

Abstract
Purpose:
The aim of this study was to investigate the correlation between the use of anabolic-androgenic steroids (AASs) among the population of Jeddah, Saudi Arabia, and their knowledge and attitudes.
Methods:
This was a community-based, cross-sectional observational study. This study was conducted using a questionnaire that was distributed among the population during the period from February 3, 2018, to February 25, 2018. This questionnaire comprised 31 questions, designed to evaluate the knowledge and attitudes toward using AASs.
Results:
A total of 300 participants were enrolled in the study. The mean age of the population was 30.66 ± 9.2 years. Fourteen participants admitted using AASs, with a percentage of 4.7%, among whom 85.7% were male (P = 0.0005). Seventy-eight percent of AAS users believed that AASs do not cause tolerance when taken for a longtime (P = 0.023). However, the majority of both AAS users and nonusers did not agree on taking AASs for a longtime. Our results showed a strong correlation between not taking AASs and not consuming energy drinks (P = 0.0023). Half of our respondents exhibited poor knowledge regarding the side effects of AASs. The level of knowledge did not correlate with the use of AAS, gender, exercising, or consuming energy drinks.
Conclusion:
The results showed poor knowledge regarding using AASs among the population of Jeddah. Thus, we recommend having a national awareness program in order to prevent the possible side effects of misusing AASs.
Keywords: Anabolic-androgenic steroid, Jeddah, knowledge, testosterone
INTRODUCTION
Anabolic-androgenic steroids (AASs) are synthetic testosterone hormones. Testosterone is the male gonadal hormone, which is synthesized and released from Leydig cells in the testes.[1] This hormone is responsible for the development and maturation of male secondary characteristics, such as a deep voice and the growth of facial hair. Its effect is beyond the androgenic effect, and it has an anabolic effect as well. This hormone promotes protein synthesis, maintains muscle mass, increases bone density, and stimulates erythropoiesis.[1] Testosterone and AASs are used clinically as a hormone replacement therapy for male hypogonadism.[2] Furthermore, AASs have been approved to be used as a treatment for osteoporosis alone or with estrogen in menopausal women, as well as for severe burns[3] and human immunodeficiency virus-induced muscle wasting.[4] However, a supraphysiological dose of AAS can cause serious side effects, including negative feedback inhibition to the hypothalamic–pituitary axis, consequently causing infertility and gynecomastia in men.[5] Other adverse effects caused by AASs include aggressiveness,[6,7] abnormal renal function,[8] hypertension, and heart failure.[9,10]
Although the World Anti-Doping Agency listed AASs as prohibited substances,[11] they are misused by athletes to enhance their performance and increase their muscle mass with a short duration. Certainly, the widespread use of AASs by athletes and bodybuilders increases their general acceptance among the public.[12] Furthermore, the recent changes of the attitudes of people toward healthy lifestyles and exercise can contribute to the use of AASs among them.[13]
While it has been shown in a meta-analysis that the global prevalence of AAS use was 3.3%,[14] the estimated prevalence of AAS users in the USA is 79.6%.[15] Therefore, AASs are widely used among different geographic locations. Few studies were conducted to estimate the prevalence and knowledge of AAS users in Saudi Arabia.[13,16,17,18] However, none of them was conducted specifically on the population of Jeddah. Thus, the aim of this study was to assess the level of knowledge, attitude, and practice of the population of Jeddah toward using AASs. The results of this study can aid in planning a national public awareness program about using AASs.
METHODS
Study design and setting
This observational, cross-sectional survey was conducted to correlate the use of AASs with the knowledge of the population of Jeddah, Saudi Arabia. It was conducted using an electronic questionnaire comprising 31 questions divided into three parts [Table 1]. The first part was related to the demographic data of the participants. The aim of the second part was to assess the beliefs of the participants regarding using AASs. The aim of the third and last part was to assess the level of knowledge of the participants regarding using AASs and their side effects. The questionnaire was in Arabic. The first version of the questionnaire was distributed to a random population as a pilot study. This questionnaire was reviewed and validated by a statistician. The validated version of the questionnaire was distributed electronically during the period from February 3, 2018 to February 25, 2018. This questionnaire was self-reported by the participants. However, the participants must agree to participate before starting the questionnaire. Moreover, the study was well explained at the beginning of the questionnaire. The study protocol and questionnaire were approved by the Unit of Biomedical Ethics-Research Committee, Faculty of Medicine, King Abdulaziz University (reference no. 171-19).
Table 1.
Main questions in the study questionnaire
| Part | Main question |
|---|---|
| Part I | |
| Demographic data | Demographic data included age, gender, level of education, height and weight, marital status, number of children, job, using AASs, type of AAS, and source of AAS |
| Part II | |
| Attitude of the participants regarding using AASs | Do you agree to use AASs for a long time? Do you think AASs cause tolerance after prolonged use, consuming energy drinks, exercising, and having routine medical checkups? |
| Part III | |
| Knowledge regarding using AASs and their side effects | Do you know that AASs can cause hypertension, heart failure, gynecomastia in males, and infertility? |
AASs: Anabolic-androgenic steroids
Sampling
Our pilot study showed that the mean number of newly registered participants in the different gym facilities in Jeddah is 5000. Thus, the sample size was calculated using Raosoft sample size calculator (http://www.raosoft.com/samplesize.html). On the basis of a 95% confidence level, 5% margin of error and assuming that only third of the population will response to the questionnaire, the estimated final sample size was 304 participants. The inclusion criteria were being an adult, being either male or female, any nationality, and willingness to participate. The exclusion criteria were being under 18 years of age and having any physical and/or mental conditions that prevent the participant from answering questions.
Statistical analysis
Data were entered and analyzed using the Statistical Package for the Social Sciences (SPSS) software, version 23.0.0 (SPSS Inc., Chicago, IL, USA). Descriptive statistics were carried out for all variables and expressed as the mean ± standard deviation for continuous variables, such as age and body mass index (BMI), and as frequencies and percentages for each answer about the level of knowledge, attitude, and belief toward the use of AASs. Factors associated with AAS users and the correlation between AAS users and level of knowledge were analyzed by a Chi-squared test. P <0.05 was considered statistically significant.
RESULTS
Sociodemographic data
In this study, a total of 300 participants answered the online questionnaire. Table 2 shows the sociodemographic characteristics of the participants included in the study. The mean age of the participants was 30.66 ± 9.2 years. The majority were females, comprising 59.7% of all participants, whereas 40.3% of them were males. Half of the participants were single. Almost 40% of the participants in the study were students, whereas only 6.7% were athletes.
Table 2.
Sociodemographic characteristics of the participants (n=300)
| Parameters | Count (%) |
|---|---|
| Age (years) | 30.66±9.2 |
| Gender | |
| Male | 121 (40.3) |
| Female | 179 (59.7) |
| Marital status | |
| Single | 152 (50.7) |
| Married | 148 (49.3) |
| Job | |
| Free business | 53 (18.6) |
| Administrative | 100 (35.1) |
| Athlete | 19 (6.7) |
| Student | 113 (39.6) |
| Using AASs | |
| Yes | 14 (4.7) |
| No | 286 (95.3) |
AASs: Anabolic-androgenic steroids
Characteristics of anabolic-androgenic steroid users
In our population, only 14 participants admitted using AASs once in their lives [Table 3]. Both AAS users and nonusers were comparable in terms of the mean age, BMI, and number of children (P = 0.285, P = 0.778, and P = 0.24, respectively). Compared to AAS nonusers, AAS users were mostly males (P = 0.0005) (12 males and only 2 females). A third of AAS users were students, whereas 14.3% were athletes. Regarding the reasons behind using AASs, 37.2% of the users stated that they used AASs because of the previous personal experiences, whereas only 11.4% used AASs as per their coach's advice or for other personal experiences [Figure 1]. The AAS users in this study reported taking AASs through injections and orally. The three most common types of AASs used in our population were stanozolol, methandrostenolone, and methenolone.
Table 3.
Comparison of the demographic characteristics between anabolic-androgenic steroid users and nonusers
| Variable | AAS user (n=14), % | AAS nonuser (n=286), % | P |
|---|---|---|---|
| Mean age (years) | 27.64 | 30.58 | 0.285 |
| Mean BMI (kg/m2) | 25.85 | 27.03 | 0.778 |
| Number of children (mean) | 1.43 | 2.23 | 0.24 |
| Gender | |||
| Male | 85.7 | 38.1 | 0.0005 |
| Female | 14.3 | 61.9 | |
| Job | |||
| Student | 35.7 | 39.9 | 0.685 |
| Administrative | 35.7 | 35 | |
| Free business | 14.3 | 18.9 | |
| Athlete | 14.3 | 6.5 |
AASs: Anabolic-androgenic steroids, BMI: Body mass index
Figure 1.
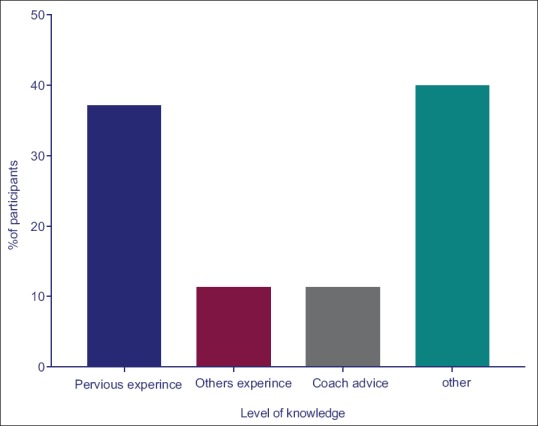
Reasons for using anabolic-androgenic steroids
Assessment of the knowledge and attitude toward using anabolic-androgenic steroids
Table 4 shows the participants’ beliefs regarding using AASs among AAS users and nonusers. The majority of participants from both groups did not agree with using AASs for a longtime (P = 0.018). Only one AAS user and two AAS nonusers agreed on using AASs for a longtime. Significantly, the majority of AAS users (78.6%) did not agree that AASs cause tolerance (P = 0.023). Compared to AAS users, the majority of AAS nonusers did not consume energy drinks (P = 0.0023).
Table 4.
Beliefs and attitudes toward using anabolic-androgenic steroids between anabolic-androgenic steroid users and nonusers
| Variable | Percentage of AAS users (n=14) | Percentage of AAS nonusers (n=286) | P |
|---|---|---|---|
| Do you agree on using AASs for a long time? | |||
| Yes | 7.1 | 0.7 | 0.018 |
| No | 92.9 | 99.3 | |
| Do you think AASs cause tolerance after prolonged use? | |||
| Yes | 21.4 | 52.4 | 0.023 |
| No | 78.6 | 47.6 | |
| Consuming energy drinks | |||
| Yes | 42.9 | 13.3 | 0.0023 |
| No | 57.1 | 86.7 |
AASs: Anabolic-androgenic steroids
Table 5 shows the frequency and percentage of participants’ knowledge regarding the potential adverse effects of AASs. Around 40% of the participants knew that AASs can cause hypertension. In the same line, half of the participants knew that AASs can cause heart failure. However, 65.8% of the participants knew that AASs can cause gynecomastia in males.
Table 5.
Frequency and percentage of participants’ knowledge regarding the potential adverse effects of anabolic-androgenic steroids
| Question | Frequency (%) |
|---|---|
| Do you know AASs can cause hypertension? | |
| Yes | 122 (40.7) |
| No | 168 (59.3) |
| Do you know AASs can cause heart failure? | |
| Yes | 154 (51.3) |
| No | 146 (48.7) |
| Do you know AASs can cause gynecomastia in males? | |
| Yes | 197 (65.7) |
| No | 103 (34.3) |
AASs: Anabolic-androgenic steroids
Next, the level of the participants’ knowledge toward AASs was assessed. Figure 2 shows that half of the participants had poor knowledge, and only 23% of them showed a strong level of knowledge. Table 6 shows the characteristics of the participants according to their level of knowledge. There was no significant difference in the level of knowledge between AAS users and nonusers (P = 0.691). In the same line, the level of knowledge was comparable between males and females (P = 0.5), participants who were exercising (P = 0.157), participants on regular medical checkups (P = 0.222), and participants consuming energy drinks (P = 0.252). Overall, all groups showed inadequate knowledge regarding AASs.
Figure 2.
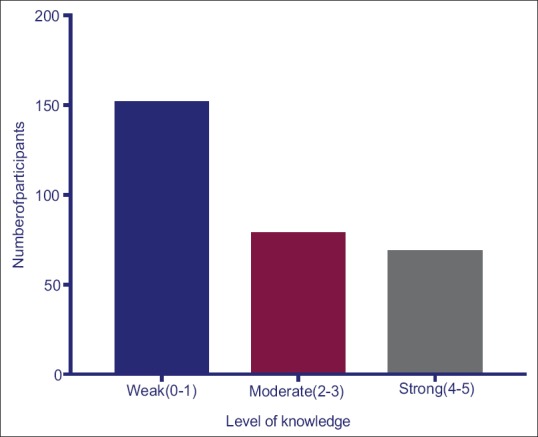
Levels of participants’ knowledge
Table 6.
Characteristic of participants according to their level of knowledge
| Characteristics | Level of knowledge (%) | P | ||
|---|---|---|---|---|
| Poor (0-1) | Moderate (2-3) | Strong (4-5) | ||
| Using AASs | ||||
| User (n=14) | 35.7 | 28.6 | 35.7 | 0.691 |
| Nonuser (n=286) | 44.8 | 29.4 | 25.9 | |
| Gender | ||||
| Male (n=121) | 47.9 | 25.6 | 26.4 | 0.5 |
| Female (n=179) | 52.5 | 26.8 | 20.7 | |
| Exercising | ||||
| Yes (n=73) | 41.1 | 32.9 | 26 | 0.157 |
| No (n=227) | 53.7 | 24.2 | 22 | |
| Routine medical checkup | ||||
| Yes (n=53) | 45.3 | 22.6 | 32.1 | 0.222 |
| No (n=247) | 51.8 | 27.1 | 21.1 | |
| Consuming energy drinks | ||||
| Yes (n=44) | 47.7 | 36.4 | 15.9 | 0.252 |
| No (n=238) | 47.9 | 26.5 | 25.6 | |
AASs: Anabolic-androgenic steroids
DISCUSSION
In this study, we assessed the knowledge, attitudes, and practices of the population of Jeddah toward using AASs. Moreover, we characterized AAS users among the population of Jeddah. Although the participants who admitted that they had used AASs were only 14, it was significant that the use of AASs was strongly correlated with the male gender. In the same line, our results showed that there is a strong correlation between who are not consuming energy drinks and those who are using AASs. Finally, our results indicated that the majority of our participants showed poor knowledge toward using AASs and their adverse effects.
The prevalence of AAS users in our population was 4.7%. However, previous studies in Saudi Arabia reported a much higher prevalence of AAS users in Riyadh (capital of Saudi Arabia) (30.5%)[16] and Jazan (31%).[18] The differences between our results and theirs could be due to the geographical distribution. Remarkably, Althobiti et al. recently conducted a national cross-sectional survey on 4860 gym-going participants from different regions in Saudi Arabia.[13] They reported that the prevalence of AAS users in all regions of Saudi Arabia was 9.8%. However, more than half of them (54.2%) were living in the central region of Saudi Arabia (where the city of Riyadh belongs). The prevalence of AAS users in our study was lower than that reported in other Arabian countries, such as Jordan (26%),[19] Kuwait (22.7%),[20] and UAE (22%).[21] Notably, it has been shown in the previous studies that the prevalence of AAS users was much higher in Western countries, such as the USA (79.6%)[15] and UK (70%).[22] These differences in the prevalence can be attributed to the fact that using AASs in Arabian countries in general, particularly in Saudi Arabia, is socially unaccepted and illegal. This prevents many AAS users from admitting using AASs. In agreement with the survey performed in Riyadh by Al Bishi and Afify,[17] the most common types of AASs reported to be used were stanozolol and methandrostenolone. This reflects the preference and availability of AASs in Saudi Arabia.
In our study, we showed that only 11% of our population used AASs as per their coach's advice. On the contrary, it has been shown in other studies carried out in Saudi Arabia,[13] Jordan,[19] and Kuwait[20] that the gym coach was the main source of information and the main provider of AASs.
In this study, efforts have been made to characterize the patients at risk of using AASs. The factor that most predicts using AASs in our population was the male gender. This is in agreement with a previous study that was carried out in the UK.[18] Remarkably, to the best of our knowledge, no previous research was carried out in Saudi Arabia with the intention of estimating the percentage of females using AASs. In our study, we found two women out of 14 to be AAS users. This highlights the importance of including women in future surveys. Another significant predictive factor for using AASs is the consumption of energy drinks. Our results showed a significant correlation between not consuming energy drinks and not using AASs. The percentage of AAS users among athletes was more than twice as high as in AAS nonusers, although this was not significant. This reflects the fact that athletes are at a higher risk of using AASs. The difference in the number of children was not significant between AAS users and nonusers. However, this could be related to the current cultural preference, where families tend to be smaller. In agreement with the previous studies,[13] there was no difference in the BMI between AAS users and nonusers. Noticeably, both groups tend to be in the overweight range. This trend was noticed in other studies as well.[13]
Interestingly, the majority of our population showed poor knowledge about the adverse effects of AASs. There were no significant differences in the level of knowledge with regard to using AASs, gender, and exercising. This poor level of knowledge was also observed in previous studies that were performed on Arabian populations such as those in Riyadh,[16,17] UAE,[21] and Jordan.[19] This highlights the need for a pan-national awareness program on the use of AASs and their adverse effects.
Although this is the first study carried out on the population of Jeddah regarding the use of AASs, it had some limitations that must be declared. There is a risk of recall bias since the questionnaire was self-reported. However, this method has been chosen in order to guarantee the participants’ privacy and confidentiality while answering some questions that may cause embarrassment. Furthermore, the small number of AAS users could be another limitation in this study, which could not be prevented using an online survey. Another explanation for the small percentage of AAS users in our study could be attributed to the fact that more females responded to our survey than males, because using AASs is less common in females, especially in our community.
CONCLUSION
Our results helped shed light on the inadequate level of knowledge about the use of AASs among the population of Jeddah, Saudi Arabia. Based on our results, a national public awareness program is needed to educate the community about using AASs and their adverse effects. This program must target all the population of Jeddah, regardless of their age, gender, and fitness habits. Awareness companions must not be exclusive to athletes only. Schools, shopping malls, and primary health-care centers must be covered. Despite the small percentage of AAS users in our survey, the real number of AAS users in Jeddah could be higher owing to underreporting bias by the participants. Thus, more large-scale community-based surveys are required.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
The authors would like to thank all the participants in this survey for their cooperation and time. Special thanks to Dr. Fatma M. Al-Qudsi for reviewing the questionnaire.
REFERENCES
- 1.Joseph JF, Parr MK. Synthetic androgens as designer supplements. Curr Neuropharmacol. 2015;13:89–100. doi: 10.2174/1570159X13666141210224756. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Wu C, Kovac JR. Novel uses for the anabolic androgenic steroids nandrolone and oxandrolone in the management of male health. Curr Urol Rep. 2016;17:72. doi: 10.1007/s11934-016-0629-8. [DOI] [PubMed] [Google Scholar]
- 3.Demling RH, Orgill DP. The anticatabolic and wound healing effects of the testosterone analog oxandrolone after severe burn injury. J Crit Care. 2000;15:12–7. doi: 10.1053/jcrc.2000.0150012. [DOI] [PubMed] [Google Scholar]
- 4.Shahidi NT. A review of the chemistry, biological action, and clinical applications of anabolic-androgenic steroids. Clin Ther. 2001;23:1355–90. doi: 10.1016/s0149-2918(01)80114-4. [DOI] [PubMed] [Google Scholar]
- 5.Nieschlag E, Vorona E. Mechanisms in endocrinology: Medical consequences of doping with anabolic androgenic steroids: Effects on reproductive functions. Eur J Endocrinol. 2015;173:R47–58. doi: 10.1530/EJE-15-0080. [DOI] [PubMed] [Google Scholar]
- 6.Beaver KM, Vaughn MG, Delisi M, Wright JP. Anabolic-androgenic steroid use and involvement in violent behavior in a nationally representative sample of young adult males in the United States. Am J Public Health. 2008;98:2185–7. doi: 10.2105/AJPH.2008.137018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Piacentino D, Kotzalidis GD, Del Casale A, Aromatario MR, Pomara C, Girardi P, et al. Anabolic-androgenic steroid use and psychopathology in athletes. A systematic review. Curr Neuropharmacol. 2015;13:101–21. doi: 10.2174/1570159X13666141210222725. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Herlitz LC, Markowitz GS, Farris AB, Schwimmer JA, Stokes MB, Kunis C, et al. Development of focal segmental glomerulosclerosis after anabolic steroid abuse. J Am Soc Nephrol. 2010;21:163–72. doi: 10.1681/ASN.2009040450. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Hartgens F, Kuipers H. Effects of androgenic-anabolic steroids in athletes. Sports Med. 2004;34:513–54. doi: 10.2165/00007256-200434080-00003. [DOI] [PubMed] [Google Scholar]
- 10.Nieschlag E, Vorona E. Doping with anabolic androgenic steroids (AAS): Adverse effects on non-reproductive organs and functions. Rev Endocr Metab Disord. 2015;16:199–211. doi: 10.1007/s11154-015-9320-5. [DOI] [PubMed] [Google Scholar]
- 11.World Anti-Doping Agency. The World Anti-Doping Code Prohibited List. World Anti-Doping Agency; 2017. [Last accessed on 2018 Dec 10]. Available from: https://www.wada-ama.org/en/prohibited-list . [Google Scholar]
- 12.Hall RC, Hall RC. Abuse of supraphysiologic doses of anabolic steroids. South Med J. 2005;98:550–5. doi: 10.1097/01.SMJ.0000157531.04472.B2. [DOI] [PubMed] [Google Scholar]
- 13.Althobiti SD, Alqurashi NM, Alotaibi AS, Alharthi TF, Alswat KA. Prevalence, attitude, knowledge, and practice of anabolic androgenic steroid (AAS) use among gym participants. Mater Sociomed. 2018;30:49–52. doi: 10.5455/msm.2018.30.49-52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Sagoe D, Molde H, Andreassen CS, Torsheim T, Pallesen S. The global epidemiology of anabolic-androgenic steroid use: A meta-analysis and meta-regression analysis. Ann Epidemiol. 2014;24:383–98. doi: 10.1016/j.annepidem.2014.01.009. [DOI] [PubMed] [Google Scholar]
- 15.Perry PJ, Lund BC, Deninger MJ, Kutscher EC, Schneider J. Anabolic steroid use in weightlifters and bodybuilders: An internet survey of drug utilization. Clin J Sport Med. 2005;15:326–30. doi: 10.1097/01.jsm.0000180872.22426.bb. [DOI] [PubMed] [Google Scholar]
- 16.Jabari M, Al-Shehri H, Al-Faris A, Al-Sayed M, Algaeed F, Al-Sobaie N, et al. The prevalence of anabolic androgenic steroid use amongst athletes in Riyadh (Saudi arabia) Electron Physician. 2016;8:3343–7. doi: 10.19082/3343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Al Bishi KA, Afify A. Prevalence and awareness of anabolic androgenic steroids (AAS) among gymnasts in the Western Province of Riyadh, Saudi Arabia. Electron Physician. 2017;9:6050–7. doi: 10.19082/6050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Bahri A, Mahfouz MS, Marran NM, Dighriri YH, Alessa HS, Khwaji MO, et al. Prevalence and awareness of anabolic androgenic steroid use among male body builders in Jazan, Saudi Arabia. Trop J Pharm Res. 2017;16:1425–30. [Google Scholar]
- 19.Tahtamouni LH, Mustafa NH, Alfaouri AA, Hassan IM, Abdalla MY, Yasin SR, et al. Prevalence and risk factors for anabolic-androgenic steroid abuse among Jordanian collegiate students and athletes. Eur J Public Health. 2008;18:661–5. doi: 10.1093/eurpub/ckn062. [DOI] [PubMed] [Google Scholar]
- 20.Alsaeed I, Alabkal JR. Usage and perceptions of anabolic-androgenic steroids among male fitness centre attendees in Kuwait – A cross-sectional study. Subst Abuse Treat Prev Policy. 2015;10:33. doi: 10.1186/s13011-015-0030-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Al-Falasi O, Al-Dahmani K, Al-Eisaei K, Al-Ameri S, Al-Maskari F, Nagelkerke N, et al. Knowledge, attitude and practice of anabolic steroids use among gym users in Al-Ain district, United Arab Emirates. Open Sports Med J. 2008;2:75–81. [Google Scholar]
- 22.Baker JS, Graham MR, Davies B. Steroid and prescription medicine abuse in the health and fitness community: A regional study. Eur J Intern Med. 2006;17:479–84. doi: 10.1016/j.ejim.2006.04.010. [DOI] [PubMed] [Google Scholar]