

Abstract
Objectives:
We hypothesized that the additional activation of motor units (MU) and the elevation of metabolic energy turnover resulting from whole-body vibration (WBV) superimposed to high intensity resistance training on a smith machine persist after 6 weeks of training with progressively increasing loads and vibration frequencies.
Methods:
Two groups of healthy male subjects performed either 6 weeks of Resistive Vibration Exercise (RVE, squats and heel raises with WBV, n=13) or Resistive Exercise (RE using the same protocol, n=13). During the first (pre) and the last training session (post), we determined the oxygen uptake changes normalized to total training weight (∆V’O2/ttw) and the normalized MU activity from rectus femoris (squats) and gastrocnemius lateralis (heel raise) muscles filtered for vibration frequencies and harmonics (EMG/ttw).
Results:
At pre measurement, RVE induced higher EMG/ttw (squats) than RE alone (group effect, P=0.006). At post measurement, EMG/ttw was reduced (time effects between P=0.087 and P<0.001 for both groups and exercises). At pre and post measurement, ∆V’O2/ttw was higher during RVE than during RE (group effects between P=0.005 and P=0.099 for both exercises).
Conclusions:
RVE permanently elevated metabolic energy turnover, although the initially observed additional MU activity by RVE could not be preserved in the working musculature.
Keywords: Strength Training, Squats, Heel Raises, EMG, Spirometry
Introduction
The effects of whole-body vibration (WBV) on motor unit (MU) activity in leg muscles measured as EMG amplitude and on the metabolic energy turnover measured as the rate of respiratory oxygen uptake (V’O2) have been studied widely over the last approx. 18 years[1,2]. An acute exposure of WBV added to conventional resistive exercise (resistive vibration exercise, RVE) increases both the MU activity and the metabolic energy turnover more than resistive exercise (RE) alone[3-7]. However, positive long-term effects of RVE still seem to be diverse concerning its increased effectiveness compared to RE[8-12]. At least few studies used progressively increasing vibration frequencies and training loads[8-12] to minimize potential early undesirable adaptation processes.
The additional activation of motor units during RVE in comparison to RE alone was only shown in subjects, who were not regularly exposed to WBV[5,6,13]. In addition, it could be shown that WBV on side-alternating vibration platforms – as performed in our current study – compared to synchronous vibrations leads to higher neuromuscular activity[5] and therefore, may result in larger training effects. However, Rosenberger et al.[13] demonstrated that after only 3 sessions within 5 days of daily squatting, the significant additional MU activity declined and the difference between EMG amplitudes in RE and RVE was not significant anymore when using the same vibration frequency and the same training load throughout the training period. The additional activity of MU by WBV in comparison with mere resistance exercise was also abolished after a 9-weeks long training with free squats and additional progressively increased loads applied by a barbell performed with and without WBV on a side-alternating platform at frequencies increased from 20 Hz to 25 Hz[8]. Frequencies higher than 25 Hz were not applied because the subjects showed problems with performing the training protocol[8]. The authors of this study[8] reject the hypothesis that WBV could optimize resistance training by further increasing neuromuscular responses. In our current study, the vibration frequency was progressively increased from 20 to 40 Hz on a side-alternating platform, which became possible by transferring the squatting on a smith machine, which facilitates the control of body posture because rails control the motion of weights. To our knowledge, 40 Hz is the highest frequency ever used in combination with resistance training on a side-alternating platform.
Thus, assuming a proper vibration-reducing body posture, e.g. through flexed legs and body weight shifted to the forefoot, the vibration transmission from the feet to the trunk and head can be reduced[14-16]. Damping of vibration along the vertical body was shown as a decline of vibration acceleration with increasing distance from the vibration plate[13,15]. This damping reduces the risk of damaging organs in the trunk and head[1,17,18] being less resistant to mechanical stresses than e.g. muscle or bone. On the other hand, damping reduces the mechanical stimulus to proximal muscles located at higher distance from the vibration plate. In conjunction with the distance-dependent effect, Rosenberger et al.[19] found additional training effects of RVE over RE only on ankle plantar flexor muscle cross-sectional area, isometric ankle plantar flexion force, and drop jump contact time (reactive jump where the calf muscles produce the main force). Therefore, in terms of MU activity of the legs, one would assume that the lower leg muscles are more prone to become positively affected than the upper leg muscles, since they are closer to the vibration platform.
It is also known that the additional mechanical stimulus of WBV leads to an acute enhanced energy turnover indicated by an increased oxygen uptake[3,7,20]. This effect becomes stronger with increasing vibration frequency, vibration amplitude, and additional training load[3,7,21,22]. However, RE with additional loading of only 40 % body weight was not enough to show a greater oxygen uptake than squatting without additional loading on a vibration platform[3], whereas RE with much higher additional loading (70% of the One-Repetition-Maximum (1RM)) was necessary to exceed the oxygen uptake compared to squatting without additional loading on a vibration platform[3,23]. This shows that the additional mechanical stimulus of WBV in combination with squatting already is a potent acute enhancer of oxygen uptake levels. However, it is not known, whether the increase in metabolic energy turnover by WBV during resistive exercise persists after long-term training or the elevation of energy turnover between RVE and RE - like the activity of motor units[13] - also declines to not significantly different levels in adaptation to the mechanical WBV stimulus.
In this study, we focused on the changes in muscle MU activity and respiratory oxygen uptake responses to WBV added to squat and heel raises exercises (RVE) in comparison with squat and heel raises exercises alone (RE). As a novel aspect, we applied progressive high intensity resistance training combined with progressively increased vibration frequencies from 20 to 40 Hz on a side-alternating vibration platform. We hypothesized that (1) when applied without previous adaptation (pilot study on acute effects of 20 Hz vs. 40 Hz vibration frequency), MU activity normalized to total training weight (current training load + current body weight, EMG/ttw) during acute RVE is higher at 40 Hz than at 20 Hz and (2) RVE pre and post 6 weeks of progressively increased RVE results in greater EMG/ttw and ∆V’O2/ttw than RE only. As an exploratory factor, we examined the potential increase in MU recruitment with increasing number of repetitions.
Material and methods
Experimental approach
This manuscript describes aspects tested in the “EVE” study (“Molecular and functional Effects of resistive Vibration Exercise”). A complete study overview of the EVE study has been published elsewhere[24].
A strength training study over 6 weeks was performed with two groups either training squats and heel raises alone (Resistive Exercise, RE) or performing the same training with an additional WBV stimulus (Resistive Vibration Exercise, RVE). Rosenberger et al.[13] found that an acute increase in EMG amplitude evoked by WBV decreased to insignificant levels after one week of training. Therefore, we aimed at minimizing this adaptation process to the vibration stimulus by increasing the RVE vibration frequency weekly from 20 to 40 Hz over the 6-weeks of training. This study was designed to validate stronger acute and long-term effects of strength training in RVE in comparison with RE alone by measuring (1) muscle activity with EMG of the m. rectus femoris and the m. gastrocnemius lateralis and (2) whole-body oxygen uptake with spirometry (V’O2). Therefore, EMG and V’O2 were measured in both groups during the initial training (pre) and after the 6 weeks of training at the final training (post).
Subjects
Twenty-six recreationally physically active (exercising not more than 2-3 times per week) healthy male subjects participated in this training study (RVE (n=13): age= 24.3±3.3 yrs., height= 1.79±0.05 m, body mass= 74.7±6.9 kg, maximum cycle ergometer test= 3.3±0.4 W/kg body weight; RE (n=13): age= 23.4±1.4 yrs., height= 1.79±0.05 m, body mass= 75.0±4.7 kg, maximum cycle ergometer test= 3.3±0.3 W/kg body weight[24]) after providing a written informed consent. The mean age, height, body mass and maximum cycle ergometer test values were not significantly different between the two groups. The study received an ethical approval from the Ethics Committee of the North Rhine Medical Association (Ärztekammer Nordrhein, vote no. 2010174), Düsseldorf, Germany. All subjects were aware that they could withdraw from the study at any time.
Exclusion criteria were smoking, regular medication, diabetes, participation in strength training during the past six months, and competitive sports. Subjects were stratified into two groups based on their maximum vertical jump height to ensure two groups with comparable neuromuscular fitness. A coin was then tossed to determine which group will perform RVE and which one RE.
Training protocol
Subjects trained 2-3 times per week for six weeks (week 1 and 2: 2 training sessions per week, week 3 to 6: 3 training sessions per week) resulting in a total of 16 training sessions. On each of the training days, all of the subjects performed two warm-up sets each followed by 1 minute rest. The warm-up consisted of 10 squats and 15 heel raises with 15 kg load. The subsequent main training program consisted of 2 sets of 8 squats and 12 heel raises with 1 minute break between the two exercises and each set. Finally, a third set of both exercises was performed with the maximum number of possible repetitions. The number of squats in the third set was used as an indicator to adjust the training load for both exercises for the next training session (less than 8 repetitions = decrease in training load by approx. 5%, 8 repetitions = same training load, more than 8 repetitions = increase in training load by approx. 5% or maximum 10 kg). The first loading was set to 80 % of the 1RM of the squat performance measured before the initial training session (RM tables used from[25]). The movement speed was controlled by a metronome with a 2 seconds eccentric and 2 seconds concentric phase for squats and a 1 second eccentric and 1 second concentric phase for heel raises and, if necessary, by the instructions of an operator. During squats, the subjects moved downward until the thigh was approximately horizontal to the ground and then upward until a knee flexion angle of approximately 5° was reached. Thus, full extension of the knee was avoided. In addition, during squatting, the subjects of RVE were instructed to shift their total weight to the forefoot as much as necessary to dampen the transmission of inconvenient or even painful vibrations going to the head. In consequence of this indispensable safety measure during squats in RVE, the plantar flexor muscles were loaded more than in RE performing ordinary squats. During squats in RE, the subjects were not instructed to load the forefoot similar to the RVE condition because this would be too difficult to control by the subjects and the operators and it would have caused more variability in the exercise performance and its potential effects. During heel raises, the RVE subjects were instructed to go down as much as possible for the downward movement while avoiding strong vibrations going to the head. Similarly, the RE subjects were instructed not to touch the platform with their heels for the downward movement. This was necessary since during WBV the normal stance or exercising with small knee angles as experienced during squatting and heel raises increases the likelihood of negative side effects and should be avoided[16]. In sum, through these instructions, it was the best possible way to truly compare RVE and RE. RVE subjects trained on a side-alternating vibration platform (Galileo Fitness, Novotec Medical GmbH, Pforzheim, Germany) at frequencies between 20-40 Hz and an amplitude of 3-4 mm (6-8 mm peak-to-peak). The manufacturer´s settings were used in our study and not verified by accelerometer. To our knowledge, the combination of 40 Hz vibration frequency on a side-alternating vibration platform with 6-8 mm peak-to-peak amplitude and high intensity resistance training is new for testing. The vibration frequency was gradually increased by 5 Hz per week with the last two weeks of training at 40 Hz. This approach (progressively increasing vibration frequency and training load) was done to avoid an early muscle activity decrease especially in the upper leg[13] and keep the subject’s training performance at its individual maximum during each training session. RE subjects performed the same training while the vibration platform was turned off. Both groups performed their training wearing gymnastic shoes.
Accuracy of loading
The training load for squats and heel raises was based on 80% of the 1RM of the squat exercise, resulting in 8 repetitions[25]. Due to organizational reasons we had to keep the same loads for the heel raises (knowing that the stimulus will be lighter), but increased the repetitions by 50% (to 12 repetitions) to counteract the lighter stimulus. Post-study analysis showed that the maximum repetitions of the 3rd set (mean over all sessions during the training period) for squats were approx. 75-77% of the 1RM (RE: 9.4±1.6 repetitions, RVE: 9.6±1.7 repetitions) and for heel raises approx. 60 % of the 1RM (RE: 20.8±4.0 repetitions, RVE: 20.5±5.8 repetitions) based on calculations by Baechle and Earle[25]. Thus, the loading for squats seemed to be in the range of a hypertrophic stimulus, whereas the loading for the heel raises showed the expected endurance focused stimulus.
Training compliance
In RE, ten subjects completed all of the 16 training sessions, whereas the remaining three subjects missed one training session. In RVE, four subjects completed all of the 16 training sessions, whereas the remaining nine subjects missed one training session.
Training loads
The training loads were comparable between the two groups at the first training session (RE: 81.5±7.7 kg, RVE: 75.2±6.5 kg) and significantly increased in both groups compared with their last training session (RE: 130.2±18.5 kg, RVE: 110.2±15.8 kg). There was a significantly lower increase in training load over the 6 weeks of training (time*group effect: P<0.05) in RVE (RE: 59.8±17.3 %, RVE: 46.9±19.0 %). Post-hoc analyses revealed that RE trained with significantly higher training loads compared to RVE from training sessions 13 to 16.
The acute effect of vibration frequency on muscle activity (pilot study on acute effects of 20 Hz vs. 40 Hz vibration frequency)
Subjects trained with 20 Hz vibration frequency during the initial training and with 40 Hz vibration frequency during the final training. Therefore, we conducted a pilot acute vibration frequency study to evaluate potential bias induced by training at different frequencies[26] by measuring motor unit activity using surface electromyography (EMG; identical procedure as stated in our “Measurement of surface EMG” paragraph). Six healthy male subjects were included into this study (age: 27.5±7.0 yrs.; height: 1.82±0.05 m; body mass: 78.7±7.6 kg), which was conducted in a cross-over design with regards to the two different vibration frequencies (20 Hz and 40 Hz). The two training sessions were separated by 1 week, and the training loads were 85±11 kg. The training conditions were identical to those applied in the long-term study with the only difference that the third set of both exercises was performed with only 8 squats or 12 heel raises (and not with maximum repetitions).
Measurement of surface EMG
Motor unit activity in muscles was measured using surface electromyography (EMG) with bipolar surface electrodes (Blue Sensor - N10A, Ambu GmbH, Bad Nauheim, Germany) of the left leg of all subjects for pre and post measurements and for the pilot study on acute effects of 20 Hz vs. 40 Hz vibration frequency. In detail, EMG was recorded from rectus femoris muscle, which was involved in knee extension during squats - and from gastrocnemius lateralis muscle performing plantar flexion during heel raises. In addition, the EMG of the m. rectus femoris is affected by the vibration transmitted via the patellar tendon, while the EMG of the m. gastrocnemius lateralis is affected by the vibration transmitted via the Achilles tendon. MU activity of the gastrocnemius lateralis and rectus femoris muscles were measured using the electrodes positioning recommendations of the European SENIAM-project (Surface Electromyography for the Non-Invasive Assessment of Muscles, www.SENIAM.org). The measurements were performed by trained personnel of the DLR with a mobile EMG device (TeleMyo 2400T G2, Noraxon USA Inc., Scottsdale, Arizona, USA) using the MyoResearch software (Version 1.07, Noraxon USA Inc., Scottsdale, Arizona, USA). Before applying the electrodes, the corresponding skin areas were shaved and cleaned with alcohol to reduce the resistance between the electrodes to less than 10 kΩ (on 5 occasions, the resistance was between 10 kΩ and 24 kΩ). The electrodes were connected by 6-cm cables to a preamplifier (Noraxon USA Inc., Scottsdale, AZ, USA) operating with a frequency band from 5 to 500 Hz. The distance between the two sensor areas of an electrode pair was 2 cm. To reduce the electromagnetically induced artifacts in the EMG signal, the preamplifiers and the 6-cm cables to the electrodes were tightly fixed to the skin using medical adhesive tape (Leukosilk, BSN medical GmbH, Hamburg, Germany).
To analyze EMG at periods of maximum muscle load, goniometers were used to find the lowest and the highest point of motion during squats and heel raises, respectively. One goniometer was therefore fixated at the lateral side of the left knee (1-axis goniometer, biovision, Wehrheim, Germany) and a second goniometer was fixated at the lateral side of the left ankle. In the follow-up study, comparing the effects of different WBV frequencies, the motion of the barbell was recorded with an analogue position encoder (AK Industries GmbH, Thal-Marmoutier, France) to detect the lowest and the highest point of motion during squats and heel raises, respectively. For the analysis of EMG, we incorporated the first 8 squats and the first 12 heel raises of all three sets meaning that additional repetitions in the third set (used to adjust the new training load) were not evaluated for EMG amplitudes.
The raw signals from the EMG and the goniometers were recorded at a sampling rate of 1500 Hz. All raw EMG signals from RE and RVE underwent an identical filtering and evaluation procedure using the software package “signal” (version 0.7-6) of R (version 3.1.3 in RStudio version 1.1.442, Inc, Boston, MA, USA). The signals of EMG were first filtered with a 1 Hz fourth order Butterworth high pass filter. Afterwards, seven 3rd order Butterworth stop filters were sequentially applied to erase ±2 Hz frequency bandwidths around the individually determined actual mid frequencies (MF=19.0 Hz or 19.5 Hz) and 2xMF, 3xMF, 4xMF, 6xMF, 8xMF, and 10xMF, which represent the precise vibration frequencies and their harmonics or sub harmonics. An example for the effectiveness of filtering is given in [Figures 1 and 2], which show the filtered and raw EMG during one squat cycle in the frequency and in the time domain, respectively. The signals of the goniometers or the position encoder were filtered using a 1 Hz fourth order Butterworth low pass filter before determining the time points of maximum knee flexion or plantar flexion. EMG amplitudes were calculated as root mean squares (µV) over a period of ±1.5 s for squats and ±1 s for heel raises around each peak point. Finally, EMG amplitudes were normalized to the total training weight (ttw), which was the sum of the current body weight and the current training load, to achieve a better comparability of data. The resulting values of EMG/ttw (µV/kg) represent the activity of the MUs in parts of the quadriceps or triceps surae muscles lifting a load corresponding to the current 80 % of 1RM.
Figure 1.
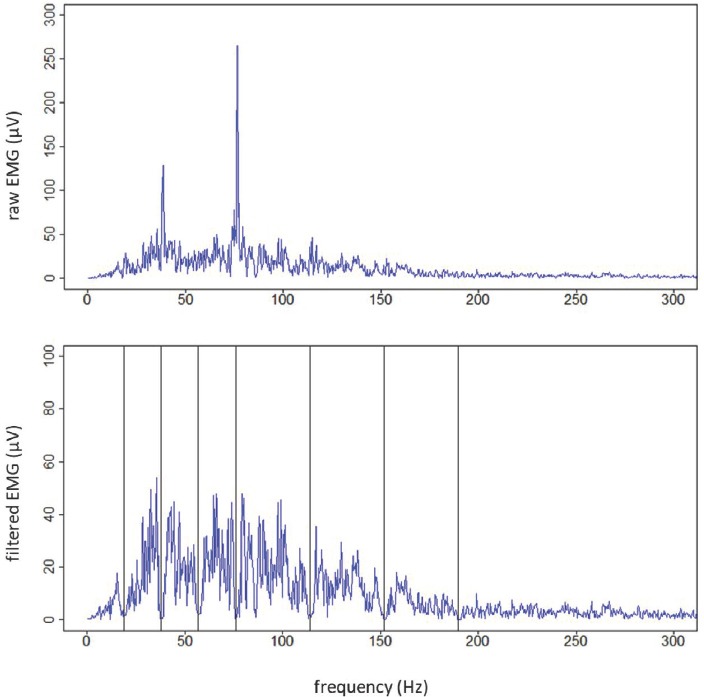
The frequency domain (FFT) of the EMG signal during a squat cycle. The upper graph shows the raw EMG signal - without filter -, the lower graph shows the filtered EMG signal with vertical lines indicating the mid frequencies of the bandwidth filters.
Figure 2.
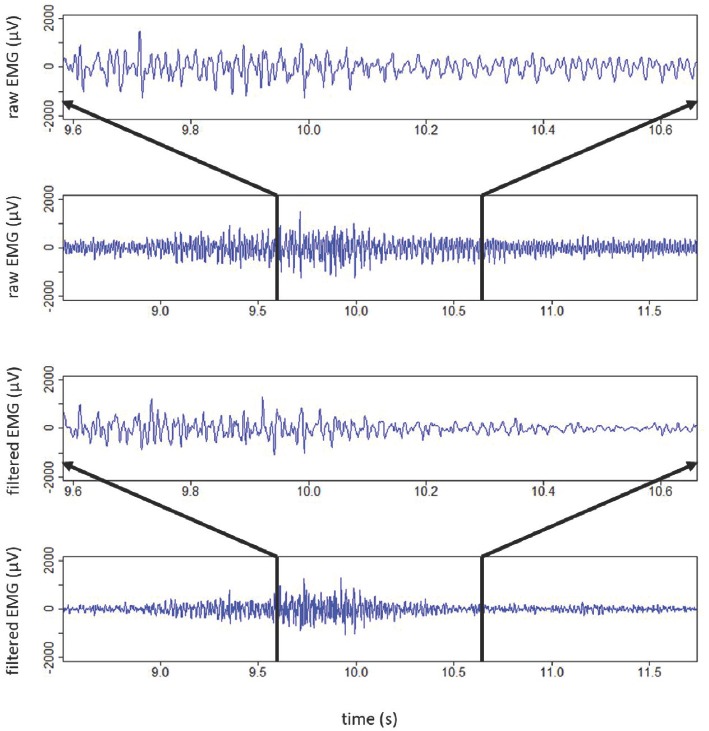
A record of an EMG signal in the time domain from the rectus femoris muscle during a single squat at 40 Hz WBV (upper two graphs show a zoomed in 1 s interval and a 3 s interval as raw EMG signal - without filter -, respectively, lower two graphs show a zoomed in 1 s interval and a 3 s interval with filter, respectively).
Measurement of normalized oxygen uptake
The specific oxygen uptake (V’O2 in ml/min) was measured pre and post training period using the mobile spirometry unit Oxycon Mobile (CareFusion Germany 234 GmbH, Hoechberg, Germany) throughout both training sessions. V’O2 was measured continuously (mean value every 5 seconds) during the 5-minute baseline (resting in a sitting position), the training intervention and the 10-minute recovery phase (resting in a sitting position). We calculated a baseline V’O2 as the mean V’O2 measured between the 2nd and the 5th minute of the baseline. The V’O2 for exercise was calculated as the mean of values throughout the whole workout time and the 1 minute of break time. Finally, ∆V’O2 was calculated and normalized to total training weight (∆V’O2/ttw, ttw = current body weight and training load) to achieve comparability of data between the two groups. Calculations were performed for each set of squats and heel raises as follows:

With this calculation, we were able to extrapolate the total oxygen uptake (during workout and 1 min break, where the body is in an oxygen debt) relative to actual workout times. However, we slightly underestimated the oxygen debt because oxygen debt was measured for 1 min only, which is too short for total metabolic recovery but was defined by the training regimen.
Statistical analyses
Statistical analysis was performed using the software SPSS 21 (IBM Corporation, Armonk, NY, USA). All variables were tested for normal distribution, skewness and kurtosis. If necessary, a box-cox transformation was applied. Total training weight (ttw), EMG/ttw for rectus femoris and gastrocnemius lateralis muscle and V’O2/ttw during squats and heel raise, respectively, were separately tested for main effects of the fixed factors time (pre and post), group (RE and RVE), set (1, 2, 3), and repetition (squats: 1 to 8; heel raises: 1 to 12) as well as the time*group effects using linear mixed models (LME) for repeated measurements. Since the factor set always turned out to be not significant, mean values of each repetition were calculated over the 3 sets and LME was calculated again with the fixed factors time, group, time*group and repetition. We examined the factor repetition to check for an increase in EMG/ttw as a potential compensation mechanism of fatigue, which did not occur in this study likely because of high percentage MU recruitment from the first contraction onwards. Furthermore, within the LME function, we applied univariate tests with Bonferroni adjustment on estimated marginal means testing the significance of time effects in each group (RE, RVE) and vice versa, the significance of group effects at each time of examination (pre, post). In a pilot study, acute effects of the vibration frequency (20 Hz vs. 40 Hz) during RVE were also tested with LME for repeated measures using the fixed factors frequency and repetition. Differences between anthropometric data of the two subject groups were tested using an independent t-test. For all tests, the significance level was set at P<0.05, also taking into consideration a tendency level of P=0.05 to 0.1. For significant univariate effects, we also calculated the effect size as Cohen’s d, which is the difference of the two compared means divided by the corresponding pooled standard deviation. A weak effect was found at d>0.2, a medium effect at d>0.5 and a strong effect at d>0.8. Values are presented as means ± standard error of the mean (SEM).
Results
Total training weight
After 6 weeks of training, total training weight (ttw) was significantly increased in both groups (main time effect, P<0.001; univariate time effect, RE: 33.3%, P<0.001, d=2.60 and RVE: 24.6%, P<0.001, d=2.24, Figure 3). There was a significant difference between the two groups (main group effect, P=0.002). However, the difference in ttw between both groups was only significant after 6 weeks of training (univariate group effect, pre: P=0.100, post: P=0.009, d=1.14). No time*group effect was found for ttw.
Figure 3.
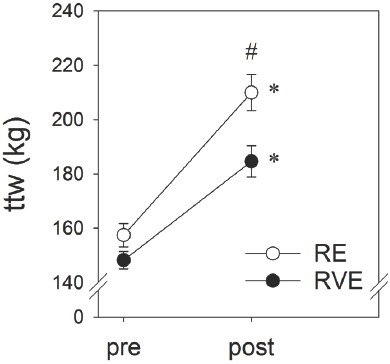
Total training weight (ttw) applied pre and post 6 weeks of RE (n=12) and RVE (n=13) (mean ± SEM), ttw = training load + body weight, RE = Resistive Exercise, RVE = Resistive Vibration Exercise, *Significant univariate time effect (pre, post) for each group, #Significant univariate group effect between RVE and RE at each time of examination.
EMG amplitudes normalized to total training weight
In the pilot study, when the neuro-muscular system was not adapted to WBV, the EMG/ttw of the rectus femoris muscle at 40 Hz RVE was 34.8% higher than at 20 Hz (main frequency effect, P<0.001, d=0.93, Figure 4). In the gastrocnemius lateralis muscle, a difference of 22.9 % (main frequency effect, P<0.001, d=0.53, Figure 4) was found between 20 and 40 Hz RVE. In both muscles and at both frequencies, we did not find a significant change in EMG/ttw between repetitions.
Figure 4.
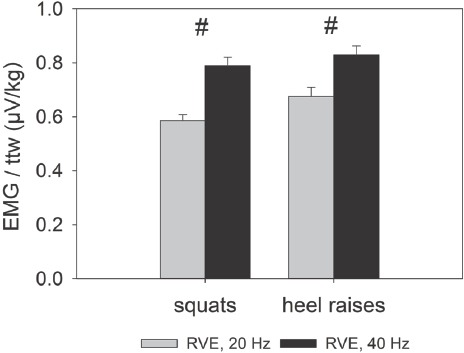
Acute effects of 20 Hz vs. 40 Hz vibration frequency: EMG amplitudes normalized to total training weight (ttw) measured as an acute response to RVE with 20 Hz or 40 Hz WBV during squats and heel raises (mean ± SEM), ttw = training load + body weight, RE = Resistive Exercise, RVE = Resistive Vibration Exercise, #Significant effect of frequency between 20 Hz and 40 Hz RVE.
In the main study on long-term training effects, one subject of the RE group did not perform the post measurement.
After the 6 weeks of training, there was a significant reduction of EMG/ttw during squats in the rectus femoris muscle (main time effect, P<0.001, Figure 5). However, looking at these groups separately, only in the RVE group the time effect was significant (univariate time effect, RE: -5.7%, P=0.087 and RVE: -30.9%, P<0.001, d=1.01). Overall, WBV did not enhance the EMG/ttw (main group effect, P=0.624, Figure 5). However, there was a significant time*group effect (P<0.001). The changes in EMG/ttw by increasing number of repetitions did not reach the level of significance (repetition effect, P=0.122). At the pre measurement, EMG/ttw in rectus femoris muscle was significantly higher during squats at 20 Hz RVE than during RE (univariate group effect, pre: 20.3%, P=0.006, d=0.52, Figure 5). After the 6 weeks of training, EMG/ttw in rectus femoris muscle was significantly lower in RVE compared to RE (univariate group effect, post: -11.9%, P=0.021, d=0.42).]
Figure 5.
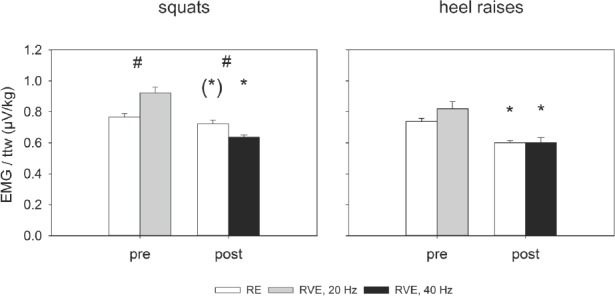
EMG amplitudes normalized to total training weight (ttw) pre and post 6 weeks of RE (squats: n=12 subjects x 8 repetitions; heel raises: n=12 subjects x 12 repetitions) and RVE (squats: n=13 subjects x 8 repetitions; heel raises: n=13 subjects x 12 repetitions) (mean ± SEM), RE = Resistive Exercise, RVE = Resistive Vibration Exercise, *Significant or (*)tendency effect of time (pre, post) for each group (RE, RVE), #Significant effect of group (RE, RVE) at each time (pre, post) of examination.
After the 6 weeks of training, we found a significant reduction of EMG/ttw during heel raises in the gastrocnemius lateralis muscle in both groups (main time effect, P<0.001; univariate time effect, RE: -18.6%, P<0.001, d=0.66 and RVE: -26.7%, P<0.001, d=0.70, Figure 5). The main effects of group and time*group were not significant during heel raises (P=0.900 and P=0.210, respectively). Also, the changes in EMG/ttw by increasing number of repetitions did not reach the level of significance (repetition effect, P=0.311).
Oxygen uptake normalized to total training weight
One subject of the RVE group and one subject of the RE group did not perform the post measurement of the long-term study.
After 6 weeks of training, ∆V’O2/ttw during squats was significantly reduced in both groups (main time effect, P=0.002; univariate time effect, RE: -10.9%, P=0.028, d=0.99 and RVE: -10.5%, P=0.016, d=0.97, Figure 6). In addition, there was a significant main group effect (P<0.001) with higher ∆V’O2/ttw at 20 Hz RVE before training (univariate group effect, pre: 14.9%, P=0.007, d=1.20) and after 6 weeks at 40 Hz RVE (univariate group effect, post: 15.4%, P=0.006, d=1.16). No time*group effect was found during squats (P=0.867).
Figure 6.
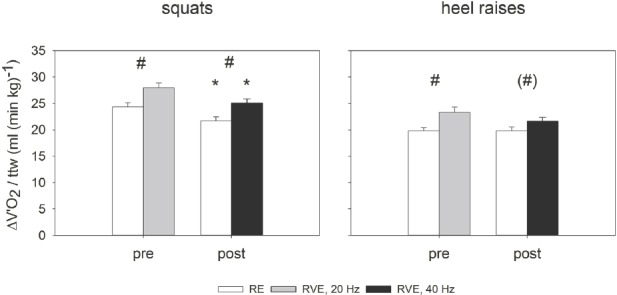
The specific oxygen uptake (∆V’O2) normalized to total training weight (ttw) pre and post 6 weeks of RE (n=12) and RVE (n=12) (mean ± SEM), RE = Resistive Exercise, RVE = Resistive Vibration Exercise, *Significant effect of time (pre, post) for each group (RE, RVE), #Significant effect of group (RE, RVE) at each time (pre, post) of examination.
During heel raises, ∆V’O2/ttw was not affected after the 6 weeks of training (main time effect, P=0.262). However, there was a significant main group effect (P=0.001). In detail, looking at these groups separately, only in the pre measurement the group effect with higher ∆V’O2/ttw during RVE was significant (univariate group effect, pre: 17.8%, P=0.005, d=1.29, post: 9.2%, P=0.099). No time*group effect was found during heel raises (P=0.269).
Discussion
Our aim for the present study was to use progressive high intensity conventional resistance training (RE) and compare it against the same training regimen plus WBV (RVE) with progressively increasing vibration frequencies. To avoid potential early (within days) neuromuscular adaptations to the vibrations stimulus, e.g. a muscle activity decline[13], we increased the vibration frequency on top of progressive training load adaptations over the training period. There were three main findings of this study. First, when the neuromuscular system was not adapted to WBV (pilot study on acute effects of 20 Hz vs. 40 Hz vibration frequency), MU activity normalized to total training weight (training load + body weight, EMG/ttw) was higher during acute RVE at 40 Hz than at 20 Hz. Second, although RVE had initially greater effects on the normalized MU activity (EMG/ttw) during squats and heel raises than RE alone (long-term study), this effect vanished after 6 weeks of training. Third, initially and after 6 weeks of training, normalized oxygen uptake (∆V’O2/ttw) was higher during RVE than during RE during squats and heel raises. However, after 6 weeks of training, ∆V’O2/ttw was reduced during squats and heel raises in both groups indicating lower specific metabolic energy costs.
It is known that an acute exposure of WBV to RE in the not adapted system increases both the MU activity of leg muscles measured as EMG amplitudes and the metabolic energy turnover measured as V’O2[3-5,13]. Our pilot study on acute effects of 20 Hz vs. 40 Hz vibration frequency showed that 40 Hz RVE increases MU activity significantly more than 20 Hz RVE. Therefore, in our long-term study, we expected to find higher normalized MU activity (EMG/ttw) in RVE during squats and heel raises than in RE also after 6 weeks of training. However, the adaptation processes of the neuromuscular system and the oxygen uptake capacity to a long-term exposure of repeated RVE are poorly investigated.
After a 9-week training intervention, Kvorning et al.[8] did not find any significant difference in MU activity during RE and RVE with a moderate progression in vibration frequency during RVE. Although, in our study we used a more pronounced progression in vibration frequencies reaching 40 Hz after 6 weeks of training, we confirmed the finding of a neuromuscular adaptation to WBV. In addition, our RVE training load was significantly lower at post measurement compared to RE, which is likely due to vibration-induced elevation of musculoskeletal forces[24].
Mechano-sensing during WBVT can trigger reflexes that may become visible as synchronous or non-synchronous MU activity[16,27-31]. Narrow banded stop filters at the vibration frequency and its harmonics applied to a bipolar surface EMG record erase electrical motion artifacts[15,31,32] and may also partially filter H-wave like compound action potentials[28]. In our study, the big electrical waves overlapping the EMG in our records during RVE (Figure 2) showed a periodic time that was corresponding with the periodic time of the currently applied vibration. The periodic time of a compound action potential elicited as stretch reflex should not vary by the vibration frequency. Moreover, during RVE subjects never reported about vibration induced muscle contractures and a resulting increase in joint stiffness. Such contractures should occur in response to involuntarily evoked, synchronized action potentials in the whole leg musculature if stretch reflexes would play a major role in response to WBV. Therefore, we conclude that our filtering of the EMG signal predominantly erased motion artifacts and voluntary non-synchronized MU activity accidently occurring at the filter frequencies. However, we cannot completely exclude that during WBV the filtering process also eliminated a small fraction of synchronized MU activity that was hidden in the large artifact signal.
Damping of vibrations plays an important role in mitigating harmful vibrations to the trunk and head[1,14-18] and reduces the acceleration amplitudes along the vertical body axis[13,15]. Therefore, one would assume that the lower leg muscles are more affected than the upper leg muscles, since they are closer to the vibration platform[15,19]. However, normalized neuromuscular responses were similar for RVE on the upper leg and on the lower leg in our study. This might be because loading progression during the 6 weeks of training was based on squat performance and therefore, heel raises loading was at lower intensities (below the intended 80 % of the 1RM) inducing less muscle activity[5,6]. However, in both, squats and heel raises, the recruited number of motor units was already high at the first repetition. A further increase in EMG/ttw with increasing number of repetitions in compensation for fatigue processes in the musculature could not be shown.
To the best of our knowledge, this is the first study analyzing long-term effects on the capacity of WBVT to increase oxygen uptake in healthy young people. Only one study[33] studied the effects of WBVT on cardiorespiratory fitness (VO2peak during bicycle ergometer test) of the healthy elderly during a 1 year fitness program. They found similar significant increases of oxygen uptake in both groups, the vibration group (lower and upper body exercises on the vibration platform) and the fitness group (cardiovascular, resistance, balance and flexibility exercises) after the 1-year program. Despite the big differences in methodology (duration, type of training/exercises, training intensity, and subject characteristics) between this study and our study, oxygen uptake in RVE and RE of our study decreased after 6 weeks of training. However, the initial additional oxygen uptake in RVE compared to RE in our study was maintained after the 6 weeks of training likely due to adaptation processes within the cardiovascular system that take more time than, for example, the neuromuscular adaptations (reduced EMG/ttw) seen in our results. Another explanation could be that since muscle temperature becomes more quickly elevated with WBV than traditional forms of warm-up[34], the potentially higher mechanically-induced heat production during intense RVE might have caused a higher oxygen uptake than in RE.
In conclusion, we confirmed the frequency-dependent increase in the acute neuromuscular response to WBV added to resistive exercise. Moreover, after 6 weeks of squat and heel raise training with progressively increasing loads and progressively increasing vibration frequencies from 20 to 40 Hz, we showed that the initially observed additional elevation in MU activity in RVE compared to RE could not be preserved after 6 weeks of training. However, the respiratory oxygen uptake in RVE was significantly elevated pre and post the 6 weeks of training compared to RE, although, it was reduced in absolute values after the 6 weeks of training. The elevation of oxygen uptake during RVE compared to RE after 6 weeks of training cannot conclusively be explained. In addition, we assume that an additional specific adjustment of the intended training intensity (80 % of the 1RM) for heel raises could have been beneficial to improve the WBV effects during heel raises. The relatively specific and marginal benefits of RVE over RE with this type of training protocol make this kind of high intensity training not suitable for the general population but rather for professional athletes having supervised exercise sessions (to ensure training safety) and the need for a different training stimulus for a rather short period of time.
Acknowledgements
The author would like to thank the subjects from the EVE-Study and the DLR personnel that helped with the study implementation. The author received a SpaceLife scholarship that is funded in equal parts by the Helmholtz Association and the German Aerospace Center (DLR).
Conceived and designed the experiments: AR AB JM JZ ES JR.
Performed the experiments: AR AB JZ JR.
Analyzed the data: AR JZ.
Contributed reagents/materials/analysis tools: ES JR.
Wrote the paper: AR JZ.
Footnotes
The authors have no conflict of interest.
Edited by: G. Lyritis
References
- 1.Rittweger J. Vibration as an exercise modality:how it may work, and what its potential might be. Eur J Appl Physiol. 2010;108(5):877–904. doi: 10.1007/s00421-009-1303-3. [DOI] [PubMed] [Google Scholar]
- 2.Cochrane DJ. Vibration exercise:the potential benefits. Int J Sports Med. 2011;32(2):75–99. doi: 10.1055/s-0030-1268010. [DOI] [PubMed] [Google Scholar]
- 3.Rittweger J, Schiessl H, Felsenberg D. Oxygen uptake during whole-body vibration exercise:comparison with squatting as a slow voluntary movement. Eur J Appl Physiol. 2001;86(2):169–73. doi: 10.1007/s004210100511. [DOI] [PubMed] [Google Scholar]
- 4.Zange J, Haller T, Müller K, Liphardt AM, Mester J. Energy metabolism in human calf muscle performing isometric plantar flexion superimposed by 20-Hz vibration. Eur J Appl Physiol. 2009;105(2):265–70. doi: 10.1007/s00421-008-0898-0. [DOI] [PubMed] [Google Scholar]
- 5.Ritzmann R, Gollhofer A, Kramer A. The influence of vibration type, frequency, body position and additional load on the neuromuscular activity during whole body vibration. Eur J Appl Physiol. 2013;113(1):1–11. doi: 10.1007/s00421-012-2402-0. [DOI] [PubMed] [Google Scholar]
- 6.Hazell TJ, Kenno KA, Jacobi JM. Evaluation of muscle activity for loaded and unloaded dynamic squats during vertical whole-body vibration. J Strength Cond Res. 2010;24(7):1860–5. doi: 10.1519/JSC.0b013e3181ddf6c8. [DOI] [PubMed] [Google Scholar]
- 7.Kang J, Porfido T, Ismaili C, Selamie S, Kuper J, Bush JA, Ratamess NA, Faigenbaum AD. Metabolic responses to whole-body vibration:effect of frequency and amplitude. Eur J Appl Physiol. 2016;116(9):1829–39. doi: 10.1007/s00421-016-3440-9. [DOI] [PubMed] [Google Scholar]
- 8.Kvorning T, Bagger M, Caserotti P, Madsen K. Effects of vibration and resistance training on neuromuscular and hormonal measures. Eur J Appl Physiol. 2006;96(5):615–25. doi: 10.1007/s00421-006-0139-3. [DOI] [PubMed] [Google Scholar]
- 9.Preatoni E, Colombo A, Verga M, Galvani C, Faina M, Rodano R, Preatoni E, Cardinale M. The effects of whole-body vibration in isolation or combined with strength training in female athletes. J Strength Cond Res. 2012;26(9):2495–506. doi: 10.1519/JSC.0b013e31823f299d. [DOI] [PubMed] [Google Scholar]
- 10.Bertuzzi R, Pasqua LA, Bueno S, Damasceno MV, Lima-Silva AE, Bishop D, Tricoli V. Strength-training with whole-body vibration in long-distance runners:a randomized trial. Int J Sports Med. 2013;34(10):917–23. doi: 10.1055/s-0033-1333748. [DOI] [PubMed] [Google Scholar]
- 11.Mester J, Kleinöder H, Yue Z. Vibration training:benefits and risks. J Biomech. 2006;39(6):1056–65. doi: 10.1016/j.jbiomech.2005.02.015. [DOI] [PubMed] [Google Scholar]
- 12.Perez-Turpin JA, Zmijewski P, Jimenez-Olmedo JM, Jove-Tossi MA, Martinez-Carbonell A, Suarez-Llorca C, Andreu-Cabrera E. Effects of whole body vibration on strength and jumping performance in volleyball and beach volleyball players. Biol Sport. 2014;31(3):239–45. doi: 10.5604/20831862.1112435. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Rosenberger A, Liphardt AM, Bargmann A, Müller K, Beck L, Mester J, Zange J. EMG and Heart Rate Responses Decline within 5 Days of Daily Whole-Body Vibration Training with Squatting. PLoS One. 2014;9(6):e99060. doi: 10.1371/journal.pone.0099060. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Wakeling JM, Nigg BM, Rozitis AI. Muscle activity damps the soft tissue resonance that occurs in response to pulsed and continuous vibrations. J Appl Physiol. 2002;93(3):1093–103. doi: 10.1152/japplphysiol.00142.2002. [DOI] [PubMed] [Google Scholar]
- 15.Pollock RD, Woledge RC, Mills KR, Martin FC, Newham DJ. Muscle activity and acceleration during whole body vibration:effect of frequency and amplitude. Clin Biomech. 2010;25(8):840–6. doi: 10.1016/j.clinbiomech.2010.05.004. [DOI] [PubMed] [Google Scholar]
- 16.Abercromby AF, Amonette WE, Layne CS, McFarlin BK, Hinman MR, Paloski WH. Vibration exposure and biodynamic responses during whole-body vibration training. Med Sci Sports Exerc. 2007;39(10):1794–800. doi: 10.1249/mss.0b013e3181238a0f. [DOI] [PubMed] [Google Scholar]
- 17.Mester J, Spitzenfeil P, Schwarzer J, Seifriz F. Biological reaction to vibration - implications for sport. J Sci Med Sport. 1999;2(3):211–26. doi: 10.1016/s1440-2440(99)80174-1. [DOI] [PubMed] [Google Scholar]
- 18.Randall JM, Matthews RT, Stiles MA. Resonant frequencies of standing humans. Ergonomics. 1997;40(9):879–86. doi: 10.1080/001401397187711. [DOI] [PubMed] [Google Scholar]
- 19.Rosenberger A, Beijer A, Johannes B, Schoenau E, Mester J, Rittweger J, Zange J. Changes in muscle cross-sectional area, muscle force, and jump performance during 6 weeks of progressive whole-body vibration combined with progressive, high intensity resistance training. J Musculoskelet Neuronal Interact. 2017;17(2):38–49. [PMC free article] [PubMed] [Google Scholar]
- 20.Hazell TJ, Lemon PW. Synchronous whole-body vibration increases VO(2) during and following acute exercise. Eur J Appl Physiol. 2012;112(2):413–20. doi: 10.1007/s00421-011-1984-2. [DOI] [PubMed] [Google Scholar]
- 21.Rittweger J, Ehrig J, Just K, Mutschelknauss M, Kirsch KA, Felsenberg D. Oxygen uptake in whole-body vibration exercise:influence of vibration frequency, amplitude, and external load. Int J Sports Med. 2002;23(6):428–32. doi: 10.1055/s-2002-33739. [DOI] [PubMed] [Google Scholar]
- 22.Kang J, Bushi JA, Ratamess NA, Faigenbaum AD, Klei S, Maconi D, Kreckel M. Acute effects of whole-body vibration on energy metabolism during aerobic exercise. J Sports Med Phys Fitness. 2016;56(7-8):834–42. [PubMed] [Google Scholar]
- 23.Justo AC, Saavedra FJ, Vilaca-Alves J, Rosa C, Neves EB, Reis VM. Comparing consumption oxygen during and after squat exercise in Smith Machine and whole-body vibration: IEEE Engineering in Medicine and Biology Society. 2015 doi: 10.1109/EMBC.2015.7319401. [DOI] [PubMed] [Google Scholar]
- 24.Beijer A, Rosenberger A, Weber T, Zange J, May F, Schoenau E, Mester J, Bloch W, Rittweger J. Randomized controlled study on resistive vibration exercise (EVE Study): protocol, implementation and feasibility. J Musculoskelet Neuronal Interact. 2013;13(2):147–56. [PubMed] [Google Scholar]
- 25.Baechle TR, Earle RW. Essentials of strength training and conditioning. Champaign: Human Kinetics; 2000. [Google Scholar]
- 26.Beijer A, Degens H, Weber T, Rosenberger A, Gehlert S, Herrera F, Kohl-Bareis M, Zange J, Bloch W, Rittweger J. Microcirculation of skeletal muscle adapts differently to a resistive exercise intervention with and without superimposed whole-body vibrations. Clin Physiol Funct Imaging. 2014;35(6):425–35. doi: 10.1111/cpf.12180. [DOI] [PubMed] [Google Scholar]
- 27.Burke D, Hagbarth KE, Lofstedt L, Wallin BG. The responses of human muscle spindle endings to vibration during isometric contraction. J Physiol. 1976;261(3):695–711. doi: 10.1113/jphysiol.1976.sp011581. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Ritzmann R, Kramer A, Gruber M, Gollhofer A, Taube W. EMG activity during whole body vibration:motion artifacts or stretch reflexes? Eur J Appl Physiol. 2010;110(1):143–51. doi: 10.1007/s00421-010-1483-x. [DOI] [PubMed] [Google Scholar]
- 29.Martin BJ, Park HS. Analysis of the tonic vibration reflex:influence of vibration variables on motor unit synchronization and fatigue. Eur J Appl Physiol Occup Physiol. 1997;75(6):504–11. doi: 10.1007/s004210050196. [DOI] [PubMed] [Google Scholar]
- 30.Roelants M, Verschueren SM, Delecluse C, Levin O, Stijnen V. Whole-body-vibration-induced increase in leg muscle activity during different squat exercises. J Strength Cond Res. 2006;20(1):124–9. doi: 10.1519/R-16674.1. [DOI] [PubMed] [Google Scholar]
- 31.Abercromby AF, Amonette WE, Layne CS, McFarlin BK, Hinman MR, Paloski WH. Variation in neuromuscular responses during acute whole-body vibration exercise. Med Sci Sports Exerc. 2007;39(9):1642–50. doi: 10.1249/mss.0b013e318093f551. [DOI] [PubMed] [Google Scholar]
- 32.Fratini A, Cesarelli M, Bifulco P, Romano M. Relevance of motion artifact in electromyography recordings during vibration treatment. J Electromyogr Kinesiol. 2009;19(4):710–8. doi: 10.1016/j.jelekin.2008.04.005. [DOI] [PubMed] [Google Scholar]
- 33.Bogaerts CG, Delecluse C, Claessens AL, Troosters T, Boonen S, Verschueren SM. Effects of whole body vibration training on cardiorespiratory fitness and muscle strength in older individuals (a 1-year randomised controlled trial) Age and Ageing. 2009;38(4):448–54. doi: 10.1093/ageing/afp067. [DOI] [PubMed] [Google Scholar]
- 34.Cochrane DJ, Stannard SR, Sargeant AJ, Rittweger J. The rate of muscle temperature increase during acute whole-body vibration exercise. Eur J Appl Physiol. 2008;103(4):441–8. doi: 10.1007/s00421-008-0736-4. [DOI] [PubMed] [Google Scholar]