

Abstract
Objective: To discuss imaging features of radiographs, computed tomography (CT), magnetic resonance imaging (MRI) and radionuclide imaging of the herniation pit of the femoral neck and their implications for pathogenesis.
Methods: Twenty‐seven patients with 31 herniation pits of the femoral neck were analyzed. All patients were examined by plain radiographs, 18 by CT, 16 by MRI, and 8 by radionuclide imaging.
Results: Thirty‐one herniation pits located in the anterior part of the femoral neck or the base of the femoral head were round, oval or ‘8’‐shaped subcortical defects. The pits were usually seen as mild radiolucent areas on radiographs, soft‐tissue attenuation with a thin sclerotic rim and a focal cortical perforation on CT and three different signal intensities on MRI. Only one of eight pits revealed mild focal increased uptake on bone radionuclide scans.
Conclusion: The occurrence of a herniation pit of the femoral neck correlates closely with the particulars of the structure of the hip joint and corresponding mechanical forces. Round or oval subcortical defects surrounded by a thin sclerotic rim in the superior lateral part of the femoral neck or the anterior lateral base of the femoral head, which are usually normal on radionuclide imaging and have focal cortical perforations on CT, are specific signs for diagnosing herniation pits of the femoral neck.
Keywords: Femur neck; Hernia; Magnetic resonance imaging; Radionuclide imaging; Tomography, X‐ray Computed
Introduction
In our daily practice, with the wide application of computed tomography (CT) and magnetic resonance imaging (MRI) of the hips, herniation pits of the femoral neck are increasingly identified. To our knowledge, since five herniation pits of the femoral neck were first described by Pitt et al. in 1982 1 , there have not been many cases reported in the English literature 2 , 3 , 4 , 5 , 6 , 7 , 8 , 9 , 10 .
In our study, in order to increase the accuracy of differential diagnosis, twenty‐seven cases with herniation pits are discussed with respect to their features in conventional radiographs, CT, MRI and radionuclide imaging as well as their pathogenesis.
Materials and methods
Patients
Twenty‐seven patients with herniation pits of the femoral neck were identified by pelvic and hip examinations between December 2000 and December 2008. All patients were diagnosed by surgical pathology or the classic imaging findings described by Pitt et al. 1 . The 27 patients (22 men and 5 women) were aged from 30 to 65 years with an average age of 45 years. Thirty‐one herniation pits of the femoral neck in all patients, involving unilateral (23 patients) or bilateral lesions (4 patients), were analyzed. Eight patients had mild hip pain and 19 patients remained asymptomatic.
Image techniques
All patients underwent anteroposterior pelvic and lateral hip radiography. CT examinations were performed in 18 patients. CT images were obtained from 5 mm scan sections and viewed at bone and soft‐tissue windows. No intravenous contrast medium was given. A 1.5‐T superconducting magnet scanner was used for 16 patients. With Torsopa coil, axial T1‐weighted spin‐echo images (time of repetition [TR] 400–600 ms/time of echo [TE] 9–25 ms), T2‐weighted fast spin‐echo images (TR 3000–4000 ms/TE 80–120 ms), and T2‐weighted frequency‐selective fat suppression images (TR 3000–4000 ms/TE 80–120 ms), as well as coronal T1‐weighted fast spin‐echo images (TR 400–600 ms/TE 9–25 ms) and T2‐weighted frequency‐selective fat suppression images (TR 3000–4000 ms/TE 80–120 ms) were obtained. The following parameters were the same for all sequences: slice thickness 4 mm with 1 mm interslice gap, field of view (FOV) 38 × 38 cm, matrix 512 × 224, and number of excitations (Nex) 2–4. The body positions in CT and MRI examinations were both supine. Radionuclide imaging was performed in eight patients 3 to 4 h after intravenous administration of 740 MBq of 99Tcm‐MDP with a Scophy Camera single photon emission computed tomography (SPECT) unit (Toshiba, Tokyo, Japan). Images were obtained with a low‐resolution parallel collimator.
Image analysis
All images were analyzed by three experienced radiologists and one nuclear‐medicine doctor.
Results
Radiographic manifestations
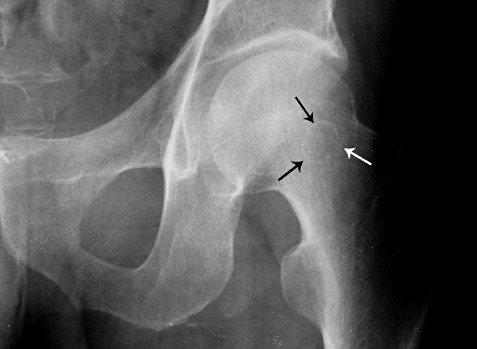
There were 31 herniation pits in the 27 patients who underwent radiographic examinations. Only 26 pits were visible on the plain radiographs. The other five pits were difficult to see on the plain films but showed on CT or MRI. Twenty‐six pits were located in different sites of the femoral neck on the anteroposterior radiographs, including 16 pits in the superior lateral base of the femoral head, nine in the superior lateral part of the femoral neck, and one in the midline of the femoral neck. However on the lateral radiographs, all pits were seen to be located either beneath the anterior surface of the femoral neck or at the base of the femoral head. Among 26 pits, 18 appeared round, one semi‐round, three oval and four ‘8’‐shaped. Eighteen pits revealed a mild radiolucent area which was surrounded by a thin clear sclerotic margin of thickness less than 2 mm in 14 pits (1, 2), a blurred margin in three pits, and without an obvious rim in one pit. The other eight pits showed a thin clear sclerotic ring with almost normal density inside the ring (3, 4).
Figure 1.

Frontal radiograph of the right femoral neck showing an ‘8’ shaped radiolucent pit with a clear border in the superior lateral part (arrow).
Figure 2.
Frontal radiograph of the left femoral neck showing a well‐rounded pit with a mildly radiolucent area in the superior lateral part (arrows).
Figure 3.
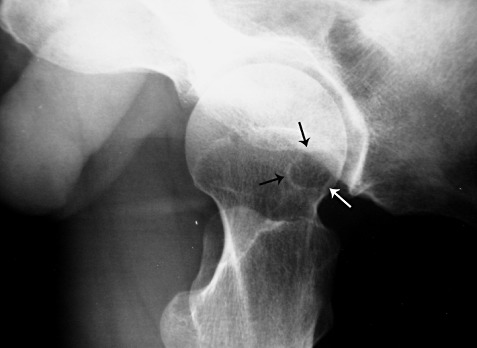
Lateral radiograph of the left femoral neck showing a well‐rounded pit beneath the anterior surface (arrows). (The same case as Fig. 2).
Figure 4.
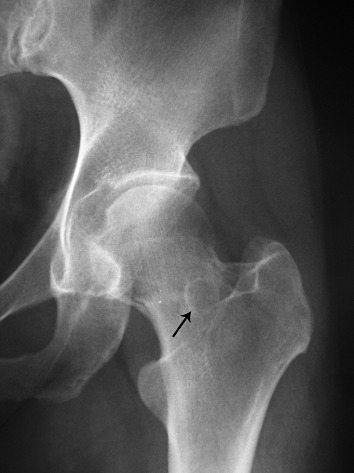
Frontal radiograph of the left femoral neck showing a well‐rounded pit with a thin clear sclerotic ring with normal density inside the ring (arrow).
CT manifestations
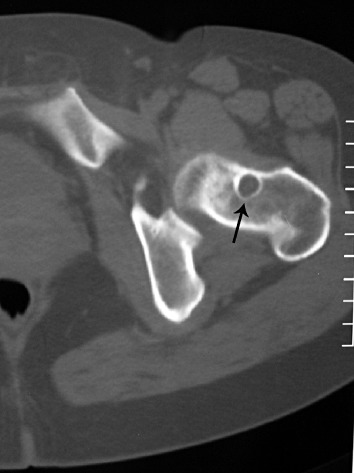
Twenty‐one pits were found in 18 patients by CT examination. Five of these 21 pits were not visible on the plain radiographs. CT revealed subcortical bone defects beneath the anterior surface of the femoral neck or the base of the femoral head. Among the 21 pits, 17 appeared round, two oval, and two ‘8’‐shaped. There were 19 pits of uniform soft‐tissue attenuation (5, 6), and two of fat‐like density (7, 8). Seventeen pits were surrounded by thin well‐demarcated sclerotic margins, two had ill‐demarcated margins, and two had no obvious rim. Twelve pits had a focal linear cortical perforation connected with the subcortical defect (Fig. 9). The size of all pits fell within the range of 1–13 mm and only two pits were larger than 10 mm. Eight patients with 11 pits underwent follow‐up studies for 5 months to 2.5 years after the original examination. No changes in the appearance and size of herniation pits were noted in 10 hips. However, in one pit in a soldier increasing size from 7 mm to 10 mm was demonstrated.
Figure 5.
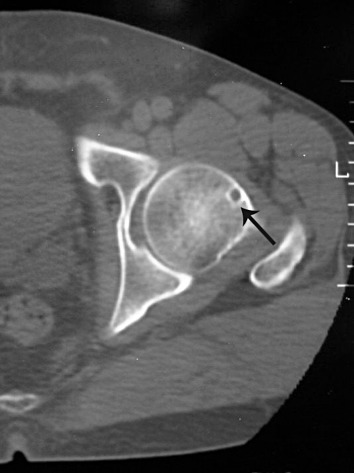
CT scan at bone window showing a pit of uniform soft‐tissue density beneath the anterior surface of the base of the left femoral head (arrow).
Figure 6.
CT scan at bone window showing a pit of uniform soft‐tissue density beneath the anterior surface of the left femoral neck (arrow).
Figure 7.
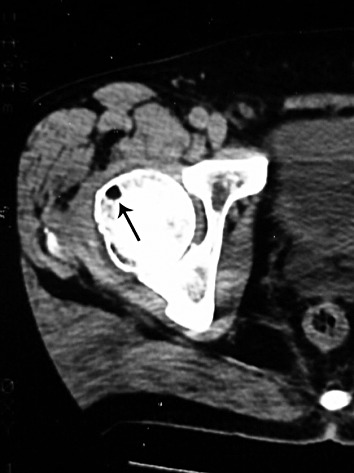
CT scan at soft‐tissue window showing a pit of uniform fat‐like density beneath the anterior surface of the base of the right femoral head (arrow). CT value within the pit is about −96 HU.
Figure 8.
CT scan at bone window showing a pit of uniform subcutaneous fat‐like density in the right femoral neck (arrow).
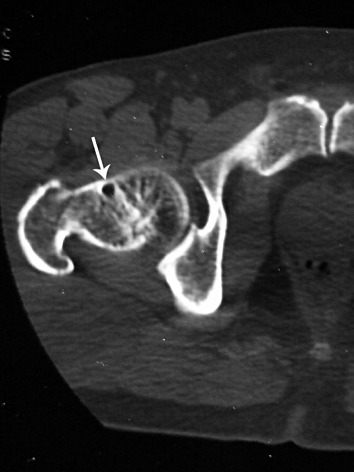
Figure 9.
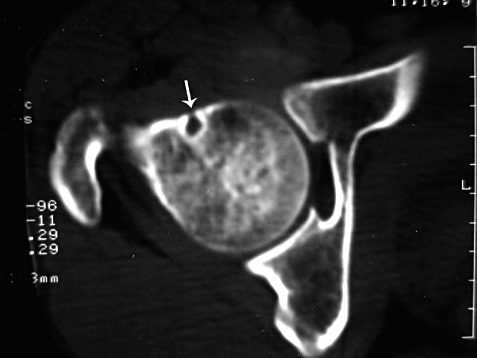
CT scan at bone window showing a pit with a focal linear cortical perforation connected with a focus in the anterior femoral neck (arrow).
MRI manifestations
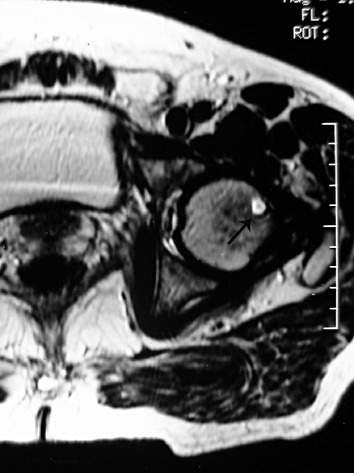
The 19 pits in 16 patients seen with MRI also showed on CT, but four of them were difficult to find on plain radiographs. The location of pits on the axial and coronal MRI was the same as that on CT and plain radiographs. Of the total of 19 pits, 14 appeared round, four oval, and one ‘8’‐shaped. Thirteen pits showed uniformly long T1 and T2 fluid‐like signals (10, 11, 12). There were four pits of uniformly low signal intensity on T1‐weighted images and unevenly high signal intensity on T2‐weighted images (13, 14). Two pits displayed uniformly fat‐like signal intensity on all sequences and became dark on T2‐weighted frequency‐selective fat suppression images (15, 16). Twelve of 16 pits were surrounded by a dark peripheral ring or arc on T2‐weighted images.
Figure 10.
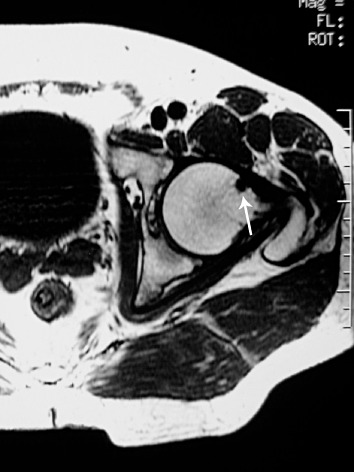
Axial T1‐weighted SE image showing a round pit of uniformly long T1 signal beneath the anterior surface of the base of the left femoral head (arrow).
Figure 11.
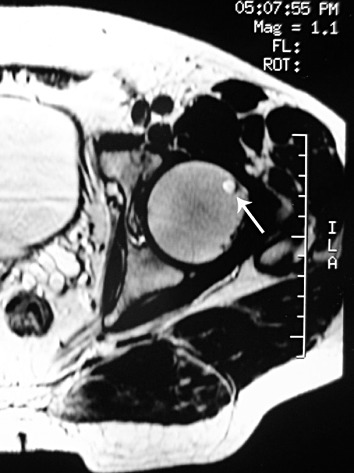
Axial T2‐weighted fast SE image showing a round pit of uniformly long T2 fluid‐like signal (arrow). (The same case as Fig. 10).
Figure 12.
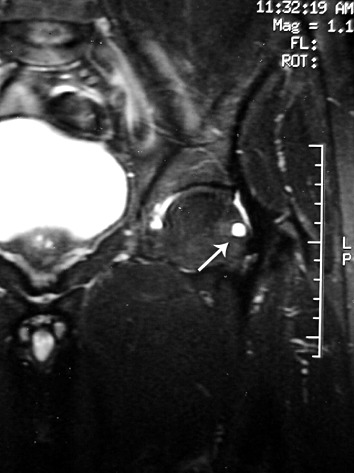
Coronal T2‐weighted frequency‐selective fat suppression image showing a pit of fluid‐like signal (arrow). (The same case as Fig. 10).
Figure 13.
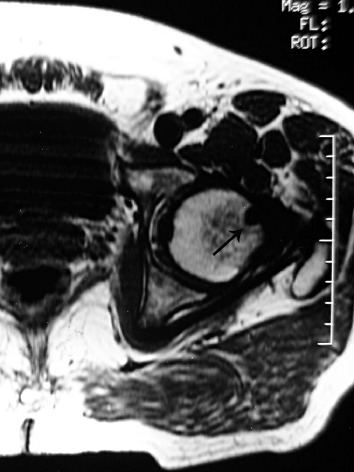
Axial T1‐weighted SE image showing a round pit of uniformly long T1 signal beneath the anterior surface of the base of the left femoral head (arrow).
Figure 14.
Axial T2‐weighted fast SE image showing a round pit of unevenly high signal intensity. The pit is surrounded by a dark peripheral arc (arrow). (The same case as Fig. 13).
Figure 15.

Axial T1‐weighted SE image showing a round pit of uniformly short T1 fat‐like signal intensity beneath the anterior surface of the femoral neck (arrow). (The same case as Fig. 8).
Figure 16.

Axial T2‐weighted fast SE image showing a pit of uniformly long T2 fat‐like signal (arrow). (The same case as Fig. 8).
Bone radionuclide imaging manifestations
Bone radionuclide imaging was done in eight patients. Ten pits were found in these eight patients by combining with the above three types of imaging modality. However, nine pits in seven patients appeared normal on bone radionuclide images except for one pit in one patient which showed an isolated focus of mild increase in activity in the same region as the pits displayed on the plain radiographs and MRI (Fig. 17).
Figure 17.
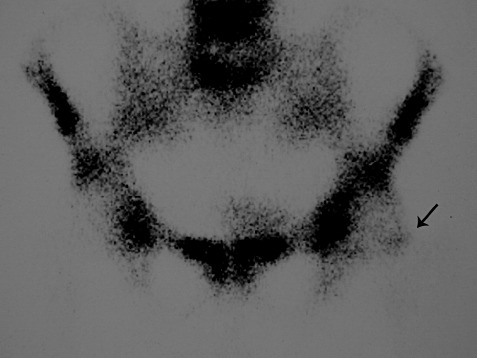
Bone radionuclide imaging showing an isolated focus of mild increased activity corresponding to the pit displayed on the MRI (arrow). (The same case as Fig. 12).
Discussion
Herniation pits of the femoral neck are benign bone pits which are located in the femoral neck or at the base of the femoral head. The prevalence of these pits is approximately 4%–5% in the adult population, and they are seen more often in older men than women 1 , 4 . In our study, the patients were predominately male and the average age was 45 years. Most herniation pits are found incidentally and not associated with obvious clinical symptoms 4 , 5 , 6 . These pits usually occur unilaterally and seldom in both hips. Correct imaging diagnosis of these pits would avert unnecessary surgical excision or biopsy.
The mechanism and follow‐up findings of herniation pits
Mechanical abrasive effects of the anterior hip capsule produce a ‘reaction area’ on the anterosuperior surface of the normal femoral neck. The surface ‘reaction area’ is the location of ingrowth of herniation pits and corresponds to the anterior overlying area of the zona orbicularis. In the ‘reaction area’, there is some fibrous tissue, neo‐cartilage, and reactive new bone which probably derive from synovial tissue 1 . Herniation of these fibrous and/or cartilaginous tissue and fluid elements into spongy bone probably occurs through the ‘reaction area’ under the pressure and mechanical abrasion of the anterior hip capsule, adjacent iliofemoral ligament and overlying iliopsoas muscle or tendon 1 , 5 , 7 . The anterior adjacent tissues overlying the hip capsule provide a ‘driving force’ when the hip alternates between extension and flexion during exercise.
Generally, most herniation pits show no change in appearance and size over short periods. However, a few pits can enlarge in the long term. The cases of growing herniation pits reported by Crabbe and Pitt were jogger, ballerina or dancer 8 . Our patient with an enlarging pit is a male soldier. It is possible that the growth of these pits is correlated with physical activities. Excessive movement of the hip may be a major contributing cause. Adult men often have more hip movement than adult women, which may be the reason for the higher incidence in men.
Imaging manifestations of herniation pits
The pit is usually round or oval and less than 10 mm in diameter. The central area of radiolucency is often surrounded by a narrow sclerotic border. The CT findings are characteristic, namely, a well‐defined subcortical lytic pit with a linear cortical perforation.
MRI manifestations depend on which histological tissues are within the lesion. If only fluid is present, the pit shows uniformly long T1 and T2 signal intensity. When both fibro‐connective tissue and fluid fill the cavity, the signal is not uniform. Amongst our cases two pits showed a pure fat‐like signal intensity on all sequences, suggesting the presence of a fat component, which has not been reported in the current literature. The pathogenesis of the two fatty pits is still unclear. We suspect that the fat component also comes from primitive synovial tissue. Most of the thin sclerotic margins around the pit on the plain radiographs or CT show dark peripheral rings or arcs on MRI. However, some margins do not show on MRI due to too thin or inapparent sclerotic margins, which may suggest these pits are in an early stage and the peripheral reactive new bone is less. Most pits are negative on bone radionuclide scans. An occasional pit shows a focus of mild increased uptake of radionuclide denoting active bone formation 9 , 10 .
The diagnosis and differential diagnosis of herniation pits
The diagnosis of herniation pits relies not only on the imaging features but also on the characteristic location, which includes the anterolateral base of the femoral head or in the superior lateral part of the femoral neck. Differential diagnosis should include intraosseous ganglia, osteoid osteoma, and degenerative cyst.
In femoral head necrosis, focal cystic pits usually occur in those hips which have specific diagnostic manifestations such as double line signs on MRI or blurred high density sclerotic lines on CT imaging. Intraosseous ganglia are beneath the articular surface and often lack linear cortical perforation on CT images. For osteoid osteoma, a spot or mass calcification within a low‐density nidus surrounded by a thicker sclerotic band is often found on CT. The osteoid matrix demonstrates low signal intensity on T1‐ and T2‐weighted imaging, while the nidus displays increased signal intensity on T2‐weighted imaging. Moreover, extralesional bone marrow edema can be seen on T2‐weighted frequency‐selective fat suppression images. Degenerative cysts associated with degenerative arthritis lie in the weight‐supporting area of the hip joint and are usually distributed in a cluster.
References
- 1. Pitt MJ, Graham AR, Shipman JH, et al. Herniation pit of the femoral neck. AJR Am J Roentgenol, 1982, 138: 1115–1121. [DOI] [PubMed] [Google Scholar]
- 2. Polger M, Aliabadi P. Radiologic vignette. The radiographic findings are typical of herniation pit of the femoral neck. Arthritis Rheum, 1993, 36: 572–574. [DOI] [PubMed] [Google Scholar]
- 3. Lee L, Manolios N, De Costa R, et al. Herniation pit of the femoral neck. J Rheumatol, 2000, 27: 2278–2280. [PubMed] [Google Scholar]
- 4. Nokes SR, Vogler JB, Spritzer CE, et al. Herniation pits of the femoral neck: appearance at MR imaging. Radiology, 1989, 172: 231–234. [DOI] [PubMed] [Google Scholar]
- 5. Daenen B, Preidler KW, Padmanabhan S, et al. Symptomatic herniation pits of the femoral neck: anatomic and clinical study. AJR Am J Roentgenol, 1997, 168: 149–153. [DOI] [PubMed] [Google Scholar]
- 6. Sopov V, Fuchs D, Bar‐Meir E, et al. Clinical spectrum of asymptomatic femoral neck abnormal uptake on bone scintigraphy. J Nucl Med, 2002, 43: 484–486. [PubMed] [Google Scholar]
- 7. Schedel H, Wicht L, Maurer J, et al. Differential diagnosis in variants or abnormalities of the hip on MRI. Bildgebung, 1994, 61: 20–24. [PubMed] [Google Scholar]
- 8. Crabbe JP, Martel W, Matthews LS. Rapid growth of femoral herniation pit. AJR Am J Roentgenol, 1992, 159: 1038–1040. [DOI] [PubMed] [Google Scholar]
- 9. Swayne LC, Colston WC. Scintigraphic findings of a femoral neck herniation pit. Clin Nucl Med, 1996, 21: 258. [DOI] [PubMed] [Google Scholar]
- 10. Thomason CB, Silverman ED, Walter RD, et al. Focal bone tracer uptake associated with a herniation pit of the femoral neck. Clin Nucl Med, 1983, 8: 304–305. [DOI] [PubMed] [Google Scholar]