

Abstract
The aim of this report is to present a case of a patient with a recurrent nasal cavity amelanotic melanoma (AM), with emphasis on diagnosis and therapy options of this clinical entity. A 65-year-old female patient presented with pain in the right cheek region and nasal obstruction. In 2013, she was diagnosed with mucosal melanoma (MM) of the left nasal cavity. After endoscopic surgery and radiotherapy, the patient was followed by the oncology team. Five years after the initial diagnosis, rhinoscopy showed a tumorous formation in the right nasal cavity. The tumor mass was without black discoloration and was the same color as the surrounding nasal mucosa. Microscopic examination after biopsy of the tumor confirmed amelanotic MM. The patient underwent an additional endoscopic surgery. A complete standard diagnostic workup for MM found metastases in head and neck lymph nodes, on both sides. MMs of head and neck are uncommon malignancies. Unique biology of MM cells causes a high rate of recurrences. This report presents an example of recurrent AM of the nasal cavity, in treatment with checkpoint inhibitor (pembrolizumab), which could provide a good therapy option for patients with MM.
Key words: Amelanotic melanoma, Nasal cavity, Mucosal melanoma, Immunotherapy, Radiotherapy
Introduction
Malignant transformation of melanocytes is the first step in the development of malignant melanoma. Melanocytes, pigment – producing cells migrate from the neural crest to the skin, mucous membranes, upper esophagus, eyes, and meninges. Cells in each of these locations have the potential for genetic and epigenetic alterations. Malignant mucosal melanomas (MM) are rare cancers. MM represents only 1.3% of all melanomas. In 2013, 830 newly diagnosed cases were estimated to occur in Europe, but its incidence appears to be increasing. MM of the head and neck region involve the nose and paranasal sinuses, oral cavity, pharynx, and larynx. Nasal MMs are clinically rare, only 4% of all nasal tumors.1,2 With high recurrence and metastasis rates, nasal MM has a poor prognosis.3 Amelanotic melanomas (AMs) thought to be biologically more aggressive than other histopathological variants of MM. Beside the difficult diagnosis, another challenge with AM are controversies in the optimal therapy protocol for this rare tumors.
We present a case with interesting clinical and histopathological features of primary malignant MM and then recurrent AM of nasal cavities in a female patient.
Case Report
A 65-year-old female patient consulted at the Clinic for Otorhinolaryngology of Clinical Hospital Centre Rijeka, in September 2018 with nasal obstruction, right facial pain and sporadic episodes of epistaxis. From medical history, the patient had tonsillectomy and nasal polyps surgery in her childhood. Still, in 2013 she was diagnosed with MM in left nasal cavity. Back then, the endoscopic examination showed a polyploid mass, dark brown to black, that obstructed the entire left nasal cavity. A biopsy of the lesion was performed and the microscopic examination showed metaplastic epithelium, stroma with numerous enlarged glands and neovascularization. The pathologist described clusters of atypical melanocytes with a brown pigment in cytoplasm. Immunohistochemistry showed strong positivity for HMB45, S-100 and microphthalmia-associated transcription factor (MITF) (Figure 1). Final diagnosis was MM. An multi-slice computed tomography (MSCT) of the paranasal sinuses revealed a tumor mass involving left inferior and middle nasal turbinates and left ethmoid cells, and swollen mucosa of frontal, maxillary and sphenoid sinus (Figure 2). The structures of the right nasal cavity were completely tumor-free. Endoscopic medial maxillactomy was performed and surgeon partially removed the nasal septum and upper lateral cartilage during the procedure. Multiple biopsy specimens from frontal, sphenoid and maxillary sinus showed no MM. Clinically, there was no lymphadenopathy and suspected distant metastasis which was confirmed by neck ultrasound and positron emission tomography- computed tomography (PET/CT). In 2013, patient was staged as T3N0M0. She received postoperative radiotherapy, with a total dose of 5400 cGy, in 27 fractions of conformal radiotherapy. She has been in regular follow up and in one of them in 2018, similar symptoms appeared, this time in the right nasal cavity. Anterior rhinoscopy showed tumor mass in right middle nasal meatus. The mass was reddish pink in color without black or brown discoloration. MSCT scan of head, orbits, and sinuses revealed a invasive mass (46×20 mm) involving right inferior and middle nasal turbinates, and maxillary sinus medial wall without intracranial and intraorbital extension (Figure 2). A second endoscopic medial maxillectomy was performed. The histopathology report showed atypical epithelioid cells and multinucleated giant cells with eosinophilic cytoplasm. Some cells were bizarre looking with mitotic activity and there was no pigment in the cytoplasm. Tumor cells revealed to be medium positive for HMB45 and S-100, and sporadically positive for MITF. This pathohistology results indicated that the lesion was AM (Figure 1). The finding of PET/CT suggested an increased accumulation in the lymph node on the right side neck in region II (18×9 mm) and left parotid lymph node (7.6×3.8 mm). Fine needle aspiration cytology for lymph nodes confirmed melanoma metastases. After complete diagnostics workup, tumor was staged as T4N1M1. Real-time polimerase chain reaction was performed for mutation detection of BRAF gene on exon 11 and exon 15, which did not determine the mutation. The patient was presented to the multidisciplinary oncology team to determine treatment plan. Taking into account previous treatment programmed cell death-1 protein (PD- 1) inhibitor, pembrolizumab was introduced. The patient received third dose, and treatment is ongoing. On last checkup there is no symptoms and clinical signs of new metastases or recurrence of local disease.
Discussion
We present a patient that developed a rare MM of the left nasal cavity and, in addition, few years later a recurrent amelanotic variant on the opposite, right side. The present case raises the question whether this is a recurrence or a new-found MM. MM arise primarily in the head and neck regions, commonly in nasal cavity involving the turbinates and nasal wall. Among nasal MM cases rare were describe as AMs.1 Thus, some authors presented a case of AM in female patient with a mass in left nasal, and other a case of sinonasal cavity AM with intraoral extension.4,5 Local recurrences in MM occur in about 50% of cases.2,6 This could be the main reason for poor prognosis and survival. As a result, five-year survival in Europe between 2000 and 2007 was only 19-23%.7,8 Reasons for high recurrence rate are probably the unique MM biology, submucosal lymphatic spread, vascular invasion, and deficient surgical resection.3 The intranasal endoscopic surgery remains controversial due to difficulty of controlling surgical margins. Most authors report that endoscopic resections are being performed commonly and may be accomplished with less complications while maintaining oncologic efficacy.2,3,6 The sentinel lymph node biopsy, used in cutaneous melanoma, is still controversial in MM. However, no significant difference in five-year survival has been observed in patients with or without lymph node reccurence.3 That was also a reason to avoid the therapeutic neck dissection in our patient. In one of rare reports found in the literature, Sharma et al. presented a case of male patient with oral MM, following the recurrent amelanotic variant of the upper lip after 4 years and primary surgical treatment for oral MM.9 The reason for recurrence of MM in our patient is difficult to explain since it occurred in the opposite nasal cavity and additionally, with different histological feature as well probably varied biological characteristics. Opposite to cutaneous melanoma, the biology of MM is poorly understood. No risk factor has been identified to explain the development of MM.1 It is well-known that malignant transformation of melanocytes is associated with the accumulation of genetic and molecular alterations in multiple signaling pathways. The MAPK pathway has been of interest since the discovery of frequent activating mutations of the BRAF kinase. Unlike skin melanoma, BRAF mutations in MM are uncommon, as it was not found in our case. BRAF mutation is detected in 3-5% of head and neck MM.1-3,6 According to Amit et al. there is no association between mutations status and survival outcomes in sinonasal MM patients.10 One of the transcriptional factors regulated by MAPK pathway is microphthalmia-associated transcription factor. MITF is essential for melanocyte differentiation, it can alternatively promote malignant behavior as an oncogene.2,11 In 2013, we demonstrated the MITF immunohistochemistry amplification in the primary MM of the left nasal cavity however in recurrent AM the MITF expression was lower. Thus, immunohistochemical markers, HMB45 and S-100, despite lower expression compare to primary MM, were essential in diagnosis of recurrent AM. MM lacking or with very low levels of melanin may grow more rapidly than pigmented melanomas. It is important to emphasize the possible chemotherapeutics and radiotherapy effect on melanogenesis, basic process for melanoma cells thus changing the tumor cells biology.11,12 Vierne et al. reported an histologically different, mainly amelanotic mandibular metastasis 16 years after adjuvant radiotherapy treatment for primary cutaneous melanoma.13 This fact opens up various dilemmas in determination of the right MM therapy. After MM staging, established by the American Joint Committee on Cancer, complete surgical excision is first-line treatment. 1 MM are composed of cells with high post-irradiation regenerative capacity, but radiation dose of 54 Gy improves local control in some studies.1-4 However, the findings are controversial. In case of our patient the question arises: was the adjuvant radiotherapy crucial for changing the biology of MM into an amelanotic, aggressive variant? In search for right therapy choice, anti-PD- 1 antibodies are implicated as potential option. Anti-PD-1 immunotherapy significantly prolong survival in patients with cutaneous melanoma and metastatic melanoma.2,14 The results of this therapy in patients with MM are lacking. Clinical trials addressing the activity of these agents in patients with MM are necessary to clarify the role of anti-PD-1 immunotherapy.
Figure 1.
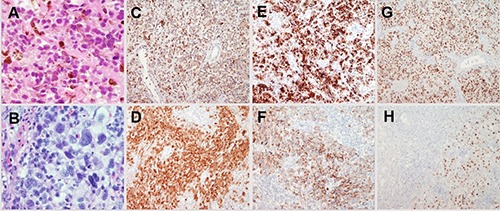
Microscopic examination (HE, magnification ×400). A) In 2013, atypical melanocytes with a brown pigment in cytoplasm. B) In 2018, pleomorphic, multinucleated giant cells with no pigment in cytoplasm. Immunohistochemistry staining profiles (magnification ×100). C, D) S-100 strong staining in both melanomas, primary and recurrent. E) HMB45 strong staining in primary mucosal melanoma. F) Moderate HMB45 staining in recurrent melanoma. G) Microphthalmia-associated transcription factor strong staining in primary mucosal melanoma. H) Weak microphthalmia-associated transcription factor staining in recurrent amelanotic melanoma.
Figure 2.
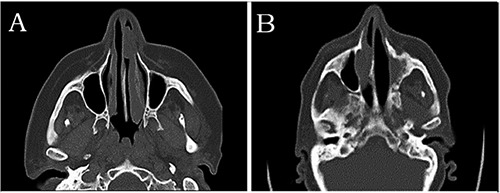
Transverse computed tomography. A) In 2013, invasive mass involving inferior and middle nasal meatus of left nasal cavity. B) In 2018, mass involving right inferior and middle nasal meatus.
Conclusions
Single case reports as ours are significant to clinical practice, especially in absence of clinical guidelines for MM treatment. We put emphasis on fact that there are critical differences between mucosal and cutaneous melanoma, which must influence future clinical decision-making. Hopes for improvement of poor survival in MM patients are based on progress in endoscopic surgery, immunotherapies and targeted treatments.
Funding Statement
Funding: none.
References
- 1.Ascierto PA, Accorona R, Botti G, et al. Mucosal melanoma of the head and neck. Crit Rev Oncol Hematol 2017;112:136-52. [DOI] [PubMed] [Google Scholar]
- 2.Gilain L, Houette A, Montalban A, et al. Mucosal melanoma of the nasal cavity and paranasal sinuses. Eur Ann Otorhinolaryngol Head Neck Dis 2014;131:365-9. [DOI] [PubMed] [Google Scholar]
- 3.López F, Rodrigo JP, Cardesa A, et al. Update on primary head and neck mucosal melanoma. Head Neck 2016;38:147-55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Dogra BB, Kandari A, Kataria M, et al. Amelanotic melanoma of the nasal mucosa: a rare case report. Med J DY Patil Univ 2015;8:543-6. [Google Scholar]
- 5.Singhvi A, Joshi A. A case of amelanotic malignant melanoma of the maxillary sinus presented with intraoral extension. Malays J Med Sci 2014;22:89-92. [PMC free article] [PubMed] [Google Scholar]
- 6.Letievant JC, Poupart M, Ambrun A, et al. Single-center retrospective series of fourteen patients with mucosal melanoma of the nasal cavity and paranasal sinuses. Eur Ann Otorhinolaryngol Head Neck Dis 2016; 133:387-91. [DOI] [PubMed] [Google Scholar]
- 7.Verma R, Lokesh KP, Gupta K, et al. Sinonasal amelanotic malignant melanoma – A diagnostic dilemma. Egypt J Ear Nose Throat Allied Sci 2015;16:275-8. [Google Scholar]
- 8.Gasparyan A, Amiri F, Safdieh J, et al. Malignant mucosal melanoma of the paranasal sinuses: two case presentations. World J Clin Oncol 2011;2:344-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Sharma LN, An J, Liu Q, et al. Primary malignant mucosal melanoma of the upper lip: a case report and review of the literature. BMC Res Notes 2015;8:499. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Amit M, Tam S, Abdelmeguid AS, et al. Mutation status among patients with sinonasal mucosal melanoma and its impact on survival. Br J Cancer 2017; 116:1564-71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Thomas NE, Kricker A, Waxweiler WT, et al. Comparison of clinicopathologic features and survival of histopathologically amelanotic and pigmented melanomas: a population-based study. JAMA Dermatol 2015;150:1306-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Skoniecka A, Zauszkiewicz-Pawlak A, Tyminska A, et al. Melanization of Bomirski hamster amelanotic melanoma cells (Ab line) depends on the type of culture medium. Folia Histochem Cytobiol 2018;56:207-14. [DOI] [PubMed] [Google Scholar]
- 13.Vierne C, Hardy H, Guichard B, et al. Mandibular metastasis of a cutaneous melanoma or metachronous amelanotic melanoma of the oral cavity? A case report and literature review. Ann Chir Plast Esthet 2014;59:277-9. [DOI] [PubMed] [Google Scholar]
- 14.Dabelić N, Marić Brozić J, Đaković N, et al. Advences in melanoma immunotherapy. Libri Oncol 2017;45: 46-51. [Google Scholar]