

Abstract
Objectives
The aim of this paper is to construct a theoretical framework for information and communication technology (ICT)-enabled partnership towards diabetes management.
Design
We conducted an inductive case study and held interviews on the development and use of an artificial pancreas (AP) system for diabetes management.
Setting
The study was carried out in the Netherlands with users of an AP system.
Participants
We interviewed six patients with type 1 diabetes, five healthcare professionals (two medical specialists and three diabetes nurses), and one policy advisor from the Ministry of Health, Welfare and Sport.
Results
We built a new theoretical framework for ICT-enabled person-centred diabetes management, covering the central themes of self-managing the disease, shared analysing of (medical) data and experiencing the partnership. We found that ICT yielded new activities of data sharing and a new role for data professionals in the provision of care as well as contributed to carefree living thanks to the semiautomated management enabled by the device. Our data suggested that to enable the partnership through ICT, organisational adjustments need to be made such as the development of new ICT services and a viable financial model to support these services.
Conclusion
The management of diabetes through ICT requires an adjustment of the partnership between persons with the chronic condition and the healthcare professional(s) in such a way that the potential for self-managing the condition by analysing the newly available (medical) data (from the AP system) together leads to an experience of partnership between patients and healthcare professionals.
Keywords: ICT, ehealth, type 1 diabetes, chronic disease management, person-centred care
Strengths and limitations of this study.
The strength of the inductive case study approach is that it provides in-depth insights into how the partnership is shaped between a person with type 1 diabetes and the healthcare professional(s) as a result of the use of an artificial pancreas (AP) system for diabetes management.
Building theory from a case study, as we have done with our research, made it possible to create a theoretical framework from case-based empirical evidence.
Our findings should be considered in the context of our study design and may not be generalised to other AP systems nor long-term use of the AP system on a larger scale.
A possible limitation of this study is that the studied technology was under development during the research period; however, this is not a major limitation, as the focus of our study is not on the technology itself but on enabling the healthcare professional–patient partnership.
Introduction
Person-centred care (PCC) actively involves the patient in the care process as an equal partner in, and expert on, living with a chronic condition.1 Persons with a chronic condition have to make decisions on a day-to-day basis about self-managing their illness, which influences the healthcare professional–patient partnership with respect to care services.2 The partnership between patients and healthcare professionals involves sustaining the relationship via deciding on goals, care planning and documentation.3 Information and communication technology (ICT) for healthcare—also known as eHealth4—might support the professional–patient partnership in PCC services and provide chronic disease management in the face of social, physical and emotional challenges.5
ICT-enabled PCC
ICT is increasingly used within chronic disease management to document and exchange information, monitor and interact. The results of the first studies on ICT enabling PCC (ICT-PCC) in chronic care are promising, with improved clinical outcomes, better health-related quality of life and increased cost-effectiveness.6 However, there is a gap in knowledge how ICT shapes the professional–patient partnership when used in daily practice.
When applying the concept of partnership in PCC to ICT systems, the technology must be tailored to the needs of both patients and healthcare professionals (personalised ICT), whereby the personal context and situation of the patient informs and guides the decision-making on the care pathway.7 However, this phenomenon of enabling the partnership through ICT is not fully understood and insights are lacking on how this partnership is influenced and transformed through ICT.8 In this study, we selected a case in which an innovative ICT-enabled PCC intervention was used for diabetes management to better understand how ICT shaped the patient–professional partnership.9
Self-management of diabetes
Training in self-management of type 1 diabetes through personalised insulin treatment leads to significant improvements in treatment satisfaction, psychological well-being and quality of life measures.10 Even though diabetes management has improved considerably over the years, patients still suffer from short-term complications such as hypoglycaemia (‘hypo’ for short) and hyperglycaemia (‘hyper’) progressing to diabetic ketoacidosis and hyperosmolar hyperglycaemic syndrome, and long-term complications such as retinopathy, neuropathy, cardiovascular disease and nephropathy that could lead to complications such as loss of eyesight and amputation.11
The treatment and care of patients with diabetes have seen fast progress and key innovations after the discovery of insulin in 1921: engineered insulin, the introduction of blood glucose monitoring by telemonitoring systems, internet applications and mobile devices.12 In addition, smart algorithms to control the blood glucose level have been developed.13 This innovation trajectory of applying smart algorithms to earlier discoveries culminated in the development of a first-generation system of an artificial pancreas (AP) that focuses on preventing unsafe blood sugar levels and aims to control blood glucose around a target of 120 mg/dL (=6.7 mmol/L).14
ICT interventions for diabetes management
Several companies worldwide are developing AP systems to regulate basal insulin delivery, by taking over the regulation of the glucose levels completely through automating insulin—and still in a development stage, also glucagon—delivery.15–18 Over the last years, significant progress has been made in AP development,19 and researchers have demonstrated the safety and feasibility of different AP systems in clinical research settings and more recently in outpatient ‘real-world’ environments.20 21 Most of the studies are about developing AP systems that would still require user entry of carbohydrate intake (hybrid closed -loop systems). Several meta-analyses focused on AP performance across different studies, and concluded that artificial pancreas systems could be an efficacious and safe approach for treating patients with type 1 diabetes.22–25 The greatest benefits of the AP are the reduced burden of diabetes management during the day, and improved overnight control of glucose levels thanks to reduced glycaemic variability, improved time in target range and reduced risk of nocturnal hypoglycaemia.26–28 Although AP users with type 1 diabetes will still need to self-manage their illness, a closed -loop system with data acted on by the users could reduce the burden.29
We chose to employ an inductive case study to focus on the dynamics of the patient–professional partnership shaped through an ICT intervention used in practice for the management of type 1 diabetes, namely an AP system. The case study was applied to answer the research question: How does ICT enable the partnership between healthcare professional(s) and the patient in chronic disease management?
Methods
Study design
We conducted an inductive case study30 and held in-depth interviews with both healthcare professionals and patients on their use of the AP system. This case study looks in particular into the dynamics of the professional–patient partnership and between different healthcare professionals, the patient experience, and how introducing ICT enables a person-centred approach to diabetes care.
Case study
We used as a case an AP system, that at the time of the study was only tested in the Netherlands. The system automatically controls the blood glucose level of patients with type 1 diabetes, and provides the substitute functionality of both insulin and glucagon delivery of a healthy pancreas. The AP system maintains the blood glucose levels in the healthy range most of the time, without restrictions with respect to factors such as diet and exercise.
The development of the person-centred AP system was started in 1994 in the Netherlands by a person who himself had been diagnosed with type 1 diabetes. His motivation for inventing a semiautonomous AP was driven by his dissatisfaction with the diabetes care treatment and the support provided with products and software applications. He started a company to develop the AP in an iterative manner, involving the users in the different steps of its development. The AP system has been described in detail by Blauw and the research group Portable bihormonal Closed Loop for Diabetes.31
Device characteristics
The wearable AP integrates the following features into one device: (i) continuous glucose monitoring (CGM); (ii) glucose control algorithms (decision-making processor); (iii) infusion pump and (iv) other sensors (see figure 1).
Figure 1.
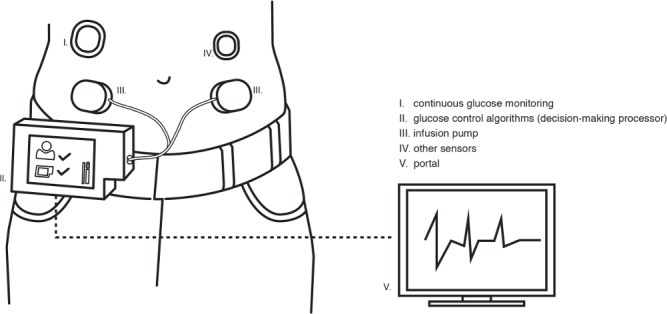
Components of the artificial pancreas system.
The control unit (i+ii) replaces human decision-making and makes more frequent dose adjustments than a person could. The AP device transmits data to a database that is accessible via a portal (v) featuring web services for monitoring.
The functions of the bihormonal AP (both insulin and glucagon) were tested with persons with type 1 diabetes in home treatment; the results indicated that the AP provided better glucose control than traditional insulin pump therapy and that the treatment is safe.32 Related studies also indicated that patients anticipate that they will accept the device33 and that for further technical development it will feature adaptive control.34
Participants
The participants were selected in the Netherlands via a combination of purposive and snowball sampling. With purposive sampling, we initially selected two types of participants, persons with type 1 diabetes and healthcare professionals who had used the AP and would potentially be able to provide rich, relevant and diverse data pertinent to the ICT enabling of the partnership.35 36 Subsequently, through snowball sampling—in which interviewees identified further participants—we recruited both persons with type 1 diabetes and healthcare professionals (medical specialists and trained diabetes nurses) with knowledge relevant to the case study, and a policy advisor.
We approached the participants via telephone, email and/or face-to-face. We sent an information letter by email with an introduction to and information about the case study, and an invitation to participate. The principal researcher introduced the study orally, stressing the person’s right to make their own choice to participate.
We interviewed 12 Dutch participants: six persons with type 1 diabetes, five healthcare professionals (two medical specialists; one paediatrician-endocrinologist and one internist-endocrinologist, three diabetes nurses), and one policy advisor from the Ministry of Health, Welfare and Sport was included because of his experience with the embedding of the AP in the healthcare context.
Four attempts to recruit specific participants were rejected. One participant indicated he was too busy while the other reasons for non-participation were that the participants2 were not familiar with the AP or the subject was too sensitive (policymaker).
Patient and public involvement
The study was designed to understand the prespectives of the participants to gain access to their experiences, feelings and preferences with the use of an AP, of patients diagnosed with type 1 diabetes and others.37 The research question was developed in an iterative manner, and based on patients’ and healthcare professionals’ insights. The AP was chosen as a case study since it was a patient-driven innovation, developed by a person who was diagnosed with type 1 diabetes himself. Patients were involved in the different phases of the study, and recruited through snow ball sampling, in which participants also supported in recruiting (other) patients.
Data collection
We held in-depth, semistructured interviews with the participants. These interviews were guided by an interview protocol, with questions focusing on the overall experience with AP in clinical practice and how the AP supported and changed the professional–patient partnership in diabetes management. The interview protocol was provided in Dutch, and is available on request.
The first author conducted the interviews via telephone/Skype or FaceTime, either at home or at work. One participant was known from a previous study. No non-participants were present during the interviews. The interviews were conducted between February and April 2017. The interviews lasted between 47 and 73 minutes. Participants were recruited until no new knowledge was gained (data saturation).38 No repeat interviews were conducted. The researcher audio-recorded the participants and took notes. We transcribed all interviews. We anonymised the data and allocated alphabet capital coding to each participant.
Analysis
In this study, we used thematic analysis to identify patterns within the data, and grouped them under codes, categories and themes, whereby we particularly sought to identify how ICT supported the partnership in diabetic/chronic disease management.39 The first two authors analysed the data in an iterative process of coding and use of NVivo software, V.12.2.0.
We started with a line-by-line coding that was derived from the research question. We processed the coding by reading and analysing the data—in which we preserved (inter-)actions using as many gerunds (‘ing’) as possible.40 The first and second authors reviewed the codes. After that, through focused coding, we organised and grouped the coded data that shared characteristics into categories.
In this phase, we left out codes that did not contribute to answering the research question from further analysis (such as data on specific treatment for children). We then moved to the process of theoretical coding—in which we clustered the categories into themes—to build a theoretical framework.
Ethical considerations
The study was approved by the researchers’ host institute. All participants, prior to the interviews, agreed to participate. Participation was voluntary and participants could withdraw at any point. The research complied with the Helsinki Declaration of the World Medical Association (2013). In our sample design, we excluded the participation of vulnerable groups. The topic of our study was not sensitive. The researchers did not use or have access to personal information or datasets; they also neither collected nor used bodily material. All personal information was de-identified. We did not ask participants for private information or experiences. The quotes chosen were sufficiently general to preclude identification of individual participants.
Results
Our analysis yielded three themes of ICT-enabled PCC towards diabetes management resulted from our analysis: self-managing the disease (I); shared analysing of (medical) data (II) and experiencing the partnership (III) (see the theoretical framework in figure 2).
Figure 2.

Theoretical framework of ICT enabling partnership in person-centred diabetes management. ICT, information and communication technology.
These three themes were based on five categories that shared characteristics resulting from 10 codes originated from the research question.
Self-managing the disease
The theme self-managing the disease indicates that the use of the AP system contributes to a substantial increase in quality of life thanks not only to the device, which takes over control of the disease (234 quotes), but also insights based (medical) data (46 quotes) that is linked to the new activity of (medical) data sharing (see figure 2).
Quality of life
Users of the AP system commonly mentioned (21 quotes) that the ICT application offers the next level of treatment for persons with diabetes, enabling carefree living that adds to their quality of life.
If you do not have to measure five times a day, but you can just let the device do its job, that’s a huge improvement for me. […] That may seem like a very small thing for healthy people, but it is, when you have diabetes, a huge boost to your quality of life, enabling you to lead a ‘normal’ life. (Person with diabetes D)
This increased quality of life is linked to the technological advancement of the AP system that takes over the activities of controlling the disease through continuously sensing measurements and algorithms. The AP semiautomates the management of diabetes by monitoring the condition and regulating the insulin and glucagon supply accordingly, giving the patient new data overviews to manage his or her condition.
(Medical) data sharing
What will change the partnership is the self-management of diabetes, which is enriched through the sharing of (medical) data among medical specialists, diabetes nurses, patients and the intelligent device professional.
I have given permission to my diabetic nurse to look into my data. How often do you do that? Well, if I go through a period of an illness, like the flu, then maybe every week. If things go well, maybe once every two months. (Person with diabetes D)
The introduction of the intelligent device (AP system) initiates a constant flow of (medical) data—physiological measurements and personal data—that is accessible through a portal (see figure 1). The new activity of (medical) data sharing is fuelled by gaining insight into (medical) data. If we stand back, we can see that the presence of an intelligent device professional changes the partnership between the healthcare professionals and the person with diabetes. Thus, the introduction of ICT could enable the (experience of the) partnership and the self-management of a disease, but it also introduces new demands on healthcare professionals, including the provision of ICT (device) support.
Shared analysing of (medical) data
The second theme, shared analysing of (medical) data, reveals the new activity in the partnership of (medical) data sharing when the ICT device is embedded in the organisation (see figure 2). This sharing of (medical) data relates to the configuring, functioning and maintaining of the device (133 quotes) and the insights in (medical) data gained through the device (46 quotes). A diabetic nurse described the data sharing as follows:
So, you can watch the person over distance. But it is not our intention to watch patients 24/7. (Diabetic nurse C)
For an eHealth service enabling the partnership, both healthcare professionals and patients need to be supported by intelligent device professionals. To enable both patients and the healthcare professional(s) to share data from the AP and to gather data and then to store, retrieve and analyse it, the technology and its data must be embedded in the organisation (see figure 2).
And of course you should also start looking at your organisation again. How do you organise this? A lot is already done digitally in the hospital, but this does not link with our system. And this type of support from the hospital has not been allocated any funding yet. So, yes, there will also be stuff that has to do with the embedding [of the device] in the organisation. (Diabetic nurse C)
This organisational embedding of the intelligent device should be linked to the organisation of ICT in the hospital setting (13 quotes), and should be supported by the setting up of a financial model (105 quotes) that allows the insights gained from the (medical) data (46 quotes) to support the professional–patient partnership (see figure 2). The introduction of the AP system could thereby potentially lead to the availability of new and rich(er) data that could be shared among the person with diabetes and the healthcare professionals and enable treatment improvements in diabetes management.
Experiencing the partnership
How the partnership is experienced is based on the reciprocity in contact, the trust in technology, (medical) data sharing and the quality of life (see figure 2).
Reciprocity in contact
Reciprocity in contact is linked to how the person with diabetes communicates with his or her medical specialist (108 quotes), diabetic nurse (51 quotes) and the intelligent device professional (18 quotes), and the other way around.
We will head towards more equal care, I think. At least, if the patient wants that too. (Medical specialist B)
The AP technology in use revealed different intensities of how the partnership was experienced by both the patient and the healthcare professionals. On the one hand, the interviewees foresaw a change in the moments of contact with the medical specialist.
Once the AP system is well integrated into health care – I do not have the illusion that it heals people – the treatment is such that medical specialists can provide far less guidance [to patients]. (Person with diabetes A)
On the other hand, they expected that the partnership with the diabetic nurse would become more intensive, as was already experienced with the insulin pump:
You actually see that when you make the switch from syringe to pump. Then suddenly the contact with the diabetic nurse becomes much more intensive and more accessible and then you can suddenly call outside office hours. (Person with diabetes B)
Diabetes nurses anticipate a change in the partnership with the person with diabetes as a result of implementing the AP.
I tell my patients they do not have to come see me every 3 months when there is no direct need. What matters is that the person with diabetes is doing well and if that is the case, I do not see what I could improve. (Diabetic nurse B)
The initiative for treatment can thus be initiated through the data instead of through existing care pathways.
The fear that healthcare professionals would become unnecessary is baseless:
In the case of the artificial pancreas, I do not expect that suddenly a whole group of healthcare professionals no longer have to come to the hospital because the technology takes over. They have enough other things to do. (Policy maker)
The findings also reveal another role in the partnership, namely the communication with the intelligent device professional (18 quotes) with whom patients or the healthcare professionals communicate about the technical part of the AP.
If you do not have a psychological problem and if your diabetes does not bother you, if your parameters are all right and well-regulated through the AP system, you see each other less often so the consultation is purely problem-oriented. When it is a technical issue, then the device is at fault and you contact the AP professional. The partnership will change towards shorter duration and interventions. If it is not going well, what is going on? (Medical specialist B)
How the partnership is experienced depends also on the configuration, functioning and maintenance of the intelligent device (133 quotes). When the person with diabetes checks the ICT technology (verifying that it has enough insulin and glucagon, the battery and sensors are OK, etc), and he or she notices that the system is not working properly, then communication with the intelligent device professional (18 quotes) is necessary to make sure that the device is technically in working order.
Trust in technology
The experience of the partnership, supported through ICT, was also connected with the category of trust in technology (see figure 2). The trust in technology was vividly described by one of the patients:
You are busy with the management of diabetes all day. If that is no longer the case, and you have trust in the technology to take over the management of the disease and that you do not have to think for yourself anymore; that gives a lot of freedom. (Patient B)
Trust in technology is related to the feeling of carefree living (21 quotes), the configuring, functioning and maintaining of the intelligent device (133 quotes), the acceptance of the intelligent device (14 quotes) and communication with the intelligent device professional (18 quotes).
(Medical) data sharing
The sharing of data has influence on how the partnership is experienced, and how patients communicate with healthcare professionals. However, the AP does not cure the disease so yearly check-ups will still be necessary.
Look, the patient still has to see his medical specialist every year. He remains responsible and needs to check certain parameters. That still has to be done because the patient still has diabetes. Even if the patient is doing well, he or she is not cured.’\ (Diabetic nurse B)
Both healthcare professionals and patients foresee that the self-management options ushered in by the AP system will result in a change in the partnership.
Quality of life
The outcomes expose that the experience of the partnership is linked to the quality of life, which increased when the intelligent device took over the daily controlling of the disease and reduced the feeling of stress involved in self-managing diabetes (see figure 2).
The most important thing for patients is that they do not have to be busy with their condition all day long. So, a bit of freedom and being able to enjoy a cup of coffee without having to do all kinds of measurements and so forth. For the simple things that are important for daily life. That is the benefit of the artificial pancreas. (Person with diabetes A)
Or as a medical specialist framed it:
If you still want to get a lot out of this life as a child, adolescent, young or older adult, you obviously gain a lot when using the AP. It is just great if you do not have to think about diabetes all the time. (Medical specialist A)
The AP replaces human decision-making, which the participants experience as carefree living because they no longer have to make dose adjustments all the time.
How persons experience the partnership varies in extent from patient to patient, but patterns can be discerned. At one end stands the person with diabetes who completely trusts the technology, allowing to take over the function of the pancreas and automatically manages the glucose levels. Such a person thus feels that he or she no longer requires the help of a medical specialist. At the other end stands the person with diabetes who just wants his healthcare professionals to take over. Therefore, the interaction between the technology and social components must also be considered (see figure 3).
Figure 3.

Partnership enabled through ICT (Artificial Pancreas system).
The introduction of ICT simultaneously changes the partnership interaction between healthcare professionals and persons with a chronic condition, strengthens the interests of the patient (self-managing the disease) and yields precise analysed data on the clinical phenomenon (see figure 3).
Discussion
Principal findings
The aim of our study was to answer the research question: How does ICT enable the partnership between healthcare professional(s) and the patient in chronic disease management? Building on the analysis of in-depth qualitative data, this inductive study has revealed three interrelated themes of ICT-enabled PCC towards diabetes management namely self-managing the disease, shared analysing of (medical) data and experiencing the partnership. We found that ICT yielded new activities of data sharing and a new role for data professionals in the provision of care as well as contributed to carefree living thanks to the semiautomated management enabled by the device. Our data suggest that to enable the partnership through ICT, organisational adjustments need to be made such as the development of new ICT services and a viable financial model to support these services.
In a recent study, it was concluded that ICT offers a viable environment to deliver PCC through ICT for patients with chronic conditions.8 However, to maximise the potential of ICT to enable patients to manage their condition, there is a need to integrate PCC principles into ICT and its organisation. These principles have been worked out in determining the preconditions for ICT-enabled PCC.7 Our study adds to the existing knowledge base with its finding that developing PCC preconditions to enable chronic disease management is just one step, and that the three defined themes are another input for ICT-enabled PCC-principles towards chronic disease management.
The introduction of a new theoretical framework provides insight into the dynamics of how the partnership between healthcare professionals and persons with a chronic disease is enabled through ICT in chronic disease management of diabetes (see figure 2). The three themes entail reordering the partnership between the person with diabetes, the internist, the diabetic nurse and the intelligent device professional. Thus, the partnership interaction between healthcare professionals and persons with a chronic condition simultaneously changes the partnership, strengthens the interests of the patient (self-management) and yields precise data on the clinical phenomenon (see figure 3). This multinodal system is more complex than either the patient–technology or patient–professional relationship alone. Therefore, the outcomes are less predictable and neglecting to consider the variation in the reactions of patients to the now more complicated entry points into the professional system, which can also lead to overestimation of the potential of disease self-management.
Over the last years, a growing body of scholarly work has been focusing on the use of (semi-)automated devices for diabetes management.14 15 The results of, for example, CGM systems and automated insulin delivery systems are promising in showing the benefits for type 1 diabetes by improving glycaemic control through personalised models of predictive control.17 18 Furthermore, researchers have demonstrated the safety and feasibility of different AP systems in clinical research settings and more recently in outpatient ‘real-world’ environments.20 21 In addition to these feasibility-focused and efficacy-focused studies on (semi-)automated devices for diabetes management, also the experiences of patients using these type of devices have been studied. A previous study on perspectives of experienced users of hybrid closed-loop systems among people with diabetes reported how context-level, system-level and person-level factors influenced patients’ trust in an AP system.41 Tanenbaum et al 41 concluded that when patients lacked trust in the system, they made an attempt to override the system, while trusting the system decreased stress and also decreased self-management burdens, which in our study was described by the participants as carefree living.
Additionally, a recent study highlighted the findings that acceptance of an AP system depends more on a stronger bond of the users with product characteristics (such as usefulness, complexity and compatibility) than technology readiness (such as innovativeness and insecurity).42 However, the researchers also concluded that the results differed between self-selected and invited persons, so researchers and product developers should be cautious when relying only on self-selected persons in the design, testing and development of AP systems. While the experiences and acceptance of AP systems have been the focus of some studies, further research directions on patient experiences will yield a better understanding what factors influence the acceptance of such automated technology. Our study suggests to take the healthcare professional–patient partnership into account as one of the factors that affect the acceptance and the use of AP systems.
Strengths and limitations
The strength of the inductive case study approach is that we were able to gain detailed insight into how the characteristic of the partnership changed between a person with type 1 diabetes and the healthcare professional(s) as a result of the use of ICT. A case study enables the creation of a comprehensive theoretical framework built on the details of a particular case.30 43 The development of this theoretical framework increases the understanding of person-centred healthcare and ICT-enabled health services that can have implications for practice.44
Through qualitative research, we delved into the anecdotal evidence of the interviews and used coding to show commonalities in the changes that the interviewees expected, through which we were able to build a framework that broadens the scope of evidence-based medicine; good evidence goes further than the results of meta-analysis of randomised controlled trials.45
We also acknowledge limitations of the study. Our findings should be considered in the context of our study design. One of the inclusion criteria to participate in the study was experience with an AP system. This system was tested as part of a separate trial during which the participants were closely monitored by clinical researchers. The use of the system was reduced to a relatively short duration. Therefore, the results may not be generalised to other AP systems nor to a long-term use of the system on a larger scale.
Furthermore, to study the partnership between patients and healthcare professionals in chronic disease management, we chose an ICT application—the AP system—that is still under development and was not as yet available on the market during the research period. However, since our focus is neither on the technology itself nor its acceptance, but on the enabling of the partnership, the case study does add to our knowledge on ICT in partnership and service provision based on digital healthcare applications.
Implications for practice and research
In order for ICT to take over the burden of self-managing disease through shared (medical) data analysis, it is necessary to embed ICT services and professions in the healthcare organisation. The introduction of ICT introduces new demands on healthcare professionals and patients, influencing how the partnership is experienced.
In addition, when introducing ICT in a healthcare context, the technology should be studied as part of a dynamic and networked healthcare environment, the so-called ‘fourth-generation studies’46 and should take a participatory development approach to guide the development, implementation and evaluation of eHealth technologies and interventions.47 Our study suggests that these types of studies should also include a focus on the partnership and how this is reshaped by the introduction of ICT. The results of our study show that to support the partnership in a sustainable manner, ICT needs to be embedded in healthcare organisations. As a result, the care pathways also need to be redesigned so we can move towards person-centred chronic disease management, offering treatment ‘when needed, where needed’ based on the availability of rich data generated by an ICT system.
Previous research has pointed to the fact that human connectedness provides the necessary conditions for communication and cooperation on which formal relations of partnership can be constructed.1 3 Our study shows that introducing an ICT-enabled PCC solution structures an integrated form of professional–patient connectedness. The self-management of the disease, but also the analysis of (medical) data and the experience of the partnership, shift the focus of professional–patient connectedness from the medical specialist to the diabetic nurse. New roles take shape such as the one of the intelligent device professional, and a different network will (have to) evolve around the patient. One of the lessons could be that it becomes more important to look at the personal progression of the disease in addition to following the existing rigid care pathways.
The expected changes in the role of healthcare professionals as a result of introducing ICT-enabled PCC towards chronic disease self-management must be addressed with the design of a new care model integrating the changing partnership. The next steps should be to study how to design care models that fit this changingpartnership as a result of ICT-enabled PCC, and how a sustainable financial model should be determined for ICT-enabled person-centred chronic disease management.
Conclusion
The management of diabetes through ICT requires an adjustment of the partnership between persons with the chronic condition and the healthcare professional(s) in such a way that the potential for self-managing the condition by analysing the newly available (medical) data (from the intelligent device AP system) together leads to an experience of partnership between patients and healthcare professionals.
Supplementary Material
Acknowledgments
The authors thank all the interviewees who participated in this study for their contribution. We like to thank Sanne Muiser for the graphic design of figures 1 and 3.
Footnotes
Contributors: SEW conceived the presented idea. SEW, LWLS and PG developed the theory. SEW wrote the interview protocol that was checked by authors PG and AK. SEW conducted the interviews, had them transcribed and checked them. SEW and LWES analysed the data in iterative steps, which was supervised - including the methodology by PG and AK. SEW and LWLS took the lead in writing the manuscript. PG and AK supervised the findings of this study. All authors take responsibility for the content. They all have contributed to the development of the research question, the conducted research and the reported results. All authors provided critical feedback and helped shape the final manuscript.
Funding: This work was supported by the Foundation for Prevention, Early Diagnostics, and E-health (PVE), a Brocher Foundation residency, and NWO KIEM.
Competing interests: None declared.
Provenance and peer review: Not commissioned; externally peer reviewed.
Data sharing statement: Data will not be made publicly available. For more information, please contact the corresponding author.
Patient consent for publication: Not required.
References
- 1. Ekman I, Swedberg K, Taft C, et al. Person-centered care-ready for prime time. Eur J Cardiovasc Nurs 2011;10:248–51. 10.1016/j.ejcnurse.2011.06.008 [DOI] [PubMed] [Google Scholar]
- 2. Bodenheimer T, Lorig K, Holman H, et al. Patient self-management of chronic disease in primary care. JAMA 2002;288:2469–75. 10.1001/jama.288.19.2469 [DOI] [PubMed] [Google Scholar]
- 3. Wolf A, Moore L, Lydahl D, et al. The realities of partnership in person-centred care: a qualitative interview study with patients and professionals. BMJ Open 2017;7:e016491 10.1136/bmjopen-2017-016491 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Eysenbach G. What is e-health? J Med Internet Res 2001;3:e20 10.2196/jmir.3.2.e20 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Huber M, Knottnerus JA, Green L, et al. How should we define health? BMJ 2011;26:343 10.1136/bmj.d4163 [DOI] [PubMed] [Google Scholar]
- 6. Wildevuur SE, Simonse LW. Information and communication technology-enabled person-centered care for the "big five" chronic conditions: scoping review. J Med Internet Res 2015;17:e77 10.2196/jmir.3687 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Wildevuur SE, Thomese GCF, Ferguson JE. & Klink A. Information and communication technologies to support chronic disease self management: Preconditions for enhancing the partnership in person-centred care. J Particip Med 2017;9:e12 10.2196/jopm.8846 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Heckemann B, Wolf A, Ali L, et al. Discovering untapped relationship potential with patients in telehealth: a qualitative interview study. BMJ Open 2016;6:e009750 10.1136/bmjopen-2015-009750 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Eisenhardt KM. Building theories from case study research. Academy of management review 1989;14:532–50. [Google Scholar]
- 10. DAFNE Study Group. Training in flexible, intensive insulin management to enable dietary freedom in people with type 1 diabetes: dose adjustment for normal eating (DAFNE) randomised controlled trial. BMJ 2002;325:746–9. 10.1136/bmj.325.7367.746 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. McKnight JA, Wild SH, Lamb MJ, et al. Glycaemic control of Type 1 diabetes in clinical practice early in the 21st century: an international comparison. Diabet Med 2015;32:1036–50. 10.1111/dme.12676 [DOI] [PubMed] [Google Scholar]
- 12. Atkinson MA, Eisenbarth GS. Type 1 diabetes: new perspectives on disease pathogenesis and treatment. Lancet 2001;358:221–9. 10.1016/S0140-6736(01)05415-0 [DOI] [PubMed] [Google Scholar]
- 13. Doyle FJ, Huyett LM, Lee JB, et al. Closed-loop artificial pancreas systems: engineering the algorithms. Diabetes Care 2014;37:1191–7. 10.2337/dc13-2108 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Garg SK, Weinzimer SA, Tamborlane WV, et al. Glucose outcomes with the in-home use of a hybrid closed-loop insulin delivery system in adolescents and adults with type 1 diabetes. Diabetes Technol Ther 2017;19:155–63. 10.1089/dia.2016.0421 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Kropff J, DeVries JH. Continuous glucose monitoring, future products, and update on worldwide artificial pancreas projects. Diabetes Technol Ther 2016;18(S2):S2-53–63. 10.1089/dia.2015.0345 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Trevitt S, Simpson S, Wood A. Artificial pancreas device systems for the closed-loop control of type 1 diabetes: What systems are in development? J Diabetes Sci Technol 2016;10:714–23. 10.1177/1932296815617968 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Buckingham BA, Christiansen MP, Forlenza GP, et al. Performance of the omnipod personalized model predictive control algorithm with meal bolus challenges in adults with type 1 diabetes. Diabetes Technol Ther 2018;20:585–95. 10.1089/dia.2018.0138 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Forlenza GP, Li Z, Buckingham BA, et al. Predictive low-glucose suspend reduces hypoglycemia in adults, adolescents, and children with type 1 diabetes in an at-home randomized crossover study: Results of the PROLOG trial. Diabetes Care 2018;41:2155–61. 10.2337/dc18-0771 [DOI] [PubMed] [Google Scholar]
- 19. NIHR Horizon Scanning Centre. Artificial pancreas device systems in development for the closed-loop control of type 1 diabetes. University of Birmingham 2015. [Google Scholar]
- 20. Kowalski A. Pathway to artificial pancreas systems revisited: moving downstream. Diabetes Care 2015;38:1036–43. 10.2337/dc15-0364 [DOI] [PubMed] [Google Scholar]
- 21. Breton MD, Cherñavvsky DR, Forlenza GP, et al. Closed-loop control during intense prolonged outdoor exercise in adolescents with type 1 diabetes: The artificial pancreas ski study. Diabetes Care 2017;40:1644–50. 10.2337/dc17-0883 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Bekiari E, Kitsios K, Thabit H, et al. Artificial pancreas treatment for outpatients with type 1 diabetes: systematic review and meta-analysis. BMJ 2018;361:1310 10.1136/bmj.k1310 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Boughton CK, Hovorka R. Is an artificial pancreas (closed-loop system) for Type 1 diabetes effective? Diabet Med 2019;36:279–86. 10.1111/dme.13816 [DOI] [PubMed] [Google Scholar]
- 24. Dai X, Luo ZC, Zhai L, et al. Artificial pancreas as an effective and safe alternative in patients with type 1 diabetes mellitus: A systematic review and meta-analysis. Diabetes Ther 2018;9:1269–77. 10.1007/s13300-018-0436-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Weisman A, Bai JW, Cardinez M, et al. Effect of artificial pancreas systems on glycaemic control in patients with type 1 diabetes: a systematic review and meta-analysis of outpatient randomised controlled trials. Lancet Diabetes Endocrinol 2017;5:501–12. 10.1016/S2213-8587(17)30167-5 [DOI] [PubMed] [Google Scholar]
- 26. Bergenstal RM, Garg S, Weinzimer SA, et al. Safety of a hybrid closed-loop insulin delivery system in patients with type 1 diabetes. JAMA 2016;316:1407–8. 10.1001/jama.2016.11708 [DOI] [PubMed] [Google Scholar]
- 27. Castle JR, Engle JM, El Youssef J, et al. Novel use of glucagon in a closed-loop system for prevention of hypoglycemia in type 1 diabetes. Diabetes Care 2010;33:1282–7. 10.2337/dc09-2254 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Hovorka R, Allen JM, Elleri D, et al. Manual closed-loop insulin delivery in children and adolescents with type 1 diabetes: a phase 2 randomised crossover trial. Lancet 2010;375:743–51. 10.1016/S0140-6736(09)61998-X [DOI] [PubMed] [Google Scholar]
- 29. Waugh N, Adler A, Craigie I, et al. Closed loop systems in type 1 diabetes. BMJ 2018;361:k1613 10.1136/bmj.k1613 [DOI] [PubMed] [Google Scholar]
- 30. Eisenhardt KM, Graebner ME. Theory building from cases: Opportunities and challenges. Acad Manage J 2007;50:25–32. 10.5465/amj.2007.24160888 [DOI] [Google Scholar]
- 31. Blauw H, van Bon AC, Koops R, et al. Performance and safety of an integrated bihormonal artificial pancreas for fully automated glucose control at home. Diabetes Obes Metab 2016;18:671–7. 10.1111/dom.12663 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Blauw H, Keith-Hynes P, Koops R, et al. A review of safety and design requirements of the artificial pancreas. Ann Biomed Eng 2016;44:3158–72. 10.1007/s10439-016-1679-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. van Bon AC, Brouwer TB, von Basum G, et al. Future acceptance of an artificial pancreas in adults with type 1 diabetes. Diabetes Technol Ther 2011;13:731–6. 10.1089/dia.2011.0013 [DOI] [PubMed] [Google Scholar]
- 34. Boiroux D, Duun-Henriksen AK, Schmidt S, et al. Adaptive control in an artificial pancreas for people with type 1 diabetes. Control Eng Pract 2017;58:332–42. 10.1016/j.conengprac.2016.01.003 [DOI] [Google Scholar]
- 35. Holloway I. Galvin K. Qualitative research in nursing and healthcare. Blackwell: Oxford, 2016. [Google Scholar]
- 36. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care 2007;19:349–57. 10.1093/intqhc/mzm042 [DOI] [PubMed] [Google Scholar]
- 37. Fossey E, Harvey C, McDermott F, et al. Understanding and evaluating qualitative research. Aust N Z J Psychiatry 2002;36:717–32. 10.1046/j.1440-1614.2002.01100.x [DOI] [PubMed] [Google Scholar]
- 38. Guest G, Bunce A. & Johnson L. How many interviews are enough? An experiment with data saturation and variability. Field Methods 2006;18:59–82. [Google Scholar]
- 39. Fereday J, Muir-Cochrane E. Demonstrating rigor using thematic analysis: a hybrid approach of inductive and deductive coding and theme development. Int J Qual Methods 2006;5:80–92. 10.1177/160940690600500107 [DOI] [Google Scholar]
- 40. Charmaz K, Belgrave LL. Grounded theory. Wiley Online Library 2015. [Google Scholar]
- 41. Tanenbaum ML, Iturralde E, Hanes SJ, et al. Trust in hybrid closed loop among people with diabetes: Perspectives of experienced system users. J Health Psychol 2017. 10.1177/1359105317718615 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Oukes T, Blauw H, van Bon AC, et al. Acceptance of the artificial pancreas: Comparing the effect of technology readiness, product characteristics, and social influence between invited and self-selected respondents. J Diabetes Sci Technol 2019. 10.1177/1932296818823728 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Yin RK. Case study research: Design and methods. London: Sage publications, 2013. [Google Scholar]
- 44. Green J, Thorogood N. Qualitative methods for health research. London: Sage Publications, 2018. [Google Scholar]
- 45. Green J, Britten N. Qualitative research and evidence based medicine. BMJ 1998;316:1230–2. 10.1136/bmj.316.7139.1230 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Greenhalgh T, Shaw S, Wherton J, et al. SCALS: a fourth-generation study of assisted living technologies in their organisational, social, political and policy context. BMJ Open 2016;6:e010208 10.1136/bmjopen-2015-010208 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. van Gemert-Pijnen J, Kip H, Kelders SM, et al. eHealth Research, Theory and Development: A Multi-Disciplinary Approach. London: Routledge, 2018. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.