

Abstract
Objective
To explore the efficacy of overlapping suture‐anchor fixation for treatment of chronic deltoid ligament injury.
Methods
Seventeen patients (11 men, 6 women of mean age 32.1 years [range, 18–58 years]) who had undergone surgery for chronic deltoid ligament injury from January 2007 to December 2011 were retrospectively analyzed. Preoperatively, they had undergone bilateral weight‐bearing posterior‐anterior radiographs, (MRI) and ultrasound examinations of the ankle. Ankle arthroscopy was performed to confirm the diagnosis, followed by surgery to clear intra‐articular proliferating synovial tissues and remove cartilage debris and scar tissue. The deep layer of the deltoid ligament was sutured onto the tip of the medial malleolus and its superficial layer sutured onto its periosteum and fixed with suture anchors. American Orthopedic Foot and Ankle Society (AOFAS) scoring system for the ankle‐hindfoot was used to evaluate the ankles pre‐ and post‐operatively.
Results
The 17 patients were followed up for 12–34 months (mean 20.1 months). The angle between the long axes of the talus and first metatarsal and the hindfoot angle measured in a hindfoot alignment view (as described by Saltzman) were reduced from 5.4° ± 1.8° and 8.2° ± 2.6° preoperatively to 4.0° ± 0.9° and 5.3° ± 1.3° postoperatively, respectively. The mean AOFAS ankle‐hindfoot score was 76.8 ± 7.0 preoperatively and 94.1 ± 3.3 at the last follow‐up visit. Ten patients were scored as excellent, six as good, and one as fair. Pain was relieved in all patients and no patients had recurrent deltoid ligament injury.
Conclusion
Using suture anchors to treat chronic deltoid ligament injury has relatively satisfactory outcomes.
Keywords: Ankle, Deltoid ligament, Suture anchor
Introduction
The deltoid ligament on the medial side of the ankle connects to two joints: the ankle and the subtalar or talocalcaneonavicular joints. This ligament is closely related to the posterior tibial tendon, spring ligament and sustentaculum tali, which together form a functional complex that plays an important role in maintaining the stability of the ankle and subtalar joints1. Biomechanical experiments have proved that excision of the tibial ligament alone may cause the talus to shift laterally by 3.13 to 4.19 mm, leading to a 3° obliquity2. Therefore, patients with deltoid ligament injury often present a series of manifestations caused by instability of the medial side of the hindfoot.
Over the past decade, structural impairment of the medial malleolus has gradually attracted the attention of clinicians. Krips et al. found that simple deltoid ligament injury accounts for 2.5% of ankle injuries3. If repairing or reconstruction surgeries cannot be performed in a timely manner after acute deltoid ligament injury, instability of the medial malleolus can occur. In 2004, Hintermann et al. proposed diagnostic criteria for medial malleolus instability, including the patient's sense that the ankle is “giving way”, pain on the antero‐medial site of the ankle, and hindfoot valgus deformity, which can be corrected by an intentional heel raise4. The main symptom is the patient's sense that the ankle is “giving way” when walking on uneven ground, downhill, or downstairs, which relates to weakness of the legs (particularly at the site of the medial malleolus). Pain may occur only in the medial malleolus or simultaneously in both the medial and lateral malleoli. If these symptoms are accompanied by stasis, edema, and other symptoms, medial malleolus ligament injury is highly likely. In addition, in patients with asymmetrical valgus deformity when standing (whereas the tibial muscle functions well and the hindfoot valgus deformity can be corrected by a heel raise), then ligament injury of the medial ankle is suggested.
At present, the means of treatment of deltoid ligament injury of the medial malleolus remains controversial. McConkey et al. suggested that partial deltoid ligament injuries can be treated by immobilization of the injured ligament with a below‐the‐knee non‐weight‐bearing cast for four months, followed by a walking brace for four to six months5. Hintermann et al.4 and Beals et al.6 recommended surgical treatment. They also suggested that surgical repair using anchors is indicated in patients with symptomatic medial malleolar sprain in whom a diagnosis of deltoid ligament injury has been confirmed by ankle arthroscopy. For patients who also have significant calcaneal valgus deformity, an additional calcaneal osteotomy can be considered6, 7.
The present study retrospectively analyzed the medical records of 17 patients with chronic ankle deltoid injury who had undergone treatment with Twinfix suture anchors (Smith & Nephew, Memphis, TN, USA). Our aims were: (i) to investigate the effectiveness of Twinfix suture anchors for patients with chronic ankle deltoid ligament injury; and (ii) to document the characteristics of midfoot and hindfoot deformities caused by chronic deltoid ligament injury.
Materials and Methods
General Information
This study included 17 patients who had undergone treatment for chronic deltoid injury from January 2007 to December 2011. They comprosed 11 males and 6 female patients, with a mean age of 32.1 years (range, 18–58 years). All patients had a history of an ankle sprain of mean duration 14.2 months (range, 7–25 months).
All 17 patients had histories of trauma or sprain. The symptoms had been alleviated by immobilization in plaster or a brace, followed by non‐weight‐bearing walking for two to four weeks. However, ankle pain and swelling, as well as other symptoms, recurred with no obvious triggers after varying periods and conservative treatment failed to achieve satisfactory results. Physical examination showed a fallen medial longitudinal arch, calcaneal valgus deformity, and significant tenderness at the tip of the medial malleolus in the injured foot while weight‐bearing. No significant tenderness was detected along the posterior tibial tendon and the heel‐raising test was negative. A preoperative X‐ray scan and CT indicated the presence of old avulsed bone fragments from the medial malleolus in two patients. MRI and a B ultrasound revealed deep injury of the deltoid ligament in all 17 patients.
Evaluation of Flatfeet
Angle between the Long Axes of the Talus and First Metatarsal (α, Fig. 1 )
Figure 1.

Weight‐bearing lateral radiograph showing the angle between the long axes of the talus and first metatarsal (α).
The angle between the long axes of the talus and first metatarsal was measured on a weight‐bearing lateral radiograph. Flatfoot deformity was diagnosed if this angle was greater than 4°8.
Angle of Hindfoot Alignment (β, Fig. 2 )
Figure 2.
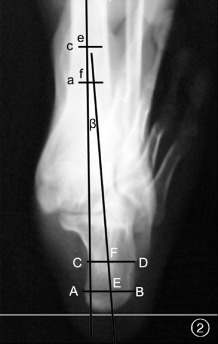
Angle of hindfoot alignment (β): In the Saltzman view, Point a is defined as 10 cm, and point b as 15 cm above the articular surface of the distal tibia's medial side. Point e and f are defined as the midpoints of the tibial width at the levels of Points a and c, respectively. The mid‐diaphyseal axis of the tibia is determined by connecting Points e and f (ef). At 7 mm and 27 mm from the lowest point of the calcaneal tuberosity, two horizontal lines, AB and CD, are drawn parallel to the weight‐bearing surface; these intersect at the calcaneus. Points E and F are determined based on AE:EB = 6:4 and CF:FD = 1:1. The line connecting E and F is used to determine the calcaneal axis. The angular deviation between the tibial axis ef and the calcaneal axis EF i defined as the angle of hindfoot alignment (β).
In accordance with the method proposed by Reilingh et al.9, in a hindfoot alignment view of the calcaneus, as described by Saltzman9 (hereinafter referred to as “the Saltzman view”), Point a is defined as 10 cm and Point c as 15 cm above the articular surface of the distal tibia's medial side. Points e and f are defined as the midpoints of the tibial width at the levels of Points a and c, respectively. The mid‐diaphyseal tibial axis is determined by connecting Points e and f (ef). At 7 mm and 27 mm from the lowest point of the calcaneal tuberosity, two horizontal lines, AB and CD, are drawn parallel to the weight‐bearing surface; these intersect at the calcaneus. Points E and F are determined based on the following formulae: AE : EB = 6:4 and CF : FD = 1:1. The line connecting E and F is used to determine the calcaneal axis. The angular deviation between the tibial axis ef and the calcaneal axis EF is defined as the angle of hindfoot alignment. Hindfoot valgus deformity is diagnosed if this angle is greater than 5°10.
Surgical Treatment
Following induction of general anesthesia, the patient was placed in a supine position. First, ankle arthroscopy was performed on the injured ankle to confirm the diagnosis of deep deltoid ligament injury. In addition, coexisting intra‐articular lesions, such as proliferating synovial membrane and damaged articular cartilage, were treated endoscopically.
With the knee of the injured leg flexed and rotated externally, a curved incision was made below the tip of the medial malleolus. After the branches of the saphenous vein and nerve had been isolated, the superficial fascia layer was exposed and cut open to expose the tibial tendon (Fig. 3a). Generally, it was exposed to the posterior colliculus of the medial malleolus at the proximal end and to the calcaneus sustentaculum at the distal end. The posterior tibial tendon was retracted distally, exposing the deep layer of the posterior tibial tendon sheath and superficial layer of the deltoid ligament. Under normal circumstances, it is often difficult to distinguish between these two layers because of their relatively close structural relationship. However, among patients in this group, this structure was intact but loose. Approximately 5 mm from the anterior colliculus of the medial malleolus, a transverse incision was made in the deep layer of the posterior tibial tendon sheath and the superficial layer of the deltoid ligament (Fig. 3b). The proximal severed end and the periosteum of the anterior colliculus of the medial malleolus were sharply dissociated and retracted laterally; causing wide‐open exposure of the bone structures of the anterior colliculus of the medial malleolus and the medial ankle joint space, and the distal ends of the ligaments prepared for subsequent usage. The medial ankle joint space was explored, after which scar tissue that had formed after deep deltoid ligament rupture was completely removed. In two patients, free bone fragments caused by old avulsed fractures of the tip of the medial malleolus were observed; these were completely excised.
Figure 3.
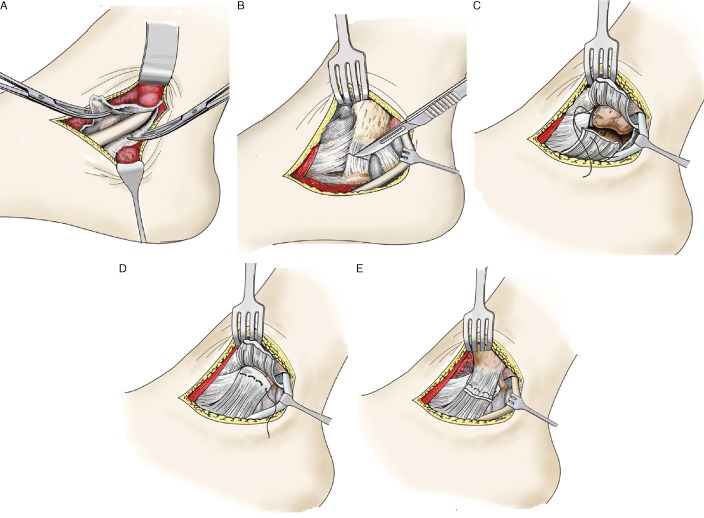
Diagram of the surgical procedure: (A) The posterior tibial tendon is exposed. (B) Approximately 5 mm from the anterior colliculus of the medial malleolus, a transverse incision is made in the deep layer of the posterior tibial tendon sheath and superficial layer of the deltoid ligament. (C) A Smith‐Nephew 3.5 mm suture anchor is placed in an anterior‐to‐posterior direction. (D) The distal end of the superficial layer of the deltoid ligament is sutured and fixed onto the bone structure of the anterior colliculus of the medial malleolus. (E) The periosteum and proximal end of the superficial deltoid ligament layers are overlapped and sutured onto the distal severed end and reinforced with suture anchors.
After the position of the anterior colliculus of the medial malleolus had been identified, a Smith‐Nephew 3.5 mm suture anchor was placed in an anterior‐to‐posterior direction at a site approximately 5 mm from the tip of the anterior colliculus (Fig. 3c). After the hindfoot had been rotated internally, the preserved distal ends of the superficial deltoid ligament layers were sutured and fixed on the anterior colliculus bone (Fig. 3d). In addition, the periosteum and proximal end of the superficial deltoid ligament layers were overlapped and sutured onto the distal severed end, followed by reinforcement with suture anchors (Fig. 3e), after which the incision was closed. The injured leg was immobilized in a neutral ankle position by a short leg plaster splint (Video S1).
Postoperative Treatment
After three weeks of immobilization with a plaster splint, the patients began partial weight‐bearing exercises on the injured leg and underwent dorsiflexion–plantar flexion ankle training. Full weight‐bearing training of the injured leg was initiated after four weeks.
Evaluation
At the last follow‐up, the patients underwent radiography of the injured foot in the Saltzman view and in a weight‐bearing lateral stance to assess the postoperative orthotics of the flatfoot deformity. The American Orthopedic Foot and Ankle Society (AOFAS) scoring system for the ankle‐hindfoot was used to evaluate preoperative and postoperative ankle performance from the perspectives of pain, function and alignment (possible total of 100 points: excellent, 90–100; good, 80–89; fair, 70–79; and poor, <70).
Results
All 17 patients were followed up for a mean of 20.1 months (12–34 months). Preoperative weight‐bearing radiographs had shown that the mean angle between the long axes of the talus and first metatarsal bone was 5.4° ± 1.8° for the injured side and 3.8° ± 0.9° for the healthy side. They had also shown that the angle of hindfoot alignment in the Saltzman view was 8.2° ± 2.6° for the injured side and 5.0° ± 1.5° for the healthy side. Postoperatively, the mean angle between the long axes of the talus and first metatarsal bone was 4.0° ± 0.9° for the injured side in the weight‐bearing stance, and the angle of hindfoot alignment in the Saltzman view was 5.3° ± 1.3° for the injured side.
Pain was relieved postoperatively to some extent in all patients. One patient still had mild swelling around the medial malleolus at the week 12 follow‐up visit; this was eliminated by four microwave‐based local treatments. None of the patients presented with postoperative bruising, superficial or deep infection, delayed wound healing, or other complications. At the last follow‐up visit, no patients had experienced recurrent deltoid ligament injury. One patient complained about one instance of “feeling of giving way” when he walked down stairs. However, there was no feeling of persistent pain in the medial region of the ankle and no limitation in walking. Ankle‐hindfoot performance was evaluated using AOFAS scores, with ten patients considered excellent (Fig. 4), six good, and one fair. The combined percentage of excellent and good was 94.1% (16/17).
Figure 4.

Male patient, 31 years old, who had a right ankle sprain 24 months prior to presentation; his pain had increased in the previous 4 months. (A) Preoperative lateral and AP radiographs showing no bone‐associated injury. (B) Posterior view of preoperative bilateral weight‐bearing showing calcaneal valgus deformity. (C) Preoperative heel‐raising test (negative). (D) Postoperative lateral and AP radiographs showing an anchor located at the anterior colliculus of the medial malleolus. (E) Posterior view of postoperative bilateral weight‐bearing showing correction of the calcaneal valgus deformity in the injured foot. (F) Postoperative heel‐raising test (negative).
Discussion
Characteristics of Foot Deformity after Chronic Deltoid Ligament Injury
Preoperative imaging and clinical examination of the foot revealed a fallen medial longitudinal arch and calcaneal valgus deformity in all 17 patients. To assess the fallen arch deformity on the injured side, we selected the two most commonly used parameters for evaluating the medial longitudinal arch and hindfoot valgus: the angle between the long axes of the talus and first metatarsal in the weight‐bearing stance and the angle of hindfoot alignment in the Saltzman view in the weight‐bearing stance. Improved outcomes after surgery were evidenced by the findings that the angle between the long axes of the talus and first metatarsal and the angle of hindfoot alignment in the Saltzman view decreased from 5.4° ± 1.8° and 8.2° ± 2.6°, respectively, preoperatively to 4.0° ± 0.9° and 5.3° ± 1.3°, respectively, postoperatively in the weight‐bearing stance. Therefore, we cannot exclude the possibility that the fallen longitudinal arch and hindfoot valgus are associated with the deltoid ligament.
Kelikian11 and Milner and Soames12 reported that the superficial layer of the deltoid ligament on the medial side of the ankle is closely related to the spring ligament; these are intertwined to support the talar head; stabilize the talocalcaneonavicular joint; and restrict abduction, tilt and pronation of the talus. In addition, the deep layer of the deltoid ligament on the medial side of the ankle restricts external rotation of the talus. Harper stated that the deltoid ligament plays an important role in restricting talus pronation13. Deltoid ligament injury may cause plantar flexion and hyper‐pronation of the talus, thus leading to a fallen medial longitudinal arch, hindfoot valgus and medial ankle instability14, 15. Hintemann et al. reported that 54 patients with deltoid ligament injury of the medial ankle presented with asymptomatic fallen medial longitudinal arches, forefoot pronation and hindfoot valgus deformities7. However, these deformities disappeared after using heel‐raises, indicating normal functioning of the posterior tibial tendon.
Reconstruction of Chronically Injured Deltoid Ligaments
In contrast with acute deltoid ligament injury accompanied by ankle fracture, Stufkens et al.1 and Hintermann16 recommended ankle arthroscopy for patients with chronically injured deltoid ligaments to confirm the diagnosis, followed by surgical exploration. Reconstruction surgery should be performed in patients with definitive deltoid ligament injury. Numerous reconstruction techniques for the deltoid ligament have been proposed within the last decade. In 2003, Bohay and Anderson reported that they used the autologous flexor hallucis longus tendon to perform deltoid ligament reconstruction in patients with severe flatfeet17. With this method, the flexor hallucis longus tendon is transferred into the medial ankle from posterior to anterior and fixed to the medial side of the talus, thus establishing a new mechanism similar to that of the anterior tibiotalar ligament. In 2010, Ellis et al. reconstructed the deltoid ligament in adult patients with severe acquired flatfeet using an autologous peroneus longus and stated that this surgical method is effective for treating flatfeet and reducing talar tilt18. Hintermann et al. fixed the autologous plantaris tendon between the medial malleolus and navicular bone to reconstruct a structure similar to that of the tibionavicular ligament19.
All 17 patients in this study underwent preoperative arthroscopy to further confirm the diagnosis of deltoid ligament injury and identify the degree of injury. Moreover, coexisting intra‐articular lesions, such as synovial hyperplasia and damaged cartilage, were treated arthroscopically. The subsequent surgical procedures involved removing the chronic ligament scar tissue, suturing the deep layer of the deltoid ligament onto the tip of the medial malleolus, overlapping and suturing of the deltoid ligament's superficial layer into the medial malleolus periosteum, and fixation with anchors. This operation is relatively simple and low‐risk, thus reducing costs caused by autologous or allogeneic tendon transplantation and eliminating the risks of related complications. Therefore, this method not only yields satisfactory postoperative outcomes but is also well accepted by patients. The percentage of excellent/good postoperative AOFAS scores was 94.1% (16/17).
Limitations of this Study
This study has the following limitations: (i) there were relatively few patients, preventing analysis of a large sample; (ii) postoperative radiographic data was not assessed; therefore, the relationship between the patients’ subjective experience of symptom relief and objective radiologic evidence of improvement remained undetermined; (iii) it was a retrospective study; and radiographic images that would have allowed comparison between the injured and contralateral mid‐ and hind‐feet were unavailable.
In summary, chronic deltoid ligament injury is relatively rare and affected patients usually present with specific midfoot and hindfoot deformity. We recommend that the treatment of deltoid ligament injury should focus on reconstruction of medial malleolus stability and restoration of normal functioning of the soft tissue structures on the medial side of the midfoot and hindfoot and of the supportive structure of the medial longitudinal arch. A surgical technique involving ankle arthroscopic examination and clearing the medial ankle joint space combined with suture anchoring is relatively promising for treating chronic deltoid ligament injury.
Video Image
Additional video images may be found in the online version of this article.
Visit http://onlinelibrary.wiley.com/doi/10.1111/os.12125/suppinfo
Supporting information
Video Image
Disclosure: No funds were received in support of this work.
References
- 1. Stufkens SA, van den Bekerom MP, Knupp M, Hintermann B, van Dijk CN. The diagnosis and treatment of deltoid ligament lesions in supination‐external rotation ankle fractures: a review. Strategies Trauma Lim Reconstr, 2012, 7: 73–85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Haddad SL, Dedhia S, Ren Y, Rotstein J, Zhang LQ. Deltoid ligament reconstruction: a novel technique with biomechanical analysis. Foot Ankle Int, 2010, 31: 639–651. [DOI] [PubMed] [Google Scholar]
- 3. Krips R, de Vries J, van Dijk CN. Ankle instability. Foot Ankle Clin, 2006, 11: 311–329. [DOI] [PubMed] [Google Scholar]
- 4. Hintermann B, Valderrabano V, Boss A, Trouillier HH, Dick W. Medial ankle instability: an exploratory, prospective study of fifty‐two cases. Am J Sports Med, 2004, 32: 183–190. [DOI] [PubMed] [Google Scholar]
- 5. McConkey JP, Lloyd‐Smith R, Li D. Complete rupture of the deltoid ligament of the ankle. Clin J Sport Med, 1991, 1: 133–137. [Google Scholar]
- 6. Beals TC, Crim J, Nickisch F. Deltoid ligament injuries in athletes: techniques of repair and reconstruction. Oper Tech Sports Med, 2010, 18: 11–17. [Google Scholar]
- 7. Hintermann B, Boss A, Schäfer D. Arthroscopic findings in patients with chronic ankle instability. Am J Sports Med, 2002, 30: 402–409. [DOI] [PubMed] [Google Scholar]
- 8. Coughlin M, Mann R, Saltzman C, et al Surgery of the Foot and Ankle, 8th edn Philadelphia, PA: Elsevier, 2007; 1020–1021. [Google Scholar]
- 9. Reilingh ML, Beimers L, Tuijthof GJ, Stufkens SA, Maas M, van Dijk CN. Measuring hindfoot alignment radiographically: the long axial view is more reliable than the hindfoot alignment view. Skeletal Radiol, 2010, 39: 1103–1108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Frigg A, Nigg B, Hinz L, Valderrabano V, Russell I. Clinical relevance of hindfoot alignment view in total ankle replacement. Foot Ankle Int, 2010, 31: 871–879. [DOI] [PubMed] [Google Scholar]
- 11. Kelikian AS. Sarrafian's Anatomy of Foot and Ankle, 3rd edn Philadelphia: Lippincott, 2011; 538–541. [Google Scholar]
- 12. Milner CE, Soames RW. The medial collateral ligaments of the human ankle joint: anatomical variations. Foot Ankle Int, 1998, 19: 289–292. [DOI] [PubMed] [Google Scholar]
- 13. Harper MC. Deltoid ligament: an anatomical evaluation of function. Foot Ankle, 1987, 8: 19–22. [DOI] [PubMed] [Google Scholar]
- 14. Lapidus PW. Kinesiology and mechanical anatomy of the tarsal joints. Clin Orthop Relat Res, 1963, 30: 20–36. [PubMed] [Google Scholar]
- 15. Yu GR, Yang YF, Zhang K, et al The effect of ankle and subtalar joint on the hindfoot motion. Zhong Hua Gu Ke Za Zhi, 2005, 25: 236–239. (In Chinese). [Google Scholar]
- 16. Hintermann B. Medial ankle instability. Foot Ankle Clin, 2003, 8: 723–738. [DOI] [PubMed] [Google Scholar]
- 17. Bohay DR, Anderson JG. Stage IV posterior tibial tendon insufficiency: the tilted ankle. Foot Ankle Clin, 2003, 8: 619–636. [DOI] [PubMed] [Google Scholar]
- 18. Ellis SJ, Williams BR, Wagshul AD, Pavlov H, Deland JT. Deltoid ligament reconstruction with peroneus longus autograft in flatfoot deformity. Foot Ankle Int, 2010, 31: 781–789. [DOI] [PubMed] [Google Scholar]
- 19. Hintermann B, Valderrabano V, Kundert HP. Lengthening of the lateral column and reconstruction of the medial soft tissue for treatment of acquired flatfoot deformity associated with insufficiency of the posterior tibial tendon. Foot Ankle Int, 1999, 20: 622–629. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Video Image