

Introduction
Double‐level spinal injury, which rarely occurs simultaneously in adults, induces complex complications. There is only one published report of this phenomenon: that of a three‐year‐old boy who was admitted to the emergency department with paraplegia after being hit by a car. Computed tomography (CT) and plain radiographs failed to reveal any bone fracture or dislocation. However, magnetic resonance imaging (MRI) showed loss of continuity with near‐complete and complete anatomic transection of the spinal cord at the T3–4 and T6–7 levels. The boy received conservative treatment and had a poor prognosis1.
The double‐level injuries of cervical distraction fracture and dislocation and thoracic cord transection in an adult have never been previously reported. Here we present a case of double‐level spinal injury caused by a traffic accident.
Case Report
A 52‐year‐old man received multiple injuries in a traffic accident. Clinical examination showed tenderness over C7 and T10 vertebrae with complete loss of sensation and motor power below T10. He had hand numbness and muscle weakness bilaterally. The Babinski reflex was negative with loss of knee and ankle reflexes. Anal and bulbocavernosus reflexes were absent. The Japan Orthopaedic Association (JOA) score was 4 and the Frankel classification A. In addition, the patient had sustained fractures of the left tibia and fibula. He had a right temporo‐parietal epidural hematoma and hemopneumothorax caused by multiple rib fractures and lung contusion. An MRI of the whole spine showed a cervical distraction fracture and dislocation at C6–7 and thoracic cord transection with disruption of the spinal cord at T10 level, with an anterior fracture of T11 (Fig. 1). There was no evidence of any associated posterior ligamentous complex damage on the MRI scan. He underwent emergency tracheal cannulation because of dyspnea and high paraplegia. After being admitted to hospital, he underwent evacuation and decompression of the right temporal‐parietal epidural hematoma and bilateral chest drainage and calcaneal traction. Five days after the accident, he underwent tracheotomy and was placed on assisted ventilation. Two weeks after the accident, he underwent anterior cervical discectomy and fusion and left tibial open reduction and internal fixation. After successful management of his tracheotomy and nutritional support, the patient was transferred to a local hospital for neurologic rehabilitation.
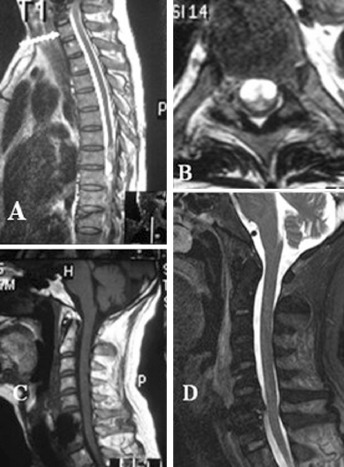
Figure 1.

(A) Preoperative sagittal T2 MRI of the thoracic spine showing transection disruption of the thoracic spinal cord at the T10 level without posterior ligamentous complex damage. (B) Preoperative transversal T2 MRI of the thoracic spine at the T10 level. (C) Preoperative sagittal T1 MRI of the cervical spine showing cervical distraction fracture and dislocation at C6 ,7. (D) Preoperative sagittal T2 MRI of the cervical spine showing the cervical spinal cord is remarkably compressed.
On the follow‐up six months later, neurologic examination showed persistent complete loss of sensation and motor power below T10. His hand numbness and muscle weakness had improved bilaterally. The Babinski reflex was still negative with loss of knee and ankle reflexes. The anal and bulbocavernosus reflexes were still absent. The JOA score was 8 and Frankel classification A. He needed intermittent catheterization and had no problems with breathing or nutrition. He was living at home and attending the hospital for functional rehabilitation weekly.
Discussion
The mechanism of double level spinal injury is not clear. Two different mechanisms were possible in this patient. One possible mechanism is that the cervical cord compression may have been caused by cervical distraction fracture and dislocation, which is very common in whiplash injury. The thoracic cord transection was probably then caused by a longitudinal traction force transmitted through the cervical cord to the thoracic cord as a result of the associated high energy injuries of cervical distraction fracture and dislocation. A second possible mechanism is that the cervical cord injury following the cervical distraction fracture and dislocation was a cervical hyperextension injury and the thoracic cord transection injury occurred independently and belonged to the category of spinal cord injury without radiologic abnormality (SCIWORA).
For a variety of reasons, including ligamentous elasticity, horizontal orientation of facet joints, anterior wedging of vertebral bodies and a relatively heavier head, SCIWORA is most frequently seen in the pediatric age group2. Because of changes in the ligamentous and bony morphology of the spine with increasing age, SCIWORA is rarely seen in skeletally mature patients. Furthermore, the thoracic spine has a mechanically stable structure supported by costotransverse articulations and the rib cage, increasing the axial loading capacity by three to four times3. As a result of the combination of the increased stability and stiffness of the thoracic spine and the progressively increasing rigidity of the aging spine, thoracic spinal cord injury without fractures or discoligamentous injuries rarely occurs in adult patients. Samsani et al. presented a case of a skeletally mature 17‐year‐old patient with disruption of the spinal cord without vertebral fractures or ligamentous injury evident on plain radiographs, CT or MRI4. The combination of multiple rib fractures with partial anterior T11 vertebral column fracture suggests an injury pattern involving violent hyperextension (Fig. 2).
Figure 2.
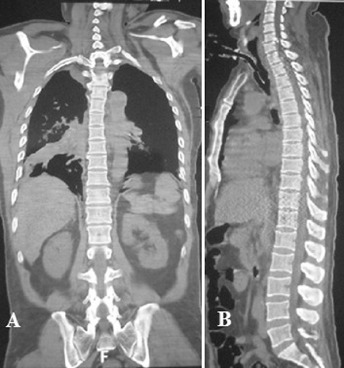
(A) Preoperative coronal CT of whole spine. (B) Preoperative sagittal CT of whole spine showing cervical distraction fracture and dislocation at C6 ,7, minor anterior fracture of thoracic vertebrae at the T11 level and no fracture or dislocation at T8 and T9.
Treatment of severely injured patients with complex double‐level spinal injury should be structured. Firstly, because cervical injuries can affect respiration and hemothoraxes can induce shock, maintenance of vital signs is of great importance. Secondly, respiratory support and prevention of pulmonary infection should be considered. Thirdly, decompression and reconstruction surgery should be performed as soon as possible after achieving respiratory stability. Fourthly, complex nursing care and general nutritional support is very important. Several weeks after removal of tracheostomies, neurologic rehabilitation should be gradually introduced. Because of our patient's poor general condition and requirement for mechanical ventilation after the first anterior cervical surgery, exploratory surgery of the thoracic cord transection was not performed and an MRI scan of the whole spine was taken (Fig. 3).
Figure 3.
(A) Preoperative sagittal T1 MRI of the thoracic spine showing transection disruption of the thoracic spinal cord at the T10 level with an anterior fracture of T11. (B) Postoperative transverse T2 MRI of the thoracic spine at the T10 level with high signals of the local effusion. (C) Postoperative sagittal T1 MRI of the cervical spine showing remarkable decompression of the cervical spinal cord. (D) Sagittal T2 MRI of the cervical spine after anterior cervical discectomy and fusion.
This report describes a rare case of the double‐level injuries of cervical distraction fracture and dislocation and thoracic cord transection in an adult. These injuries probably resulted from thoracic violent hyperextension combined with a longitudinal traction force transmitted through the cervical cord to the thoracic cord as a result of the associated high energy injuries of cervical distraction fracture and dislocation. To the best of the authors' knowledge, such a case has not been reported previously.
Disclosure: The authors state that they have no actual or potential conflicts of interest.
References
- 1. Atılgan M. Double‐level spinal cord injury without vertebral fracture or dislocation: a case report. Ulus Travma Acil Cerrahi Derg, 2012, 18: 80–82. [DOI] [PubMed] [Google Scholar]
- 2. Kothari P, Freeman B, Grevitt M, Kerslake R. Injury to the spinal cord without radiological abnormality (SCIWORA) in adults. J Bone Joint Surg Br, 2000, 82: 1034–1037. [DOI] [PubMed] [Google Scholar]
- 3. Brandser EA, el‐Khoury GY. Thoracic and lumbar spine trauma. Radiol Clin North Am, 1997, 35: 533–557. [PubMed] [Google Scholar]
- 4. Samsani SR, Calthorpe D, Geutjens G. Thoracic spinal cord injury without radiographic abnormality in a skeletally mature patient: a case report. Spine (Phila Pa 1976), 2003, 28: E78–E80. [DOI] [PubMed] [Google Scholar]