

Isolated fracture of the coracoid process (CP) is uncommon. Furthermore, CP fracture associated with acromioclavicular (AC) dislocation is even rarer. One case is reported here, and relevant published articles are reviewed.
Case report
A 37‐year‐old man fell from a height of 2 m, injuring his right shoulder. He sustained immediate pain and swelling over the right AC region. Physical examination revealed a prominent right distal clavicle and tenderness at the AC joint. Pain was elicited with abduction beyond 35°, flexion beyond 15°, and extension beyond 15°. Neurological examination of the upper limb was normal. Anteroposterior roentgenograms with and without weight showed AC joint separation and CP fracture through the base, which was confirmed by a three‐dimensional computed tomography reconstruction (Fig. 1).
Figure 1.

A three‐dimensional computed tomography reconstruction from different aspects showing a fracture of the CP (arrows).
Open reduction and internal fixation of the AC joint were performed with AO clavicular hook plate. The coracoclavicular (CC) ligament was found to be intact, and successful fixation of the CP was performed with a 4.5‐mm‐diameter cannulate screw.
Radiological assessment on the second postoperative day showed satisfactory reduction of the right AC joint and the CP (Fig. 2). The patient had an uneventful postoperative course and was discharged on the fifth postoperative day with an arm sling. Follow‐up examination on the fourth week revealed restoration of a full range of movement of the right shoulder with only mild pain.
Figure 2.
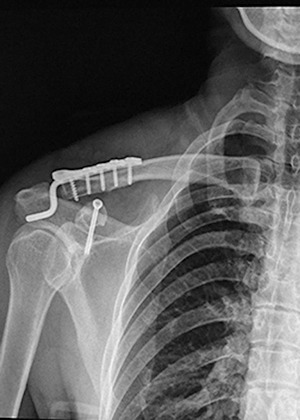
Radiological assessment post‐operatively showing satisfactory reduction of the right AC joint and CP.
Discussion
The mechanism of the injury
It is hard to know how common such injuries are since there are no reliable clinical reports. A fractured CP associated with AC dislocation has rarely been reported. The mechanism of CP fracture remained controversial. It was previously thought that the intact CC ligaments avulsed the CP cephalad. Protass et al. indicated that, in adolescents, the CC ligaments are stronger than the unfused epiphyseal plate and an injury that could result in disruption of the ligaments may only injure the epiphyseal plate if the CC ligaments remain intact 1 . Montgomery and Loyd stated that, in adults, the CP and clavicle are stronger than the CC ligaments, therefore almost all Rockwood type III AC joint injuries involve a tear of the CC ligaments rather than a fracture of the CP 2 .
However, we should notice that in four published cases there were three associated lesions: disruption of the CC ligaments, fracture of the CP, and AC dislocation 3 , 4 , 5 , 6 . It is unlikely that a force from ruptured ligaments could cause CP fracture. Direct trauma to the CP is also unlikely,because the CP is well protected by the clavicle above. So we doubt that avulsion by the CC ligaments fully explains the occurrence of CP fracture.
To our knowledge, the epiphyseal plate of the CP is near its base, and is normally completely replaced by bone between 15 and 18 years of age. We found that, in published cases of fractured CP associated with AC dislocation, the age range was from 9 to 60 years, with a median of 23.5. At the median age, the CC ligaments are weaker than the fused CP, so the CC ligaments would be ruptured rather than the CP fractured. It can only be assumed that the combined force of conjoined tendons and the pectoralis minor muscles is involved in the traumatic mechanism. As Fig. 3 shows, the first step is a sudden contraction of the conjoined tendons and pectoralis minor muscles (for protection or other reasons) resulting in fracture of the CP. In the second step, whether the CC ligament remains intact or not depends on the strength of the component residual force along the CC ligaments.
Figure 3.
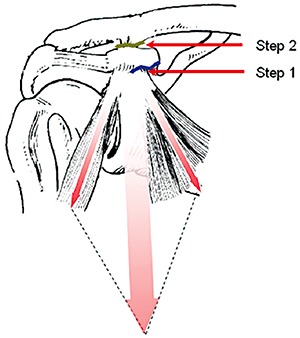
Schematic diagram for interpreting possible mechanism of CP fracture.
Diagnosis and differential diagnosis
Although CP fracture is difficult to visualize on routine roentgenogram due to marked foreshortening and projection over the acromion or blade of the scapula, special views or tomography can make the deformity apparent. The correct diagnosis can be made by careful comparison with the normal side. Unfortunately, CP fracture is easily overlooked when attention is directed toward the more obvious AC dislocation, or the fracture is confused with an unfused epiphysis. Protass et al. reported that normal unfused coracoid epiphyses tend to be evenly spaced from the scapula, thus the two coracoid processes often appear to be symmetrical 1 . This feature may help to differentiate coracoid fracture from a normally positioned unfused epiphysis, but neither of these two observations is absolute.
Treatment
Surgical treatment
Nearly half of all reported patients have been treated surgically. Surgical treatment permits direct inspection of the injury to the joint and removal of any fracture fragments or other obstructions to reduction. It also permits anatomical reduction and secure fixation, making the resumption of shoulder motion permissible earlier than with closed techniques, which is especially important for patients performing heavy work 7 . All reported patients treated surgically recovered fully, except for one reported by Wilber and Evans who was treated by an unknown surgical method and complained of persistent pain and a decreased range of movement one year postoperatively 8 . Where disrupted CC ligaments are diagnosed, they should either be repaired by suturing to the fixed CP, or man‐made materials substituted for them. Where the CC ligaments are intact, Taga et al. have suggested that fixation of the AC joint alone might be sufficient 9 . Nevertheless, fixation of both the CP and the AC joint is sometimes needed when a single procedure would be ineffective 3 . Considering that the AC joint is an amphiarthrodial joint, a clavicular hook plate for fixation of the AC joint is recommended.
Conservative treatment
More than half of all patients reported were treated conservatively with a sling, shoulder immobilizer, or plastic abduction cast. In some cases that were managed by conservative treatment, cosmetic complaints 2 , pain 10 and residual AC dislocation 10 were observed, but these complications did not jeopardize the movement of the arm. Conservative treatment fails chiefly because of interposition of the articular disc, frayed capsular ligaments and fragments of articular cartilage between the acromion and the clavicle.
In previously published cases both surgical and conservative treatment for this combined injury seemed to achieve similar long‐term follow‐up results. Surgical treatment is recommended particularly under the following circumstances: (i) failed conservative treatment; (ii) younger patients or heavy laborer; and (iii) patients who particularly desire a good cosmetic result.
Acknowledgment
This work was supported by a grant from the Clinical Scientific Research Fund of Shanghai (054119613).
References
- 1. Protass JJ, Stampfli FV, Osmer JC. Coracoid process fracture diagnosis in acromioclavicular separation. Radiology, 1975, 116: 61–64. [DOI] [PubMed] [Google Scholar]
- 2. Montgomery SP, Loyd RD. Avulsion fracture of the coracoid epiphysis with acromioclavicular separation. Report of two cases in adolescents and review of the literature. J Bone Joint Surg Am, 1977, 59: 963–965. [PubMed] [Google Scholar]
- 3. Wang KC, Hsu KY, Shih CH. Coracoid process fracture combined with acromioclavicular dislocation and coracoclavicular ligament rupture. A case report and review of the literature. Clin Orthop Relat Res, 1994, 300: 120–122. [PubMed] [Google Scholar]
- 4. Wilson KM, Colwill JC. Combined acromioclavicular dislocation with coracoclavicular ligament disruption and coracoid process fracture. Am J Sports Med, 1989, 17: 697–698. [DOI] [PubMed] [Google Scholar]
- 5. Yu KS, Chan PT, Ngai WK, et al Coracoid process fracture combined with acromioclavicular joint dislocation and coracoclavicular ligament disruption. Sicot Case‐Reports: April 2002.
- 6. Zettas JP, Muchnic PD. Fractures of the coracoid process base in acute acromioclavicular separation. Orthop Rev, 1976, 5: 77–79. [Google Scholar]
- 7. Jeffrey AD, John RC. Acute dislocations In: Canale ST, Beaty JH, eds. Campbell's Operative Orthopaedics, 11th edn. Xi'an: World Publishing Company, 2007; 3587–3592. [Google Scholar]
- 8. Wilber MC, Evans EB. Fractures of the scapula. An analysis of forty cases and a review of the literature. J Bone Joint Surg Am, 1977, 59: 358–362. [PubMed] [Google Scholar]
- 9. Taga I, Yoneda M, Ono K. Epiphyseal separation of the coracoid process associated with acromioclavicular sprain. A case report and review of the literature. Clin Orthop Relat Res, 1986, 207: 138–141. [PubMed] [Google Scholar]
- 10. Bernard TN Jr, Brunet ME, Haddad RJ Jr. Fractured coracoid process in acromioclavicular dislocations. Report of four cases and review of the literature. Clin Orthop Relat Res, 1983, 175: 227–232. [PubMed] [Google Scholar]