

Key Points
Question
What is the postoperative opioid prescribing practice and true need for opioids after thyroidectomy and parathyroidectomy?
Findings
In a cohort study of 1702 patients undergoing 1765 thyroidectomy and parathyroidectomy procedures, the mean postoperative prescribed dose of opioids was shown to be significantly reduced after initiation of preoperative patient education and use of nonopioid medications. In the last quarter of 2017, the mean (SD) dose prescribed was 19.90 (26.60) morphine milligram equivalents for parathyroidectomy, 56.72 (61.65) morphine milligram equivalents for hemithyroidectomy, and 68.15 (68.47) morphine milligram equivalents for total thyroidectomy.
Meaning
Results of the study suggest that patients undergoing thyroid and parathyroid surgery need little opioid treatment postoperatively.
This cohort study assesses the opioid prescribing practices and opioid needs for patients undergoing thyroid and parathyroid surgery.
Abstract
Importance
In recent years, the medical community’s inadvertent contribution to opioid addiction has been recognized.
Objective
To determine the opioid prescribing practices and opioid needs for patients undergoing thyroid and parathyroid surgery to help reduce postoperative opioid administration.
Design, Setting, and Participants
This retrospective cohort study included 1788 opioid-naive patients who underwent thyroid and parathyroid surgery from January 1, 2012, through December 31, 2017, at the high-volume academic endocrine surgery center at Oregon Health and Sciences University. Patients with long-term opioid treatment and those who underwent other head and neck procedures or robotic thyroidectomy were excluded. For analysis, 1765 procedures were available (723 parathyroidectomy, 400 hemithyroidectomy, and 642 total thyroidectomy).
Main Outcomes and Measures
The quantity of prescribed opioids was determined in morphine milligram equivalents (MME). Opioid refill data after discharge were also analyzed. Patients were then divided into past (1336 in group 1 [January 1, 2012, to September 30, 2016]) and current (429 in group 2 [October 31, 2016, to December 31, 2017]) prescribing practices. For each procedure, the mean quantity prescribed for each group, difference between the means, 95% CI for the difference, and effect size were calculated.
Results
A total of 1702 patients (80.0% female [n = 1361]; mean age, 51.2 years [range, 7-97 years]) undergoing 1765 procedures were included in the analysis. For parathyroidectomy, the mean (SD) opioid quantity prescribed was 176.20 (86.66) MME in group 1 vs 80.08 (74.43) MME in group 2 (effect size, 1.139); for hemithyroidectomy, 204.65 (112.24) MME in group 1 vs 112.24 (102.31) MME in group 2 (effect size, 0.842); and for total thyroidectomy, 214.87 (161.09) MME for group 1 vs 102.29 (87.72) MME for group 2 (effect size, 0.754). In the last quarter of 2017, the numbers of patients discharged without any opioid prescription were 15 of 26 (57.5%) for parathyroidectomy, 12 of 32 (37.5%) for hemithyroidectomy, and 9 of 27 (33.3%) for total thyroidectomy. Patient calls requesting pain medications for group 2 were similar or fewer, depending on the procedure. Those who were prescribed less than 75.0 MME postoperatively did not call for additional opioid prescriptions.
Conclusions and Relevance
Our study suggests that patients undergoing thyroid and parathyroid surgery need little, if any, postoperative opioids.
Introduction
The epidemic of opioid abuse has continued to plague the United States. The rate of drug overdose deaths increased from 6.1 per 100 000 standard population in 1999 to 16.3 per 100 000 in 2015, with an overall mean increase of 5.5% per year.1 According to the Centers for Disease Control and Prevention, approximately 64 000 deaths in the United States were due to opioid overdose in 2016.2
More recently awareness of this epidemic and recognition of the medical community’s inadvertent contribution to the problem with previously accepted standard opioid prescribing practices have increased. From 2006 to 2016, the mean duration of opioid prescribed increased from 13.3 to 18.1 days per prescription, an overall 35.7% increase. The rate increased annually by 4.4% from 2006 to 2008.1 Recognizing this increase as a serious health problem, the Centers for Disease Control and Prevention in 2016 issued guidelines for primary care physicians treating chronic pain with opioids.3 The guidelines state that because long-term opioid dependence begins with acute pain treatment, opioid prescribing for acute pain should not exceed the quantity needed. These guidelines are particularly relevant to surgeons because most postsurgical patients will have an acute period of postoperative pain. Unfortunately, we have a paucity of surgery-specific opioid prescribing guidelines in the literature. As a result, wide variation in opioid prescribing patterns exists among surgeons of various specialties.4,5,6,7 Furthermore, the amount prescribed is usually excessive, because studies have shown that as many as 71% of opioids prescribed postoperatively are not taken by the patient.4 In a retrospective review of a large cohort of privately insured patients in the United States undergoing major and minor surgical procedures, Brummett et al8 reported that the incidence of persistent opioid use 90 days after minor surgery in opioid-naive patients was 6%. Within this group, the incidence of persistent opioid use in patients undergoing thyroidectomy was 4.5%; for parathyroidectomy, 6%. Underlying psychiatric conditions, such as depression, are risk factors for long-term opioid use. As such, if patients are prescribed larger quantities than their real need, they may continue to use their prescribed excess opioids to alleviate depression and emotional pain, thus increasing the risk of addiction. A paucity of research quantitatively characterizes the mean volume of opioid medication that patients are prescribed after discharge from endocrine surgery. This retrospective study was conducted to determine opioid prescribing practices and opioid needs in patients who underwent thyroid and parathyroid surgery at a single institution performing high-volume endocrine procedures.
Methods
We performed a retrospective cohort study of all opioid-naive patients who underwent thyroid and parathyroid operations at the Oregon Health and Science University (OHSU), Portland, from January 1, 2012, through December 31, 2017. This protocol was approved by institutional review board of OHSU, which did not require informed consent for this retrospective review.
The electronic medical record at OHSU was queried by Current Procedural Terminology codes 60220, 60240, 60252, 60270, and 60500 during the study period. These codes reflect the specific operations of total thyroidectomy, hemithyroidectomy, and parathyroidectomy. The quantity of opioids prescribed on discharge was then collected from each patient’s discharge medication list. Those who underwent sternotomy, robotic thyroidectomy, concurrent modified neck dissection, or other head and neck procedures such as tracheotomy or tracheal resection were excluded, as well as those who were previously taking opioids for chronic pain and who were admitted for more than 2 nights. Those who underwent concurrent thyroidectomy and parathyroidectomy were categorized as undergoing thyroidectomy (hemithyroidectomy or total thyroidectomy).
In late September of 2016, several surgeons within the Thyroid and Parathyroid Center at OHSU made a concerted effort to decrease opioid prescribing in patients undergoing thyroid and parathyroid operations. Therefore, for data analysis, the groups were then subdivided into past (group 1 [January 1, 2012, to September 30, 2016]) and current (group 2 [October 31, 2016, to December 31, 2017]) prescribing practices. The concerted effort to reduce opioid prescribing included preoperative patient counselling regarding pain management, multimodality nonopioid pain management, and work with nursing on assessing pain based on functional status rather than a 1- to 10-point scale and avoiding opioid administration when possible. The following statement typifies the preoperative discussion with patients regarding postoperative pain:
You will have some soreness around the surgical site and mild discomfort when you swallow. We typically treat that with ice packs, Tylenol, and ibuprofen. It is unlikely that you will need anything more than that. We will see how you do postop and make sure that you are doing fine with this regimen. We want to avoid opioids as much as possible with this kind of surgery because they can cause nausea and vomiting, which is not ideal with a neck incision. You may also have some sore throat, which is best treated with throat lozenges.
The quantity of opioids prescribed in recovery if the patient is discharged the same day or on the floor if admitted overnight was generally used to determine the quantity of opioids to be prescribed on discharge. The total quantity of opioids prescribed was calculated by multiplying the strength of the prescribed opioids by the quantity dispensed. For standardization of data analysis, the total amount prescribed was converted to morphine milligram equivalents (MME) by multiplying the total milligrams of prescribed opioid with a standard conversion factor for the specific medication (ie, 0.15 for codeine phosphate; 1.0 for hydrocodone bitartrate; 1.5 for oxycodone hydrochloride; 4.0 for hydromorphone hydrochloride; and 2.4 for transdermal fentanyl citrate). Calls for pain medications after discharge were also captured by searching the database for opioid prescriptions dispensed that are recorded in the patient’s medication list within 3 weeks of discharge. All medical records meeting these criteria were individually reviewed to confirm a refill and incorporated into the analysis. The primary outcome was the median amount of MME administered as grouped by study period and operation type.
Statistical analysis was performed by determining the mean and SD using Excel (version 15.23; Microsoft Corporation) for all procedures and each type of surgery. For each type of procedure, the effect size and 95% CI were calculated for the mean difference between groups 1 and 2. Because of the sample size difference, the Hedges g value9 was used to determine the effect size for the difference in percentage of patients in groups 1 vs 2 who called in for additional pain medication. The effect size is considered small if g = 0.2, medium if g = 0.5, and large if g = 0.8. The effect size for the difference in percentage of calls for opioids after discharge between groups 1 and 2 was also calculated.
Results
During the study period, 1788 patients underwent head and neck endocrine surgery, of whom 86 were excluded owing to reasons stated in the methods section, leaving 1702 patients (1361 female [80.0%] and 341 male [20.0%]; mean age, 51.2 years [range, 9-97 years]). Sixty-three patients underwent 2 procedures, for example hemithyroidectomy followed by completion thyroidectomy at a later date. Therefore, the total number of procedures during the entire study period included was 1765. Between the 2 periods, 1336 patients were in group 1 and 429 were in group 2. The breakdown of procedures are as follows: 723 parathyroidectomy procedures, 400 hemithyroidectomy procedures, and 642 total thyroidectomy procedures. The patient population is summarized in Table 1.
Table 1. Patient Population Data.
| Characteristic | Data (n = 1702) |
|---|---|
| No. of female/male patients | 1361/341 |
| Age, mean (range), y | 51.2 (7-97) |
| No. of procedures, groups 1/2a | |
| Hemithyroidectomy | 285/115 |
| Total thyroidectomy | 512/130 |
| Parathyroidectomy | 539/184 |
Group 1 underwent procedures from January 1, 2012, to September 30, 2016; group 2, October 31, 2016, to December 31, 2017. Patients underwent 1765 procedures.
When looking at opioid prescription amounts, a large decrease in the total amount of opioids prescribed at discharge occurred between groups 1 and 2 for each procedure. For the 3 different procedures, the mean opioid quantity prescribed in each group, SD, the difference between the means, 95% CI, and effect size for the mean difference are summarized in Table 2. For each of the 3 procedures, the total MME prescribed each quarter steadily decreased for group 2 (Figure). In the last quarter of 2017, the mean (SD) quantity prescribed was 19.90 (26.60) MME for parathyroidectomy, 56.72 (61.65) MME for hemithyroidectomy, and 68.15 (68.47) MME for total thyroidectomy. During this last quarter, patients discharged without any opioid included 15 of 26 (57.7%) for parathyroidectomy, 12 of 32 (37.5%) for hemithyroidectomy, and 9 of 27 (33.3%) for total thyroidectomy. No increase in patient calls requesting refills for opioid medications occurred in the group discharged with a lower dose. The data for patients calling for additional pain medication after discharge are shown in Table 3 for each type of procedure. Overall, for group 1, 45 of 1336 (3.4%) called for additional pain medications after discharge, and 8 of 429 (1.9%) of group 2 (95% CI, −0.6% to 3.0%, continuity corrected). Patients undergoing hemithyroidectomy and total thyroidectomy (45 of 1042 [4.3%]) called in more than those undergoing parathyroidectomy 8 of 723 [1.1%]), as shown in Table 3. None of the patients who were prescribed less than 75.0 MME postoperatively called in for additional opioid prescriptions.
Table 2. Mean Total Opioid Quantity Prescribed at Discharge.
| Opioid Prescription | Hemithyroidectomy (n = 400) | Total Thyroidectomy (n = 642) | Parathyroidectomy (n = 723) | |||
|---|---|---|---|---|---|---|
| Group 1 | Group 2 | Group 1 | Group 2 | Group 1 | Group 2 | |
| Mean (SD) quantity, MME | 204.65 (112.24) | 112.24 (102.31) | 214.87 (161.09) | 102.29 (87.72) | 176.20 (86.66) | 80.08 (74.43) |
| Absolute difference between groups (95% CI) | 92.41 (68.63-116.19) | 112.58 (83.8-141.36) | 96.12 (83.11-109.13) | |||
| Effect size | 0.842 | 0.754 | 1.139 | |||
Abbreviation: MME, morphine milligram equivalent.
Figure. Mean (SD) Opioid Dose Prescribed at Discharge in Group 2 .
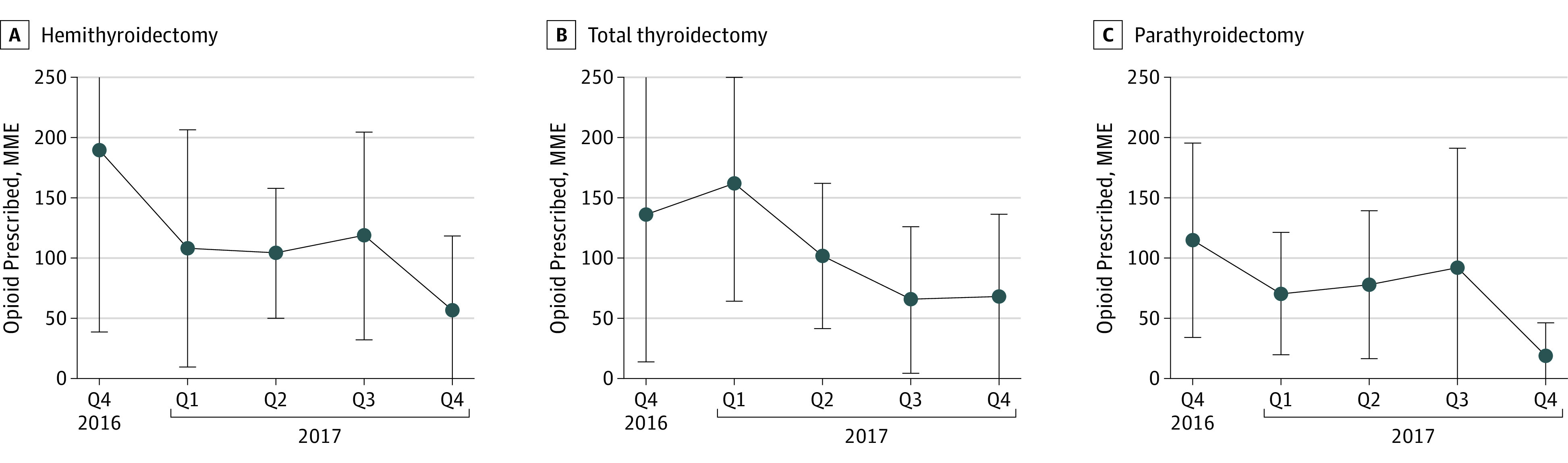
Data are stratified by quarter for patients undergoing hemithyroidectomy, total thyroidectomy, or parathyroidectomy from October 31, 2016, through December 31, 2017.
Table 3. Request for Additional Pain Medication After Discharge.
| Treatment Group | Group 1 | Group 2 |
|---|---|---|
| Hemithyroidectomy | ||
| No. of patients | 285 | 115 |
| No. of requests | 14 | 4 |
| Difference between groups, % (95% CI)a | 1.43 (4.65-5.55) | |
| Total thyroidectomy | ||
| No. of patients | 512 | 130 |
| No. of requests | 24 | 3 |
| Difference between groups, % (95% CI)a | 2.38 (2.68-5.25) | |
| Parathyroidectomy | ||
| No. of patients | 539 | 184 |
| No. of requests | 7 | 1 |
| Difference between groups, % (95% CI)a | 0.76 (2.24-2.32) | |
Indicates with continuity correction.
Discussion
This retrospective study was conducted to determine opioid prescribing practices and opioid needs in patients who underwent thyroid and parathyroid procedures at a single institution performing high-volume endocrine surgery. We found that opioid prescribing and opioid needs for patients who underwent thyroid and parathyroid surgery can be dramatically reduced through the concerted use of preoperative patient counselling regarding pain management, multimodality nonopioid pain management, working with nursing to assess pain based on functional status rather than a 1- to 10-point scale, and avoiding opioid administration when possible. We also observed tremendous variability in patterns of opioid prescribing on review of our patient data. Part of this variability can be attributed to the fact that the responsibility of opioid prescribing largely falls on the rotating residents and fellows writing the prescriptions for discharge. This process likely resulted in a wide range of doses as well as high doses seen in group 1 patients. Most of the prescribing house officers are from the head and neck surgery service or surgical oncology service, where they may have become accustomed to prescribing higher doses of opioids for larger resections and generally more painful operations compared with thyroid and parathyroid procedures. Therefore, their overprescribing for the endocrine procedures is not surprising. In addition, the use of electronic medical records with preprogrammed postsurgical order sets may also have contributed to the higher amounts in group 1. The use of an automatic opioid order with a large range, such as 5 to 15 mg of oxycodone hydrochloride every 3 hours, appears to be associated with a higher number of pills prescribed. With our electronic medical record system, these orders can be turned into outpatient prescriptions. When creating the prescription, if the option of number of days to prescribe is selected rather than the actual number of pills to prescribe, the prescription automatically calculates the total number of pills based on the higher range. Although the overall prescribed doses for group 2 are significantly lower, we found a wide range in doses prescribed. This range is likely attributed again to prescriptions being written by trainees and to the fact that a few of the surgeons at our institution had yet to move toward the practice of reducing opioid prescribing for endocrine surgery.
Our data suggest that the estimated largest possible difference in the amount of opioid prescribed between groups 1 and 2 is 116.19 MME for hemithyroidectomy, 141.36 MME for total thyroidectomy, and 109.12 MME for parathyroidectomy (the upper bounds of the 95% CI reported). This difference was achieved by instituting preoperative patient counseling, working with perioperative nursing toward the same goal, and educating house officers. The significantly lower doses of opioid prescribed in group 2, particularly during the last 6 months of the study period, suggest that the postoperative opioid need for patients undergoing thyroid and parathyroid procedures is minimal, if at all. The fact that very few patients called back for opioid refills in the group prescribed a lesser quantity supports this. A previous study by Lou and colleagues10 prospectively evaluated the quantity of postoperative opioid requirements after thyroid and parathyroid surgery and found that 83% of these patients took less than 10 MME postoperatively. In the last year, several of our surgeons in our Thyroid and Parathyroid Center at OHSU moved toward reducing opioid prescribing by aggressively pursuing the use of multimodality, nonopioid pain management strategies, such as acetaminophen administration preoperatively and local anesthesia with superficial cervical blocks intraoperatively, while maintaining appropriate pain control for the opioid-naive patients. Several prospective studies have shown the efficacy of intraoperative cervical blocks during thyroidectomy is effective in reducing postoperative opioid needs.11,12,13,14 Furthermore, the use of preoperative acetaminophen has also been shown to be effective in reducing postoperative opioid needs.15 Our current postoperative management also focuses on maximizing nonopioid pain management strategies such as liberal use of ice packs, throat lozenges, acetaminophen, and nonsteroidal anti-inflammatory drugs and reserving opioids for severe pain.
In our study, although the mean MME being prescribed was significantly reduced in group 2, the amounts being administered in the postoperative anesthesia care unit varied widely. This approach of judicious use of opioid required cooperation from the perioperative nursing team and educating them on how to better assess the character of postoperative pain in this patient population. It is not uncommon for these patients to have a sore throat due to the larynx rotating around the endotracheal during retraction of the thyroid and tracheal, and posterior neck muscle ache due to neck extension, both of which could be effectively managed without opioids.
The group that was prescribed a lower dose or no opioid appeared to be less likely to call in for a refill. Thirty-four of the 53 patients who called for refills were prescribed more than 100 MME, whereas none of the patients who received less than 75 MME or were not prescribed any opioids at discharge called for an additional or a new opioid prescription. This finding is partly attributed to preoperative education on pain management and setting expectations for opioid prescriptions. Consistent preoperative discussion with the patients about what to expect with respect to postoperative pain and its management occurred most often with the 2 attending surgeons who did not prescribe any opioids. Our results indicate that to successfully implement nonopioid pain management in opioid-naive patients, surgeons need to preoperatively educate the patient regarding postoperative pain expectation and management strategy. Research has shown that effective communication in the preoperative setting can significantly reduce postoperative opioid use and that 90% of patients who were counselled preoperatively and received preoperative oral and written education regarding pain declined opioids postoperatively.16 The ability to electronically prescribe opioids in our institution allows us to address the patient’s need promptly after discharge should it be necessary. For institutions that are not allowed to prescribe electronically, sending patients home without any opioids may not be feasible. In that setting, a small quantity of opioid prescription may be necessary. Based on the study by Lou et al,10 approximately 10 to 20 MME would seem reasonable.
Limitations
The main limitation of this study is that, although it captured the prescribed dose, it did not capture the actual quantity of opioid consumed by patients at home. Prospective studies with a large cohort, ideally multi-institutional, that actually capture amount of medication consumed are needed to accurately assess what the true opioid requirements are for thyroid and parathyroid surgery. Developing an opioid prescribing guideline specific to these procedures would allow surgeons to comfortably prescribe just the minimum amount for same-day discharge. Patients receiving opioids for chronic pain are not included in this study and require a different approach to pain management. Our current approach for these patients is to work with the physician managing the patient’s pain medication and formulate a plan such that the patient is prescribed very little additional opioids, if any, on discharge. Our institution is currently reviewing the data on this group of patients.
Conclusions
Results of this study suggest that patients undergoing thyroid and parathyroid surgery need very little, if any, postoperative opioids. Preoperative counselling of patients regarding pain and adding nonopioid adjuncts can help to minimize the quantity of opioids that are used. These patients have relatively little postoperative pain that can be potentially controlled entirely with nonopioid medications. Decreasing the volume of opioid medication prescribed at discharge will decrease waste and reduce potential for addiction.
References
- 1.Centers for Disease Control and Prevention National Center for Injury Prevention and Control . Annual Surveillance Report of Drug-Related Risks and Outcomes — United States, 2017. Surveillance Special Report 1. https://www.cdc.gov/drugoverdose/pdf/pubs/2017-cdc-drug-surveillance-report.pdf. Updated August 31, 2017. Accessed April 2, 2018.
- 2.Centers for Disease Control and Prevention National Center for Health Statistics . Provisional Drug Overdose Death Counts. https://www.cdc.gov/nchs/nvss/vsrr/drug-overdose-data.htm. Updated March 13, 2018. Accessed April 2, 2018.
- 3.Dowell D, Haegerich TM, Chou R. CDC guidelines for prescribing opioids for chronic pain: United States, 2016. JAMA. 2016;315(15):1624-1645. doi: 10.1001/jama.2016.1464 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Hill MV, McMahon ML, Stucke RS, Barth RJ Jr. Wide variation and excessive dosage of opioid prescriptions for common general surgical procedures. Ann Surg. 2017;265(4):709-714. doi: 10.1097/SLA.0000000000001993 [DOI] [PubMed] [Google Scholar]
- 5.Mutlu I, Abubaker AO, Laskin DM. Narcotic prescribing habits and other methods of pain control by oral and maxillofacial surgeons after impacted third molar removal. J Oral Maxillofac Surg. 2013;71(9):1500-1503. doi: 10.1016/j.joms.2013.04.031 [DOI] [PubMed] [Google Scholar]
- 6.Stanek JJ, Renslow MA, Kalliainen LK. The effect of an educational program on opioid prescription patterns in hand surgery: a quality improvement program. J Hand Surg Am. 2015;40(2):341-346. doi: 10.1016/j.jhsa.2014.10.054 [DOI] [PubMed] [Google Scholar]
- 7.Bates C, Laciak R, Southwick A, Bishoff J. Overprescription of postoperative narcotics: a look at postoperative pain medication delivery, consumption and disposal in urological practice. J Urol. 2011;185(2):551-555. doi: 10.1016/j.juro.2010.09.088 [DOI] [PubMed] [Google Scholar]
- 8.Brummett CM, Waljee JF, Goesling J, et al. New persistent opioid use after minor and major surgical procedures in US adults. JAMA Surg. 2017;152(6):e170504. doi: 10.1001/jamasurg.2017.0504 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Durlak JA. How to select, calculate, and interpret effect sizes. J Pediatr Psychol. 2009;34(9):917-928. doi: 10.1093/jpepsy/jsp004 [DOI] [PubMed] [Google Scholar]
- 10.Lou I, Chennell TB, Schaefer SC, et al. Optimizing outpatient pain management after thyroid and parathyroid surgery: a two-institution experience. Ann Surg Oncol. 2017;24(7):1951-1957. doi: 10.1245/s10434-017-5781-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Bagul A, Taha R, Metcalfe MS, Brook NR, Nicholson ML. Pre-incision infiltration of local anesthetic reduces postoperative pain with no effects on bruising and wound cosmesis after thyroid surgery. Thyroid. 2005;15(11):1245-1248. doi: 10.1089/thy.2005.15.1245 [DOI] [PubMed] [Google Scholar]
- 12.Aunac S, Carlier M, Singelyn F, De Kock M. The analgesic efficacy of bilateral combined superficial and deep cervical plexus block administered before thyroid surgery under general anesthesia. Anesth Analg. 2002;95(3):746-750. [DOI] [PubMed] [Google Scholar]
- 13.Dieudonne N, Gomola A, Bonnichon P, Ozier YM. Prevention of postoperative pain after thyroid surgery: a double-blind randomized study of bilateral superficial cervical plexus blocks. Anesth Analg. 2001;92(6):1538-1542. doi: 10.1097/00000539-200106000-00038 [DOI] [PubMed] [Google Scholar]
- 14.Cai HD, Lin CZ, Yu CX, Lin XZ. Bilateral superficial cervical plexus block reduces postoperative nausea and vomiting and early postoperative pain after thyroidectomy. J Int Med Res. 2012;40(4):1390-1398. doi: 10.1177/147323001204000417 [DOI] [PubMed] [Google Scholar]
- 15.Doleman B, Read D, Lund JN, Williams JP. Preventive acetaminophen reduces postoperative opioid consumption, vomiting, and pain scores after surgery: systematic review and meta-analysis. Reg Anesth Pain Med. 2015;40(6):706-712. doi: 10.1097/AAP.0000000000000311 [DOI] [PubMed] [Google Scholar]
- 16.Sugai DY, Deptula PL, Parsa AA, Don Parsa F. The importance of communication in the management of postoperative pain. Hawaii J Med Public Health. 2013;72(6):180-184. [PMC free article] [PubMed] [Google Scholar]