

Abstract
Objective:
Research suggests that college is a risky period for changes in eating behavior and beliefs. Although social health determinants relate to health behavior changes, research has not explored subjective social status, one’s societal standing, in terms of eating expectancies among college students. The present study examined the emotion dysregulation in association between subjective social status and eating expectancies among college students.
Participants:
Participants were a diverse sample of 1,589 college students (80.4% females; Mage = 22.2 years, SD = 5.27) from an urban university.
Results:
Results showed a significant indirect association of subjective social status via emotion dysregulation in relation to expectancies of eating to help manage negative affect, to alleviate boredom, and to lead to feeling out of control.
Conclusion:
These findings provide evidence that college students with lower subjective social status may have a higher risk for dysregulated emotions, and consequently, expressing maladaptive eating expectancies.
Keywords: College, eating, emotion dysregulation, expectancies, subjective social status
Entering college is a significant life event which is consistently associated with changes in lifestyle and health behaviors.1,2 Among lifestyle behaviors, disordered eating has been found to increase within the first year of college2 and is highly prevalent on college campuses.3,4 For example, Eisenberg and colleges4 found that roughly 13.5% of female students and 3.6% of male students screen positive for clinically significant symptoms of disordered eating reflected through a broad range of concerns (eg, worry about losing control over eating, perceptions of thinness/fatness).4 Further, among college students, such disordered eating is associated with a host of negative consequences, including excessive weight gain,5 problematic substance use,6 and poorer psychological health.7
To better understand the nature of disordered eating, researchers have increasingly found merit in applying expectancy theory.8 Expectancy theory posits that expectancies reflect learned relations between behaviors and their consequences that become stored in memory and guide future behavioral choices.9 There are several distinct expectancies for eating that can vary both between and within individuals (eg, eating helps manage negative affect, eating alleviates boredom, and eating leads to feeling out of control).10 As such, two individuals may eat for different reasons, and one individual may eat for multiple types of reasons. Eating expectancies have been found to be associated with various clinically-relevant aspects of disordered eating (eg, binge eating, restricting).11 For example, among college students, expectancies of eating to help manage negative affect and expectancies of eating to alleviate boredom have been associated with eating in order to cope with aversive emotional states.12 Furthermore, Hohlstein and colleagues10 found that, among college students, expectancies of eating to help manage negative affect, expectancies of eating to alleviate boredom, and expectancies of eating to lead to feeling out of control were related to bulimic symptoms. Thus, enhancing efforts to understand eating expectancies may facilitate knowledge of disordered eating among college students.
Notably, there has been increased interest in better understanding how health behaviors are impacted by social determinants of health (eg, social interactions and relationships, economic factors).13 Of social determinants of health, subjective social status, a measure of one’s relative standing in society, has consistently been found to be related to health behavior and choices.14 For instance, subjective social status has emerged as a robust predictor of health status and such effects are not attributable to income and educational level.15,16 Yet, research examining subjective social status and eating behavior and processes is highly limited, particularly among college students. Of available work, one study found that experimentally induced perceptions of low subjective social status resulted in greater caloric intake.17 However, to our knowledge, there has been no empirical test of the relationship between subjective social status and eating expectancies among college students. Given the growing diversity among college campuses,18 in conjunction with the high prevalence of disordered eating among this population,4 there is need to empirically examine how subjective social status may relate to eating expectancies among college students.
Importantly, existing work has suggested that the link between subjective social status and health behaviors may be through psychological pathways.14 Specifically, there is a growing body of literature suggesting emotion dysregulation is one transdiagnostic (psychological) mechanism that may link subjective social status to various types of maladaptive health behaviors (eg, problematic eating, smoking).19–21 Emotion dysregulation reflects difficulties engaging a set of abilities wherein one can observe, understand, evaluate, and differentiate one’s emotions and subsequently access strategies to regulate emotions and control behavioral responses.22,23 Among college students, emotion dysregulation has consistently been found to be related to disordered eating19,20 as well as maladaptive eating expectancies.24
Theoretically, college students reporting lower subjective social status may experience more intense aversive emotional episodes.25 College students that can effectively regulate such distress may be able to maintain better control over their cognitive and behavioral responses.26 However, college students who have difficulties regulating such affective states may be more likely to take measures to escape or avoid such aversive states by engaging in eating behavior.26,27 As a result, college students may be more apt to adopt maladaptive cognitive expectancies related to the function and control of their eating.28,29 Indeed, because of such emotion dysregulation, these individuals may experience greater expectancies of eating to help manage negative affect, expectancies of eating to alleviate boredom, and expectancies that eating will lead to feeling out of control.24 Yet, to our knowledge, there has not been an empirical test of an emotion dysregulation model for subjective social status and eating expectancies relations among college students. This lack of research is surprising given that the proposed model may shed light on clinically relevant psychological pathways involved in disordered eating (eg, binge eating). For example, the current model may provide clinical guidance and suggest future implications of targeting emotion dysregulation specifically for college students experiencing maladaptive eating expectancies because of lower perceived social status.
The current study tested the hypothesis that a clinically-important social determinant of health factor, subjective social status, would exert an indirect effect on eating expectancies via emotion dysregulation among college students (see Figure 1). It was hypothesized that higher subjective social status would be negatively associated with emotion dysregulation, which in turn, would be related to expectancies of eating: to help manage negative affect, to alleviate boredom, and to lead to feeling out of control. It was further hypothesized that any effect of subjective social status on eating expectancies via emotion dysregulation would be evident over and above variance accounted for by theoretically-relevant covariates, including gender, race/ethnicity, and negative affectivity.30–32
Figure 1.
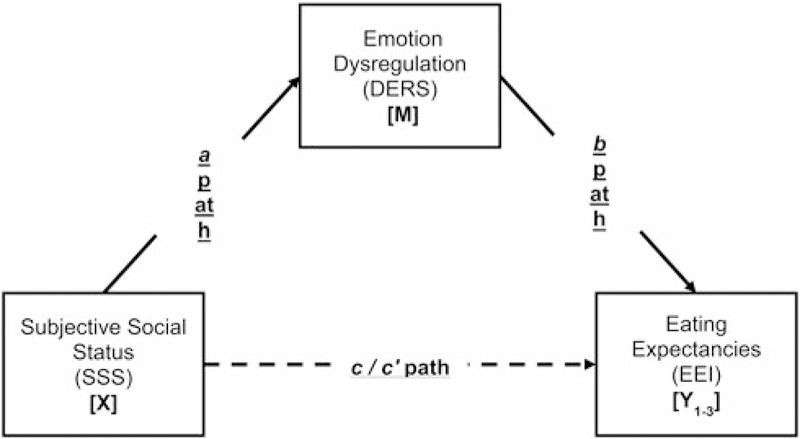
Conceptual model. Note: a path = Effect of X on M; b paths = Effect of M on Yi; c paths = Total effect of X on Yi; c’ paths = Direct effect of X on Yi controlling for M. Three separate paths were conducted (Y1–3) with the predictor (X). Covariates included gender, race/ethnicity, and negative affectivity.
Methods
Participants
Participants were 1,589 college students (80.4% females; Mage = 22.2 years, SD = 5.27). The sample was racially/ethnically diverse and representative of the university’s student body: 29.6% Hispanic (n = 470), 27.2% Asian/Pacific Islander (n = 433), 23.8% White (non-Hispanic; n = 378), 14.2% Black (non-Hispanic; n = 226), and 4.7% other race/ethnicities (n = 74).
Measures
Demographic questionnaire
A demographic questionnaire was used to collect data, including gender, race/ethnicity, and age for descriptive purposes. Gender and race/ethnicity were utilized as covariates in the current study.
Positive and negative affect schedule (PANAS)33
The PANAS is a self-report measure that assesses the extent to which participants experienced 20 different feelings and emotions (eg, distressed, excited). Items are rated on a 5-point Likert-type scale ranging from 1 (Very slightly or not at all) to 5 (Extremely). The measure yields two factors, negative and positive affectivity. The PANAS has demonstrated strong psychometric properties in clinical and nonclinical samples.33,34 The PANAS negative affectivity subscale (PANAS-NA) was utilized in the current study (α = .90).
Subjective social status (SSS)14
Subjective social status was assessed with the community version of the MacArthur Scale.14 Participants were presented with a picture of a 10-rung ladder. Respondents were asked to rate from 1 (worst) to 10 (best) where they stand in the community, relative to others, where higher rungs indicate higher status (ie, more money, more education, and better jobs). This measure has demonstrated adequate reliability and validity in previous work35–37 and has been utilized among racially diverse U.S. samples38 adolescents,39 young adults,40 and college students.41
Difficulties in emotion regulation scale (DERS)22
The DERS is a 36-item self-report measure that assesses how often respondents experience dysregulated emotional states on a 5-pont Likert-type scale from 1 (almost never) to 5 (almost always). The DERS assesses six subscale facets including Non-Acceptance of Emotional Responses, Difficulties Engaging in Goal-Directed Behavior, Impulse Control Difficulties, Lack of Emotional Awareness, Access to Emotion Regulation Strategies, and Lack of Emotional Clarity which can be summed to create a global index of emotion dysregulation (possible range = 36–180). The DERS has strong psychometric properties.22,27 Internal consistency for the DERS total score was excellent (Cronbach’s α = .93).
Eating expectancy inventory (EEI)10
The EEI is a 34-item self-report measure used to assess the cognitive expectancies of eating. Specifically, the EEI assesses 5 subscale facets: eating helps manage negative affect; eating is pleasurable and useful as a reward; eating leads to feeling out of control; eating enhances cognitive competence; and eating alleviates boredom. Respondents were asked to rate on a 7-point Likert-type scale the degree to which they 1 (completely disagree) to 7 (completely agree) for each item. The EEI subscales have demonstrated sound psychometric properties among college, clinical, and adolescent samples.10,42 Eating helps manage negative affect (Cronbach’s α = .95), eating alleviates boredom (Cronbach’s α = .73), and eating leads to feeling out of control (Cronbach’s α = .80) were utilized in the current study.
Procedure
The present sample included university students who participated in a study conducted at a large, south-western university. Participants were recruited via flyers and university website postings. Participants received extra credit towards their psychology course as compensation. Exclusion criteria included being younger than age 18 and nonproficiency in English (to ensure comprehension of study questions). All participants provided informed consent which was completed over the internet before proceeding to the online self-report survey. Quality assurance questions were placed throughout the survey to protect against sporadic responding and ensure the integrity of the data. Identifying information was not retained for each participant; there was no link between each participant’s identity and study responses. This study protocol was approved by the Institutional Review Board where the study took place. The data were collected from September 2015 through May 2017.
Analytic strategy
Sample descriptive statistics and zero-order correlations among study variables were examined. Primary analyses included three regression-based path models. In all models, covariates included gender, race/ethnicity, and negative affectivity. Subjective social status served as the predictor, and emotion dysregulation served as the indirect variable in all models (y1–3): (1) expectancies of eating to help manage negative affect, (2) expectancies of eating to alleviate boredom, and (3) expectancies of eating to lead to feeling out of control; see Figure 1.
Analyses were conducted using bootstrapping techniques through PROCESS, a conditional modeling program that utilizes an ordinary least squares-based path analytical framework to test for both direct and indirect effects.43 An indirect effect is the product of path a (the association between the predictor [x] and the proposed explanatory variable [m]) and path b (the association between the proposed mediator variable [m] and the dependent variable [yi] controlling for x). As recommended, the confidence intervals around the point-estimate were subjected to 10,000 bootstrap re-samplings and 95-percent confidence intervals (CIs) were estimated.44–46 The effects can be assumed to be statistically significant if the CIs around their product do not include zero.45,47 To further strengthen the specificity and interpretation of results, alternative models were tested by reversing the pro-posed mediator for each of the three models.44
Results
Bi-variate relations
Zero-order correlations among all study variables are presented in Table 1. Subjective social status was negatively correlated with emotion dysregulation (r = –.147, p<.001) and expectancies of eating to lead to feeling out of control (r = –.062, p<.05). Emotion dysregulation was positively correlated with all criterion variables (r’s = .210–.326, p’s<.001).
Table 1.
Descriptive statistics and bivariate correlations between study variables (N = 1,589).
| Variable | Mean/n (SD/%) | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
|---|---|---|---|---|---|---|---|---|---|
| 1. Gendera | 1,278 (80.4%) | − | |||||||
| 2. Race/Ethnicitya | 378 (23.8%) | .037 | − | ||||||
| 3. Negative Affectivitya | 21.09 (7.83) | −.011 | −.006 | − | |||||
| 4. Subjective Social Statusb | 5.79 (1.76) | −.027 | .033 | −.123*** | − | ||||
| 5. Emotion Dysregulationc | 85.94 (23.29) | −.018 | .044 | .614*** | −.147*** | − | |||
| 6. Eating Expectancies-Negative Affectd | 57.96 (24.15) | .008 | .030 | .259*** | −.024 | .326*** | − | ||
| 7. Eating Expectancies-Boredomd | 16.36 (5.62) | .057* | .014 | .153*** | −.040 | .210*** | .607*** | − | |
| 8. Eating Expectancies-Controld | 11.55 (5.86) | .001 | −.004 | .246*** | −.062* | .344*** | .467*** | .270*** | − |
Note.
p<.001
p<.05.
Covariate
Predictor
Mediator
Criterion
Gender: % listed as females (Coded: 0 = male and 1= female); Race/Ethnicity: % listed as White (non-Hispanic); Negative Affectivity = Positive and Negative Affect Schedule-Negative Affect subscale33; Subjective Social Status = Subjective Social Status Scale-Community Item14; Emotion Dysregulation = Difficulties with Emotion Regulation Scale22; Eating Expectancies-Negative Affect = Eating Expectancy Inventory-Eating Helps Manage Negative Affect subscale10; Eating Expectancies-Boredom = Eating Expectancy Inventory-Eating Alleviates Boredom subscale10; Eating Expectancies-Control = Eating Expectancy Inventory-Eating Leads to Feeling out of Control subscale.10
Indirect effects
Regression results are presented in Table 2. The total effects model with subjective social status and covariates in the model was significant (R2 = .07, F[4, 1584] = 28.97, p < . 001) for expectancies of eating to help manage negative affect. The full model with emotion dysregulation accounted for a significant amount of variance (R2 = .11, F[5, 1583] = 40.36, p < . 001). The test of the indirect effect indicated that subjective social status was associated with expectancies of eating to help manage negative affect indirectly through the effect of emotion dysregulation (a*b = –0.277, SE = 0.084, CI95% = –0.459, –0.129).
Table 2.
Indirect effect of subjective social status on eating expectancies subscales via emotion dysregulation.
| Y | Path | R2 | b | SE | t | p | CI (l) | CI (u) |
|---|---|---|---|---|---|---|---|---|
| 1 | SSS → DERS (a) | .385 | −0.987 | 0.262 | −3.76 | <.001 | −1.502 | −0.473 |
| DERS → EEI-NA (b) | .113 | 0.280 | 0.031 | 8.95 | <.001 | 0.219 | 0.342 | |
| SSS → EEI-NA (c’) | 0.380 | 0.328 | 1.16 | .248 | −0.264 | 1.024 | ||
| SSS → EEI-NA (c) | .068 | 0.103 | 0.335 | 0.31 | .758 | −0.554 | 0.760 | |
| SSS → DERS → EEI-NA (a*b) | −0.277 | 0.084 | −0.459 | −0.129 | ||||
| 2 | DERS → EEI-BOR (b) | .049 | 0.045 | 0.008 | 5.94 | <.001 | 0.030 | 0.060 |
| SSS→ EEI-BOR (c’) | −0.020 | 0.079 | −0.26 | .799 | −0.175 | 0.135 | ||
| SSS → EEI-BOR (c) | .027 | −0.064 | 0.080 | −0.81 | .419 | −0.221 | 0.092 | |
| SSS → DERS → EEI-BOR (a*b) | −0.044 | 0.015 | −0.079 | −0.020 | ||||
| 3 | DERS → EEI-CON (b) | .121 | 0.078 | 0.008 | 10.36 | <.001 | 0.064 | 0.093 |
| SSS → EEI-CON (c’) | −0.029 | 0.079 | −0.37 | .712 | −0.185 | 0.126 | ||
| SSS → EEI-CON (c) | .061 | −0.107 | 0.082 | −1.31 | .191 | −0.267 | 0.053 | |
| SSS → DERS → EEI-CON (a*b) | −0.077 | 0.023 | −0.126 | −0.035 |
Note. Path a is equal in all cases Y1−3; therefore, it presented only once to avoid redundancies. N for analyses is 1,589 cases. The standard error and 95% CI for the indirect effects (a*b) are obtained through bootstrapping with 10,000 resamples. a path = Effect of X on M; b paths = Effect of M on Yi; c’ paths = Direct effect of X on Yi controlling for M; c paths = Total effect of X on Yi. SSS = Subjective Social Status-Community14; DERS = Difficulties with Emotion Regulation Scale22; Eating Expectancies-Negative Affect = Eating Expectancy Inventory-Eating Helps Manage Negative Affect subscale10; Eating Expectancies-Boredom = Eating Expectancy Inventory-Eating Alleviates Boredom subscale10; Eating Expectancies-Control = Eating Expectancy Inventory-Eating Leads to Feeling out of Control subscale.10 Covariates included gender, race/ethnicity, and negative affectivity.
For expectancies of eating to alleviate boredom, the total effect model was significant (R2 = .03, F[4, 1584] = 11.15, p < .001). The full model with emotion dysregulation was also significant (R2 = .05, F[5, 1583] = 16.18, p < .001). The test of the indirect effect indicated that subjective social status was associated with expectancies of eating to alleviate boredom, which occurred indirectly through the greater levels of emotion dysregulation (a b = –0.044, SE = 0.015, CI95% =–0.079,–0.020).
In terms of expectancies of eating to lead to feeling out of control, the total effects model accounted for significant variance (R2 = .06, F[4, 1584] = 25.88, p < .001). The model with emotion dysregulation accounted for additional variance for eating leads to feeling out of control (R2=0.12, F[5, 1583] =43.54, p<.001). Results indicated that, in the test of the indirect effect through emotion dysregulation, subjective social status was associated with expectancies of eating to lead to feeling out of control (a*b=–0.077, SE=–0.023, CI95%= –0.126, –0.035).
Specificity analyses
To further strengthen the interpretation of results, alternative models were tested by reversing the proposed mediator for each of the three models;44 specifically, emotion dysregulation was the predictor, subjective social status was the indirect variable, and all three criterion variables remained the same. The indirect effects of the alternate models were nonsignificant for expectancies of eating to help manage negative affect (a*b = 0.003, SE = –0.003, CI99% = –0.011, 0.002), expectancies of eating to alleviate boredom (a*b = 0.001, SE = 0.001, CI99% = –0.001, 0.002), and expectancies of eating to lead to feeling out of control (a*b = 0.001, SE = 0.001, CI99% = –0.001, 0.002).
Discussion
The current study examined the role of emotion dysregulation in the relation between subjective social status and eating expectancies among a large and highly racially/ethnically diverse sample of college students. As hypothesized, subjective social status yielded a significant indirect effect through emotion dysregulation on eating expectancies. Specifically, lower reported subjective social status was related to increased emotion dysregulation, which in turn, was related to greater expectancies of eating to: help manage negative affect, to alleviate boredom, and to lead to feeling out of control. The observed indirect effects were evident after adjusting for gender, race/ethnicity, and negative affectivity. Furthermore, the tested competing models were nonsignificant, which provides additional empirical support for the proposed model. The current findings are broadly in line with past work high-lighting the association of emotion dysregulation with subjective social status48 and eating expectancies24 and uniquely extends past work to indicate that emotion dysregulation may play an important mechanistic role in the association between subjective social status and eating expectancies among college students.
It is interesting to note that, although there is theoretical and past empirical support for an association between subjective social status and eating behav-iors,17 the direct and total association for subjective social status and eating expectancies were nonsignificant in the present study. This finding is consistent with at least one other study of college students24 and suggests that lower subjective social status may by itself not “predispose” college students to adopt mal-adaptive eating expectancies among this population. Rather, subjective social status “works through” emotion dysregulation in terms of maladaptive eating expectancies.
Clinically, the present investigation may serve to conceptually inform the development of specialized intervention strategies including targeted weight management or eating education programs for college students with lower reported subjective social status. Specifically, it may be beneficial to understand and clinically address emotion dysregulation to enhance psychological flexibility related to maladaptive eating expectancies (eg, “Eating is a way to vent my anger”) and ultimately facilitate change in eating behaviors. Cognitive-behavioral therapy may be one promising approach to target emotion dysregulation. For example, Fairburn and colleagues49 have proposed a transdiagnostic cognitive-behavioral intervention to target dysfunctional mood modulatory behavior to improve eating behavior and disorders. Future work may benefit from exploring how such therapeutic tac-tics may reduce emotion dysregulation among a non-clinical eating disorder college student sample to reduce maladaptive expectancies of eating and perhaps facilitate improvements in weight management and eating behaviors.
There are several limitations to consider in the current study. First, the data were cross-sectional in nature, and therefore, did not permit testing of temporal sequencing. Future work is needed to determine the directional effects of these relations using prospective designs. Second, there is the possibility that the noted relations may be observed, in part, because of shared method variance. Future studies may benefit from implementing a multi-method assessment approach to cross-index the nature of the relations observed in the current study. Third, although there was a significant indirect effect of subjective social status on eating expectancies through emotion dysregulation, the current study investigated only a single, yet novel, underlying mechanism. Future work should therefore focus on additional explanatory variables that may underlie this association, including other transdiagnostic factors (eg, anxiety sensitivity, distress intolerance, anhedonia). Fourth, 80.4% of the sample were female college students. Future studies may benefit from sampling a larger pool of males from the student population to ensure generalizability of the results to college students. Finally, the current study did not screen for the presence of eating disorders or measure indices of obesity (eg, body mass index [BMI]). Thus, future work may benefit from examining the observed associations as they relate to clinic-ally significant disordered eating, BMI, and obesity.
Overall, the current study provides novel empirical support for the role of emotion dysregulation in the relation between subjective social status and several maladaptive eating expectancies among college students. Future work is needed to replicate and extend the present findings using longitudinal methodology and utilizing alternative analytic tactics including Structural Equation Modeling.
Acknowledgments
Funding
No funding was used to support this research and/or the preparation of the manuscript.
Footnotes
Conflict of interest disclosure
The authors have no conflicts of interest to report. The authors confirm that the research presented in this article met the ethical guidelines, including adherence to the legal requirements, of United States and received approval from the Institutional Review Boards of the University of Houston and University of Texas.
Data availability statement
A dataset is available upon request.
References
- 1.Delinsky SS, Wilson GT. Weight gain, dietary restraint, and disordered eating in the freshman year of college. Eat Behav 2008;9(1):82–90. [DOI] [PubMed] [Google Scholar]
- 2.Eleanor S, Jacquie L, Peter G, Jean R, Megan F, Margo B. Eating habits associated with body weight gain in female university students: a UK-based study of Slimming World members. Br Food J 2017; 119(12):2571–2582. [Google Scholar]
- 3.Kelly-Weeder S. Binge drinking and disordered eating in college students. J Am Acad Nurse Pract 2011; 23(1):33–41. [DOI] [PubMed] [Google Scholar]
- 4.Eisenberg D, Nicklett EJ, Roeder K, Kirz NE. Eating disorder symptoms among college students: prevalence, persistence, correlates, and treatment-seeking. J Am Coll Health 2011;59(8):700–707. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Hunt TK, Forbush KT, Hagan KE, Chapa DAN. Do emotion regulation difficulties when upset influence the association between dietary restraint and weight gain among college students? Appetite 2017;114: 101–109. [DOI] [PubMed] [Google Scholar]
- 6.Dunn EC, Larimer ME, Neighbors C. Alcohol and drug-related negative consequences in college students with bulimia nervosa and binge eating disorder. Int J Eat Disord 2002;32(2):171–178. [DOI] [PubMed] [Google Scholar]
- 7.Masuda A, Price M, Anderson PL, Wendell JW. Disordered eating-related cognition and psychological flexibility as predictors of psychological health among college students. Behav Modif 2010;34(1):3–15. [DOI] [PubMed] [Google Scholar]
- 8.Odgen J. The Psychology of Eating Carlton, Victoria: Blackwell Publishing Ltd; 2003. [Google Scholar]
- 9.Fischer S, Smith GT, Anderson KG, Flory K. Expectancy influences the operation of personality on behavior. Psychol Addict Behav 2003;17(2):108–114. [DOI] [PubMed] [Google Scholar]
- 10.Hohlstein LA, Smith GT, Atlas JG. An application of expectancy theory to eating disorders: development and validation of measures of eating and dieting expectancies. Psychol Assessment 1998;10(1):49–58. [Google Scholar]
- 11.Smith GT, Simmons JR, Flory K, Annus AM, Hill KK. Thinness and eating expectancies predict subsequent binge-eating and purging behavior among adolescent girls. J Abnorm Psychol 2007;116(1):188–197. [DOI] [PubMed] [Google Scholar]
- 12.Hennegan JM, Loxton NJ, Mattar A. Great expectations. Eating expectancies as mediators of reinforcement sensitivity and eating. Appetite 2013; 71(Supplement C):81–88. [DOI] [PubMed] [Google Scholar]
- 13.Commission on Social Determinants of Health C. Closing the Gap in a Generation: Health Equity through Action on the Social Determinants of Health Geneva: World Health Organization; 2008. [DOI] [PubMed] [Google Scholar]
- 14.Adler NE. Health disparities through a psychological lens. Am Psychol 2009;64(8):663–673. [DOI] [PubMed] [Google Scholar]
- 15.Singh-Manoux A, Marmot MG, Adler NE. Does subjective social status predict health and change in health status better than objective status? Psychosom Med 2005;67(6):855–861. [DOI] [PubMed] [Google Scholar]
- 16.Adler NE, Epel ES, Castellazzo G, Ickovics JR. Relationship of subjective and objective social status with psychological and physiological functioning: preliminary data in healthy white women. Health Psychol 2000;19(6):586–592. [DOI] [PubMed] [Google Scholar]
- 17.Cardel MI, Johnson SL, Beck J, et al. The effects of experimentally manipulated social status on acute eating behavior: a randomized, crossover pilot study. Physiol Behav 2016;162(Supplement C):93–101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.U.S. Department of Education NCfES. Digest of Education Statistics 2016; https://nces.ed.gov/fastfacts/display.asp?id=98, 2018.
- 19.Ambwani S, Slane JD, Thomas KM, Hopwood CJ, Grilo CM. Interpersonal dysfunction and affect-regulation difficulties in disordered eating among men and women. Eat Behav 2014;15(4):550–554. [DOI] [PubMed] [Google Scholar]
- 20.Muehlenkamp JJ, Peat CM, Claes L, Smits D. Self-injury and disordered eating: expressing emotion dysregulation through the body. Suicide Life Threat Behav 2012;42(4):416–425. [DOI] [PubMed] [Google Scholar]
- 21.Kauffman BY, Farris SG, Alfano CA, Zvolensky MJ. Emotion dysregulation explains the relation between insomnia symptoms and negative reinforcement smoking cognitions among daily smokers. Addict Behav 2017;72:33–40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Gratz KL, Roemer L. Multidimensional assessment of emotion regulation and dysregulation: development, factor structure, and initial validation of the Difficulties in Emotion Regulation Scale. J Psychopathol Behav Assess 2004;26(1):41–54. [Google Scholar]
- 23.Tull MT, Aldao A. Editorial overview: new directions in the science of emotion regulation. Curr Opin Psychol 2015;3:iv–ix. [Google Scholar]
- 24.Kauffman BY, Bakhshaie J, Lam H, Alfano C, Zvolenksy MJ. Insomnia and eating expectancies among college students: the role of emotion dysregulation. Cognit Behav Ther 2018. doi: 10.1080/16506073.2018.1466910. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Johns M, Inzlicht M, Schmader T. Stereotype threat and executive resource depletion: examining the influence of emotion regulation. J Exp Psychol Gen 2008; 137(4):691–705. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Evers C, Marijn Stok F, de Ridder DTD. Feeding Your Feelings: emotion regulation Strategies and Emotional Eating. Pers Soc Psychol Bull 2010;36(6): 792–804. [DOI] [PubMed] [Google Scholar]
- 27.Whiteside U, Chen E, Neighbors C, Hunter D, Lo T, Larimer M. Difficulties regulating emotions: do binge eaters have fewer strategies to modulate and tolerate negative affect? Eat Behav 2007;8(2):162–169. [DOI] [PubMed] [Google Scholar]
- 28.Aspen V, Darcy AM, Lock J. A review of attention biases in women with eating disorders. Cogn Emot 2013;27(5):820–838. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Kittel R, Brauhardt A, Hilbert A. Cognitive and emotional functioning in binge-eating disorder: a systematic review. Int J Eat Disord 2015;48(6):535–554. [DOI] [PubMed] [Google Scholar]
- 30.Croll J, Neumark-Sztainer D, Story M, Ireland M. Prevalence and risk and protective factors related to disordered eating behaviors among adolescents: relationship to gender and ethnicity. J Adolesc Health 2002;31(2):166–175. [DOI] [PubMed] [Google Scholar]
- 31.Lee-Winn AE, Reinblatt SP, Mojtabai R, Mendelson T. Gender and racial/ethnic differences in binge eating symptoms in a nationally representative sample of adolescents in the United States. Eat Behav 2016;22: 27–33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Haedt-Matt AA, Keel PK. Revisiting the affect regulation model of binge eating: a meta-analysis of studies using ecological momentary assessment. Psychol Bull 2011;137(4):660–681. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Watson D, Clark LA, Tellegen A. Development and validation of brief measures of positive and negative affect: the PANAS scales. J Pers Soc Psychol 1988; 54(6):1063–1070. [DOI] [PubMed] [Google Scholar]
- 34.Watson D. Emotions and social behavior, Mood and Temperament Guilford Press; 2000. [Google Scholar]
- 35.Franzini L, Fernandez-Esquer ME. The association of subjective social status and health in low-income Mexican-origin individuals in Texas. Soc Sci Med 2006;63(3):788–804. [DOI] [PubMed] [Google Scholar]
- 36.Ostrove JM, Adler NE, Kuppermann M, Washington AE. Objective and subjective assessments of socioeconomic status and their relationship to self-rated health in an ethnically diverse sample of pregnant women. Health Psychol 2000;19(6):613–618. [DOI] [PubMed] [Google Scholar]
- 37.Reitzel LR, Kendzor DE, Cao Y, Businelle MS. Subjective social status predicts quit-day abstinence among homeless smokers. Am J Health Promot 2014; 29(1):43–45. [DOI] [PubMed] [Google Scholar]
- 38.Adler N, Singh-Manoux A, Schwartz J, Stewart J, Matthews K, Marmot MG. Social status and health: a comparison of British civil servants in Whitehall-II with European- and African-Americans in CARDIA. Soc Sci Med 2008;66(5):1034–1045. [DOI] [PubMed] [Google Scholar]
- 39.Goodman E, Adler NE, Kawachi I, Frazier AL, Huang B, Colditz GA. Adolescents’ perceptions of social status: development and evaluation of a new indicator. Pediatrics 2001;108(2):E31. [DOI] [PubMed] [Google Scholar]
- 40.Karvonen S, Rahkonen O. Subjective social status and health in young people. Sociol Health Illn 2011;33(3): 372–383. [DOI] [PubMed] [Google Scholar]
- 41.Zorotovich J, Johnson EI, Linn R. Subjective social status and positive indicators of well-being among emerging adult college students. Coll Student J 2016; 50(4):624–635. [Google Scholar]
- 42.Simmons JR, Smith GT, Hill KK. Validation of eating and dieting expectancy measures in two adolescent samples. Int J Eat Disord 2002;31(4):461–473. [DOI] [PubMed] [Google Scholar]
- 43.Hayes AF. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach. Methodology in the Social Sciences New York, NY: The Guilford Press; 2013. [Google Scholar]
- 44.Preacher KJ, Hayes AF. SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behav Res Methods Instrum Comput 2004;36(4): 717–731. [DOI] [PubMed] [Google Scholar]
- 45.Preacher KJ, Hayes AF. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav Res Methods 2008;40(3):879–891. [DOI] [PubMed] [Google Scholar]
- 46.Hayes AF. Beyond Baron and Kenny: statistical mediation analysis in the new millennium. Commun Monogr 2009;76(4):408–420. [Google Scholar]
- 47.Zhao X, Lynch JG, Chen Q. Reconsidering Baron and Kenny: myths and truths about mediation analysis. J Consum Res 2010;37(2):197–206. [Google Scholar]
- 48.Zvolensky MJ, Paulus DJ, Bakhshaie J, et al. Subjective social status and anxiety and depressive symptoms and disorders among low income latinos in primary care: the role of emotion dysregulation. Cogn Ther Res 2017;41(5):686–698. [Google Scholar]
- 49.Fairburn CG, Cooper Z, Shafran R. Cognitive behaviour therapy for eating disorders: a “transdiagnostic” theory and treatment. Behav Res Ther 2003;41(5): 509–528. [DOI] [PubMed] [Google Scholar]