

Abstract
Rationale:
Secondary hyperparathyroidism (SHPT) is often complicated with chronic renal failure. Though the total parathyroidectomy (TPTX) with forearm autotransplantation (FAT) has been commonly used to treatment refractory renal SHPT, the recurrence of SHPT is not infrequent, resulting from hyperplastic autograft, remnant parathyroid tissues, and supernumerary parathyroid gland (SPG).
Patient concerns:
A 67-year-old man undergoing TPTX+FAT 4 years previously for renal SHPT, who received regular hemodialysis with active vitamin D supplements of Rocaltrol treatment postoperatively, was admitted to our hospital with progressively elevated serum intact parathyroid hormone (iPTH) from 176 to 1266 pg/mL for 8 months and bilateral ankle joints pain for 1 month. 99mTc-sestamibi dual-phase imaging with single positron emission tomography (SPECT)/computed tomography (CT) revealed a nodule in suprasternal fossa, besides a nodule in autografted site, accompanied with intense radioactivity.
Diagnosis:
Recurrent SHPT was easily diagnosed based on previous medical history, painful joints, increased serum iPTH level and positive findings of 99mTc-sestamibi imaging. Routine postoperative pathology showed that the nodules were consistent with an adenomatoid hyperplasic autograft and a supernumerary parathyroid adenoma in suprasternal fossa, respectively.
Interventions:
Reoperation for removing nodules in suprasternal fossa and autografted site was performed 1 month later. Then regular hemodialysis 3 times a week with Rocaltrol was continued.
Outcomes:
During 12 months of follow-up, the joints pain improved obviously and the serum iPTH level ranged from 30.1 to 442 pg/mL.
Lessons:
Although rare, recurrent renal SHPT may be caused by a coexistence of both hyperfunctional autograft and SPG after TPTX+FAT. The 99mTc-sestamibi parathyroid imaging with SPECT/CT is helpful to locate the culprits of recurrent renal SHPT before reoperation. To prevent recurrence of renal SHPT, the present initial surgical procedures should be further optimized in patient on permanent hemodialysis.
Keywords: hyperplasia, parathyroid adenoma, recurrence, secondary hyperparathyroidism
1. Introduction
Hyperparathyroidism is usually classified primary, secondary, and tertiary.[1] Secondary hyperparathyroidism (SHPT) is a major complication for patients with chronic renal failure on long-term dialysis.[2] SHPT is characterized by an increase in the intact parathyroid hormone (iPTH) synthesis and secretion and progressive hyperplasia of parathyroid gland, which can lead to high-turnover bone disease, interstitial and vascular calcifications, and as well as cardiovascular morbidity and mortality.[3] For the patients with severe SHPT which is no response to medical treatment, the parathyroidectomy is generally considered and may improve biological parameters, relieve clinical symptoms, such as bone and joint pain, itching, muscle weakness, psychological irritability and easy fatigue, and reduce mortality.[4] Unfortunately, early surgical failure with persistent disease may occur in 5% to 10% of patients and recurrence reaches 20% to 30% at 5 years.[5] The common causes for persistence or recurrence, leading to inevitable reoperation, are attributed to the hyperplastic autografted tissue, remnant parathyroid tissues left in the neck, and/or the presence of ectopic or supernumerary parathyroid glands (SPGs) missed in initial operation.[6,7] Herein, we reported an unusual case of recurrent SHPT caused by adenomatoid hyperplastic autografts coexisting with supernumerary parathyroid adenoma (SPA) after total parathyroidectomy (TPTX) with forearm autotransplantation (FAT).
2. Case report
A 67-year-old Chinese man was admitted to our hospital with bilateral ankle joints pain for 1 month and progressively elevated serum iPTH from 176 to 1266 pg/mL (normal, 15.0–65.0 pg/mL) for 8 months in November 2017. He had a history of polycystic liver and kidney disease for 24 years, hemodialysis for 16 years, and left nephrectomy for infection for 5 years, respectively. He had undergone the TPTX+FAT 4 years previously for renal SHPT, in which total 4 parathyroid glands were excised and then confirmed as hyperplasia histopathologically, and about 30 mg tissues of the left upper parathyroid gland implanted into right forearm at the same time (Fig. 1). Postoperatively, he received regular hemodialysis with active vitamin D supplements of Rocaltrol treatment.
Figure 1.
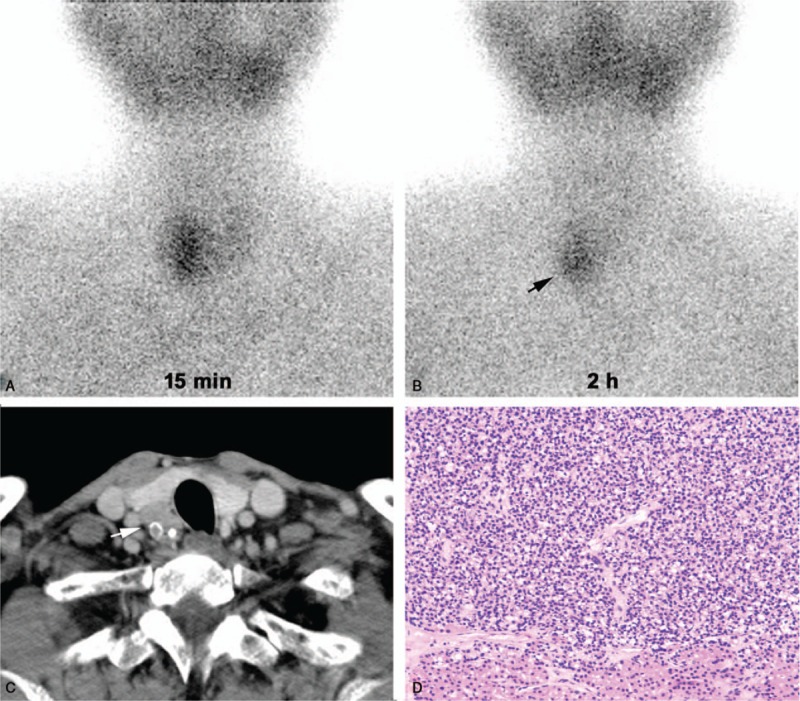
99mTc-sestamibi parathyroid dual-phase scan (A, B) revealed intense radioactivity at the middle-lower region of the right thyroid lobe (black arrow) and cervical contrast-enhanced computed tomography (C) showed multiple enhanced nodules behind thyroid gland (right lower: 3.0 × 2.5 cm, white arrow) before initial surgery. Hematoxylin-eosin stain (D, ×200) confirmed the nodules as parathyroid hyperplasia.
Physical examination revealed a subcutaneous mass with about 3 cm in diameter in autografted site of right forearm. The serum iPTH in right forearm was >12,500 pg/mL. The serum calcium and phosphate was 2.61 mmol/L (normal, 2.03–2.54 mmol/L) and 1.65 mmol/L (normal, 0.87–1.45 mmol/L), respectively. Based on this, the autograft-dependent recurrent SHPT was clinically taken for granted. 99mTc-sestamibi dual-phase imaging with single positron emission tomography (SPECT)/computed tomography (CT) was further performed for preoperative re-evaluation. The images revealed an unexpected nodule (1.5 × 1.2 cm) in suprasternal fossa, besides a nodule (2.5 × 1.0 cm) in autografted site, accompanied with intense radioactivity (Fig. 2). Subsequently, these nodules also were confirmed in cervical contrast-enhanced CT and ultrasonography of right forearm, respectively. The findings suggested that it might be a coexistence of hyperfunctional autograft and SPG.
Figure 2.
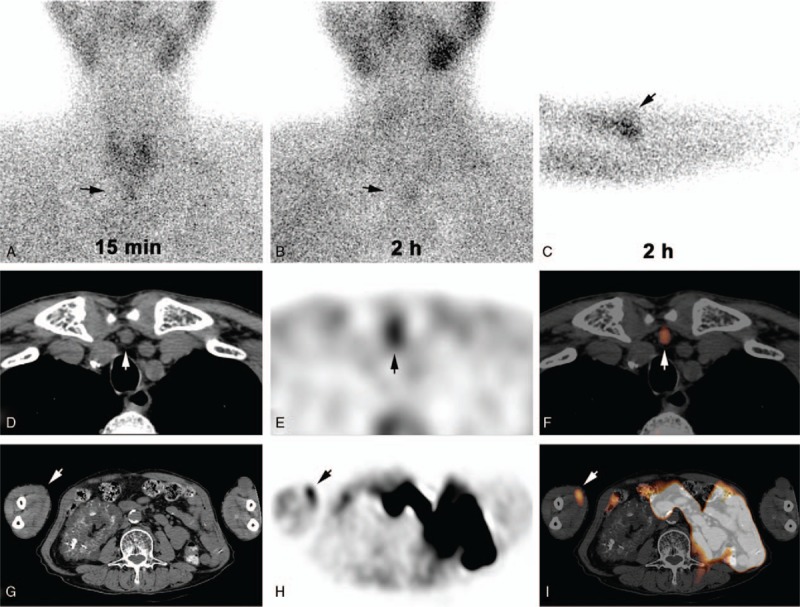
99mTc-sestamibi parathyroid (A, B) and autograft (C) dual-phase scan and SPECT/CT (CT images: D, G; SPECT images: E, H; fusion images: F, I) at 2 hours after administration indicated a nodule (1.5 × 1.2 cm) in suprasternal fossa and a nodule (2.5 × 1.0 cm) in autografted site of right forearm, accompanied with intense radioactivity (arrow). SPECT/CT = single positron emission tomography/computed tomography.
One month later, reoperation for removing the nodules in autografted site and suprasternal fossa was performed and the adenomatoid hyperplastic autograft with SPA was proven through histopathology (Fig. 3). Afterwards, he went on regular hemodialysis 3 times a week with active vitamin D supplements of Rocaltrol. During 12 months of follow-up, the joints pain improved obviously and the serum iPTH, calcium, and phosphate level ranged from 30.1 to 442 pg/mL, 1.96 to 2.86 mmol/L, and 0.81 to 2.68 mmol/L, respectively. This case was approved by the research ethics committee of our institution (No. 2018–763). Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Figure 3.
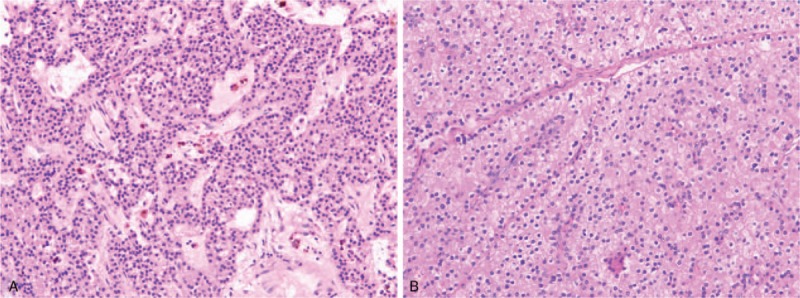
Hematoxylin-eosin stain (×200) showed that the nodules were consistent with a supernumerary parathyroid adenoma (A) in suprasternal fossa and an adenomatoid hyperplasic autograft (B) in right forearm after reoperation, respectively.
3. Discussion
Up to now, although the optimal surgical procedure is still controversial to treat refractory renal SHPT, the TPTX+FAT, involving resection of all parathyroid tissue and immediate transplantation of parathyroid autograft into the nondominant forearm muscle, and subtotal parathyroidectomy, involving resection of all but a ≤50 mg remnant of an in situ parathyroid gland, are widely used and there are no significant differences regarding the efficacy and recurrence rate between them.[2,8] TPTX+FAT is recommended in a patient who has to continue hemodialysis for long periods after the operation, because of being easier and safer to remove the enlarged parathyroid autografts from the forearm at recurrence compared with neck re-exploration.[9,10] In fact, the risk of persistent or recurrent SHPT cannot be negligible after TPTX+FAT, resulting in a reoperation.[6,7,9,10] Tominaga et al[6] reported that persistent renal SHPT was identified in 4.2% patients (49/1156) after initial TPTX+FAT and 42.8% (21/49) of them required reoperation. Yumita et al reported that 40 of 155 hemodialysis patients developed recurrent or persistent renal SHPT after TPTX+FAT.[7] Therefore, it is very important to remove all parathyroid glands at the initial operation and to choose adequate parathyroid tissue for the autograft, in order to prevent persistent and recurrent renal SHPT.[9]
In clinical practice, parathyroid scintigraphy with 99mTc-sestamibi is often recommended to preoperatively locate the hyperfunctional parathyroid glands in patients with hyperparathyroidism.[11–14] Compared with planar imaging and SPECT alone, SPECT/CT can yield higher accuracy of localization and fewer false-positive findings for parathyroid adenomas.[15,16] In patients with recurrent SHPT after surgery, the dual-phase parathyroid and autograft imaging combined with SPECT/CT may clearly locate hyperfunctional parathyroid lesions, particularly for ectopic parathyroid adenoma or SPA.[17–19] Indeed, through 99mTc-sestamibi imaging with SPECT/CT, we had located the unexpected SPA in suprasternal fossa and hyperplastic autograft of right forearm in present patient, and then the surgical resection was guided precisely. Lately, Thanseer et al[20] reported that compared with ultrasonography and 99mTc-sestamibi imaging with or without SPECT/CT, the 18F-fluorocholine positron emission tomography/CT imaging was superior for accurate preoperative localization of parathyroid adenomas, especially for ectopic or small parathyroid lesions.
It is well known the lesions responsible for persistent or recurrent renal SHPT are mainly the parathyroid autografts, as well as in some cases previously undetected residual or ectopic parathyroid glands, including SPGs.[6,7] Neyer et al[21] reported that intraoperative tissue selection with a stereomagnifier may help to identify autograft tissue with optimal functional characteristics and a low proliferative potential, thus minimizing the recurrence of hyperparathyroidism. Moreover, parathyroid scintigraphy may also help surgeons to choose the most appropriate gland to be partially preserved because the use of parathyroid tissue with high 99mTc-sestamibi uptake intensity might represent a higher risk of recurrence.[13] For our patient, the appropriate autograft tissue was chosen from the smallest parathyroid gland without intense radioactivity in initial surgery, but recurrence is still inevitable. In the last decade, some researchers thought that TPTX+FAT should be abandoned as a treatment of renal hyperparathyroidism, because of frequent recurrence.[8] Recently, a systematic review showed that alone TPTX was superior to TPTX+FAT, while referring to the rate of recurrent renal SHPT.[4] Even so, it needs to be further evaluated whether TPTX without FAT is a feasible alternative surgical option for the refractory renal SHPT.
SPGs are reported to be found in 13% of random autopsies, which can explain the postoperative persistence or recurrence of renal SHPT. Accordingly, 30% (87/290) of patients with renal SHPT presented SPGs during initial surgery and 32% (8/25) of reoperative patients with persistent or recurrent renal SHPT were attributed to SPGs.[22] Typically, Hines and Gordon[23] reported that a total of 8 parathyroid glands were removed in a patient with SHPT during 3 neck explorations over a 3-year period. The most common location of SPGs or ectopic parathyroid glands is the thymus.[24] The intrathymic parathyroid glands were resected in 44.5% (205/461) of patients with renal SHPT during initial surgery, which were ectopic in 181 (39.3%) and supernumerary in 30 patients (6.5%). The frequency of intrathymic SPGs was 7.4% (29/392) in permanent hemodialysis patients.[25] During reoperations, SPGs were also mainly found to be located in thymus, as well as retroesophageal grove, carotid sheath, and mediastinum. Therefore, thymectomy is essential in patients with fewer than 4 parathyroid glands identified at typical positions and can be recommended routinely in patients on permanent hemodialysis during the initial surgical exploration to prevent recurrences arising from anterior mediastinal glands.[22,24–26] Unfortunately, though total 4 parathyroid glands were removed, thymectomy was no performed in initial surgery in our patient, because of ignoring the fact that he had to receive permanent hemodialysis postoperatively, leading to SPA formation.
Although the common cause of recurrence involve in autografts or SPG, the recurrent renal SHPT caused by a coexisting of both them after TPTX+FAT is still very rare. To our best knowledge, only 3 cases (including present patient) were reported in the literature to date, and the SPG was located in the region of thymus in 2 cases of them.[17,27] Hindie et al[17] reported a 59-year-old woman with recurrent renal SHPT attributed to hyperplastic autografts and intrathymic SPG 16 years after TPTX+FAT and 4 years after autografts ablation. Yeh et al[27] reported a 42-year-old woman with rapidly recurrent renal SHPT originating from both multinodular hyperplastic autografts and residual parathyroid gland behind thyroid within 15 months after TPTX+FAT. It might be the major reasons for recurrent renal SHPT that autografts hyperplasia was simulated by the cumulative exposure to the uremic environment, including uremia itself and disorders of calcium, phosphate, or vitamin D metabolism under permanent hemodialysis after initial surgery in these patients, likewise for underlying SPG hyperplasia.[27]
4. Conclusion
Although rare, the recurrent renal SHPT may be caused by hyperplastic autograft coexisting with SPA after TPTX+FAT. The 99mTc-sestamibi parathyroid imaging with SPECT/CT is an useful modality for locating the culprits of recurrent renal SHPT before reoperation. To prevent recurrence of renal SHPT, the nowadays initial surgical procedures of parathyroidectomy should be further optimized in patient on permanent hemodialysis.
Author contributions
Conceptualization: Jun Zhang.
Data curation: Jun Yang, Dan Tian.
Writing – original draft: Jun Zhang.
Writing – review & editing: Meng-Jie Dong.
Footnotes
Abbreviations: iPTH = intact parathyroid hormone, SHPT = secondary hyperparathyroidism, SPA = supernumerary parathyroid adenoma, SPECT/CT = single positron emission tomography/computed tomography, SPG(s) = supernumerary parathyroid gland(s), TPTX+FAT = total parathyroidectomy with forearm autotransplantation.
JZ and M-JD have contributed equally to this work.
This work was supported by Zhejiang Province Medical Health Science Foundation (grant no. 2016KYB099).
The authors have no conflicts of interest to disclose.
References
- [1].Fraser WD. Hyperparathyroidism. Lancet 2009;374:145–58. [DOI] [PubMed] [Google Scholar]
- [2].Guideline Working Group JSFD. Clinical practice guideline for the management of secondary hyperparathyroidism in chronic dialysis patients. Ther Apher Dial 2008;12:514–25. [DOI] [PubMed] [Google Scholar]
- [3].Li JG, Xiao ZS, Hu XJ, et al. Total parathyroidectomy with forearm auto-transplantation improves the quality of life and reduces the recurrence of secondary hyperparathyroidism in chronic kidney disease patients. Medicine (Baltimore) 2017;96:e9050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].Liu ME, Qiu NC, Zha SL, et al. To assess the effects of parathyroidectomy (TPTX versus TPTX+AT) for secondary hyperparathyroidism in chronic renal failure: a systematic review and meta-analysis. Int J Surg 2017;44:353–62. [DOI] [PubMed] [Google Scholar]
- [5].Taieb D, Urena-Torres P, Zanotti-Fregonara P, et al. Parathyroid scintigraphy in renal hyperparathyroidism: the added diagnostic value of SPECT and SPECT/CT. Clin Nucl Med 2013;38:630–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Tominaga Y, Katayama A, Sato T, et al. Re-operation is frequently required when parathyroid glands remain after initial parathyroidectomy for advanced secondary hyperparathyroidism in uraemic patients. Nephrol Dial Transplant 2003;18suppl:i65–70. [DOI] [PubMed] [Google Scholar]
- [7].Yumita S. Intervention for recurrent secondary hyperparathyroidism from a residual parathyroid gland. Nephrol Dial Transplant 2003;18suppl:i62–4. [DOI] [PubMed] [Google Scholar]
- [8].Melck AL, Carty SE, Seethala RR, et al. Recurrent hyperparathyroidism and forearm parathyromatosis after total parathyroidectomy. Surgery 2010;148:867–73. discussion 873-5. [DOI] [PubMed] [Google Scholar]
- [9].Tominaga Y, Uchida K, Haba T, et al. More than 1,000 cases of total parathyroidectomy with forearm autograft for renal hyperparathyroidism. Am J Kidney Dis 2001;38:S168–71. [DOI] [PubMed] [Google Scholar]
- [10].Tominaga Y, Matsuoka S, Sato T. Surgical indications and procedures of parathyroidectomy in patients with chronic kidney disease. Ther Apher Dial 2005;9:44–7. [DOI] [PubMed] [Google Scholar]
- [11].Rodriquez JM, Tezelman S, Siperstein AE, et al. Localization procedures in patients with persistent or recurrent hyperparathyroidism. Arch Surg 1994;129:870–5. [DOI] [PubMed] [Google Scholar]
- [12].Palestro CJ, Tomas MB, Tronco GG. Radionuclide imaging of the parathyroid glands. Semin Nucl Med 2005;35:266–76. [DOI] [PubMed] [Google Scholar]
- [13].Taieb D, Hindie E, Grassetto G, et al. Parathyroid scintigraphy: when, how, and why? A concise systematic review. Clin Nucl Med 2012;37:568–74. [DOI] [PubMed] [Google Scholar]
- [14].Fuster D, Depetris M, Torregrosa JV, et al. Advantages of pinhole collimator double-phase scintigraphy with 99mTc-MIBI in secondary hyperparathyroidism. Clin Nucl Med 2013;38:878–81. [DOI] [PubMed] [Google Scholar]
- [15].Sandqvist P, Nilsson I, Grybäck P, et al. SPECT/CT's advantage for preoperative localization of small parathyroid adenomas in primary hyperparathyroidism. Clin Nucl Med 2017;42:e109–14. [DOI] [PubMed] [Google Scholar]
- [16].Heiba SI, Jiang M, Rivera J, et al. Direct comparison of neck pinhole dual-tracer and dual-phase MIBI accuracies with and without SPECT/CT for parathyroid adenoma detection and localization. Clin Nucl Med 2015;40:476–82. [DOI] [PubMed] [Google Scholar]
- [17].Hindie E, Zanotti-Fregonara P, Just PA, et al. Parathyroid scintigraphy findings in chronic kidney disease patients with recurrent hyperparathyroidism. Eur J Nucl Med Mol Imaging 2010;37:623–34. [DOI] [PubMed] [Google Scholar]
- [18].Arveschoug AK, Brochner-Mortensen J, Bertelsen H, et al. Supernumerary parathyroid glands in recurrent secondary hyperparathyroidism. Clin Nucl Med 2002;27:599–601. [DOI] [PubMed] [Google Scholar]
- [19].Thelen MH, Kuwert T, Lerch H, et al. Double-phase Tc-99m MIBI scintigraphy in secondary hyperparathyroidism relapsing after parathyroidectomy and removal of a parathyroid autograft. Clin Nucl Med 1996;21:609–11. [DOI] [PubMed] [Google Scholar]
- [20].Thanseer N, Bhadada SK, Sood A, et al. Comparative effectiveness of ultrasonography, 99mTc-Sestamibi, and 18F-fluorocholine PET/CT in detecting parathyroid adenomas in patients with primary hyperparathyroidism. Clin Nucl Med 2017;42:e491–7. [DOI] [PubMed] [Google Scholar]
- [21].Neyer U, Hoerandner H, Haid A, et al. Total parathyroidectomy with autotransplantation in renal hyperparathyroidism: low recurrence after intra-operative tissue selection. Nephrol Dial Transplant 2002;17:625–9. [DOI] [PubMed] [Google Scholar]
- [22].Pattou FN, Pellissier LC, Noel C, et al. Supernumerary parathyroid glands: frequency and surgical significance in treatment of renal hyperparathyroidism. World J Surg 2000;24:1330–4. [DOI] [PubMed] [Google Scholar]
- [23].Hines OJ, Gordon HE. Secondary hyperparathyroidism in a patient with eight parathyroid glands. J Clin Endocrinol Metab 1998;83:2384–6. [DOI] [PubMed] [Google Scholar]
- [24].Welch K, McHenry CR. The role of transcervical thymectomy in patients with hyperparathyroidism. Am J Surg 2012;203:292–5. discussion 295-6. [DOI] [PubMed] [Google Scholar]
- [25].Schneider R, Waldmann J, Ramaswamy A, et al. Frequency of ectopic and supernumerary intrathymic parathyroid glands in patients with renal hyperparathyroidism: analysis of 461 patients undergoing initial parathyroidectomy with bilateral cervical thymectomy. World J Surg 2011;35:1260–5. [DOI] [PubMed] [Google Scholar]
- [26].Boltz MM, Zhang N, Zhao C, et al. Value of prophylactic cervical thymectomy in parathyroid hyperplasia. Ann Surg Oncol 2015;22suppl:S662–8. [DOI] [PubMed] [Google Scholar]
- [27].Yeh C, Lin Y, Yang W, et al. Rapid recurrence of hyperparathyroidism from both nodularly hyperplastic autograft at forearm and residual tissues at neck after parathyroidectomy in a hemodialysis patient with calciphylaxis. Am J Med Sci 2006;331:284–7. [DOI] [PubMed] [Google Scholar]