

Abstract
Objective: To evaluate the early and middle‐term results of in situ single screw fixation and subtrochanteric osteotomy of the femur with external fixator for slipped capital femoral epiphysis (SCFE).
Methods: From June 1998 to July 2008, 11 patients (seven male [eight hips] and four female [four hips]) of average age 14.3 years (range, 9–18 years) were treated in our hospital. According to the Southwick measurement, seven hips were mildly affected (<30°), two moderately (30–50°), and three severely (>50°). The average body mass index (BMI) was 31.1 g/m2 (range, 27–35 g/m2). All the mild and moderate cases underwent in situ single screw fixation, and the three severe cases subtrochanteric osteotomy of femur with external fixator. All cases were evaluated both clinically and radiographically at 3 months, 6 months and every year postoperatively.
Results: All cases were followed up for 2–12 years (average 5.6 years). The Harris hip score increased from a mean of 74.8 (70 ∼ 85) points preoperatively to 90.6 (70 ∼ 100) points postoperatively. X‐ray films showed epiphyseal closure in the in situ single screw fixation cases, and no further increase in epiphyseal‐shaft angle. Partial reduction of slipped epiphysis with normal joint spaces was observed after subtrochanteric osteotomy of the femur in the external fixator cases.
Conclusion: In situ single screw fixation for treating mild and moderate SCFE has a satisfactory clinical outcome, and the advantage of prevention of further slippage. Subtrochanteric osteotomy of the femur with external fixator is suitable for severe SCFE with late deformity; the realignment procedure can correct deformity and postpone or prevent subsequent osteoarthritis.
Keywords: Epiphyses, Hip, Osteotomy, Treatment outcome
Introduction
Slipped capital femoral epiphysis (SCFE) is the most common of the adolescent hip disorders, usually occurs in obese children and is slightly more common in males. The cause of idiopathic SCFE is unknown. It may be associated with endocrine disorders, renal bone dysplasia, and a history of radiation treatment 1 . It disrupts the normal relationship of the femoral head with the acetabulum, resulting in anterior‐superior dislocation of the femoral neck at the physeal plate level (except for the rare valgus slip, in which the displacement is posterior‐superior), and that affects the proximal femoral epiphysis adversely. The displacement can be acute and severe or very gradual and mild. There is a high incidence of the disease in Western countries, its diagnosis and treatment having been reported often. However, there have been few case reports about Chinese patients.
The age of onset is reported to range from 10 to 15 years. An SCFE diagnosis mandates institution of treatment as soon as possible to prevent progression of the slippage, and to prevent complications such as osteonecrosis of the femoral head (ONFH) or chondrolysis 2 . Delay in diagnosis clearly worsens the prognosis. Long‐term complications after correction of the slip often include limitation in movement, particularly flexion and internal rotation, associated with secondary osteoarthritis, which forces the patients to undergo artificial joint replacement at a young age. Recent studies suggest that SCFE requires emergency surgical treatment in order to minimize the likelihood of complications 3 , 4 . The aim of the present research was to evaluate the early and middle‐term results of in situ single‐screw fixation and subtrochanteric osteotomy of the femur with external fixator for SCFE.
Materials and methods
Patients' data
From June 1998 to July 2008, 11 patients (12 hips) were treated in our hospital. There were seven male (eight hips) and four female patients (four hips) with an average age of 14.3 years (range, 9–18 years). The average BMI was 31.1 g/m2 (range, 27–35 g/m2). One case was of acute onset following minor trauma and the others were chronic. The main symptoms in nine patients (ten hips) were hip pain, including three with ipsilateral thigh and knee pain, and one with groin pain; in the other two cases (two hips) the affected side had limited mobility and weight‐bearing capacity. In five cases (five hips) the patients also had claudication. Physical examination showed mild external rotation of the hips, groin tenderness at the midpoint, and limitation of hip mobility which was most obvious for internal rotation. The time interval between the onset of symptoms and diagnosis was 1 to 30 months with an average of 6 months. One case was associated with hypothyroidism.
Anteroposterior (AP) pelvic and frog‐type X‐ray films were taken before surgery to measure the degree of SCFE. According to measurement of the Southwick 5 , 6 (epiphyseal–shaft) angle, six cases (seven hips) were Grade I (mild, <30°), two cases (two hips) Grade II (moderate, 30–50°), and 3 cases (3 hips) Grade III (severe, >50°). All the mild and moderate cases underwent in situ single screw fixation, and the three severe cases were subjected to subtrochanteric osteotomy of the femur with external fixator.
Surgical procedures
In situ single screw fixation
Patients with Grade I and II hips were treated with in situ single screw fixation. The patients were placed in a supine position. The operator applied gentle traction, abduction and internal rotation to achieve operative hip reduction. Under fluoroscopic guidance, a guide pin was then driven into the center of the epiphysis and perpendicular to the physis through the greater trochanter. A 1 cm incision was made in the needle entry area, and a channel created along the guide pin. After measuring the length of screw required, a 6.5‐mm‐diameter cannulated screw was inserted along the guide pin. The principle was to make sure the screw was in the center of the epiphysis and perpendicular to the physis both on the AP and lateral views. The screw thread had to inserted through the entire epiphysis with appropriate pressure without puncturing the femoral head.
Subtrochanteric osteotomy of the femur with external fixator
Patients with Grade III hips were treated with subtrochanteric osteotomy of femur combined with external fixation. The patients were placed in a supine position with the affected hip elevated. A 5–6 cm longitudinal incision was made from 2 cm above the greater trochanter along the long axis of the femur. The skin, subcutaneous tissue and deep fascia were incised, and the vastus lateralis muscle then pulled to the front. The inferior surface of the greater trochanter was exposed, then the guide wire for external fixation was inserted from the lateral side of the greater trochanter. The osteotomy plane was set 2 cm under the subtrochanteric surface, and another guide wire for external fixation was inserted 8 cm under the osteotomy plane. The osteotomy was performed with a wire saw, the femur abducted and externally rotated, then adjusted and the external fixation installed. Two 5‐mm‐diameter Steinmann pins were inserted into the upper and inferior aspects of the osteotomy surface, and then attached to the external fixator. Another external fixator was fixed to the anterolateral femur in the same way. The two external fixators were then connected with a link rod (Fig. 1).
Figure 1.
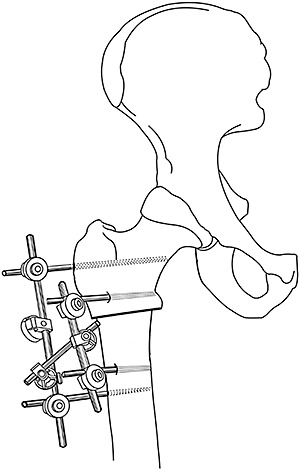
Diagrammatic representation of the external fixator.
During the operation, fluoroscopic guidance was observed carefully. Care was taken to ensure that the neck‐shaft angle shown in the AP X‐ray film and the angle formed by vertical line of the femoral epiphyseal plate and the axis of the femoral shaft in the lateral X‐ray view were the same as in the healthy hip. Any coxa vara and external rotation deformity were corrected after fixation.
Postoperative management and follow‐up
There was no need for traction and immobilization after the operation. Antibiotics were used for the first 48 hours after surgery. The patients with unilateral lesions were restricted to weight‐bearing with crutches for 2–3 days postoperatively, instructed to avoid weight‐bearing for the first 6 weeks, then to advance to 50% weight‐bearing for the second 6 weeks, and to 75% for the third 6 weeks. Unrestricted activities were permitted 1 year after the operation. One patient with bilateral in situ screw fixation was fitted with abduction cast immobilization for 8 weeks after operation and then began limited weight‐bearing with crutches for the next 6 months. All cases were evaluated both clinically and radiographically at 3 months, 6 months and every year postoperatively. The Harris score system was used to assess hip function every year postoperatively. The screw was removed after epiphyseal closure had occurred and the external fixator was removed when the osteotomy had healed.
Results
All cases were followed up for 2–12 years with an average of 5.6 years. The internal fixations of six cases (seven hips) were removed 1 to 3 years after surgery. Three patients with subtrochanteric osteotomy with external fixation were followed up for 3 months after surgery, and the external fixators removed after their X‐ray films showed healing of osteotomy. Except for one patient with in situ single‐screw fixation, all the patients' symptoms, especially limb pain, were relieved by surgery, including resolution of limping gait. The Harris hip score increased from a mean of 74.8 (70 ∼ 85) points preoperatively to 90.6 (70 ∼ 100) points postoperatively, 10 hips being classified as excellent (2, 3), one as good, one as fair and none as poor. The combined excellent and good rate was 91.7% (11/12).
Figure 2.

A 13 year male patient with left hip pain for 5 months, the Harris score was 74. (a,b) Preoperative AP and lateral X‐ray films show grade I SCFE. (c,d) Postoperative AP and lateral X‐ray films show in situ single‐screw fixation. (e,f) Two year after the operation, AP and lateral X‐ray films show epiphyseal closure and no further increase in epiphyseal‐shaft angle.
Figure 3.
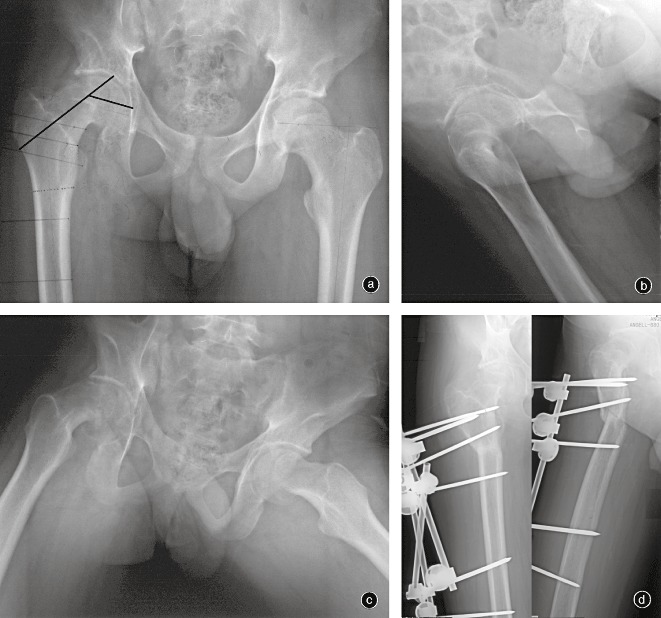
A 18 year male patient with right hip pain and claudication for 2 years, the Harris score was 72 points. (a,b) Preoperative AP and lateral X‐ray films show grade III SCFE with coxa vara (c) Preoperative Lauenstein X‐ray films show the extent of slipping. (d) Postoperative AP and lateral X‐ray films show good correction of deformity.
The X‐ray films showed epiphyseal closure and increased density of the femoral head in the in situ single‐screw fixation cases, with no further increase in epiphyseal‐shaft angle and no significant changes in femoral head shape. Partial reduction of the slipped epiphysis with normal joint spaces was observed in the patients with subtrochanteric osteotomy of the femur with external fixator. There were no bony hyperplasia of the femoral head and acetabulum and no joint space narrowing in any of the cases.
Screw loosening was found in one Grade II patient with in situ single screw fixation six months after surgery. The loose screw was replaced by a longer screw of the same diameter with pressure. After 2‐years of follow‐up, the slip angle had not increased, but mild pain and claudication symptoms had persisted, and the functional recovery of the hip was poor. The Harris score was 70 points both before and 2 years after surgery, the X‐ray films showed epiphyseal closure and that the femoral head had enlarged slightly, but without joint space narrowing
Discussion
Early diagnosis of slipped capital femoral epiphysis
Slipped capital femoral epiphysis is the most common of the adolescent hip disorders. Patients typically present with knee, hip, groin, and thigh pain, and external rotation of the extremity with a limp (out‐toe gait) is one of the commonest signs. Because its symptoms are not obvious in some cases, it is easy to misdiagnose clinically. The most important physical findings are in the range of hip movement. Because limited internal rotation is universal in SCFE patients, this symptom should place the physician on high alert. It had taken 30 months from the onset of symptoms to make the diagnosis in one of the patients in our group, by which time the disease had progressed to severe coxa vara, necessitating an osteotomy. Imaging examinations for the diagnosis of SCFE includes X‐ray, CT scan and ultrasound 7 . Plain radiographs are generally sufficient for the diagnosis of SCFE. AP and frog‐leg lateral views should be requested, and sometimes a Lauenstein view (both hips in abduction and external rotation) is a more sensitive diagnostic tool for an early slip. On the AP view, Klein's line, which is drawn along the superior aspect of the femoral neck, will normally intersect some part of the femoral head. In SCFE, however, this line does not intersect the femoral head.
Operative techniques for slipped capital femoral epiphysis
In situ single‐screw fixation
The treatment of SCFE aims to prevent further slippage and decrease the risk of later osteoarthritis of the hip. In situ single‐screw fixation is the widely accepted golden standard of treatment for SCFE 1 , 2 , it is a minimally invasive procedure and the technique is easy 1 , 8 . In a study of 59 hips of grade I and II SCFE patients undergoing in situ single‐screw fixation with an average 30‐year follow‐up, only 20% of grade I and 33% of grade II patients showed mild osteoarthritis on imaging 8 . Another group of 53 hips with an average of 2‐years follow‐up showed a 94% excellent and good rate, only one case showing chondrolysis 9 . The excellent and good rate of this study was 91.7%, similar to that previously reported. However, this procedure is suitable only for mild to moderate patients and the surgical indications should be strictly observed.
A single screw significantly reduces the risk of penetrating articular surface and minimizes injury to the epiphysis. The complications of nailing in situ include nail penetration and inaccurate positioning, fractures of the femoral neck at the subtrochanteric level, and progression of the slip due to loss of anchorage in the epiphysis. An experienced surgeon who is familiar with special anatomical relationships in this area can avoid most of these complications. The nail must enter the central part of the epiphysis, so it is essential that the direction of the slip of the epiphysis should be carefully studied on both the AP and lateral views before operating.
Subtrochanteric osteotomy of the femur with external fixator
For severe SCFE patients (Grade III), limitation of flexion and external rotation deformity can cause difficulties with sitting and other flexion activities as well as in gait. This can result in the patient having symptoms of pain, stiffness, femoro‐acetabular impingement and osteoarthritis and, ultimately, joint damage 10 . Therefore, a number of realignment procedures have been recommended 11 , 12 , 13 . Subtrochanteric osteotomy of the femur with external fixator can correct the external rotational deformity as well as coxa vara. This procedure does not cut the joint capsule, effectively preserves the blood supply of the femoral head and reduces the incidence of ONFH. All three patients had good treatment outcomes; this may be related to implementing surgery before cartilage lesions had developed. However, there are few cases in this group and the follow‐up time is short; its long‐term results are still to be observed.
Kartenbender et al. reported the clinical results of a group of 35 SCFE patients (39 hips) treated with Imhauser osteotomy 14 . The mean follow‐up time was 13.7 years (range, 8–17 years). 77% of the patients had good to excellent clinical results, and 67% had good to excellent results on radiology. Only two patients developed osteonecrosis. Another study of three patients with mild slips and signs of impingement treated with in situ pinning and immediate arthroscopic osteoplasty was reported recently 15 . Overall, treatment of Grade III SCFE patients is still a relatively difficult problem. Jerne et al. reported 36 patients (37 hips) with SCFE who were treated by realignment osteotomy 16 . The mean follow‐up time was 33.8 years (26 to 42 years). The clinical and radiological results were excellent or good in 41% (9/22) of the hips treated by subcapital osteotomy, in 36% (4/11) treated by intertrochanteric osteotomy and in none treated by manipulative reduction. In all, seven hips (19%) had had arthrodesis or total hip replacement. The natural history of SCFE was probably not improved by any of the treatments used in the study. Therefore, the diagnosis of SCFE should be made as soon as possible, so as not to delay treatment.
In summary, SCFE is a common adolescent hip disorder which would result in little short‐term morbidity and few long‐term sequelae if the diagnosis was made and treatment performed prior to the development of severe deformity. A‐P and frog‐leg lateral radiographs are necessary for the timely diagnosis of SCFE in its early stages, when simple in situ surgical treatment can prevent severe secondary hip dysfunction. At later stages, with more deformity present, more complex treatment can still be effective 17 .
Disclosure
The manuscript submitted does not contain information about medical device(s)/drug(s). No benefits in any form have been, or will be, received from a commercial party related directly or indirectly to the subject of this manuscript.
Acknowledgments
This work was supported by the National Natural Science Foundation of China under grant No. (30672117).
References
- 1. Gholve PA, Cameron DB, Millis MB. Slipped capital femoral epiphysis update. Curr Opin Pediatr, 2009, 21: 39–45. [DOI] [PubMed] [Google Scholar]
- 2. Fabry G. Clinical practice: the hip from birth to adolescence. Eur J Pediatr, 2010, 169: 143–148. [DOI] [PubMed] [Google Scholar]
- 3. Pelillo F, De Sanctis N, Benazzo F, et al Slipped upper femoral epiphysis (SUFE): to do or not to do in sufe. Hip Int, 2009, 19 (Suppl 6): S13–S17. [DOI] [PubMed] [Google Scholar]
- 4. Aronsson DD, Loder RT, Breus GJ, et al Slipped capital femoral epiphysis: current concepts. J Am Acad Orthop Surg, 2006, 14: 666–679. [DOI] [PubMed] [Google Scholar]
- 5. Southwick WO. Osteotomy through the lesser trochanter for slipped capital femoral epiphysis. J Bone Joint Surg Am, 1967, 49: 807–835. [PubMed] [Google Scholar]
- 6. Southwick WO. Slipped capital femoral epiphysis. J Bone Joint Surg Am, 1984, 66: 1151–1152. [PubMed] [Google Scholar]
- 7. Terjesen T. Ultrasonography for diagnosis of slipped capital femoral epiphysis: comparison with radiography in 9 cases. Acta Orthop Scand, 1992, 63: 653–657. [DOI] [PubMed] [Google Scholar]
- 8. Hansson G, Billing L, Högstedt B, et al Long‐term results after nailing in situ of slipped upper femoral epiphysis. A 30‐year follow‐up of 59 hips. J Bone Joint Surg Br, 1998, 80: 70–77. [DOI] [PubMed] [Google Scholar]
- 9. Kenny P, Higgins T, Sedhom M, et al Slipped upper femoral epiphysis. A retrospective, clinical and radiological study of fixation with a single screw. Pediatr Orthop B, 2003, 12: 97–99. [DOI] [PubMed] [Google Scholar]
- 10. Diab M, Hresko M, Millis MB. Intertrochanteric versus subcapital osteotomy in slipped capital femoral epiphysis. Clin Orthop Relat Res, 2004, 427: 204–212. [DOI] [PubMed] [Google Scholar]
- 11. Tokmakova KP, Stanton RP, Mason DE. Factors influencing the development of osteonecrosis in patients treated for slipped capital femoral epiphysis. J Bone Joint Surg Am, 2003, 85: 798–801. [DOI] [PubMed] [Google Scholar]
- 12. Schai P, Exner G. Corrective Imhauser intertrochanteric osteotomy. Oper Orthop Traumatol, 2007, 19: 368–388. [DOI] [PubMed] [Google Scholar]
- 13. Leunig M, Slongo T, Ganz R. Subcapital realignment in slipped capital femoral epiphysis: surgical hip dislocation and trimming of the stable trochanter to protect the perfusion of the epiphysis. Instr Course Lect, 2008, 57: 499–507. [PubMed] [Google Scholar]
- 14. Kartenbender K, Cordier W, Katthagen BD. Long‐term follow‐up study after corrective Imhäuser osteotomy for severe slipped capital femoral epiphysis. J Pediatr Orthop, 2000, 20: 749–756. [DOI] [PubMed] [Google Scholar]
- 15. Leunig M, Horowitz K, Manner H, et al In situ pinning with arthroscopic osteoplasty for mild SCFE: a preliminary technical report. Clin Orthop Relat Res, 2010, 468: 3160–3267 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Jerne R, Hansson G, Wallin J, et al Long‐term results after realignment operations for slipped upper femoral epiphysis. J Bone Joint Surg Br, 1996, 78: 745–750. [PubMed] [Google Scholar]
- 17. Weigall P, Vladusic S, Torode I. Slipped upper femoral epiphysis in children–‐delays to diagnosis. Aust Fam Physician, 2010, 39: 151–153. [PubMed] [Google Scholar]