

Abstract
Objectives
Despite the growing numbers and proportion of older adults with bipolar disorder (OABD), there are very limited guidelines for the use of lithium with its double‐edged potential for effectiveness and toxicity in this population. The primary aims of this Delphi survey were: (a) To determine the place of lithium among the preferred choices for maintenance treatment of OABD. (b) To provide detailed clinical guidelines for the safe and effective use of lithium in OABD.
Methods
In the face of limited evidence, the Delphi survey method was used to achieve consensus by a group of 25 experts in OABD from nine countries. An oversight committee monitored and analyzed the results of each survey and formulated more focused questions with each subsequent iteration.
Results
A 100% response rate was achieved for all three iterations of the survey. Lithium was the preferred choice for maintenance monotherapy in OABD. Serum levels of 0.4‐0.8 mmol/L were recommended for ages 60‐79 and serum levels of 0.4‐0.7 mmol/L were recommended for ages 80 and over. Specific recommendations achieved consensus for second line monotherapy as well as for other drugs to be used in combination with lithium if necessary. Guidelines for routine monitoring of lithium in OABD were provided for laboratory investigations and clinical assessments.
Conclusions
Lithium remains the preferred choice for maintenance monotherapy in OABD. Laboratories should report the therapeutic range for serum levels of lithium separately for older adults.
Keywords: Delphi, lithium, maintenance, older adults
1. INTRODUCTION
Older adults with bipolar disorder (OABD), generally regarded as age 60 years or over, represent 6% of geriatric psychiatry outpatient visits and 10% of geriatric psychiatry inpatients.1 OABD is expected to comprise 50% of all cases of bipolar disorder by 2030.2 Despite these significant numbers, international guidelines for the treatment of bipolar disorders have generally not considered the specific management needs associated with OABD to date.3
Based on a recent review of clinical practice guidelines (CPGs) and pharmaco‐epidemiological data for all ages, lithium remains the first‐line treatment for maintenance monotherapy despite the availability of several other choices for mood stabilization.4, 5, 6 Treatment with lithium has been shown to reduce the risk of suicide7, 8 and psychiatric admissions.4 Emerging epidemiological and neurophysiological evidence suggests that lithium may have neuroprotective properties and reduce the risk of dementia9, 10 and conceivably of cancer.11 The results of neuroimaging studies have suggested that adults with bipolar disorder treated with lithium have better preserved cortical gray matter volume.12, 13 Notably, OABD who were using lithium reported positive attitudes toward treatment.14
On the other hand, lithium, just like all of the other mood stabilizers including antipsychotic agents, represents a double‐edged sword for older adults. One concern has been its possible role in increasing the risk of chronic renal failure15, 16 although there is also considerable recent epidemiological evidence that the risk is not as concerning as originally considered.17 Other concerns include hypothyroidism,18 hypercalcemia,19 neurotoxicity,20 and parkinsonism.21 As the cohort of bipolar patients successfully maintained on lithium reaches their 70’s and 80’s, the age associated decrease in renal clearance may lead to higher lithium levels. This in turn leads to increased risk of side effects and outright toxicity if typical adult doses are not lowered.20, 22 Several commonly used drugs in older adults, such as diuretics, ACE Inhibitors and non‐steroidal anti‐inflammatory drugs, can interact with lithium and cause higher serum levels, thereby increasing the risk of toxicity.23 Furthermore, symptoms of toxicity (eg, tremor, gastrointestinal upset, and neurological disturbance) can be misinterpreted as other conditions commonly seen in later life, such as parkinsonism or dementia.21 A “prescribing cascade” may ensue,24 with additional medications introduced unnecessarily to assist in the management of the observed symptoms (eg, dopaminergic agents, cognitive enhancers, and gastrointestinal drugs). Clearly, more evidence and guidelines are needed that balance the risks and benefits of lithium use in OABD.25, 26
The first randomized control study of lithium for OABD was only recently published.27 The investigators compared the efficacy of lithium and divalproex in older adults for acute mania and mixed presentations, but not for maintenance therapy. Both drugs were shown to be efficacious and well tolerated, although lithium was associated with greater reduction in mania scores. While the evidence for its effectiveness remains high, the use of lithium in OABD has been declining compared to atypical antipsychotic agents and divalproex—a phenomenon for which there is no good supportive evidence.28, 29This increasing reluctance to prescribe lithium in OABD is most likely due to concerns about its toxicity, limited experience of younger clinicians with the use of lithium, and the impact of pharmaceutical marketing.29
The most recent reviews of CPGs on the use of lithium for all ages recommend a target maintenance therapeutic serum level range of 0.6‐0.8 mmol/L. The recently recommended therapeutic range is lower than the ones provided by most laboratories around the world which do not take into account the age of patients, phase of illness, or medical comorbidities. Malhi et al6 have summarized the limited recommendations in CPGs for older adults which are not detailed. Their recommended therapeutic range was 0.6‐0.8 mmol/L but reported other ranges that varied from 0.4 to 1.3 mmol/L. Moreover, they noted that one of the limitations of CPGs is the lack of sensitivity to real world presentations.6
In the face of compelling evidence for the effectiveness of lithium in bipolar disorder and its potential for neuroprotection combined with the lack of specific and detailed guidelines for its use in OABD, the ISBD task force on OABD conducted a Delphi survey of maintenance treatment for lithium in older adults in order to provide better direction for clinicians on the safety and effectiveness of lithium use in this vulnerable population. This survey focused on the question of maintenance therapy in OABD because of the clinical concern that the large cohort of adults who has been maintained on mood stabilizers for many years are now reaching old age. This study aims to fill the gap in data for this phase of treatment in OABD. Clinical experience also suggests that lithium toxicity may be missed in older adults and that the “therapeutic” range for lithium reported by most labs could be misleading and lead to a false sense of “safe practice,” especially to clinicians with limited experience in the use of lithium in OABD.
The primary aims of the survey were:
To determine the place of lithium among the preferred choices for maintenance treatment of OABD.
To provide clinical guidelines for the safe and effective use of lithium in OABD.
2. METHODS
2.1. Study Design and Procedure
In the face of very limited systematic evidence for maintenance treatment in OABD, the Delphi method was chosen as a technique for obtaining consensus from a group of experts. Such panels generally consist of 10‐25 experts.30 The Delphi method has been used since the 1950’s as a means of achieving consensus of expert opinion on a wide range of real‐world knowledge.31 It consists of a series of surveys where each wave represents a refinement of the previous one through a systematic process of feedback from the group.30 This leads to a progressive move toward consensus.30, 31 This is viewed as a type of “virtual meeting” that anonymizes the experts to each other and facilitates independent thought and the gradual formation of a considered opinion through a systematic process of communication and feedback.30 An oversight committee is commonly set up to monitor unintentional bias. Because of the interest in correcting a perceived loss of confidence in the use of lithium in OABD, the potential bias in this initiative needed checks and balances. Without more valid evidence for lithium use in OABD, a systematic approach to expert consensus is the best way of providing direction to clinicians—perhaps enhancing the current clinical practice guidelines (CPG's) whose methodology varies considerably.6
Three iterations, not more than 15‐20 minutes in length, were sent electronically to each expert at approximately 1‐month intervals (see Supporting information S1, S2, S3). All questions were framed within the clinical scenario of maintenance treatment in OABD. The first iteration was open‐ended and asked about demographic features of the participant experts, their choice of mood stabilizers by order of preference, suggested therapeutic range for lithium levels, recommended routine laboratory investigations and clinical assessments during lithium maintenance, and clinical signs of lithium toxicity. Other prescribing practices were explored including the impact of subtype diagnosis and dosing schedules.
The questions separated the recommendations into two broad age groups within OABD, ages 60‐79 and 80 years, or over. Each survey asked the experts to comment on the items presented and provide a brief rationale for each answer. Participants were given opportunities to identify other areas of concern or controversy. Each iteration was reviewed by an oversight committee (KS, OA, NH, AS, SS, AD, MS). The members of the oversight committee were also respondents in the survey. A cumulative impression of the group judgment for each item was presented by the oversight committee to the experts for the purpose of reviewing or revising their answers. The next iteration was then sent to all participants with each iteration comprised of questions that narrowed the focus based on previous responses. These iterations continued until consensus was reached (at least 80% agreement for each item) or the pre‐set limit of three iterations elapsed, in which case non‐consensus items were identified.
A flow chart describing the Delphi Method is presented in Figure 1.
Figure 1.

The Delphi method: A systematic feedback process toward achieving consensus [Colour figure can be viewed at wileyonlinelibrary.com]
2.2. Participants
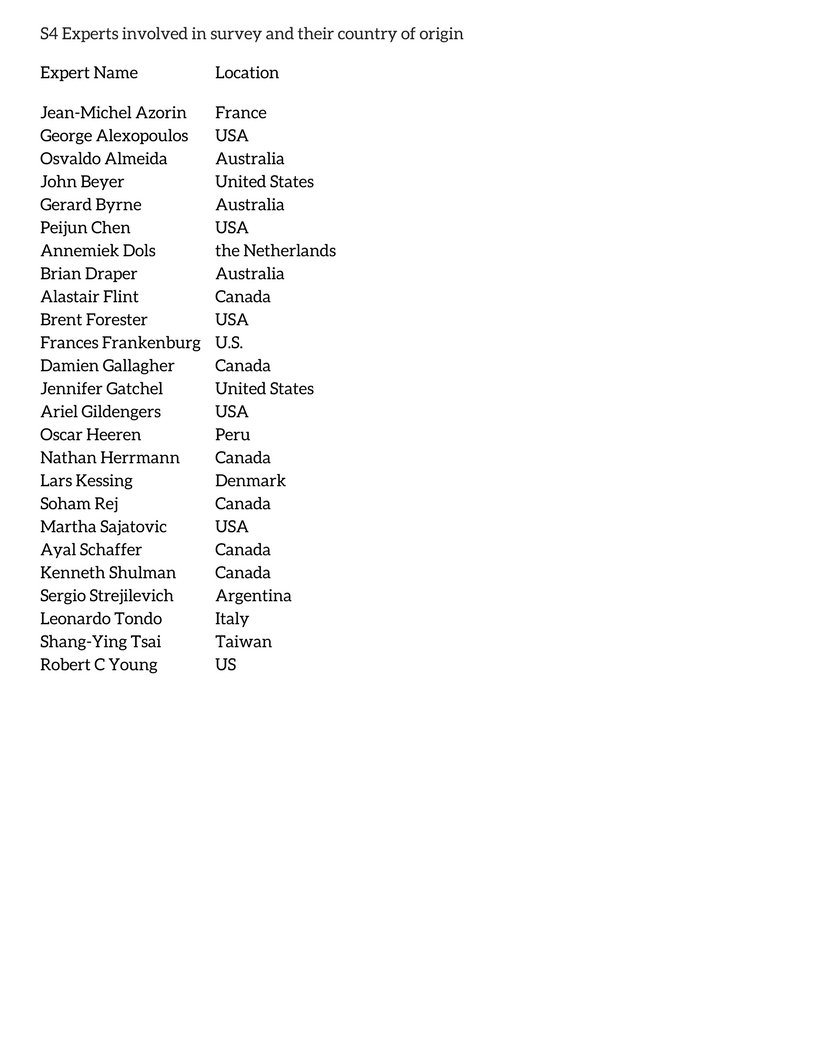
An invitation to participate on the panel was extended to all the physician members of the ISBD OABD task force. This proved to be an excellent convenience sample from which to identify the best available internationally representative experts in this clinical arena. Members of the task force were then asked to nominate other potential experts for inclusion on the panel. Twenty‐seven experts were invited to take part in the Delphi survey. One did not respond to two invitations and another reported limited experience with OABD. This left an expert group of 25 psychiatrists, 23 of whom identified themselves as geriatric psychiatrists and two as general psychiatrists with expertise in bipolar disorders. Table S4 summarizes the list of the experts involved in this survey and their countries of origin.
3. RESULTS
3.1. Response rate
A complete response rate of 100% was achieved for all three iterations of the survey.
3.2. Preferred choice for the maintenance of OABD
There was 100% consensus that lithium should be the drug of choice for maintenance monotherapy in OABD. Second line medications considered appropriate for monotherapy maintenance of OABD included lamotrigine, olanzapine, quetiapine, and valproate (See Table 1). No consensus was achieved regarding order of preference and hence the results of this question were reported as a group of optional choices listed in alphabetical order.
Table 1.
Recommendations for maintenance therapy for older adults with bipolar disorder (OABD)
| Target serum lithium range | First‐line choices to COMBINE with lithium maintenance treatment for OABD | Second‐line choices for monotherapy treatment for OABD | |
|---|---|---|---|
| Age | mmol/L | ||
| 60‐79 | 0.4‐0.8 | Lamotrigine | Lamotrigine |
| 80+ | 0.4‐0.7 | Quetiapine | Olanzapine |
| Valproate | Quetiapine | ||
| Valproate | |||
If maintenance of OABD with lithium requires adjunctive treatment, the following group of medications were recommended (once again no consensus was achieved regarding order of preference): lamotrigine, quetiapine, and valproate. The experts (84%) did not recommend a different therapeutic range for lithium when used in combination with another psychotropic agent.
3.3. Advice for the safe use of lithium in OABD
After the third iteration, the expert panel achieved consensus regarding the target serum concentration of lithium: 0.4 to 0.8 mmol/L for OABD aged 60 to 79 years and 0.4 to 0.7 mmol/L for those aged 80 years or over. Sixty‐four percent of panel members indicated that the diagnosis of bipolar I and II should not influence the target therapeutic range. There was no consensus regarding the preferred pattern for the daily dosing of lithium: once or twice per day.
Recommendations for maintenance therapy for older adults with bipolar disorder (OABD) can be seen in Table 1.
Table 2 shows the therapeutic ranges of the serum concentration of lithium reported by the local laboratories used by the expert panelists. We requested this information to determine the current practice of laboratories in reporting the therapeutic range for serum lithium levels and to ascertain whether local laboratories provided separate guidelines for older adults. The most common level at the lower limit of the therapeutic range was 0.6 mmol/L (45%) while the most common level for upper limit was 1.2 mmol/L (60%). The current ranges reported by the labs are well above the range recommended by the experts and by recent CPG's for all adults. None of the labs reported a separate therapeutic range for older adults.
Table 2.
Therapeutic range for serum lithium levels in labs used by experts
| Range | No. labs |
|---|---|
| 0.6‐1.2 | 7 |
| 0.5‐1.2 | 3 |
| 0.5‐1.0 | 3 |
| 0.4‐1.3 | 2a |
| 0.6‐1.5 | 1 |
| 0.6‐1.0 | 1 |
| 0.7‐1.2 | 1 |
| 0.8‐1.2 | 1 |
| No specific therapeutic range; intoxicated level alerted when>1.5 mmol/L | 1 |
One lab was used by multiple experts.
A summary of the consensus recommendations regarding the routineassessment of OABD receiving maintenance treatment with lithium can be seen in Table 3. On that basis, it is recommended that OABD maintained on lithium should be assessed by a clinician at least every 6 months.
Table 3.
Routine laboratory and clinical monitoring
| Frequency | Lab testing | Clinical assessments |
|---|---|---|
| 3‐6 months |
Lithium level Serum creatinine eGFR BUN |
Tremor Gait |
| 6‐12 months |
Thyroid function (TSH) Fasting glucose Fasting cholesterol (lipids) Triglycerides Weight (including waist circumference) Calcium |
|
| 12 months | Hematology | Routine cognitive screening (MMSE and/or MoCA) |
| As concerns rise | General and comprehensive neurological assessments |
Table 4 describes the expert consensus regarding the common signs of lithium toxcity among OABD.
Table 4.
Common signs of lithium toxicity among OABD
| Consensus reached |
|
| Consensus not reached |
|
4. FURTHER RESEARCH
From comments received, experts suggested that further research is needed in OABD on the following:
Lithium's long‐term effects on renal function and specifically the concern about chronic renal failure
Lithium's and the atypical antipsychotics’ effect on metabolic function
Guidelines for the use of other mood stabilizers such as lamotrigine, quetiapine, olanzapine, and risperidone
The potential neuroprotective properties of lithium and potential for protection from cancers.
5. DISCUSSION
The results of this survey indicate that lithium remains the preferred choice of experts for mood stabilization during the maintenance phase of OABD. This recommendation must be viewed in the context of a significant and steady decline in use of lithium in this population, likely as a result of excessive anxiety about its safety profile in later life and the lack of pharmaceutical marketing. Hence these findings should provide some reassurance and guidance for clinicians to be more confident in their use of lithium in older adults. The recommended maintenance serum range for lithium for ages 60‐79 is 0.4 to 0.8 mmol/L, while for people aged 80 years or over is 0.4 to 0.7 mmol/L. Surprisingly there was not much difference in the recommended therapeutic range for these two age groups. The most obvious difference compared with published guidelines pertains to the lower therapeutic limit of 0.4 mmol/L compared to 0.6 mmol/L recommended by Malhi et al6and 0.5 mmol/L recommended by Wijeratne and Draper.32 Our group of experts concluded that 0.4 mmol/L may be sufficient for a proportion of OABD. The recommended upper limits of lithium in the serum in this survey were also well below those recommended by others, implying that our experts believe that a lower concentration of lithium may be more effective in later than early life, or that concerns about adverse effects demand greater caution when using lithium in older age. Some experts seemed to favor slightly higher serum lithium levels for Bipolar I patients but this did not achieve consensus. Increased efforts should be made to have laboratories report levels specifically for older adults that are in keeping with those recommended by clinical practice guidelines and by this survey. Certainly, the current therapeutic range for lithium levels reported by laboratories is much higher than is recommended by the most recent clinical practice guidelines6, 33 and the results of this survey for OABD. This current practice by local laboratories puts older adults at risk of lithium toxicity and adds urgency to this clinical issue. Providing separate more appropriate therapeutic ranges of serum lithium levels for older adults should help to minimize the risk of toxicity in this vulnerable population.20
With regard to lithium administration, the experts did not reach consensus on the value of twice compared to once daily dosing. The uncertainty in the literature on this point was reflected by the fact that some experts gave the same reason (less stress on the kidneys) for both options. The majority favored once daily dosing but this did not reach the consensus threshold.
Guidelines for safe monitoring of lithium levels and related laboratory and clinical testing suggest that older adults with bipolar disorder should be seen routinely at least every three to six months with specific laboratory tests and clinical assessments administered as described in the results: renal functioning every 3‐6 months, metabolic and endocrine testing every 6 months, and hematology yearly. Routine clinical assessment of gait and tremor should take place every 3‐6 months and routine cognitive testing should be done annually using the MMSE34 or MoCA.35 By seeing OABD every 3‐6 months, clinicians will be able to monitor the clinical course and detect significant clinical or medical concerns at an early stage. In centers where the availability of psychiatrists is limited, family physicians or allied health professionals can supplement the necessary frequency of clinical monitoring. Special attention must be given to the signs of lithium toxicity in order to avoid the “prescribing cascade” that mistakes lithium side effects and signs of toxicity for another disorder such as parkinsonism, dementia, or gastrointestinal disorder. As most side effects of lithium are dose dependent, these guidelines offer room to lower the dose and serum level without loss of effectiveness.
The safety measures recommended for lithium use in this survey should not suggest that the other possible choices for mood stabilizers are safer and without their own risks. Indeed, there is much that we do not know about the adverse effects of the atypical antipsychotics and other mood stabilizers in OABD inviting more specific research on this issue. Notwithstanding the potential side effects and toxicity associated with lithium use in OABD, the experts still concluded that lithium is the preferred choice for maintenance treatment in OABD. Similarly, despite the consensus in this survey, it should be clear that maintenance treatment with lithium is not necessarily the best option for all OABD and clinicians must continue to make individualized choices based on multiple factors.
Given the scope of the Delphi survey the oversight team decided not to drill down on the question of lithium's effects on long‐term renal function. Some members of the OABD task force argued in favor of reassuring clinicians about the long‐term safety of lithium with regard to chronic kidney disease. However, since this was not explicitly addressed in the survey we are unable to comment definitively on that issue in our recommendations which must reflect the results of the Delphi survey and not simply the opinion of the OABD task force members.
Lessons learned from the use of a Delphi survey include the need to remain focused on specific goals and objectives while avoiding excessive time and energy on controversial areas that are unlikely to achieve consensus. Specifically, we avoided a focus on the controversial area of lithium and renal function and limited our focus to the specific place and use of lithium in the maintenance treatment of OABD. We also refrained from drilling down on the other recommended mood stabilizers.
The successful recruitment of experts was done by personal connections as far as possible with individualized invitations rather than “cold call” emailing that is much less likely to attract participation. Utilizing an existing structure, such as the OABD task force, from which to recruit experts ensured a high degree of interest and motivation to participate in a survey that may take three over four iterations. The use of brief questionnaires, timely feedback and short intervals between iterations helped to maintain motivation and interest in the study and continued participation in the survey on repeated iterations. Our 100% response rate for all three iterations is a testament to those factors and avoided the potential for a low response rate with multiple iterations, one of the common limitations of a Delphi survey.
It was important to identify quickly those issues for which consensus was not possible or likely, and not try to force consensus. The oversight team helped to formulate the next iteration of questions designed to sharpen the focus of the survey and obtain as much consensus as possible. It made most sense to use the Discussion to elaborate on the issues where there was no consensus. Use of the oversight team to review results objectively and avoid unintended guidance of responses due to preconceived ideas was critical.
In the face of very limited published data to inform clinical practice, it has been argued that consensus expert opinion must be explicitly recognized by CPG authoring groups.33 Given the impact that CPG's have on clinical practice, this is an important consideration for maintenance treatment of OABD. Expert opinion is based on a combination of vast clinical experience and accumulated knowledge from a wide range of sources which should strengthen the credibility of CPGs which tend to focus on published “evidence.” A “hybrid” CPG that includes both published data and expert opinion may be more relevant and practical for clinicians.33 The recent CANMAT and ISBD bipolar disorder guidelines provide an example of such a hybrid section on older adults but still lack specifics with regard to therapeutic serum levels of lithium and relevant laboratory and clinical investigations for OABD.36 A hybrid approach also addresses some of the concerns about real world effectiveness raised by Malhi et al6 in their critical review of CPGs. Future CPGs for OABD should incorporate expert consensus recommendations until such time as RCT data are available to guide practice.
These guidelines for OABD could help to stem the unwarranted decline in lithium prescriptions that has been evident in recent years. Pending further systematic data regarding the use of lithium for maintenance therapy in OABD, these Delphi survey recommendations offer robust guidance to clinicians on how best to use lithium for the effective and safe maintenance treatment of OABD.
Supporting information
{kind=link}
{kind=link}
ACKNOWLEDGMENTS
Expert panel members are listed in supplemental Appendix S4. OABD task force members are listed in supplemental Appendix S5. The authors thank Rhona Shulman for help in the design of the Figure, Tables and formatting of the manuscript.
Shulman KI, Almeida OP, Herrmann N, et al. Delphi survey of maintenance lithium treatment in older adults with bipolar disorder: An ISBD task force report. Bipolar Disord. 2019;21:117–123. 10.1111/bdi.12714
REFERENCES
- 1. Sajatovic M, Strejilevich SA, Gildengers AG, et al. A report on older‐age bipolar disorder from the International Society for Bipolar Disorders Task Force. Bipolar Disord. 2015;17(7):689‐704. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Jeste DV, Alexopoulos GS, Bartels SJ, et al. Consensus statement on the upcoming crisis in geriatric mental health: research agenda for the next 2 decades. Arch Gen Psychiatry. 1999;56(9):848‐853. [DOI] [PubMed] [Google Scholar]
- 3. Dols A, Kessing LV, Strejilevich SA, et al. Do current national and international guidelines have specific recommendations for older adults with bipolar disorder? A brief report. Int J Geriatr Psychiatry. 2016;31(12):1295‐1300. [DOI] [PubMed] [Google Scholar]
- 4. Joas E, Karanti A, Song J, Goodwin GM, Lichtenstein P, Landen M. Pharmacological treatment and risk of psychiatric hospital admission in bipolar disorder. Br J Psychiatry. 2017;210(3):197‐202. [DOI] [PubMed] [Google Scholar]
- 5. Lahteenvuo M, Tanskanen A, Taipale H, et al. Real‐world effectiveness of pharmacologic treatments for the prevention of rehospitalization in a finnish nationwide cohort of patients with bipolar disorder. JAMA Psychiatry. 2018;75(4):347‐355. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Malhi GS, Gessler D, Outhred T. The use of lithium for the treatment of bipolar disorder: Recommendations from clinical practice guidelines. J Affect Disord. 2017;217:266‐280. [DOI] [PubMed] [Google Scholar]
- 7. Cipriani A, Hawton K, Stockton S, Geddes JR. Lithium in the prevention of suicide in mood disorders: updated systematic review and meta‐analysis. BMJ. 2013;346:f3646. [DOI] [PubMed] [Google Scholar]
- 8. Song J, Sjolander A, Joas E, et al. Suicidal behavior during lithium and valproate treatment: a within‐individual 8‐year prospective study of 50,000 patients with bipolar disorder. Am J Psychiatry. 2017;174(8):795‐802. [DOI] [PubMed] [Google Scholar]
- 9. Gerhard T, Devanand DP, Huang C, Crystal S, Olfson M. Lithium treatment and risk for dementia in adults with bipolar disorder: population‐based cohort study. Br J Psychiatry. 2015;207(1):46‐51. [DOI] [PubMed] [Google Scholar]
- 10. Kessing LV, Forman JL, Andersen PK. Does lithium protect against dementia? Bipolar Disord. 2010;12(1):87‐94. [DOI] [PubMed] [Google Scholar]
- 11. Huang RY, Hsieh KP, Huang WW, Yang YH. Use of lithium and cancer risk in patients with bipolar disorder: population‐based cohort study. Br J Psychiatry. 2016;209(5):393‐399. [DOI] [PubMed] [Google Scholar]
- 12. Hajek T, Kopecek M, Hoschl C, Alda M. Smaller hippocampal volumes in patients with bipolar disorder are masked by exposure to lithium: a meta‐analysis. J Psychiatry Neurosci. 2012;37(5):333‐343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Sun YR, Herrmann N, Scott C, Black SE, Khan MM, Lanctot KL. Global grey matter volume in adult bipolar patients with and without lithium treatment: a meta‐analysis. J Affect Disord. 2018;225:599‐606. [DOI] [PubMed] [Google Scholar]
- 14. Rej S, Schuurmans J, Elie D, Stek ML, Shulman K, Dols A. Attitudes towards pharmacotherapy in late‐life bipolar disorder. Int Psychogeriatr. 2016;28(6):945‐950. [DOI] [PubMed] [Google Scholar]
- 15. Rej S, Herrmann N, Shulman K, et al. Lithium use, but not valproate use, is associated with a higher risk of chronic kidney disease in older adults with mental illness. J Clin Psychiatry. 2017;78(8):e980–e985. [DOI] [PubMed] [Google Scholar]
- 16. Rej S, Shulman K, Herrmann N, et al. Prevalence and correlates of renal disease in older lithium users: a population‐based study. Am J Geriatr Psychiatry. 2014;22(11):1075‐1082. [DOI] [PubMed] [Google Scholar]
- 17. Kessing LV, Gerds TA, Feldt‐Rasmussen B, Andersen PK, Licht RW. Use of lithium and anticonvulsants and the rate of chronic kidney disease: a nationwide population‐based study. JAMA Psychiatry. 2015;72(12):1182‐1191. [DOI] [PubMed] [Google Scholar]
- 18. Shulman KI, Sykora K, Gill SS, et al. New thyroxine treatment in older adults beginning lithium therapy: implications for clinical practice. Am J Geriatr Psychiatry. 2005;13(4):299‐304. [DOI] [PubMed] [Google Scholar]
- 19. Shine B, McKnight RF, Leaver L, Geddes JR. Long‐term effects of lithium on renal, thyroid, and parathyroid function: a retrospective analysis of laboratory data. Lancet. 2015;386(9992):461‐468. [DOI] [PubMed] [Google Scholar]
- 20. Sun M, Herrmann N, Shulman KI. Lithium toxicity in older adults: a systematic review of case reports. Clin Drug Investig. 2018;38(3):201‐209. [DOI] [PubMed] [Google Scholar]
- 21. Marras C, Herrmann N, Fischer HD, et al. Lithium use in older adults is associated with increased prescribing of Parkinson medications. Am J Geriatr Psychiatry. 2016;24(4):301‐309. [DOI] [PubMed] [Google Scholar]
- 22. Sproule BA, Hardy BG, Shulman KI. Differential pharmacokinetics of lithium in elderly patients. Drugs Aging. 2000;16(3):165‐177. [DOI] [PubMed] [Google Scholar]
- 23. Juurlink DN, Mamdani MM, Kopp A, Rochon PA, Shulman KI, Redelmeier DA. Drug‐induced lithium toxicity in the elderly: a population‐based study. J Am Geriatr Soc. 2004;52(5):794‐798. [DOI] [PubMed] [Google Scholar]
- 24. Rochon PA, Gurwitz JH. The prescribing cascade revisited. Lancet. 2017;389(10081):1778‐1780. [DOI] [PubMed] [Google Scholar]
- 25. Berk M, Cowdery S, Williams L, Malhi GS. Recalibrating the risks and benefits of lithium therapy. Br J Psychiatry. 2017;211(1):117‐2. [DOI] [PubMed] [Google Scholar]
- 26. Shulman KI. Lithium for older adults with bipolar disorder: should it still be considered a first‐line agent? Drugs Aging. 2010;27(8):607‐615. [DOI] [PubMed] [Google Scholar]
- 27. Young RC, Mulsant BH, Sajatovic M, et al. GERI‐BD: a randomized double‐blind controlled trial of lithium and divalproex in the treatment of mania in older patients with bipolar disorder. Am J Psychiatry. 2017;174(11):1086‐1093. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Rej S, Herrmann N, Shulman K, Fischer HD, Fung K, Gruneir A. Current psychotropic medication prescribing patterns in late‐life bipolar disorder. Int J Geriatr Psychiatry. 2017;32(12):1459‐1465. [DOI] [PubMed] [Google Scholar]
- 29. Shulman KI, Rochon P, Sykora K, et al. Changing prescription patterns for lithium and valproic acid in old age: shifting practice without evidence. BMJ. 2003;326(7396):960‐961. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Okoli C. The Delphi method as a research tool: an example, design considerations and applications. Information & Management. 2004;42(1):15‐29. [Google Scholar]
- 31. Hsu C‐C. The Delphi technique: making sense of consensus. Practical Assessment, Research & Evaluation. 2007;12(10):117‐8. [Google Scholar]
- 32. Wijeratne C, Draper B. Reformulation of current recommendations for target serum lithium concentration according to clinical indication, age and physical comorbidity. Aust N Z J Psychiatry. 2011;45(12):1026‐1032. [DOI] [PubMed] [Google Scholar]
- 33. Eibling D, Fried M, Blitzer A, Postma G. Commentary on the role of expert opinion in developing evidence‐based guidelines. Laryngoscope. 2014;124(2):355‐357. [DOI] [PubMed] [Google Scholar]
- 34. Folstein MF, Folstein SE, McHugh PR. “Mini‐mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189‐198. [DOI] [PubMed] [Google Scholar]
- 35. Nasreddine ZS, Phillips NA, Bedirian V, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53(4):695‐699. [DOI] [PubMed] [Google Scholar]
- 36. Yatham LN, Kennedy SH, Parikh SV, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) and International Society for Bipolar Disorders (ISBD) 2018 guidelines for the management of patients with bipolar disorder. Bipolar Disord. 2018;20(2):97‐170. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials