 0.97 | 0.96 | 0.96 | 0.94 |
| Individual-level variables | ||||
| Male (ref = Female) | 0.84 | 0.008 | 0.82 | 0.002 |
| Race/ethnicity (ref = Black) | ||||
| Hispanic | 1.23 | 0.0001 | 1.17 | 0.004 |
| White | 1.32 | 0.005 | 1.26 | 0.02 |
| Foreign born | 1.37 | <.0001 | 1.24 | <.0001 |
| History of homelessness | 0.59 | 0.01 | 0.62 | 0.02 |
| Age at HIV diagnosis (ref = 40–49) | ||||
| 13–19 | 0.61 | 0.003 | 0.61 | 0.004 |
| 20–29 | 0.91 | 0.19 | 0.87 | 0.06 |
| 30–39 | 1.06 | 0.40 | 1.04 | 0.55 |
| 50–59 | 1.19 | 0.01 | 1.17 | 0.02 |
| 60+ | 1.12 | 0.22 | 1.04 | 0.66 |
| Year of HIV diagnosis (ref = 2009) | ||||
| 2010 | 1.18 | 0.04 | 1.18 | 0.04 |
| 2011 | 1.39 | <.0001 | 1.39 | <.0001 |
| 2012 | 1.40 | <.0001 | 1.40 | <.0001 |
| 2013 | 1.71 | <.0001 | 1.61 | <.0001 |
Higher values mean more stability.
Higher values mean mote affluence.
Higher values mean more disadvantage.
In the bivariate analysis, heterosexuals living in UHFs where less than 5% of residents were Black were 36% more likely to be suppressed than their counterparts living in UHFs where more than 30% of residents were Black (URR=1.36, p=.002). The magnitude of this relationship was attenuated in the multivariable analysis and was no longer statistically significant (ARR=1.05, p=.65).
No other UHF-level exposures were significantly associated with durable suppression. All individual-level variables – sex, race/ethnicity, nativity, history of homelessness, age at diagnoses, and year of diagnosis – were significantly associated with achieving durable viral suppression in both the bivariate and multivariable models (Table 4).
In the sensitivity analysis, the magnitude of the relationship between durable viral suppression and living in UHFs where less than 1% of residents were food distressed was strengthened (ARR=1.72, p=.01). The corresponding e-PAR% for the sensitivity analysis indicates that 39% of all durable viral suppression cases in the analysis were attributable to living in a neighborhood where less than 1% of residents were food distressed (e-PAR%=39.12, CI= 24.43, 51.06). The relationship between durable viral suppression and living in UHFs where less than 5% of residents were Black remained non-significant (ARR=1.10, p=.39).
Discussion
In this analysis of NYC surveillance and administrative data, we found that individuals with heterosexual transmission risk were more likely to maintain viral suppression if they lived in a UHF where a smaller percentage of residents were food distressed (<1% vs. at least 5%). Our results also indicate that there may be a dose-response relationship between the percentage of residents who are food distressed and durable viral suppression. Our sensitivity analyses found that excluding UHFs with <10 participants weakened the association between the percent of food distressed residents and viral suppression, but strengthened the association between the percent of food distressed residents and durable viral suppression. Heterosexuals were marginally more likely to achieve viral suppression if they lived in a UHF where fewer (<5%) residents were Black, compared to a UHF where more (at least 30%) residents were Black; however, e-PAR%s indicate that this association would contribute little to heterosexual viral suppression in NYC.
Quasi-experimental research has established a relationship between spatial access to food outlets in impoverished neighborhoods and individual resident’s food insecurity (Richardson et al., 2017). Individual food insecurity, in turn, has been associated with difficulty achieving or maintaining HIV viral suppression (Aibibula, Cox, Hamelin, McLinden, et al., 2017; Kalichman et al., 2010; Weiser et al., 2013). Weiser et al. (2011) suggest food insecurity may cause weight loss, low body mass index, low albumin, and micronutrient deficiencies, which in turn link with risk for opportunistic infections and shorter HIV survival time (S. D. Weiser et al., 2011). Food-insecure individuals may also forgo medical appointments (S. D. Weiser et al., 2011), or experience difficulties accessing and adhering to HAART(Aranka Anema et al., 2009; Kalichman et al., 2010; S. D. Weiser et al., 2011), when limited funds are spent on food rather than on healthcare (Cunningham et al., 1999). A prior analysis of NYC DOHMH surveillance data found no association between living in a food-distressed UHF district and suppression among men who have sex with men (MSM). Given the history of AIDS-related activism among MSM in NYC, it is possible that MSM living in food-distressed areas are better able to connect rapidly with a host of social services post-diagnosis, including nutritional supports.
As was found for MSM in the previous analysis of NYC DOHMH surveillance data (Jefferson et al., 2017), the percent of residents who were Black was related to viral suppression (albeit with a borderline significance), but was unrelated to durable viral suppression. This exposure’s different relationship to these two outcomes may have arisen because maintaining viral suppression over time requires access to more structural resources, such as a strengthened neighborhood economic base and retention of pharmacies trained in providing HAART medication. However, it is also worth noting that neighborhoods where more residents were Black may have norms promoting HIV testing and risk-reduction practices (E. A. Arnold & Bailey, 2009), which could facilitate early HIV detection, linkage to care, and HAART initiation. The effects of such protective norms may be undermined for Blacks and Latinos in neighborhoods with a “high” percent of residents who were Black, by high levels of structural (Massey & Denton, 1993) and interpersonal racism (Collins, 2014).
Many place-based exposures explored in this analysis were not significant. This may reflect NYC DOHMH and community-based organizations’ broad and long-standing efforts to reduce HIV health disparities, which may explain an attenuated association between place and viral suppression outcomes.
Limitations
This analysis has several limitations. We were restricted to individual-level variables available in the NYC DOHMH surveillance registry. We were therefore unable to control for some potentially important covariates, such as individual income, food insecurity, and education. Analyses were not longitudinal. We could not examine whether or how selection into UHFs shaped UHF/suppression relationships or make causal claims. We operationalized “place” in terms of residential UHF at HIV diagnosis. This may have led us to misclassify place-based exposures. Finally, persons who lacked ZIP code data were excluded from analyses.
Conclusion
Despite these limitations, we found that living in neighborhoods with a “low” percent of residents who were Black was marginally associated with achieving viral suppression after HIV diagnosis. Living in neighborhoods with a “low” percent of residents who were food distressed also was marginally associated with suppression, and was associated with durable suppression To inform interventions, future multilevel research should explore associations in longitudinal panels or cohorts between the percent of residents who are Black, the percent of residents who are food distressed, and HIV viral suppression, and analyze the causal pathways through which these place-based exposures affect viral suppression outcomes.
Acknowledgments
Funding
This work was supported by R01 DA035707 (Campbell, Des Jarlais) and by the Emory Center for AIDS Research (P30 AI050409; Curran.) The authors declare that they have no conflict of interest.
Appendix A.
Components Generated by Principal Components Analysis of Stability, Wealth, Economic Disadvantage, and Healthcare Access Variables
| Component | Constituent Variables | Correlations of constituent variables with component |
|---|---|---|
| Stability₸ | ||
| Eigenvalue: 21.27 | Percent same home | 0.996 |
| Variance explained: 95% | Male: female sex ratio | 0.08 |
| Wealthⱡ | ||
| Eigenvalue: 2.59 | Percent college educated | 0.60 |
| Variance explained: 86% | Percent high income households | 0.58 |
| Percent expensive homes | 0.55 | |
| Economic disadvantageⱡ | ||
| Eigenvalue: 4.39 | Median income | −0.47 |
| Variance explained: 88% | Percent unemployed | 0.43 |
| Percent in poverty | 0.45 | |
| Percent on public assistance | 0.46 | |
| Percent without a high school education | 0.43 | |
| Poor access to healthcare‡ | ||
| Eigenvalue: 0.005 | Percent uninsured | 0.93 |
| Variance explained: 87% | Percent went without needed care | 0.37 |
Covariance matrix used as there are only two constituent variables, both measured on the same scale. Note the correlation matrix eigenvector was 1.32 and it explained 68% of the variance.
Correlation matrix used.
Covariance matrix used as there are only two constituent variabiles, both measured on the same scale. Note the correlation matrix eigenvector was 1.60 and it explained 80% of the variance.
Footnotes
Disclosure Statement
No potential conflict of interest was reported by the authors.
References
- Adimora AA, & Schoenbach VJ (2002). Contextual factors and the black-white disparity in heterosexual HIV transmission. Epidemiology, 13(6), 707–712. doi: 10.1097/01.ede.0000024139.60291.08 [DOI] [PubMed] [Google Scholar]
- Adimora AA, Schoenbach VJ, & Floris-Moore MA (2009). Ending the epidemic of heterosexual HIV transmission among African Americans. Am J Prev Med, 37(5), 468–471. doi: 10.1016/j.amepre.2009.06.020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Aibibula W, Cox J, Hamelin AM, McLinden T, Klein MB, & Brassard P (2017). Association Between Food Insecurity and HIV Viral Suppression: A Systematic Review and Meta-Analysis. AIDS Behav, 21(3), 754–765. doi: 10.1007/s10461-016-1605-5 [DOI] [PubMed] [Google Scholar]
- Aibibula W, Cox J, Hamelin AM, Moodie E, Naimi AI, McLinden T, … Brassard P (2017). Food insecurity may lead to incomplete HIV viral suppression and less immune reconstitution among HIV/hepatitis C virus-coinfected people. HIV Med. doi: 10.1111/hiv.12561 [DOI] [PubMed] [Google Scholar]
- Anema A, Fielden SJ, Castleman T, Grede N, Heap A, & Bloem M (2014). Food Security in the Context of HIV: Towards Harmonized Definitions and Indicators. AIDS Behav, 18, S476–S489. doi: 10.1007/s10461-013-0659-x [DOI] [PubMed] [Google Scholar]
- Anema A, Kerr T, Milloy MJ, Feng C, Montaner JS, & Wood E (2014). Relationship between hunger, adherence to antiretroviral therapy and plasma HIV RNA suppression among HIV-positive illicit drug users in a Canadian setting. AIDS Care, 26(4), 459–465. doi: 10.1080/09540121.2013.832724 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Anema A, Vogenthaler N, Frongillo EA, Kadiyala S, & Weiser SD (2009). Food insecurity and HIV/AIDS: current knowledge, gaps, and research priorities. Current HIV/AIDS Reports, 6(4), 224–231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arnold EA, & Bailey MM (2009). Constructing home and family: How the ballroom community supports African American GLBTQ youth in the face of HIV/AIDS. Journal of gay & lesbian social services, 21(2–3), 171–188. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arnold M, Hsu L, Pipkin S, McFarland W, & Rutherford GW (2009). Race, place and AIDS: the role of socioeconomic context on racial disparities in treatment and survival in San Francisco. Soc Sci Med, 69(1), 121–128. doi: 10.1016/j.socscimed.2009.04.019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arnsten JH, Demas PA, Grant RW, Gourevitch MN, Farzodegan H, Howard AA, & Schoenboum EE (2002). Impact of active drug use on antiretroviral therapy adherence and viral suppression in HIV-infected drug users. J Gen Intern Med, 17(5), 377–381. doi: 10.1046/j.1525-1497.2002.10644.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beach MC, Keruly J, & Moore RD (2006). Is the Quality of the Patient‐Provider Relationship Associated with Better Adherence and Health Outcomes for Patients with HIV? J Gen Intern Med, 21(6), 661–665. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beattie C (2015). Structural barriers to HIV viral load suppression at an urban HIV/AIDS care center. Paper presented at the 143rd APHA Annual Meeting and Exposition (October 31-November 4, 2015). [Google Scholar]
- Blackstock OJ, Addison DN, Brennan JS, & Alao OA (2012). Trust in primary care providers and antiretroviral adherence in an urban HIV clinic. J Health Care Poor Underserved, 23(1), 88–98. doi: 10.1353/hpu.2012.0006 [DOI] [PubMed] [Google Scholar]
- Buot ML, Docena JP, Ratemo BK, Bittner MJ, Burlew JT, Nuritdinov AR, & Robbins JR (2014). Beyond race and place: distal sociological determinants of HIV disparities. PLoS One, 9(4), e91711. doi: 10.1371/journal.pone.0091711 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Burgoyne R (2005). Exploring direction of causation between social support and clinical outcome for HIV-positive adults in the context of highly active antiretroviral therapy. AIDS Care, 17(1), 111–124. [DOI] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention. (2016). Selected National HIV Prevention and Care Outcomes in the United States. In. Atlanta. [Google Scholar]
- Collins PH (2014). Hegemonic Masculinity and Black Gender Ideology In O’Hara R. G. a. J. F. (Ed.), Composing Gender. Boston: Bedford/St. Martin’s. [Google Scholar]
- Cooper HL, Arriola KJ, Haardörfer R, & McBride CM (2016). Population-Attributable Risk Percentages for Racialized Risk Environments. Am J Public Health, 106(10), 1789–1792. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crepaz N, Tang T, Marks G, Mugavero MJ, Espinoza L, & Hall HI (2016). Durable Viral Suppression and Transmission Risk Potential Among Persons With Diagnosed HIV Infection: United States, 2012–2013. Clinical Infectious Diseases, 63(7), 976–983. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cunningham WE, Andersen RM, Katz MH, Stein MD, Turner BJ, Crystal S, … Shapiro M (1999). The impact of competing subsistence needs and barriers on access to medical care for persons with human immunodeficiency virus receiving care in the United States. Medical Care, 37(12), 1270–1281. doi: 10.1097/00005650-199912000-00010 [DOI] [PubMed] [Google Scholar]
- Davies HTO, Crombie IK, & Tavakoli M (1998). When can odds ratios mislead? Bmj, 316(7136), 989–991. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eberhart MG, Voytek C, Hillier A, Metzger D, Blank M, & Brady K (2014). Travel distance to HIV medical care: a geographic analysis of Weighted survey data from the medical monitoring project in Philadelphia, PA. AIDS Behav, 18(4), 776–782. [DOI] [PubMed] [Google Scholar]
- Food Access Research Atlas (2010). [Google Scholar]
- Ford CL, & Airhihenbuwa CO (2010). Critical race theory, race equity, and public health: toward antiracism praxis. Am J Public Health, 100(S1), S30–S35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Friedman SR, Cooper HL, Tempalski B, Keem M, Friedman R, Flom PL, & Des Jarlais DC (2006). Relationships of deterrence and law enforcement to drug-related harms among drug injectors in US metropolitan areas. AIDS, 20(1), 93–99. [DOI] [PubMed] [Google Scholar]
- Goranson C KS, Jasek J, Olson C, Kerker B. (2009). The New York City Community Health Survey Atlas, 2007. Retrieved from [Google Scholar]
- Gross R, Yip B, Lo Re V, Wood E, Alexander CS, Harrigan PR, … Hogg RS (2006). A simple, dynamic measure of antiretroviral therapy adherence predicts failure to maintain HIV-1 suppression. Journal of Infectious Diseases, 194(8), 1108–1114. doi: 10.1086/507680 [DOI] [PubMed] [Google Scholar]
- Hall HI, Frazier EL, Rhodes P, Holtgrave DR, Furlow-Parmley C, Tang T, … Skarbinski J (2013). Differences in Human Immunodeficiency Virus Care and Treatment Among Subpopulations in the United States. Jama Internal Medicine, 173(14), 1337–1344. doi: 10.1001/jamainternmed.2013.6841 [DOI] [PubMed] [Google Scholar]
- Hess K HX, Lansky A, Mermin J, Hall HI. (2016). Estimating the lifetime risk of a diagnosis of HIV infection in the United States. Paper presented at the Conference on Retroviruses and Opportunistic Infections (CROI), Boston. [Google Scholar]
- Hughes EP, & Kearney TD (2003). Optimization with the SAS® System: What It Is, What’s New, and Why You Should Be Using It. In.
- Jefferson KA, Kersanske LS, Wolfe ME, Braunstein SL, Haardörfer R, Des Jarlais DC, … Cooper HL (2017b). Place-Based Predictors of HIV Viral Suppression and Durable Suppression Among Men Who Have Sex With Men in New York City. AIDS Behav, 21(10), 2987–2999. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kalichman SC, Cherry C, Amaral C, White D, Kalichman MO, Pope H, … Macy R (2010). Health and treatment implications of food insufficiency among people living with HIV/AIDS, Atlanta, Georgia. Journal of Urban Health, 87(4), 631–641. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kalichman SC, Hernandez D, Cherry C, Kalichman MO, Washington C, & Grebler T (2014). Food insecurity and other poverty indicators among people living with HIV/AIDS: effects on treatment and health outcomes. J Community Health, 39(6), 1133–1139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Katz MH, Hsu L, Lingo M, Woelffer G, & Schwarcz SK (1998). Impact of socioeconomic status on survival with AIDS. Am J Epidemiol, 148(3), 282–291. [DOI] [PubMed] [Google Scholar]
- Koss CA, Natureeba P, Nyafwono D, Plenty A, Mwesigwa J, Nzarubara B, … Young SL (2016). Brief Report: Food Insufficiency Is Associated With Lack of Sustained Viral Suppression Among HIV-Infected Pregnant and Breastfeeding Ugandan Women. J Acquir Immune Defic Syndr, 71(3), 310–315. doi: 10.1097/qai.0000000000000860 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liebschutz J, Schwartz S, Hoyte J, Conoscenti L, Christian AB Sr., Muhammad L, … James T (2010). A Chasm Between Injury and Care: Experiences of Black Male Victims of Violence. Journal of Trauma-Injury Infection and Critical Care, 69(6), 1372–1378. doi: 10.1097/TA.0b013e3181e74fcf [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marconi VC, Grandits GA, Weintrob AC, Chun H, Landrum ML, Ganesan A, … Lifson A (2010). Research Outcomes of highly active antiretroviral therapy in the context of universal access to healthcare: the US Military HIV Natural History Study. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Massey DS, & Denton NA (1993). American apartheid: Segregation and the making of the underclass: Harvard University Press. [Google Scholar]
- Mendoza JA, Paul ME, Schwarzwald H, Liu Y, Martinez R, Nicklas TA, & Baranowski T (2013). Food insecurity, CD4 counts, and incomplete viral suppression among HIV+ patients from Texas Children’s Hospital: a pilot study. AIDS Behav, 17(5), 1683–1687. doi: 10.1007/s10461-013-0419-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- Northridge ME (1995). Public health methods--attributable risk as a link between causality and public health action. Am J Public Health, 85(9), 1202–1204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pollack CE, Griffin BA, & Lynch J (2010). Housing Affordability and Health Among Homeowners and Renters. Am J Prev Med, 39(6), 515–521. doi: 10.1016/j.amepre.2010.08.002 [DOI] [PubMed] [Google Scholar]
- Richardson AS, Ghosh-Dastidar M, Beckman R, Flórez KR, DeSantis A, Collins RL, & Dubowitz T (2017). Can the introduction of a full-service supermarket in a food desert improve residents’ economic status and health? Ann Epidemiol, 27(12), 771–776. [DOI] [PMC free article] [PubMed] [Google Scholar]
- SAS Institute. (2011). The SAS system for Windows, 9.3. Cary, NC. [Google Scholar]
- Sewell AA, Massey DS, & Denton NA (2010). A Different Menu: Racial Residential Segregation and the Persistence of Racial Inequality. Race and Ethnic Relations in the 21st Century: History, Theory, Institutions, and Policy, 287–296. [Google Scholar]
- Shacham E, Lian M, Onen NF, Donovan M, & Overton ET (2013). Are neighborhood conditions associated with HIV management? HIV Med, 14(10), 624–632. doi: 10.1111/hiv.12067 [DOI] [PubMed] [Google Scholar]
- Singh S, Bradley H, Hu X, Skarbinski J, Hall HI, & Lansky A (2014). Men living with diagnosed HIV who have sex with men: progress along the continuum of HIV care--United States, 2010. MMWR Morb Mortal Wkly Rep, 63(38), 829–833. [PMC free article] [PubMed] [Google Scholar]
- Stone VE (2012). HIV/AIDS in Women and Racial/Ethnic Minorities in the US. Current infectious disease reports, 14(1), 53–60. [DOI] [PubMed] [Google Scholar]
- Terry v. Ohio, No. No. 67, 392 1 (Supreme Court 1968).
- Walker RE, Butler J, Kriska A, Keane C, Fryer CS, & Burke JG (2010). How does food security impact residents of a food desert and a food oasis? Journal of Hunger & Environmental Nutrition, 5(4), 454–470. [Google Scholar]
- Wallace R (1990). Urban desertification, public health and public order: ‘planned shrinkage’, violent death, substance abuse and AIDS in the Bronx. Soc Sci Med, 31(7), 801–813. [DOI] [PubMed] [Google Scholar]
- Wallace R, Wallace D, Andrews H, Fullilove R, & Fullilove MT (1995). THE SPATIOTEMPORAL DYNAMICS OF AIDS AND TB IN THE NEW-YORK METROPOLITAN REGION FROM A SOCIOGEOGRAPHIC PERSPECTIVE - UNDERSTANDING THE LINKAGES OF CENTRAL CITY AND SUBURBS. Environment and Planning A, 27(7), 1085–1108. doi: 10.1068/a271085 [DOI] [Google Scholar]
- Wang EA, McGinnis KA, Fiellin DA, Goulet JL, Bryant K, Gibert CL, … Vogenthaler N (2011). Food insecurity is associated with poor virologic response among HIV-infected patients receiving antiretroviral medications. J Gen Intern Med, 26(9), 1012–1018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weiser SD, Frongillo EA, Ragland K, Hogg RS, Riley ED, & Bangsberg DR (2009). Food Insecurity is Associated with Incomplete HIV RNA Suppression Among Homeless and Marginally Housed HIV-infected Individuals in San Francisco. J Gen Intern Med, 24(1), 14–20. doi: 10.1007/s11606-008-0824-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weiser SD, Tsai AC, Gupta R, Frongillo EA, Kawuma A, Senkungu J, … Martin JN (2012). Food insecurity is associated with morbidity and patterns of healthcare utilization among HIV-infected individuals in a resource-poor setting. AIDS (London, England), 26(1), 67. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weiser SD, Young SL, Cohen CR, Kushel MB, Tsai AC, Tien PC, … Bangsberg DR (2011). Conceptual framework for understanding the bidirectional links between food insecurity and HIV/AIDS. Am J Clin Nutr, 94(6), 1729s–1739s. doi: 10.3945/ajcn.111.012070 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weiser SD, Yuan C, Guzman D, Frongillo EA, Riley ED, Bangsberg DR, & Kushel MB (2013). Food insecurity and HIV clinical outcomes in a longitudinal study of urban homeless and marginally housed HIV-infected individuals. AIDS, 27(18), 2953–2958. doi: 10.1097/01.aids.0000432538.70088.a3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wiewel EW (2014). Association of neighborhood-level socioeconomic status (SES) with time from HIV diagnosis to viral suppression among newly diagnosed New Yorkers, 2006–2010. Paper presented at the 142nd APHA Annual Meeting and Exposition (November 15-November 19, 2014). [Google Scholar]
- Woods SJ, Wineman NM, Page GG, Hall RJ, Alexander TS, & Campbell JC (2005). Predicting immune status in women from PTSD and childhood and adult violence. Advances in Nursing Science, 28(4), 306–319. [DOI] [PubMed] [Google Scholar]
- Yehia BR, Rebeiro P, Althoff KN, Agwu AL, Horberg MA, Samji H, … North Amer ACC (2015). Impact of Age on Retention in Care and Viral Suppression. Jaids-Journal of Acquired Immune Deficiency Syndromes, 68(4), 413–419. [DOI] [PMC free article] [PubMed] [Google Scholar]