

Abstract
The objectives of a cross-sectional, semi-quantitative study were to: i) assess the prevalence of water insecurity and its association with water access-related behaviors such as time, distance, and sources of water; ii) identify major themes of concern raised in reference to anxiety, water quality/quantity, and perceived health risk domains of water insecurity, and; iii) examine the relationship between water insecurity, hygiene practices, and diarrheal incidence among children in rural areas of the Menoua Division in the Western Region of Cameroon In-person interviews were conducted with 18 years or older women living with at least one child between 2 and 5 years old (n=134). Participants spent on average 17±12 minutes walking to a drinking water source. Prevalence of water insecurity was 58%, and it was associated with a lower hygiene score among caretakers, i.e., hygiene score of water secure: 9.2±1.2 vs. insecure:8.2±2.2, F(1, 132)=8.096, P<0.01). Overall, the incidence of diarrhea among children was 18%, and it was significantly higher among water insecure households (79%) compared with secure households (21%, P=0.02). In conclusion, access to improved sources of water is an issue in rural areas. Addressing water insecurity is critical in promoting optimal health and development of children due to its association with poor hygiene practices among caretakers.
Key words: water insecurity, children, diarrhea, food utilization, hygiene
Introduction
Diarrhea, a condition of passing at least three loose or liquid stools within 24 hours, is the second leading cause of death among children aged five years or younger.1,2 Every day, 1,400 children die due to diarrhea. 2 This primarily occurs in low-income and middle-income countries where diarrhea kills more children than acquired immunodeficiency syndrome, malaria, and measles combined.1,2 According to the World Health Organization (WHO), 50% of all undernutrition cases in children are related to repeated diarrhea and intestinal worm infections.3 Consequently, Water Access, Sanitation, and Hygiene (WASH) promotion has become the primary strategy in improving the growth of children.4 However, the implementation of WASH components relies on availability of safe water.4 In a meta-analysis of 46 studies, Fewtrell et al.5 found that water supply interventions were effective in reducing water-related illnesses (diarrhea, cholera, and typhoid).
Every human has the right to sufficient, safe, physically accessible, and affordable water for personal and domestic use. However, inadequate access to safe, clean, and sufficient amounts of water is a huge issue. According to the recent report by the United Nations (UN)-Water, there are approximately 663 million people experiencing poor water access with half of these people living in sub-Saharan.6 Based on the recent established indicators, inadequate water access is defined as daily water use per person of <50 liters of water and/or access that requires a lengthy collection time of >30 minutes. Additionally, it is recognized that a long distance to a water source (>1000 meters) results in poor water access.7 These data provide critical information on access and adequacy of water use. However, to measure the extent of psychosocial distress and inconsistency in access to water, an assessment of water insecurity at the household level is critical.
Using the following definition of water insecurity, ‘insufficient and uncertain access to adequate water for an active and healthy lifestyle,’ a few studies have been conducted to understand the reasons for the prevalence of water insecurity and its association with social and psychological issues at the household level. One of the earliest studies was conducted in Bolivia in 2009 and included 72 households. The results indicated that water insecurity was associated with lower household income and coping behaviors, such as borrowing water from a neighbor and requesting private vendors to give water using credit.8 In a cross-sectional study in Ethiopia, it was found that water insecurity was positively associated with psychosocial distress among women.9 Further, in an intervention study, Stevenson et al.10 found that water insecurity remained a significant predictor of psychosocial distress, even after controlling for food insecurity and the quality of the previous year’s harvest. Similarly, a cross-sectional study with postnatal women living in urban Nepal demonstrated that water insecurity was associated with high rates of depression and low ratings on physical health-related quality of life.11 Hence, though limited, the current literature indicates that water insecurity is associated with poor coping behaviors and anxiety. To advance the understanding on water insecurity and its role in predicting WASH-related activities, we conducted a study to determine the inter-relationship between water insecurity, hygiene practices, and incidence of diarrhea among children. The objectives of this study were to (1) Assess the prevalence of water insecurity and its association with water access-related behaviors such as time, distance, and sources of water; (2) identify major themes of concern raised in reference to anxiety, water quality/quantity, and perceived health risk domains of water insecurity, and; (3) examine the relationship between water insecurity, hygiene practices, and diarrheal incidence among children in rural areas of the Menoua Division in the Western Region of Cameroon.
Materials and Methods
Cameroon is a Central African country situated below the Gulf of Guinea. The study was conducted in the Menoua Division located in the West Region of the country. The Menoua Division is one of the eight divisions of the West Region and includes 22 villages. It covers an area of 1380 km2 with a population of about 372,244 inhabitants.12 The climate encountered there is of the equatorial monsoon type, and there are two main seasons: the dry season (a long, dry season from December to March and a short, dry season from June to August) and rainy season (a long, rainy season from September to December and a short, rainy season from March to June). The temperatures range from 13.66°C to 25.35°C with annual average rainfall of 1717.7 mm.12,13 Agriculture constitutes the mainstay of the economy with more than 80% of the inhabitants being farmers.12 A cross-sectional semiquantitative study involving in-depth interviews with caretakers was conducted in a village of the Menoua division from January 2017 to April 2017. Approval was obtained from the University of North Carolina’s Institutional Review Board and the Cameroon National Committee of Ethics for Human Research to conduct the study. Women meeting the following selection criteria were recruited: (1) 18 years or older; (2) self-reported as currently not pregnant; (3) primary meal preparer of the household; (4) taking care of and living with at least one child between 2 and 5 years old. We recruited them using either a door-to-door approach or by going to communal places, such as clinics and schools. Upon indicating interest, caretakers were given details about the study and their written consents were obtained. The interviews were conducted at the participants’ homes or in a private setting in their preferred language, i.e., English, French, or Yemba. Interviews in English and French were conducted by a research assistant, while interviews in a local dialect, Yemba, were conducted with the help of a local interpreter. During the interviews, one child between the ages of 2 and 5 years (or the youngest child, if there was more than one child within this age range) in the household was selected as an index child to enquire about diarrheal episodes and the occurrence of other hygiene-related diseases.
Prior to conducting the main phase study, a pilot study was conducted with 15 women to (1) finalise logistics of recruitment and outreach; (2) estimate the average length of the interview; (3) establish the timeline for the main phase study; and (4) test and revise the questionnaire to ensure it is culturally appropriate, relevant, and applicable to the study area. The pilot phase was also used to train the local interpreter in interview techniques and data confidentiality. To calculate the sample size for the main phase study, prevalence of food insecurity in the study area was used as an indicator for two reasons: (1) there were no published data available on water-use in the study area and (2) the other overarching goal was to assess the relationship between food and water insecurity among study participants. A sample size of 134 was estimated using an α level of .05 and 80% power. The interview questionnaire included the following five sections: (1) Socio-economic and demographic characteristics, (2) Water in/security status, (3) Water access-related behaviors (water sources, distance, time), (4) Frequency of handwashing practices, and (5) Occurrence of diarrhea and other hygiene-related illnesses (the questionnaire with the above five sections is available online as supplementary material).
Data analyses
Analyses were conducted using SPSS 23 (IBM Corporation, Somers, NY, USA). Water in/security was measured using a sixitem scale developed by Aihara et al.11 Each item was scored following a three-point Likert style (never/rarely, sometimes, always). Reponses of “sometimes” and “always” were considered affirmative responses and one point was given. The scores ranged from 0 to 6. Based on the score, the participants were grouped into the following two categories: a score of 0 score=water secure; ≥1 score=water insecure. For each affirmative response, participants were asked to explain the response in detail. These responses were organized into the following three areas: (1) anxiety/stress, (2) quantity and quality of water, and (3) sickness due to water.
The participants were asked about how frequently they washed their hands with soap and water at the following five key stages: before cooking, before eating, before feeding the child, after defecation, and after cleaning the child’s stool. For each stage, the frequency of hand washing was scored as follows: (1) never/rarely: score 0; (2) sometimes: score 1, and; (3) always: score 2. The total score ranged from 0 to 10, with the maximum score of 10 representing always washing hands with soap and water at all the five critical steps of hygiene.
For the occurrence of diarrhea and other hygiene-related illnesses, participants were asked if the index child had any of the listed condition in the past 30 days, with “yes” and “no” options. To maintain consistency, diarrhea was described to participants as having three or more stools of a soft or watery consistency in 24 hours. The caretaker was also asked to evaluate the index child’s overall health as either excellent/good (good health status) or average/ poor (poor health status).
Descriptive statistics were conducted to describe socio-demographic characteristics and prevalence of water insecurity. Bivariate tests (chi-square, one-way ANOVA) were conducted to detect differences in water sources, walking distance in minutes, and other water-related behaviors by water security versus insecurity status. Bivariate comparisons were also made to detect differences in the hygiene/handwashing score. Incidents of diarrhea and other hygiene-related illnesses in the past 30 days among index children were compared between water security and insecurity status. Results were considered significant at a probability value of ≤ 0.05.
Results
Of the total 134 interviews with participants, 128 (96%) were conducted in French. Of the remaining six interviews, three were conducted in English, and the remaining in Yemba.
Socio-demographic information
The mean age of the participants was 36±11 years, while on average, the age of the children selected for the study was 3 years. As shown in Table 1, average household size was 6±2 and the number of children living in the households ranged from one to six. The monthly median household income was $ 60-90, falling in the category of moderate to low household incomes by the local standards. Only 17% of the caretakers had a high school education or higher. Most (78%) of the participants were either married or living with a partner, and approximately 72% of them were Christian (Table 1). Most of the caretakers reported having a farm and owning livestock. Although many caretakers identified themselves as housewives, working on their farms was common to produce food for the household and grow cash crops, such as coffee, beans, maize, tubers, sweet potatoes, Irish potatoes, and fresh vegetables (tomatoes, green peppers, leafy vegetables). Approximately 22% of caretakers were small- scale food or grocery sellers, mainly involved in selling items, such as salt, Maggi, palm and refined oil, tomato paste, bread, beignets, and ready-to-eat food.
Water access-related behaviors
Of the 134 participants, only five reported having access to running tap water, while 39 caretakers reported having a well in their compound. Among the participants, 60% reported using a separate source of water for drinking and general household chores. In general, participants were more concerned about drinking water and used the water source they perceived to be cleanest and safest. For those who used a different source of water for drinking versus household chores, on average they spent 17±12 minutes walking to reach the water source used for drinking water, while for household chores, it took an average of 11±10 minutes from home to the water source (Table 2). The return time was not noted specifically, but participants reported it was longer, since walking with full containers of water or carrying water on trolleys slowed down the walking pace. Participants reported using containers, such as plastic containers, buckets, and large bottles to fetch water. The frequency of making a trip to fetch water was higher for water needed for household chores, and the amount of water collected during each trip was 106±134 liters (Table 2). Households often used trolley-like equipment (metal board on small wheels) to carry substantial amounts of water each trip. Approximately one-fourth of the caretakers reported fetching water, and overall, everyone in the household except the head of the household was responsible for fetching water. Filter and water purification practices were not very common, however, many of those who owned wells reported treating their water with salt and chlorine. That water was then primarily used for household chores.
Prevalence of water insecurity
Using the six-item water insecurity scale, we asked caretakers if they experienced each of the items during the last 30 days. As shown in Figure 1, the highest level of affirmative response (37%) was obtained for item 1, enquiring if the caretaker was worried about not getting enough water. About one-fourth of the participants affirmed not having enough water for household chores or drank poor quality water. Although it was uncommon, 10% of the participants reported borrowing water, and 5% reported that they sometimes or always became sick due to unclean water (Figure 1). Of the total number of participants, 42% had water security, while the remaining 58% were water insecure, confirming experiencing at least one of the six statements on the survey.
Table 1.
Description of socio-demographic characteristics of women living in a rural village of the Menoua division, West region of Cameroon (n =134).
| Socio-demographic characteristics | Mean±SD or n (%) |
|---|---|
| Women’s age (in years) | 36±11 |
| Index child’s age (in months) | 39±10 |
| Household sizea | 6±2 |
| Number of children living in the household (below 18 years) | 4±2 |
| Monthly household income ($);be | |
| 0-30 | 20(15) |
| 30-60 | 38(28) |
| 60-90 | 14(10) |
| 90-120 | 21(16) |
| 120-150 | 8(6) |
| ≥150 | 16(12) |
| Education | |
| No formal schooling | 4(3) |
| Some school | 107(80) |
| High school | 20(15) |
| College education | 3(2) |
| Marital status | |
| Married/having a partner | 105(78) |
| Single | 19(14) |
| Widow | 10(8) |
| Religion | |
| Christian | 96(72) |
| Muslim | 6(5) |
| Othersc | 32(24) |
| Occupation | |
| Housewife | 52(39) |
| Small scale food/grocery seller | 29(22) |
| Working on the farms | 16(12) |
| Dress stylist/hair stylist | 16(12) |
| Othersd | 21(16) |
| Owned a farm | 128(95) |
| Owned a livestock | 102(76) |
| Had electricity at home | 127(95) |
SD=Standard deviation
aTotal number of individual living in a household
bself-reported in local currency, which was later converted into dollar amount, and n = 117: since 17 participants did not know or refused to answer. The amount represents an earned income and does not include non-monetary resources such as food from farms and livestock products
ctraditional beliefs such as animism and skull cult
danimal breeding, community health worker, teacher, office worker
epercentages are rounded to a nearest full digit.
Table 2.
Description of the sources, time, distance and other water access related behaviors practiced among households living in a rural village of the Menoua division- West region of Cameroon (n=80).a
| Sources, distance, time and other water access related variables | Mean±SD or n (%) | |
|---|---|---|
| Drinking water | Chores water | |
| One-way walking time from house to water source (in minutes)b | 17±12 | 11±10 |
| How long the water lasted (in days) | 6±5 | 2±2 |
| Quantity of water fetched each turn (in L) | 35±22 | 106±134 |
| Sources of waterc | ||
| Individual well/community well | - | 45(56) |
| Public groundwater | 34(45) | - |
| Public standpipe | 39(51) | 14(18) |
| River | 3(4) | 21(26) |
| Caretaker involved in fetching water activity | 33(25) | 41(31) |
| Treated water before used | 4(3) | 17(13) |
aTo maintain consistency in examining variables such as walking time and days the water lasted, participants who reported using same source of water for drinking and household chores were excluded from the analyses. Hence, the sample size for this table is 80 i.e., 60% who used separate sources of water for drinking and household chores.
bParticipants were asked to estimate the time they spent walking from their houses to the specific water source.
cFor drinking water, n=76, since one participant reported using piped water at home and three participants who purchased bottled water were excluded from the analysis.
dChlorine and salt were the main agents used to treat water.
Major themes of the three areas of water insecurity
Anxiety/worry
For all the participants, having piped water was uncommon. Walking a certain distance to fetch water was a common practice among participants. Hence, anxiety related to water occurred when the normal routine of fetching water from the river, community well, or other sources was disrupted. The main thing that disrupted this routine was when a household member or caretaker was sick. Additionally, there was anxiety when water demand increased, for instance, having a newborn baby forced the caretakers to carry water from a cleaner water source, which most of the time was farther from their houses. Participants reported that the worry of having enough water also increased when the person primarily responsible for fetching water, including the caretaker, had other demanding activities to complete, such as working on the farm or going to school.
Participants were also worried about the water source, such as public groundwater and standpipe, drying up during the dry season. This concern was especially pronounced for drinking water. Therefore, water collection time greatly increased because of the reduced water flow and the long queue at the water source. Additionally, water flowed for a short period of time in the morning, and as a result, women reported waking up very early to ensure water was running and available.
Quantity/quality of water
Both the quantity and quality of water was a concern in the study area. Participants reported that during the dry season, the water they used for chores was often brown in color because of the mud. They also washed their laundry directly at the river site in order to spare the water they had at home. During the rainy season, participants often collected rain water and used it for both drinking and household purposes, making the water fetching process less of a burden for them. Those who borrowed water said they did it because their supply was finished, and there was either nobody available to carry more or the water source was closed or dry.
Sickness due to water
Only 4% of the participants reported becoming sick during the past 30 days because of lack of a clean water supply. In fact, most of the caretakers felt they had been using poor quality water all their life and couldn’t relate to the fact that fever or diarrhea could be due to the water. Nevertheless, some did acknowledge that sickness might result from contaminated water, but then they showed some resignation since there was no other option available.
Frequency of handwashing and the association with water insecurity
Hygiene behaviors
In estimating the frequency of washing hands with soap and water at the five critical stages, it was found that, on average, participants scored 8.6±1.9 with a minimum score of 0 and maximum score of 10. As indicated in Figure 2, it was seen that the hygiene/handwashing scores were significantly higher in the water secure group than the insecure group (9.2±1.2 vs. 8.2±2.3, respectively, F (1, 132)=8.096, P=0.005).
Incidence of diarrhea and other hygienerelated illnesses
Overall, 18% of caretakers in our sample reported that their children had diarrhea in the past 30 days. The most commonly reported health issues were respiratory diseases with 82% of the women reporting that the index child experienced it in the past 30 days. In a report of health statuses of the index children, 17% of the women reported their child’s health was poor.
In comparing water security versus water insecurity, a significant difference was found for incidence of diarrhea. It was found that 79% of children from water insecure households had episodes of diarrhea in the past 30 days compared with 21% of children from water secure households (P=0.022, Figure 3). Although it was not statistically significant, more children from water insecure households were reported to have health conditions, such as respiratory diseases, appetite trouble, fever, and skin infections compared with their counterparts from water secure households (Figure 3).
Figure 1.
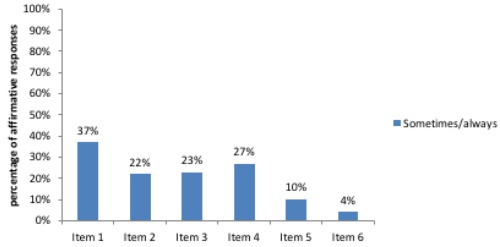
Number of affirmative responses on water security scale by each item (n=134).
Figure 2.

Differences in the total hygiene score between water secure and insecure caretakers living in rural areas of the Menoua division, West region of Cameroon (n=134)
Discussion
Overall, the results of our study indicate that water insecurity is an issue in rural areas of western Cameroon and correlates with substandard hygiene practices and incidence of diarrhea among children. Our results were similar to those of other water insecurity studies in that more than half of the participants in our study experienced some level of water insecurity. In a study conducted in Botswana, the prevalence of water insecurity was 60%, and it was associated with the daily use of an unimproved source of water.14 In a study conducted by Stevenson et al.9 in drought prone communities in Ethiopia, they found that water insecurity scores ranged from 3 points to as high as 11 points of the total 23-point/statement scale. Further, water insecurity was significantly positively associated with the use of an unprotected water source and time required to fetch water.9 In a recent study with pregnant women in Kenya, Krumdieck et al.15 found that 77% of them had at least some experience of water insecurity in the previous month. All these studies indicate that water insecurity is a common problem in rural areas of Africa.
The recent report on the progress toward the Sustainable Development Goals of clean water and sanitation indicates that, not a water shortage, but poor public service, negligence, and weak infrastructure were the primary causes of poor water access in rural areas.16 The participants in our study spent an average of 17 minutes walking from their houses to their drinking water sources. Similar results were found throughout the rest of the country. Based on the 2004 Cameroon Demographic and Health Survey (DHS) data, Pickering and Davis (2012)17 found that the mean oneway walking time from the household to the water source was approximately 20 minutes in rural areas. Results from a study conducted in Nepal showed that fetching water was a time-consuming activity and depended upon walking time to and fro, queuing time, and number of trips, and that time spent collecting water represented 56% of the total coping costs for poor households.18
In our study, the statement on anxiety and worry as a result of poor water access received the maximum affirmative responses. Similarly, several studies have found that water insecure women experience high levels of stress, anxiety, and psychosocial distress compared with women with water security.10,19,20 Our results also showed that the hygiene/handwashing level was significantly better among water secure women than insecure women. This was also found in an intervention study that also showed that improving water access resulted in a significant increase in the amount of water used for drinking and for some household chores, such as bathing, house cleaning, and laundry.10 Hence, there is a potential direct link between access to water and hygiene practices. Optimal handwashing practices at all the five critical stages means washing hands at least 10 times per day.21 This can be difficult to achieve for people who are already struggling to obtain water for drinking and for their primary household chores.
Many studies have demonstrated that optimal handwashing is associated with a reduction of diarrhea incidence among children. 22,23 A model developed by Pickering and Davis (2012)17 revealed that a fiveminute reduction in the one-way walking time to the water source could lead to a 14% decrease in diarrhea incidence. Hence, the current evidence, including our study, demonstrates the link between water access and security, hygiene practices, and reduction of diarrhea among children.
In our study, drinking water was on average stored for six days in order to reduce water fetching trips. Such a long storage of drinking water generally offers greater opportunities for pathogen contamination via repeated water withdrawal from the containers with dirty utensils and hands, resulting in more diarrhea episodes.17 The common sources of water in our study included public groundwater and wells. However, these sources of water could be causing water-related diseases since, according to the results of a study conducted in an urban area of Cameroon, 100% of wells and public groundwater sources were fecally contaminated.24
One limitation of our study would be the possibility of social desirability bias, thereby over reporting of handwashing practices. However, statistically significant differences in handwashing practices were still observed between water secure and water insecure groups. Secondly, the water insecurity scale that was used was originally developed for an urban setting. Thus, there is a possibility that certain aspects of a rural setting were not captured in the scale. Third, the study period included both the dry and wet seasons, increasing the possibility of seasonal bias in estimating prevalence of water insecurity in the study area.
Figure 3.
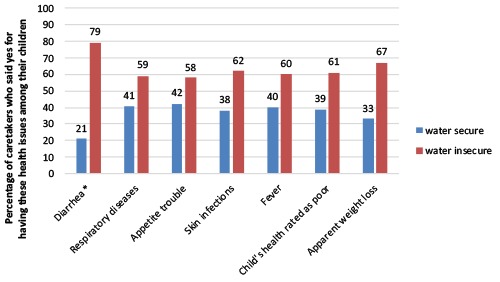
Comparison of presence of diarrhea and other health issues in the past month among children living in water secure and insecure households in rural areas of the Menoua Division-West Cameroon (n=134)
Conclusions
Results of this study confirm that water security is critical in ensuring optimal health and development among children by reducing incidences of diarrhea and promoting better hygiene practices among caretakers. Further, studies are warranted to develop a validated scale to measure water security at the household level and assess how it is associated with health behaviors among caretakers. Similar to previous literature, the results of our study also demonstrate high levels of “opportunity cost” associated with water access in a rural region, such as long walking distances to water sources and high incidence of diarrhea among children in rural areas. However, there is a knowledge gap in understanding the relationship between water insecurity, diet quality, and nutritional health among mothers and children. It is unclear how water insecurity is associated with food production at the household level, daily food intake, and growth and development of children.
Funding Statement
Funding: none.
References
- 1.Liu L, Johnson HL, Cousens S, et al. Global, regional, and national causes of child mortality: an updated systematic analysis for 2010 with time trends since 2000. Lancet 2012;379:2151-61. [DOI] [PubMed] [Google Scholar]
- 2.United Nations International Children Emergency Fund. Diarrhoea remains a leading killer of young children, despite the availability of a simple treatment solution. 2017. Available from: https://data.unicef.org/topic/childhealth/diarrhoeal-disease/ [accessed 13 September 2017] [Google Scholar]
- 3.Pruss-Ustun A, Bos R, Gore F, Bartram J. Safer water, better health: costs, benefits and sustainability of interventions to protect and promote health. Geneva: World Health Organization; 2008. [Google Scholar]
- 4.United Stated Agency for International Development. 2015 WASH & Nutrition –Water and development strategy & multi-sectoral nutrition strategy Implementation Brief. 2015. Available from: https://www.usaid.gov/sites/default/files/documents/1865/USAID_WASH_Nutrition_Brief_2015.pdf [Google Scholar]
- 5.Fewtrell L, Kaufmann RB, Kay D, et al. Water, sanitation, and hygiene interventions to reduce diarrhea in less developed countries: a systematic review and meta-analysis. Lancet Glob Health 2005;5:42-52. [DOI] [PubMed] [Google Scholar]
- 6.United Nations. The Millennium Development Goals Report. New York: United Nations; 2015. Available from: http://www.un.org/millenniumgoals/2015_MDG_Report/pdf/MDG%202015%20rev%20(July%201).pdf [Google Scholar]
- 7.United Nations Department of Economic and Social Affairs. International Decade for Action “Water for Life” 2005-2015. 2014. Available from: http://www.un.org/waterforlifedecade/human_right_to_water.shtml [accessed 1 February 2018] [Google Scholar]
- 8.Hadley C, Wutich A. Experience-based measures of food and water security: biocultural approaches to grounded measures of insecurity. Hum Org 2009;68:451-60. [Google Scholar]
- 9.Stevenson EG, Greene LE, Maes KC, et al. Water insecurity in 3 dimensions: an anthropological perspective on water and women's psychosocial distress in Ethiopia. Soc Sci Med 2012;75:392-400. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Stevenson EGJ, Ambelu A, Caruso BA, et al. Community water improvement, household water insecurity, and women’s psychological distress: an intervention and control study in Ethiopia. Plos One 2016;11:e0153432. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Aihara Y, Shrestha S, Sharma J. Household water insecurity, depression and quality of life among postnatal women living in urban Nepal. J Water Health 2016;14:317-24. [DOI] [PubMed] [Google Scholar]
- 12.Seino RA, Ghogomu RT, Manjeli Y, et al. A faunal survey of the Oedipodinae (Acrididae: Orthoptera) of the Menoua Division in Cameroon. Int J Fauna Biol Stud 2013;1:15-9. [Google Scholar]
- 13.Molua EL, Lambi CM. Climate, hydrology and water resources in Cameroon. Pretoria: The Centre for Environmental Economics and Policy in Africa (CEEPA); 2006. [Google Scholar]
- 14.Kujinga K, Vanderpost C, Mmopelwa G, Masamba WR. Analysis of gender and other social dimensions of household water insecurity in Ngamiland, Botswana. J Manag Sustain 2014;4:86. [Google Scholar]
- 15.Krumdieck NR, Collins SM, Wekesa P, et al. Household water insecurity is associated with a range of negative consequences among pregnant Kenyan women of mixed HIV status. J Water Health 2016;14:1028-31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.World Health Organization and the United Nations Children’s Fund. Progress on drinking water, sanitation and hygiene: 2017 update and SDG baselines. Geneva: 2017. Available from: https://www.unicef.org/publications/files/Progress_on_Drinking_Water_Sanitation_and_Hygiene_2017.pdf [Google Scholar]
- 17.Pickering AJ, Davis J. Freshwater availability and water fetching distance affect child health in sub-Saharan Africa. Environ Sci Technol 2012;46: 2391-7. [DOI] [PubMed] [Google Scholar]
- 18.Pattanayak SK, Yang JC, Whittington D, Bal Kumar KC. Coping with unreliable public water supplies: averting expenditures by households in Kathmandu, Nepal. Water Resour Res. 2005;41. [Google Scholar]
- 19.Aihara Y, Shrestha S, Kazama F, Nishida K. Validation of household water insecurity scale in urban Nepal. Water Policy 2015:wp2015116. [Google Scholar]
- 20.Boateng GO, Collins SM, Mbullo P, et al. A novel household water insecurity scale: Procedures and psychometric analysis among postpartum women in western Kenya. PloS One 2018; 13:e0198591. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Luby SP, Halder AK, Huda T, et al. The effect of handwashing at recommended times with water alone and with soap on child diarrhea in rural Bangladesh: an observational study. PLoS Med 2011;8:e1001052. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Ejemot-Nwadiaro RI, Ehiri JE, Arikpo D, et al. Hand washing promotion for preventing diarrhoea. Cochrane Datab Syst Rev 2015;9:1-95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Iyer P, Sara J, Curtis V, Scott B, Cardosi J. The handwashing handbook. A guide for developing a hygiene promotion program to increase handwashing with soap. Washington DC: World Bank; 2005. [Google Scholar]
- 24.Yongsi HBN. Suffering for water, suffering from water: access to drinkingwater and associated health risks in Cameroon. J Health Popul Nutr 2010;28:424-35. [DOI] [PMC free article] [PubMed] [Google Scholar]