

Abstract
Objective: To study the asphericity of the femoral head in femoroacetabular impingement using the radiological indices alpha angle and triangular index, and correlation with risk factors.
Methods: The study was conducted retrospectively from January 2008 to June 2010 on 50 consecutive patients with suspected cam type femoroacetabular impingement of the hip who reported to the orthopaedics outpatients department of the Postgraduate Institute of Medical Education and Research. Ten controls were also used in the study. Radiographs of the affected hip were taken and then the alpha angle and triangular index were measured and correlated with various risk factors.
Results: In the anteroposterior view the alpha angle range was from 55° to 106° for the cases and from 54° to 70° for the controls. In the lateral view the range was from 62° to 104° for the cases and from 54° to 62° for the controls. The mean alpha angle in the anteroposterior view was measured as 75°± 10° in the cases and 61°± 6° in the controls, and the mean in the lateral view was 74°± 8° in the cases and 58°± 6° for the controls. The triangular index range in the radiographs was from 1 to 7 in the cases and from 0 to 1 for the controls. The mean triangular index in the radiographs was 2.9 ± 1.2 for the cases and 0.2 ± 0.4 for the controls.
Conclusion: There was no significant correlation between the age and gender of the patient and the femoroacetabular impingement. However, there was significant correlation between the body mass index of the patient and the femoroacetabular impingement.
Keywords: Epidemiological factors, Femoroacetabular impingement, Hip joint
Introduction
Femoroacetabular impingement is a condition of abnormal contact, which might arise as a result of either an abnormal morphological feature involving the proximal femur and/or the acetabulum. It might occur in patients with otherwise normal or near normal anatomic structure of the hip who experience impingement as a result of subjecting the hip to excessive and supra‐physiological range of movement 1 , 2 . Often a combination of factors might lead to femoroacetabular impingement.
Femoroacetabular impingement as a cause of early degenerative changes in the hips of young adults has been recognized and described only recently 2 , 3 , 4 , 5 . There are two types of femoroacetabular impingement. The first or cam impingement is caused by an abnormal femoral head with increasing radius into the acetabulum during forceful motion, especially flexion 5 , 6 . The resulting shear forces produce outside‐in abrasion of the acetabular cartilage and/or its avulsion from the labrum and the subchondral bone in a rather constant anterosuperior rim area. Chondral avulsion in turn leads to tear or detachment of the principally uninvolved labrum. The second or pincer impingement is the result of linear contact between the acetabular rim and femoral head‐neck junction. The femoral head might have normal morphological features and the abutment is the result of acetabular abnormality 6 .
In the early stage of femoroacetabular impingement, the anatomical deformity is characterised by an increase in the radius of the femoral head caused by a slight varus deformity of the head‐neck junction in the anteroposterior plane, combined with a posterior displacement, resulting in the characteristic hump deformity of the femoral head‐neck junction 7 , 8 . Normally the femoral head is spherical in shape, which can be determined using a circular template corresponding to the appropriate size of the femoral head. However, in the case of early femoroacetabular impingement, an anterolateral prominence is seen at the femoral head‐neck junction outside of the circle that is extended in a convex shape to the base of the neck. This is called asphericity 9 , 10 (Fig. 1).
Figure 1.
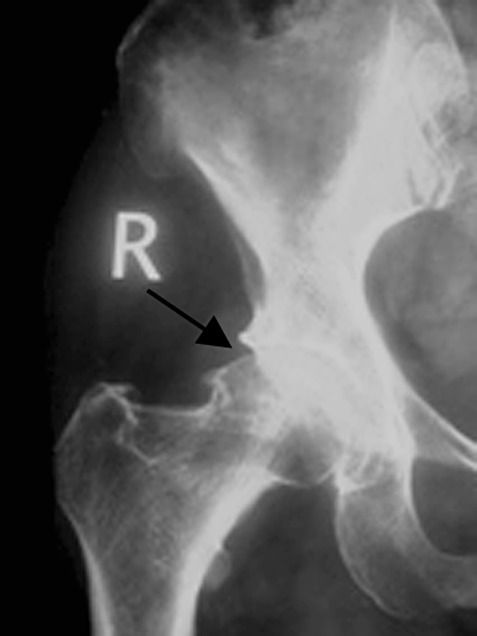
X‐ray film of a 35‐year‐old man, who complained of hip pain, showing cam type femoroacetabular impingement.
In the present study, we aimed to study asphericity of the femoral head in femoroacetabular impingement using new radiological indices such as the alpha angle and triangular index in an Asian population, the sex and age distribution of femoroacetabular impingement in an Asian population, and the correlation between body mass index (BMI) and femoroacetabular impingement.
Materials and methods
The present study was conducted retrospectively from January 2008 to June 2010 on 50 consecutive patients with suspected femoroacetabular impingement of the hip who reported to the orthopaedics outpatients department of the Postgraduate Institute of Medical Education and Research. Ten controls were also used in the study. The following inclusion and exclusion criteria applied:
Inclusion criteria
-
1
Patients with chief complaints of:
-
(a)
groin or buttock pain with walking
-
(b)
restriction of movements.
-
(a)
-
2
Patients with signs of:
-
(a)
crepitus with movement
-
(b)
decreased range of movement
-
(c)
positive impingement test.
-
(a)
-
3
Patients with roentgenographic changes of:
-
(a)
bony enlargement
-
(b)
mild to moderate narrowing of hip joint space.
-
(a)
Exclusion criteria
-
(a)
congenital joint abnormality
-
(b)
history of prior trauma
-
(c)
increased erythrocyte sedimentation rate
-
(d)
positive rheumatoid arthritis factor
-
(e)
diffuse involvement of joint in X‐ray
-
(f)
positive human leukocyte antigen B27.
Patients for the control were selected from emergency orthopaedic services of the Postgraduate Institute of Medical Education and Research, Chandigarh, and various indices were measured for correlation with respect to accuracy and cost‐effectiveness.
The radiographs were obtained with the patient supine, positioned with the patellae pointing straight upwards and feet mounted in holders. The frog leg lateral was taken with the patient supine, the ipsilateral knee flexed and the leg abducted so that the sole of the foot contacted the contralateral leg at the level of the knee; the leg was then externally rotated while ensuring that the pelvis did not rotate away from the plane of the table.
The center of the femoral head was identified using Mose's circles, which consisted of a transparent sheet of plastic with concentric circular markings 1 mm apart. The longitudinal axis of the femoral head was identified by connecting the center of the femoral head to the midpoint of the narrowest place on the femoral neck, which corresponds to bisecting a line drawn from the tip of the greater trochanter to the apex of the lesser trochanter.
The alpha angle was measured by drawing a line perpendicular to the femoral neck at its narrowest point. A second line (b) was drawn perpendicular to this point, bisecting the femoral neck. A best fit circle was drawn, outlining the femoral head. The (alpha) angle was calculated as the angle formed between line b and the point where the femoral head protrudes anterior to the circle (Fig. 2).
Figure 2.
A 42‐year‐old man with a body mass index of 32 and positive impingement test, complained of hip pain that was aggravated by walking. A radiograph showed a hump formation. The alpha angle was estimated to be 90°.
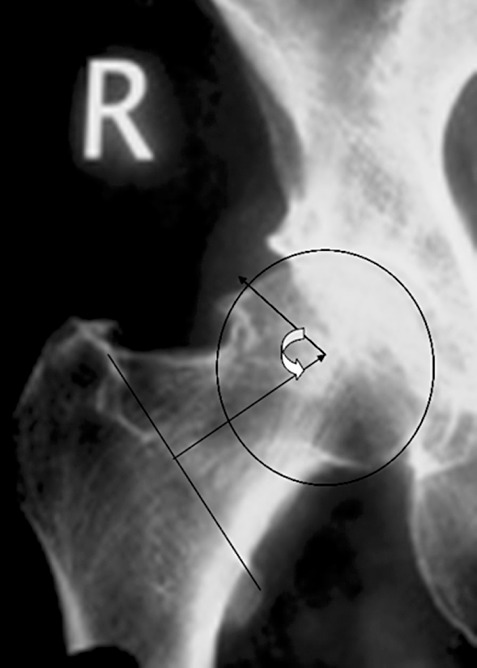
The triangular index (Fig. 3) was calculated as follows: the length of the natural femoral head radius was marked laterally along the longitudinal axis of the femoral neck. At the point half the length of the radius along this axis, the perpendicular height to the superior border of the head‐neck junction was measured. From this height the corresponding radius was calculated using pythogram axiom for right‐angled triangles.
Figure 3.

Triangular index of Gosvig et al. 15 R is the radius of the femoral head at the level of the narrowest part of the femoral neck and R' is the radius of the femoral head at the level of the hump. The triangular index is the difference between the R' and R.
The weight and height of the patients were measured to calculate the BMI. Patients with a BMI greater than 25 was considered obese. Finally, the indices were correlated with various risk factors such as age, sex, inheritance and obesity.
Evaluation of results
The shape of the femoral head was classified as normal if the femoral head was spherical in both the anteroposterior and lateral view. A hip was classified as aspherical if the head protruded out of a circle drawn around the head and extended anteriorly in a convex shape to the base of the neck. Patients were considered to have asphericity if the alpha angle was greater than 65°, or in the triangular index, if the resultant radius exceeded the natural radius of the femoral head by 2 mm on a roentgenography with 1.2 magnification. Because there was usually a difference in magnification at the various institutes or centers, we decided to find the ratios between the resultant radius and the natural radius to minimize the error due to magnification.
Results
Among the 60 patients enrolled in the study, 50 were cases and 10 were controls. For each patient, a roentgenography of the hip joint in both the anteroposterior and frog leg lateral view were taken.
Age distribution
The patients in the study were aged between 21 and 78 years. The mean age in the control group was 48.9 ± 4.6 years and the mean age in the femoroacetabular impingement group was 52.4 ± 13.2 years. The majority of patients were older and the distribution in the two groups was similar.
Sex distribution
There were 27 men and 23 women in the cases and the 10 controls had an equal distribution of male and female patients.
Weight distribution
The height and weight of all patients in the study were recorded. The BMI was measured. According to international standards, patients with a BMI greater than 25 were labelled as obese. There were 33 obese and 17 non‐obese patients in the case group and four obese and six non‐obese patients in the control group.
Family distribution
There was no family history of a similar illness in the cases and controls.
Alpha angle
In the anteroposterior view, the alpha angle range was from 55° to 106° for the cases and from 54° to 70° for the controls. In the lateral view the range was from 62° to 104° for the cases and from 54° to 62° for the controls. The mean alpha angle in the anteroposterior view was measured as 75°± 10° in the cases and 61°± 6° in the controls, and the mean in the lateral view was 74°± 8° in the cases and 58°± 6° for the controls. In the cases, the alpha angle in males in the anteroposterior view ranged from 62° to 104°, whereas in females it ranged from 55° to 106°. The average mean angle in males was 75°± 10°, whereas in females it was 73°± 9°. In the lateral view the average alpha angle in males was the same as in the anteroposterior view with a range from 64° to 104° and the females also had the same mean as that of the anteroposterior view with a range from 62° to 104°. In the anteroposterior radiograph, patients younger than 50 years had an alpha angle in the range from 55° to 106° with a mean of 82°± 22° and patients older than 50 years had a range from 62° to 88° with a mean of 75°± 13°. In the lateral radiograph, patients younger than 50 years showed an alpha angle in the range from 62° to 104° with a mean of 83°± 19° and those older than 50 years showed from 64° to 90° with a mean of 77°± 13°. In the anteroposterior radiograph, patients who were not obese (i.e. BMI lesser than 25) had an alpha angle in the range from 55° to 104° with a mean of 79°± 24° and those who were obese had a range from 62° to 104° with a mean of 84°± 22°. In the lateral roentgenograph, the alpha angle range in non‐obese patients was from 62° to 104° with a mean of 83°± 21°, whereas in obese patients the range was from 70° to 104° with a mean of 87°± 17°.
Triangular index
The triangular index range in the radiographs was from 1 to 7 in the cases and from 0 to 1 for the controls. The mean triangular index in the radiographs was 2.9 ± 1.2 for the cases and 0.2 ± 0.4 for the controls. In patients younger than 50 years the index ranges were from 2 to 6 with a mean of 4 ± 2 in the radiographs, whereas in older patients it ranged from 1 to 7 with a mean of 4 ± 3 in the radiographs. In male patients the index ranged from 1 to 7 with a mean of 4 ± 3 in the radiographs. In female patients it ranged from 1 to 4 with a mean of 2.5 ± 1.5 in the radiographs. In obese patients the index ranged from 1 to 7 with a mean of 4 ± 3 in the radiographs and in non‐obese patients the index ranged from 1 to 6 with an average of 1.5 ± 1.
Triangular ratio
Because there were differences in the size of the femoral head, which might be due to either the difference in the physical status of the patient or the difference in the distance between the sources of the X‐ray beam to the patient, we decided to take the ratios between the two radii. The mean ratio in the anteroposterior radiograph was 1.12 with a standard deviation of ±0.05.
Discussion
Femoroacetabular impingement has been proposed as a major etiological factor in the development of osteoarthritis of the hip 11 , 12 , 13 . Current knowledge suggests that early diagnosis and surgery are efficacious in relieving hip symptoms and enhancing hip function. Efforts continue to further optimize diagnostic strategies. The initial radiographic evaluation is critical in formulating an accurate diagnosis. Different radiographic views and imaging techniques have been used to assess deformities of the anterolateral femoral head‐neck junction 10 .
In the present study, the alpha angle in the anteroposterior view ranged from 55° to 106° for the cases and 54° to 70° for the controls. In the lateral view the range was from 62° to 104° for the cases and from 54° to 62° for the controls. The mean alpha angle in the anteroposterior view was measured as 75°± 10° in the cases and 61°± 6° in the controls, and the mean lateral view was 74°± 8° in the cases and 58°± 6° in the controls. In comparison with previously published results, Clohisy et al. 14 stated that the mean average alpha angle in the anteroposterior view was 71.5° with a range from 38° to 132° in the cases and 51.2° with a range from 36° to 94° in the controls, and in the frog leg lateral view the average was 65.2° with a range from 38° to 114° in the cases and the mean was 43.7° with a range from 31° to 76° in the controls.
In the present study, the mean triangular index measured in the anteroposterior radiographs was 2.9 ± 1.2 in the range from 1 to 7 for the cases and the mean was 0.2 ± 0.4 with a range from 0 to 1 for the controls. Gosvig et al. 15 had correlated the alpha angle and the triangular index in diagnosing the cam type femoroacetabular impingement and stated that the alpha angle was more variable with rotation of the femoral head, whereas the triangular index is not variable within 20° internal rotation and 20° external rotation. However, Gosvig et al. 15 did not give any mean or range for the triangular index. Due to the huge variation in the size of the femoral head, we estimated the ratios of the radius of the femoral head with the hump radius.
The triangular ratio was measured in all anteroposterior radiographs, which was a new parameter to be measured. We found that in the radiographs the mean ratio was 1.12 with a standard deviation of ±0.05 and a range from 1.06 to 1.29 in the cases and 1.02 ± 0.02 with a range from 1.00 to 1.04 in the controls. It is a very useful parameter because it is not altered with the size of the head or the source‐to‐film distance. Therefore, with this parameter we can diagnose a case of femoroacetabular impingement even with a digital radiograph. To our knowledge, this parameter has not been described in the literature so far.
Risk factors such as age, sex, weight and inheritance were correlated with different indices. None of our patients had a family history of osteoarthritis or femoroacetabular impingement. Therefore, there was no correlation between inheritance and femoroacetabular impingement.
Correlation with age
The P‐value ranged from 0.858 to 1.00 for all indices, and because the P‐value was greater than 0.05 there was no correlation between the age of the patient and femoroacetabular impingement. Ito et al. 4 studied the femoral head‐neck offset and stated that younger patients had significantly smaller mean offset when compared with the controls, which might lead to femoroacetabular impingement. Therefore, until now, there has been no study that correlated femoroacetabular impingement with age.
Correlation with gender
The P‐value ranged from 0.693 to 1.00 for all indices, and because the P‐value was greater than 0.05 there was no significant correlation between gender and femoroacetabular impingement. Ito et al. 4 studied the femoral head‐neck offset and stated that there was no significant difference between genders. Therefore, there has been no study that compared gender with femoroacetabular impingement.
Correlation with BMI
The P‐value ranged from 0.003 to 0.045 in all indices, and because the P‐value was less than 0.05 there was a significant correlation between BMI and femoroacetabular impingement. To our knowledge, no study has reported on the correlation of weight with femoroacetabular impingement.
Conclusions
-
1
There was no significant correlation between the age of a patient and femoroacetabular impingement.
-
2
There was no significant correlation between the gender of a patient and femoroacetabular impingement.
-
3
There was significant correlation between the weight of a patient and femoroacetabular impingement.
-
4
None of the cases had a family history of similar problems.
Disclosure
None of the authors received funding or any financial support, and all authors have full control of the primary data and will allow the Journal to review the data if requested. Each author certifies that their institution has approved or waived approval for the human protocol for this investigation and that all investigations were conducted in conformity with ethical principles of research.
References
- 1. Nötzli HP, Wyss TF, Stoecklin CH, et al The contour of the femoral head‐neck junction as a predictor for the risk of anterior impingement. J Bone Joint Surg Br, 2002, 84: 556–560. [DOI] [PubMed] [Google Scholar]
- 2. Beck M, Kalhor M, Leunig M, et al Hip morphology influences the pattern of damage to the acetabular cartilage: femoroacetabular impingement as a cause of early osteoarthritis of the hip. J Bone Joint Surg Br, 2005, 87: 1012–1018. [DOI] [PubMed] [Google Scholar]
- 3. Ganz R, Parvizi J, Beck M, et al Femoroacetabular impingement: a cause for osteoarthritis of the hip. Clin Orthop Relat Res, 2003, 417: 112–120. [DOI] [PubMed] [Google Scholar]
- 4. Ito K, Minka MA 2nd, Leunig M, et al Femoroacetabular impingement and the cam‐effect. A MRI‐based quantitative anatomical study of the femoral head‐neck offset. J Bone Joint Surg Br, 2001, 83: 171–176. [DOI] [PubMed] [Google Scholar]
- 5. Siebenrock KA, Schoeniger R, Ganz R. Anterior femoro‐acetabular impingement due to acetabular retroversion. Treatment with periacetabular osteotomy. J Bone Joint Surg Am, 2003, 85: 278–286. [DOI] [PubMed] [Google Scholar]
- 6. Leunig M, Werlen S, Ungersböck A, et al Evaluation of the acetabular labrum by MR arthrography. J Bone Joint Surg Br, 1997, 79: 230–234. [DOI] [PubMed] [Google Scholar]
- 7. Stulberg SD, Cordell LD, Harris WH, et al Unrecognised childhood hip disease. A major cause of idiopathic osteoarthritis hip In: Hip Society , ed. The Hip: Proceedings of the Third Open Scientific Meeting of the Hip Society. St Louis, MO: CV Mosby Company, 1975; 212–228. [Google Scholar]
- 8. Tönnis D, Heinecke A. Acetabular and femoral anteversion: relationship with osteoarthritis of the hip. J Bone Joint Surg Am, 1999, 81: 1747–1770. [DOI] [PubMed] [Google Scholar]
- 9. Tanzer M, Noiseux N. Osseous abnormalities and early osteoarthritis: the role of hip impingement. Clin Orthop Relat Res, 2004, 429: 170–177. [PubMed] [Google Scholar]
- 10. Jäger M, Wild A, Westhoff B, et al Femoroacetabular impingement caused by a femoral osseous head‐neck bump deformity: clinical, radiological, and experimental results. J Orthop Sci, 2004, 9: 256–263. [DOI] [PubMed] [Google Scholar]
- 11. Meyer DC, Beck M, Ellis T, et al Comparison of six radiographic projections to assess femoral head/neck asphericity. Clin Orthop Relat Res, 2006, 445: 181–185. [DOI] [PubMed] [Google Scholar]
- 12. Klaue K, Durnin CW, Ganz R. The acetabular rim syndrome. A clinical presentation of dysplasia of the hip. J Bone Joint Surg Br, 1991, 73: 423–429. [DOI] [PubMed] [Google Scholar]
- 13. Fitzgerald RH Jr. Acetabular labrum tears. Diagnosis and treatment. Clin Orthop Relat Res, 1995, 311: 60–68. [PubMed] [Google Scholar]
- 14. Clohisy JC, Nunley RM, Otto RJ, et al The frog‐leg lateral radiograph accurately visualized hip cam impingement abnormalities. Clin Orthop Relat Res, 2007, 462: 115–121. [DOI] [PubMed] [Google Scholar]
- 15. Gosvig KK, Jacobsen S, Palm H, et al A new radiological index for assessing asphericity of the femoral head in cam impingement. J Bone Joint Surg Br, 2007, 89: 1309–1316. [DOI] [PubMed] [Google Scholar]