

Abstract
Objective: To discuss the classification, management and outcome of fractures of the ulnar coronoid process.
Methods: Retrospective analysis was carried out in 31 patients (19 men and 12 women of average age 29.8 years [range, 18–52 years]) with fractures of the ulnar coronoid process. The fractures were classified into four major groups based on the extent of injury to the ulnar coronoid process, the state of the anterior bundle of the ulnar collateral ligaments (UCL) and elbow stability. A fracture of the coronoid process less than halfway up was defined as type I (eleven cases); of the middle of the coronoid process with injury of the UCL as type II (nine cases); of the base of coronoid process with dislocation of the elbow joint, sometimes with injury of the UCL, as type III (six cases); and severe comminuted fracture of the coronoid process with elbow instability as type IV (five cases). We chose treatment according to the type of injury.
Results: Follow‐up was 18–72 months (average 28.6 months). All patients achieved fracture union without inflammation, neural injuries or elbow instability. One type III and two type IV patients had traumatic osteoarthritis, and two type III and two type IV developed heterotopic ossification. There was a statistically significant difference between the ranges of movement of the two‐side joints in type IV.
Conclusion: We choose conservative treatment for type I fractures unless the bone fragment affected movement of the elbow joint, in which case we chose operative treatment so that elbow stability was not affected. Type II and type III fractures with elbow instability were reduced by internal fixation and the ligament repaired or reconstructed. In type IV cases, bone reconstruction was necessary to recover elbow stability. Proper post‐operative rehabilitation can decrease the occurrence of traumatic osteoarthritis.
Keywords: Elbow joint, Joint instability, Ulnar fractures
Introduction
The study of traumatic elbow instability has recently been focused on fractures of the coronoid process of the ulna 1 , 2 , 3 , 4 . Ulnar coronoid process fractures often result in elbow joint instability 1 . Over the last few years, we have recognized that ulnar coronoid fracture is much more complex than we had thought. Regan and Morrey classified ulnar coronoid process fractures into three types 5 , but did not take into account ulnar coronoid process fractures with injury of the ulnar collateral ligaments (UCL), severe comminuted fracture with elbow instability and reconstruction of the ulnar coronoid process. So we suggest here a relatively rational and comprehensive method of classification according to the clinical findings, and study the individual treatment of different types of fracture. The purpose of this report is to call attention to these fractures. This retrospective study was to review our experience and results in the treatment of fracture of the ulnar coronoid process.
Materials and methods
Materials
Thirty‐one patients with a fracture of the coronoid process of the ulna were treated between February 1998 and April 2004 in the affiliated hospital of Nantong university. There were 19 men and 12 women with an average age of 29.8 years (range, 18 to 52 years). The fracture was in the left arm in 9 patients, and the right in 22. The dominant arm was involved in all 31 patients. The injuries all resulted from falls from standing height on to the outstretched hand (the humerus impacting on the ulnar coronoid process with the elbow extended). There was associated dislocation of the elbow joint in nine patients and concomitant fracture of the radial head in three patients. All patients were treated for acute injury and diagnosed in our hospital.
Classification of coronoid process fractures
On the basis of the radiographs and operative findings, the size and location of fragments, the presence or absence of injury to the anterior bundle of the medial collateral ligaments, and elbow stability, the fractures were categorized into four types: Type I –avulsion of the tip of the coronoid process, the fragment involving less than 50% of the coronoid process (Fig. 1); Type II –fracture involving 50% of the coronoid process (Fig. 2a) and therefore compromising the insertion of the anterior bundle of the UCL, this type is always associated with injury of the anterior bundle of the UCL; Type III –fracture at the base of the coronoid process combined with dislocation of the elbow joint, the UCL may or may not be injured (Fig. 3a,b); Type IV—severe comminuted fracture of the coronoid process combined with elbow instability. Reconstruction of the ulnar coronoid process and the anterior bundle of the UCL are required for this type (Fig. 4a,b). Eleven patients had a Type I fracture, that is a simple fracture of the ulnar coronoid process without instability of the elbow; nine had a type II fracture with a positive valgus stress test, indicating damage to the UCL; dislocation or subluxation of the elbow occurred in six patients with type III fracture, who therefore required mobilization of the elbow; five patients had a type IV fracture, that is a severe comminuted fracture with instability of the elbow. Among the 31 patients, none had a sagittal fracture.
Figure 1.

Oblique radiograph demonstrating a type I fracture of the coronoid process.
Figure 2.

Type II fracture of the coronoid process. (a) Lateral radiograph showing that the fracture involves 50% of the coronoid process. (b, c) Immediate postoperative radiographs showing anatomical reduction maintained by K‐wires.
Figure 3.

Type III fracture of the coronoid process. (a) Anterior‐posterior (AP) and (b) lateral radiographs demonstrating a basal coronoid fracture and posterior dislocation of the elbow. (c) AP and (d) lateral radiographs showing anatomical reduction maintained by two lag screws.
Figure 4.
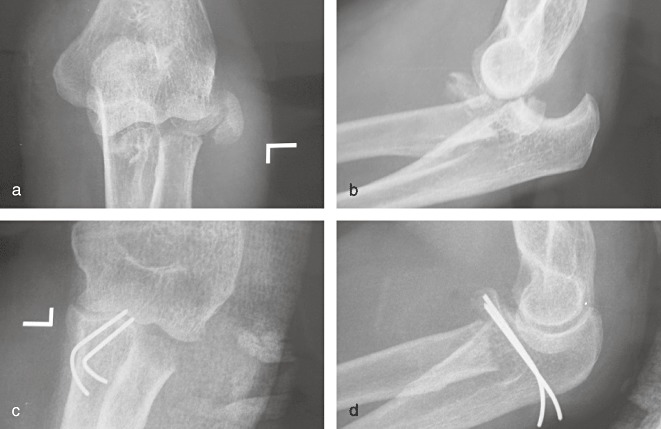
Type IV fracture of the coronoid process. (a) AP and (b) lateral radiographs demonstrating severe comminuted fractures of both the coronoid process and the radial head. (c) AP and (d) lateral radiographs showing reconstruction of the coronoid process with two K‐wires.
The principles for treating ulnar coronoid process fracture
Our study has shown that fracture of the ulnar coronoid process involving 50% or less of it will not result in posterior dislocation of the elbow. Patients with Type I fracture without displacement of the fragment are treated by immobilization of the elbow with a cast or splint for 4 weeks. Operative treatment is chosen when the fragment is displaced. General anatomic study shows that the anterior bundle of the UCL lies halfway up the ulnar coronoid, so the anterior part of the UCL will be damaged if the fragment involves 50% of the process. Therefore, the UCL must be repaired or reconstructed in patients with type II fracture. Patients with type III fracture associated with instability of the elbow joint should be treated operatively, including exploring for injury to the UCL 6 . As severe coronoid process fractures are difficult to reduce by internal fixation, in patients with type IV fracture the ulnar coronoid process should be reconstructed by autologous bone grafting to restore half its height, and the UCL should be reconstructed to avoid instability of the elbow joint 7 , 8 .
Among the eleven patients with type I fracture, nine were treated by immobilization of the elbow for 4 weeks with a long arm cast or splint, then the fixation was taken off to allow exercises to restore mobility. Twenty‐two patients were treated operatively; including two with type I fracture, in whom loose bodies had to be removed as they would have affected the range of movement of the elbow joint. Of the nine patients with type II fracture associated with injury of the anterior bundle of the UCL, six were treated by direct suture of the ligaments; three were treated by reconstruction of the anterior bundle of the UCL at its insertion, and the fractures of coronoid process were fixed with K‐wires (Fig. 2b,c). Six patients with type III fracture, including four with a concomitant injury of the anterior bundle of the UCL, were treated by open reduction and internal fixation combined with ligament suturing (Fig. 3c,d). Of the five patients with type IV fracture, four were treated by reconstruction of the ulnar coronoid process using autologous iliac crest bone graft. The remaining patient, who had a fracture of the radial head, was treated by reconstruction of the coronoid process with a fragment of the radial head after radial head excision 9 , and reconstruction of the anterior bundle of the UCL with the tendon of palmaris longus (Fig. 4c,d).
Treatment
In the twenty‐two patients treated operatively, brachial plexus anesthesia and tourniquet were used. The incision extended from 1 cm proximal to the medial epicondyle to 3 cm above the ulnar coronoid process. The vena basilica and the posterior antebrachial cutaneous nerve were protected when the skin and superficial fascia was incised. The anterior bundle of the UCL and the capsule were exposed between the two heads of the flexor carpi ulnaris muscle. The ulnar nerve was protected when the UCL was separated. For the patients with type I fracture, the capsule was incised and the loose bodies removed before suturing the capsule. In the patients with type II or III fracture, the fragment was fixed to the damaged site with Kirschner pins or screws and the anterior bundle of the UCL was explored. If the anterior bundle of the UCL was injured, it was sutured directly or secured to the medial part of coronoid process through drilled holes. For patients with type IV fracture, loose bodies were removed, then autologous bone grafting (always using autologous iliac crest bone) was performed to reconstruct the ulna coronoid process to achieve half the height of the ulna, the anterior bundle of the UCL was reconstructed with the tendon of palmaris longus through holes drilled from the epicondyle to the medial part of the reconstructed coronoid process. Some data suggest that the anterior bundle of the UCL is at tension when the elbow is flexed to 45° 10 . The surgery was conducted by the same surgeon using 3‐0 tendon suture.
Postoperative treatment
Among the patients treated operatively, the two with type I fracture were encouraged to mobilize the elbow on the second day without a cast or postoperative splint. The remaining patients were treated by immobilization of the elbow with a cast or splint for 4 weeks. Rehabilitation was undertaken after removing the cast or splint. The Kirschner pins and screws were taken out after the bone had healed.
Statistical analysis
The Stata 7.0 (Stata, College Station, TX, USA) was adopted. The final outcome was evaluated by paired t‐test comparing the movement of the elbow joint of the normal and injured sides. We considered differences significant when P < 0.05.
Results
General condition
Among the 31 patients, 22 were treated surgically. The average time to bone union was 7.8 weeks (range, 8–10 weeks). The average duration of follow‐up for the 31 patients was 28.6 months (range, 18–72 months). All patients were subjectively satisfied with the final outcome. At the final follow‐up three patients, including one with type III fracture and two with type IV had developed traumatic osteoarthritis; and heterotopic ossification had occurred in four patients, including two with type III fracture and two with type IV. None had the complications of inflammation or neuropathies. All patients returned to their previous employment except for one with type IV fracture who had stiffness of the elbow joint postoperatively.
Pain
At the final follow‐up, six patients including one with type I fracture, two with type II and three with type IV complained of occasional pain on a rainy day or at the extremes of flexion and extension. None of the remaining twenty‐five patients had significant pain.
Movement of the elbow joint
The patients were evaluated according to the system of Broberg and Morrery 9 . It is a 100‐point system based on movement (40 points), strength (20 points), stability (5 points) and pain (35 points). Categorical ratings were assigned, with 95–100 points rating as excellent, 80–94 as good, 60–79 as fair and <60 as a poor result. The results were categorized as excellent in twenty‐five patients (eleven type one, eight type II, five type III, one type IV), good in four (one type II, one type III, two type IV), fair in one (one type IV), and poor in one (type IV). Heterotopic ossification occurred in four patients, including two with type III fracture and two with type IV fracture, two of four patients had gross restriction of the elbow joint. One of them, who had a second surgery to resect the heterotopic bone, ultimately achieved a fair result. The other patient who underwent a second surgery had radiographic signs of severe traumatic arthritis and restriction of the elbow joint postoperatively, leading to a poor result. Another patient with type IV fracture who had restriction of the elbow joint with traumatic osteoarthritis and swollen soft‐tissue achieved a fair result.
Statistical analysis showed no significant difference between the normal and injured sides with regard to the range of movement of the elbow joint for types I–III. For type IV, there was a significant difference, which shows that type IV affects the stability of the elbow joint, and that reconstruction of the ulna coronoid process and the anterior bundle of the UCL affects the range of movement of the elbow joint (Table 1).
Table 1.
Comparison between the normal and injured sides of range of movement of the elbow joint
| Type | Cases | Normal side | Injured side | t value | P value |
|---|---|---|---|---|---|
| I | 11 | 148.2°± 2.4° | 144.8°± 2.6° | 1.62 | >0.05 |
| II | 9 | 145.4°± 2.1° | 140.3°± 3.3° | 1.46 | >0.05 |
| III | 6 | 146.0°± 3.2° | 134.6°± 3.8° | 1.81 | >0.05 |
| IV | 5 | 145.8°± 2.4° | 91.6°± 9.7° | 5.47 | <0.05 |
Discussion
The effect of the ulna coronoid process on stability of the elbow joint
The coronoid process of the ulna has been recognized as the keystone of the elbow–a critical element for stable, effective elbow function 11 , and for resisting the stress of the biceps brachii, musculus brachialis and triceps, which draws the elbow joint backwards 12 . The anterior bundle of the UCL lies along the middle of the ulna coronoid process, so ulnar coronoid process fracture is always associated with injury to the UCL.
The anterior bundle of the medial collateral ligament is the strongest and stiffest elbow collateral ligament, maintaining stability of the elbow joint to valgus stress 13 . According to Heim's four column theory (the ring maintaining the elbow), the ulnar coronoid is the main part of the anterior and medial columns of the elbow. So for patients with ulnar coronoid process fracture, reconstruction of the height and shape of the ulna coronoid process is necessary, and operative repair or reconstruction of the anterior bundle of the UCL is also typically required.
The mechanism of ulnar coronoid process fractures
The movements of the elbow joint include flexion and extension, and posterior dislocation is common. The mechanism of injury involves an axial load with varus torque usually from a fall on the outstretched hand (the ulnar coronoid process impacted against the humerus), and is usually associated with injury to the UCL. Patients with ulnar coronoid process fracture and injury to the UCL usually have recurrent dislocation or persistent subluxation of the elbow when treated inadequately 14 . In this series of patients, due to timely treatment there were no cases with habitual dislocation.
The diagnosis and treatment of ulnar coronoid process fractures
Morrey et al. thought that the ulnar coronoid process might be an indicator of elbow stability, as fracture of the coronoid process is always accompanied by injury to the UCL 15 . So it is important to correctly diagnose and treat fracture of the ulnar coronoid process combined with injury to the UCL. An ulnar coronoid process fracture with injury to the UCL should be considered when a patient complains of instability, pain, swelling and limitation of movement. Some fractures or dislocations of the elbow joint can be recognized by routine X‐ray assessment (anteroposterior and lateral view). However ulnar coronoid process fracture is easily missed because the ulnar coronoid process overlaps the radial head on lateral X‐ray film. In this series of 31 patients, seven fractures were not seen on routine X‐ray examination; including two with type I fracture, four with type II, and one with type III; instead they were diagnosed by oblique X‐ray examination. So it is suggested that not only routine radiographs but also an oblique radiograph of such patients should be taken. If the films are ambiguous for diagnosis of coronoid process fracture, valgus stress testing of the elbow should be performed and compared to the opposite elbow, and arthrography, arthroscopy, and MRI are also encouraged for further evaluation 11 .
The treatment is different according to the type of ulnar coronoid process fracture. Traditionally, Regan and Morry's 5 classification of coronoid fractures is based on the anterior‐to‐posterior size of the fracture fragment, with a modifier to indicate the presence or absence of elbow dislocation: Type I–avulsion of the tip of the coronoid process, which does not require internal fixation; Type II–a single or comminuted fragment involving 50% or less of the process, which has a potential risk of recurrent dislocation of the elbow; Type III–a single or comminuted fragment involving more than 50% of the process, which requires secure internal fixation for stability of the elbow and early rehabilitation. More recently, coronoid process fractures have been classified according to the location and morphology of the fragment, which determines the overall pattern of elbow injury and thereby helps to guide treatment of ulnar coronoid process fracture 16 .
However, the current accepted classification may be too simplistic to characterize fracture of coronoid fully, as it does not consider the absence or presence of UCL injury and its implications for elbow joint instability. According to anatomical and clinical data, the anterior bundle of the UCL lies halfway up the ulnar coronoid process, so a fracture here is usually combined with injury of the UCL 17 , 18 . The anterior bundle of the UCL is the major part of the UCL, and it maintains stability of the elbow in regard to valgus stress 13 . So injury to the anterior bundle of the UCL should be taken into account with regard to the classification of coronoid process fractures.
In this series of patients, according to our classification, nine with type II fracture had a concomitant injury of the anterior bundle of the UCL, and four of six patients who sustained a type III fracture had associated injury of the anterior bundle of the UCL. These were managed by open reduction and internal fixation, combined with repair or reconstruction of the anterior bundle of the UCL. At final follow‐up, valgus stress test of the elbow failed to show any significant instability of the elbow. It has been recommended by Shiba et al. that any free fracture fragment should be removed because of its effect on flexion of the elbow in patients with severe coronoid process fracture 19 . Reconstruction of the ulnar coronoid process and the anterior bundle of the UCL is required for patients with severe coronoid process fracture (type IV). At final follow‐up, four of the five patients with type IV fracture showed stability of the elbow, and were able to return to their previous employment and their avocation. The remaining patient had a limited range of movement of the joint resulting from reconstruction of bone without articular cartilage, leading to traumatic arthritis postoperatively. Moritomo et al. have reported good results from using an osteocartilaginous graft from the ipsilateral olecranon to replace congruent articular cartilage where it is missing from the joint surface 20 . Therefore, reconstruction using osteocartilaginous grafts with a blood supply or an ulnar coronoid process prosthesis should be adopted for the restoration of the elbow joint and minimizing the occurrence of elbow degeneration and osteoarthritis.
References
- 1. Pugh DM, Wild LM, Schemitsch EH, et al. Standard surgical protocol to treat elbow dislocations with radial head and coronoid fractures. J Bone Joint Surg Am, 2004, 86: 1122–1130. [DOI] [PubMed] [Google Scholar]
- 2. Ring D, Jupiter JB, Zilberfarb J. Posterior dislocation of the elbow with fractures of the radial head and coronoid. J Bone Joint Surg Am, 2002, 84: 547–551. [DOI] [PubMed] [Google Scholar]
- 3. Ring D, Jupiter JB. Fracture‐dislocation of the elbow. J Bone Joint Surg Am, 1998, 80: 566–580. [PubMed] [Google Scholar]
- 4. McKee MD, Pugh DM, Wild LM, et al. Standard surgical protocol to treat elbow dislocations with radial head and coronoid fractures. Surgical technique. J Bone Joint Surg Am, 2005, 87 (Suppl. 1): S22–S32. [DOI] [PubMed] [Google Scholar]
- 5. Regan W, Morrey B. Fractures of the coronoid process of the ulna. J Bone Joint Surg Am, 1989, 71: 1348–1354. [PubMed] [Google Scholar]
- 6. Durig M, Muller W, Ruedi TP, et al. The operative treatment of elbow dislocation in the adult. J Bone Joint Surg Am, 1979, 61: 239–244. [PubMed] [Google Scholar]
- 7. O'Driscoll SW, Morrey BF, Korinek S, et al. Elbow subluxation and dislocation. A spectrum of instability. Clin Orthop Relat Res, 1992, 280: 186–197. [PubMed] [Google Scholar]
- 8. Broberg MA, Morrey BF. Results of treatment of fracture‐dislocations of the elbow. Clin Orthop Relat Res, 1987, 216: 109–119. [PubMed] [Google Scholar]
- 9. Broberg MA, Morrey BF. Results of delayed excision of the radial head after fracture. J Bone Joint Surg Am, 1986, 68: 669–674. [PubMed] [Google Scholar]
- 10. Wang YH, Ji B, Wu J, et al. Biomechanical and clinical study of the ulnar collateral ligaments of elbow joint (Chin). Jiepou Yu Linchuang, 2005, 10: 184–186. [Google Scholar]
- 11. Morrey BF, An KN. Stability of the elbow: osseous constraints. J Shoulder Elbow Surg, 2005, 14 (Suppl.): S174–S178. [DOI] [PubMed] [Google Scholar]
- 12. Cage DJ, Abrams RA, Callahan JJ, et al. Soft tissue attachments of the ulnar coronoid process. An anatomic study with radiographic correlation. Clin Orthop Relat Res, 1995, 320: 154–158. [PubMed] [Google Scholar]
- 13. Floris S, Olsen BS, Dalstra M, et al. The medial collateral ligament of the elbow joint: anatomy and kinematics. J Shoulder Elbow Surg, 1998, 7: 345–351. [DOI] [PubMed] [Google Scholar]
- 14. Ablove RH, Moy OJ, Howard C, et al. Ulnar coronoid process anatomy: possible implications for elbow instability. Clin Orthop Relat Res, 2006, 449: 259–261. [DOI] [PubMed] [Google Scholar]
- 15. Morrey BF, Askew LJ, An KN, et al. Rupture of the distal tendon of the biceps brachii. A biomechanical study. J Bone Joint Surg Am, 1985, 67: 418–421. [PubMed] [Google Scholar]
- 16. O'Driscoll SW, Jupiter JB, Cohen MS, et al. Difficult elbow fractures: pearls and pitfalls. Instr Course Lect, 2003, 52: 113–134. [PubMed] [Google Scholar]
- 17. Regan WD, Korinek SL, Morrey BF, et al. Biomechanical study of ligaments around the elbow joint. Clin Orthop Relat Res, 1991, 271: 170–179. [PubMed] [Google Scholar]
- 18. Matzon JL, Widmer BJ, Draganich LF, et al. Anatomy of the coronoid process. J Hand Surg Am, 2006, 31: 1272–1278. [DOI] [PubMed] [Google Scholar]
- 19. Shiba R, Sorbie C, Siu DW, et al. Geometry of the humeroulnar joint. J Orthop Res, 1988, 6: 897–906. [DOI] [PubMed] [Google Scholar]
- 20. Moritomo H, Tada K, Yoshida T, et al. Reconstruction of the coronoid for chronic dislocation of the elbow. Use of a graft from the olecranon in two cases. J Bone Joint Surg Br, 1998, 80: 490–492. [DOI] [PubMed] [Google Scholar]