

Abstract
Depression and insomnia are very significant pathologies in cancer patients as they contribute to the patient’s overall cure and quality of life. Moreover, untreated depression and ongoing insomnia are associated with decreased immune responses and lower survival rates. With all disease states and especially with cancer, close attention to drug-drug interactions and the potential impact on the efficacy of therapy is paramount. One area of particular interest due to the lack of well-done clinical trials is drug-drug interaction(s) between antidepressants and cancer treatment. Pharmacokinetics of a certain drug allows for prediction of certain drug interactions based on chemical properties of the agents involved. If the agents depend on their metabolites for activity, active drug level will be decreased through this enzyme inhibition. In this paper, we looked at the cytochrome-P450 drug interactions between antidepressants and sleep aids with Selective Estrogen Receptor Modulators (SERM). Newer SERM metabolisms are less influenced by interactions with medications used to treat depression. However, tamoxifen metabolism could be severely altered by several antidepressants. This has direct consequences as patients on tamoxifen and antidepressant can have double the risk of relapse to cancer in two years. We discussed those interactions and made recommendations for clinical use.
Key words: depression, insomnia, cancer patients, drugs interaction
Introduction
Depression and insomnia are very significant pathologies in cancer patients as they contribute to the patient’s overall cure and quality of life. Moreover, untreated depression and ongoing insomnia are associated with decreased immune responses and lower survival rates. Depression in cancer patients is the phenotypic manifestation of cancer and cancer treatment-mediated structural and functional brain dysfunction, which affects the hippocampus and decreases hippocampal neurogenesis.1-4 As many as 35% of cancer patients suffer from depression and over 10% have major depressive disorder.5,6 Similarly, insomnia affects up to 50% of patients with cancer.7 Therefore, pharmacological options are often employed to address insomnia and/or depression in this patient population.
With all disease states and especially with cancer, close attention to drug-drug interactions and the potential impact on the efficacy of therapy is paramount. One area of particular interest due to the lack of welldone clinical trials is drug-drug interaction(s) between antidepressants and cancer treatment. Without reliable clinical trials to vet the potential drug-drug interactions, we are left with theoretical evidence and educated deductive reasoning. With that said, the pharmacological treatment of depression in patients with cancer presents unique challenges caused by drug-drug interactions between antidepressants and cancer pharmacotherapy, which may lower the effectiveness of cancer treatment.1-4 Despite the impact of depression in patients with cancer, studies looking at the efficacy of antidepressant medications in this population are very few and of low quality. On the other hand, the pharmacological options available for treatment of insomnia pose less of a challenge in terms of drugdrug interactions for patients currently on cancer pharmacotherapy.
Methodology
We approached the topic of drug interactions in setting of depression and/or insomnia and breast cancer from two different perspectives. First, the pharmacokinetics of a certain drug allows for prediction of certain drug interactions based on chemical properties of the agents involved. In general, inhibitors of cytochrome P450 enzyme(s) will reduce metabolism of enzyme substrates. If the agents depend on their metabolites for activity, active drug level will be decreased through this enzyme inhibition. For instance, tamoxifen is a prodrug, a biologically inactive compound that requires CYP2D6 enzymatic activation to yield the active metabolite, endoxifen. Therefore, enzymatic inhibition of CYP2D6 will decrease metabolism of parent drug tamoxifen and thus decrease level of active metabolite endoxifen. On the other hand, inducers of cytochrome P450 enzyme(s) will increase metabolism and excretion of enzyme substrates, which will result in either increased level of active metabolites or decreased level of active parent drugs. Secondly, consideration for the clinical significance of drug interactions to inform our clinical decisions is a must. In regards to pharmacodynamics, changes in drug levels secondarily to cytochrome P450 inhibition or induction may not be as clinically significant as hypothetically predicted depending on the therapeutic indexes of the agents involved.
Selective Estrogen Receptor Modulators (SERMs): tamoxifen, raloxifene, toremifene
Selective estrogen receptor modulators (SERMs), including tamoxifen, raloxifene and toremifene, are drugs commonly used in breast cancer treatment. Particularly, tamoxifen, a cost effective SERM that is commonly used, is a prodrug that is metabolized through various cytochrome P450 enzymes, specifically CYP3A4, CYP3A5 and CYP2D6, to give three active metabolites.7 Therefore, drugs that inhibit these enzymes, especially CYP2D6, may decrease tamoxifen active metabolite level, potentially diminishing tamoxifen’s anti-cancer effect. Importantly, this drug-drug interaction through cytochrome P450 metabolic pathways may increase the recurrence of cancer in patients concomitantly taking tamoxifen and a CYP2D6 inhibitor.8
Conversely, SERMs that are not reliant on CYP2D6 for metabolism pose a less complicated challenge in regards to drug-drug interactions relative to tamoxifen. Raloxifene undergoes glucuronidation while toremifene utilizes CYP3A4 for its metabolism. Therefore, the challenge in using raloxifene or toremifene concomitantly with CYP2D6 inhibitors such as certain antidepressants is unparalleled to tamoxifen. The differences in metabolism and the pathways employed by each medication partially explain the variations in drug-drug interactions between SERMs and antidepressants.9,10 Overall, the clinical pharmacodynamic effects of each drug interaction are largely dependent on the therapeutic indexes of drugs involved.
Pharmacological treatment for depression
Pharmacological interventions for depression include several categories of medications, including selective serotonin reuptake inhibitors (SSRI), serotonin norepinephrine reuptakes inhibitors (SNRI), and tricyclic antidepressants (TCA).
Upon review of clinical trials and pharmacokinetic studies of various antidepressants and their potential impact on the metabolism of SERMs, especially tamoxifen, the following conclusions were drawn. As shown in Figure 1, paroxetine, fluoxetine and bupropion are amongst the strongest CYP2D6 inhibitors of the antidepressants.1-6,8-17 Despite the controversial evidence available regarding the clinical significance of these strong inhibitory activity on tamoxifen’s anticancer effect, it is premature to dismiss these interactions given the lack of strong evidence proving unchanged mortality rate with paroxetine, fluoxetine and bupropion. On the other hand, Trazodone,11 citalopram12-15,18,19 and escitalopram12,13,15,18,19 are metabolized through various cytochrome P450 enzymes but are not an inhibitor of these enzymes; therefore, they are reasonable candidates for treatment of depression or mood disorders in the setting of breast cancer treatment with tamoxifen, a CYP2D6 substrate. Similarly, venlafaxine12,14,15 is a good option albeit very minor inhibitory activity on CYP2D6 relative to other SSRIs and SNRIs. Given a variety of safe options based on the available clinical evidence for treatment of depression and concomitant tamoxifen, take caution when prescribing antidepressants with strong CYP2D6 inhibitory activity like paroxetine, fluoxetine and bupropion to patients currently taking tamoxifen.
Figure 1.
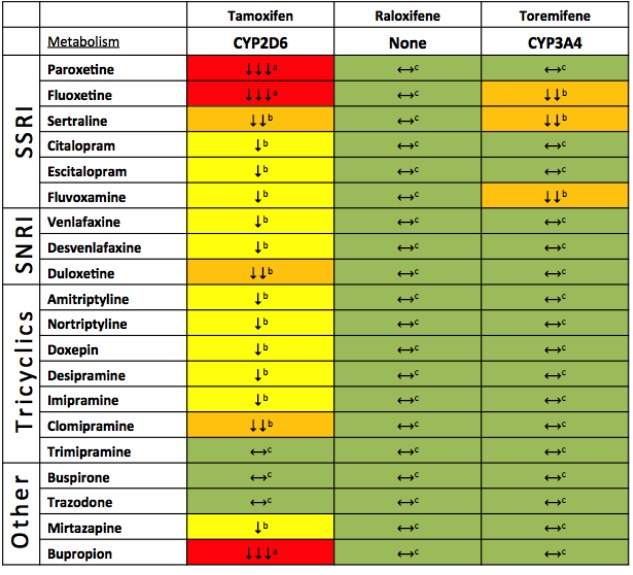
Cytochrome-P450 Drug Interactions between Antidepressants and Selective Estrogen Receptor Modulators (serms). Classification of antidepressants’ cytochrome P450 inhibition based on available pharmacokinetic data.1-6,8-17 Green (⟷): No inhibition; Yellow (↓): Mild inhibition; Orange (↓↓): Moderate inhibition; Red (↓↓↓): Strong inhibition. Recommendation based on clinical relevance of cytochrome P450 interactions. aConsider therapy modification: Evidence available to support clinically significant decrease in efficacy of selected breast cancer pharmacotherapy as measured by all-cause mortality and/or breast cancer recurrence. bMonitor therapy: Lack of evidence available or available evidence suggests clinically insignificant decrease in efficacy of selected breast cancer pharmacotherapy as measured by all-cause mortality and/or breast cancer recurrence. Cno action required: No known or expected clinically significant interaction.
Figure 2.
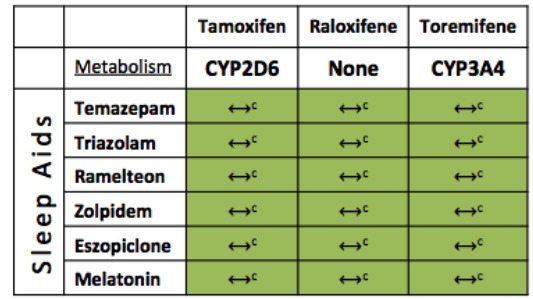
Cytochrome-P450 Drug Interactions between Selected Sleep Aids and Selective Estrogen Receptor Modulators (SERMs). Classification of sleep aids’ cytochrome P450 interactions based on available pharmacokinetic data. Green (⟷): No interaction. Recommendation based on clinical relevance of cytochrome P450 interactions. cNo action required, No known or expected clinically significant interaction.
Pharmacological treatment of insomnia
Pharmacological interventions for insomnia also include several categories of medications such as benzodiazepines, hypnotics and others. Although there are variations in the metabolic pathway of each SERM as stated above, available pharmacokinetic and pharmacodynamic data show no clinically relevant interactions between the selected sleep aids and SERMs. Figure 2 details the relative metabolic pathway employed by each SERM as well as the level of drug-drug interactions with various sleep aids commonly used in practice.16,17,20-24
Funding Statement
Funding: none.
References
- 1.Gust J, Hay KA, Hanafi LA, et al. Endothelial Activation and Blood-Brain Barrier Disruption in Neurotoxicity after Adoptive Immunotherapy with CD19 CAR-T Cells. Cancer Discov 2017;7:1404-19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Vitali M, Ripamonti CI, Roila F, et al. Cognitive impairment and chemotherapy: a brief overview. Crit Rev Oncol Hematol 2017;118:7-14. [DOI] [PubMed] [Google Scholar]
- 3.Ren X, St Clair DK, Butterfield DA. Dysregulation of cytokine mediated chemotherapy induced cognitive impairment. Pharmacol Res 2017;117: 267-73. [DOI] [PubMed] [Google Scholar]
- 4.Wardill HR, Mander KA, Van Sebille YZ, et al. Cytokine-mediated blood brain barrier disruption as a conduit for cancer/ chemotherapy-associated neurotoxicity and cognitive dysfunction. Int J Cancer 2016;139:2635-45. [DOI] [PubMed] [Google Scholar]
- 5.Zainal NZ, Nik-Jaafar NR, Baharudin A, et al. Prevalence of depression in breast cancer survivors: a systematic review of observational studies. Asian Pac J Cancer Prev 2013;14:2649-56. [DOI] [PubMed] [Google Scholar]
- 6.Ng CG, Boks MP, Zainal NZ, et al. The prevalence and pharmacotherapy of depression in cancer patients. J Affect Disord 2011;131:1-7. [DOI] [PubMed] [Google Scholar]
- 7.Appiani F, Carroll BT, Munoz C, et al. Tamoxifen-SSRIs interaction: clinical manifestations of inhibition and lack of inhibition of CYP2D6. Ann Clin Psychiatry 2011;23:152-3. [PubMed] [Google Scholar]
- 8.[No authors listed]. Antidepressants and tamoxifen. Drug interactions may increase risk of cancer recurrence or death. Harv Ment Health Lett 2010;26:6-7. [PubMed] [Google Scholar]
- 9.Kim J, Peraire C, Sola J, et al. Drug interaction potential of toremifene and Ndesmethyltoremifene with multiple cytochrome P450 isoforms. Xenobiotica 2011;41:851-62. [DOI] [PubMed] [Google Scholar]
- 10.Fareston. Package insert: GTx, INc, TN, 2011. [Google Scholar]
- 11.Chubak J, Bowles EJ, Yu O, et al. Breast cancer recurrence in relation to antidepressant use. Cancer Causes Control 2016;27:125-36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Desmarais JE, Looper KJ. Interactions between tamoxifen and antidepressants via cytochrome P450 2D6. J Clin Psychiatry 2009;70:1688-97. [DOI] [PubMed] [Google Scholar]
- 13.Hemeryck A, Belpaire FM. Selective serotonin reuptake inhibitors and cytochrome P-450 mediated drug-drug interactions: an update. Curr Drug Metab 2002;3:13-37. [DOI] [PubMed] [Google Scholar]
- 14.Jin Y, Desta Z, Stearns V, et al. CYP2D6 genotype, antidepressant use, and tamoxifen metabolism during adjuvant breast cancer treatment. J Natl Cancer Inst 2005;97:30-9. [DOI] [PubMed] [Google Scholar]
- 15.English BA, Dortch M, Ereshefsky L, et al. Clinically significant psychotropic drug-drug interactions in the primary care setting. Curr Psychiatry Rep 2012;14:376-90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Information: P. Temazepam. In: Mallinckrodt Inc SL, MO, ed., 2002. [Google Scholar]
- 17.Moltke L. Zolpidem metabolism in vitro: responsible cytochromes, chemical inhibitors, and in vivo correlations. Br J Clin Pharmacol 1999;48:89-97. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Donneyong MM, Bykov K, Bosco-Levy P, et al. Risk of mortality with concomitant use of tamoxifen and selective serotonin reuptake inhibitors: multi-database cohort study. BMJ 2016;354:i5014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Lash TL, Cronin-Fenton D, Ahern TP, et al. Breast cancer recurrence risk related to concurrent use of SSRI antidepressants and tamoxifen. Acta Oncol 2010;49:305-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Information P. Restoril, temazepam. Mallinckrodt Inc, St Louis, MO: 2002. [Google Scholar]
- 21.Information P. Triazolam. In: Pharmacia & Upjohn Company K, MI, ed., 2003. [Google Scholar]
- 22.Information P. Ramelteon. In: Takeda Pharmaceuticals America I, Lincolnshire, ed., 2005. [Google Scholar]
- 23.Brielmaier BD. Eszopiclone (Lunesta): a new nonbenzodiazepine hypnotic agent. Proc (Bayl Univ Med Cent) 2006;19:54-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Whirl-Carrillo M, McDonagh EM, Hebert JM, et al. Pharmacogenomics knowledge for personalized medicine. Clin Pharmacol Therapeut 2012;92: 414-17. [DOI] [PMC free article] [PubMed] [Google Scholar]