

Abstract
Background:
High-grade glioma cells consume mainly glucose and cannot compensate for glucose restriction. Apoptosis may potentially occur under carbohydrate restriction by a ketogenic diet (KD). We explored the feasibility and safety of KD during standard treatment of chemoradiation in patients with glioblastoma multiforme.
Methods:
A full liquid KD induced ketosis within 2 weeks before start of chemoradiation. After 6 weeks, the KD was modified with solid foods and medium-chain-triglyceride emulsions and used for an additional 6 weeks while maintaining ketosis. During the total study period (14 weeks), feasibility, safety, coping (both patient and partner), quality of life (QoL), neurological functioning and impairment were measured. Overall survival was analyzed with actuarial estimates.
Results:
Eleven patients started the study protocol, nine reached ketosis and six (67%) completed the study. Severe adverse effects did not occur. The majority of coping scores ranged from 3 to 6 on a 10-point scale at all timepoints; QoL, neurological functioning, and impairment did not essentially change over time; overall survival ranged between 9.8 and 19.0 months.
Conclusion:
KD was feasible and safe as an adjuvant to standard chemoradiation treatment of glioblastoma multiforme. A supportive partner and intensive counseling were essential for coping. Future research should identify possible beneficial effects on overall survival.
Clinical trial registration:
Netherlands Trial Registry: NTR5167 (registration date 29-01-2015), http://www.trialregister.nl/trialreg/index.asp
Keywords: adjuvant therapy, brain tumor, coping, metabolic therapy, side effects
Introduction
The median survival duration of patients with glioblastoma multiforme (GBM) is 15 months after multimodal therapy combining surgery, radiotherapy (RT) and chemotherapy (CT).1 As high-grade glioma cells consume mainly glucose,2 dietary carbohydrate restriction has been suggested as a possible therapeutic strategy to improve the survival duration.3,4 In recent in vitro and in vivo studies, cancer growth was inhibited by the ketosis and increased lipolysis induced by low-carbohydrate diets.5–7 It seems, therefore, that GBM cells do not compensate for glucose restriction, whereas normal brain cells do so by metabolizing ketone bodies. Apoptosis may potentially occur under carbohydrate restriction.8,9 An extremely carbohydrate-restricted diet, the ketogenic diet (KD; high-fat, low-carbohydrate diet), could be of interest because it mimics the metabolic response to starvation when ketones become the main fuel for the brain. Although low-carbohydrate intake alone has been found effective on survival in the treatment of GBM in several animal models and in vitro studies, combining current therapies with KD was even more effective.10 For example, the KD as adjuvant to radiation therapy in mice with GBM showed an impressive synergistic effect as compared with RT alone. The underlying mechanism is not yet clarified but this effect is presumed to be higher due to radiation cytotoxicity as a result of sensitization of the tumor cells by KD.10
Although glycemic modulation by carbohydrate-restricted diets is currently a topic under investigation in cancer research, clinical data are still scarce. Systematic reviews of the preclinical and early clinical studies available suggest positive effects on survival in malignant gliomas.11–13
In summary, the KD may have several beneficial effects in cancer treatment, but more clinical data to support this is needed. However, the strict regimen of KD puts great demands on the patient and partner, with risk of noncompliance. We report a prospective study designed to test the feasibility (including coping) and safety of the KD as a treatment option for GBM in combination with standard chemoradiation treatment.
Methods
Study design
We performed an open-label, single-center, nonrandomized prospective study in adults with first diagnosis of a histologically proven GBM after surgical resection and receiving subsequent standard treatment with chemoradiation at the Erasmus MC, University Medical Center, Rotterdam, The Netherlands.
This study was approved by the local medical ethical committee of the Erasmus MC (MEC-2014-537, date of approval 19 January 2015), provided that written informed consent was obtained from both patients and partners. The study was registered in The Netherlands Trial Registry: NTR5167 (registration date 29 January 2015 http://www.trialregister.nl/trialreg/index.asp) and performed according to the Declaration of Helsinki 2013.
Patients
Patient inclusion was done stepwise. First, eligible patients were included if they met the following criteria: first diagnosis of a histologically proven GBM, age ⩾ 18 years, availability of a supportive partner or family member who is able to help with calculating, preparing and providing the meals, Karnofsky Performance Scale (KPS) score > 70, and both patient and partner able and willing to complete study-specific diaries and questionnaires. Second, inclusion was finalized if the patient had reached and sustained a ketone level of 3 mmol/l and tolerated the exclusively liquid KD formula for 3 days before start of chemoradiation.
Exclusion criteria were dexamethasone (DXM) use at time of inclusion, hypertriglyceridemia (>10 mmol/l) with or without hypercholesterolemia (>7.5 mmol/l) despite treatment, (history of) hepatic, renal, gastrointestinal or pancreatic disease, diabetes mellitus, untreated or uncontrolled hypertension, underweight [body mass index (BMI) < 16 kg/m2] or overweight (BMI > 30 kg/m2) and carbohydrate content of any concomitant medication exceeding 1000 mg/day without a suitable alternative.
Standard treatment
The standard treatment for GBM is surgery or biopsy followed by combined RT and CT. Fractionated RT with a total of 60 Gy is usually started within 6 weeks after surgery and combined with temozolomide (TMZ, 75 mg/m2) daily followed by six adjuvant 4-week cycles in which TMZ is taken for the first 5 days of every cycle. By standard protocol, all patients were prescribed DXM after surgery, to manage cerebral edema; this was stopped before start of the study.14
Ketogenic diet
The KD is a high-fat (70–90% energy), low-carbohydrate (5–19% energy) diet. Patients consumed an exclusively fluid KD with a 4:1 diet ratio (4 g fat versus 1 g protein plus carbohydrates, 90% energy from fat) from baseline to end of chemoradiation. Once a ketone level > 3 mmol/l was reached and sustained for 3 days, the patient was allowed a snack with the same 4:1 diet ratio once a day. After 6 weeks chemoradiation, the fluid KD was modified to a solid-food KD (diet ratio 1.5–2.0:1) with median chain triglyceride (MCT; 70% energy from fat with the consistency of an emulsion) which was continued for another 6 weeks. Patients and partners were encouraged to vary the KD prescriptions with recipes from a ketogenic cooking book and the use of a KD calculation program (Microsoft Office Excel, Microsoft Windows, Schiphol, The Netherlands).
During the study, the nutritional compositions of both KDs were fine tuned, based on ketone levels, glucose levels and tolerance.
Patient characteristics
Baseline patient characteristics collected were sex, age, weight, height, BMI, date of diagnosis, tumor location, kind of tumor resection, isocytric dehydrogenase type (IDH type) methylation status, methylguanide deoxyribonucleic acid methyltransferase (MGMT) methylation status, and use of antiepileptic drugs (AEDs). Resting energy expenditure (REE) was measured at baseline and after 6 weeks, 3-day food intake and physical activity data (determined with the short questionnaire to assess health-enhancing physical activity, SQUASH) were collected both at baseline, at 6 weeks and at the end of the study.
Outcome measures
The primary outcome of this study was feasibility, defined as at least 60% of patients successfully following the KD for 14 weeks after start of protocol treatment.
Feasibility was determined by tabulating the number of patients reaching and sustaining ketosis of 3 mmol/l in blood (beta-hydroxy butyrate, BHB) and having tolerated the full liquid KD for 3 days at start of chemoradiation, the number of withdrawals during the study, and the number of patients who completed the full study period of 14 weeks.
The secondary outcomes were: safety, based on adverse effects (AEs), adequate and stable ketosis (3–4 mmol/l), extent of coping with the KD by both patient and partner, quality of life (QoL), neurological functioning, functional impairment (KPS) and overall survival (OS), defined as time from diagnosis till date of death.
Safety was measured by recording all AEs ⩾ grade 2, based on common terminology criteria of adverse events (CTCAE, version 4.03 2010, Nih publication no 09-5410, US dept of Health and Human Services, USA).15 AEs (e.g. gastrointestinal complaints, fatigue) were all noted in a study diary and reviewed weekly by the dietician.
Laboratory parameters (e.g. lipid profile, carnitine, lactate) other than those required for the standard treatment protocol14 were collected at baseline, after 6 weeks and at the end of the study. Blood ketone levels (once a day in the afternoon) and glucose levels (twice a day, fasting and in the afternoon) were measured with an electronic device, noted in a study diary and reviewed daily by the dietician. Glucose levels > 2.5 mmol/l were considered adequate.
The ability of coping with the diet was measured at baseline, after 6 weeks and at the end of the study with our self-designed questionnaires for both patient and partner (questionnaires are shown as supplementary material). They included 12 (baseline), 15 (6 weeks) or 14 (end of study) questions. Items addressed were, for example, the practical information provided, daily measurement of glucose and ketone levels, and calculating and preparing recipes. The item scores could range from 0 to 10 and indicated the level of difficulty experienced when applying the KD in daily practice and coping with it, with 10 being the highest level of difficulty. Other items reflecting the level of received information could range from 0 to 10 (0 reflecting adequate and 10 reflecting not enough).
QoL was measured with the EORTC QLQ-C-30 (version 3, Êuropean Organization for Research and Treatment of Cancer, Protocol 15861, Amsterdam, The Netherlands)16 at the start, after 6 weeks, and at the end of the study and compared with normative data of the Dutch cancer survival population.17 EORTC QLQ-30 scores were transformed to 0–100 scores using standard procedures and calculations.
A neurologist examined the patients at the start and end of the study. Adaptive behavior of the patient was assessed at start and end of the study with the Vineland Adaptive Behavior Scales: interview edition, expanded form (VABS II, version 2005, NCS Pearson, Inc. Bloomington MN, USA18). The patient’s level of functional impairment was measured with the KPS19 at baseline and at the end of the study.
OS was calculated as time in months from diagnosis to death.
Study procedures
Figure 1 shows the flowchart of the study procedures.
Figure 1.

Study flow chart.
BMI, body mass index; CT, chemotherapy; KD, ketogenic diet; MCT, medium-chain triglycerides; RT, radiotherapy.
The patient and his/her partner were extensively informed by the neurosurgeon and dietician and included in the study when inclusion criteria were met and informed consent was signed.
The carbohydrate content of all prescribed medication was evaluated by the pharmacist and, if necessary, the medication was changed not to exceed 1000 mg/day. We distinguished two study phases. Phase A marked the start of the exclusively fluid KD continued during the period of chemoradiation. Phase B marked the end of chemoradiation and modification of the liquid KD into KD-MCT.
The patient and partner were daily coached by telephone or e-mail by the dietician and a nurse practitioner and were seen monthly in the outpatient clinic. Any additional support was provided on an individual basis.
Statistical analysis
Data analysis was mainly descriptive and restricted to the patients who had reached ketosis and maintained it for at least 3 days before CT/RT treatment (i.e. the patients who started phase A). Data included were: the number of patients included in the study, the number of days on KD, the reason for not starting with the KD protocol treatment and the reason for early termination (i.e. <14 weeks on the KD). Individual ketone and glucose levels and those of the total group were summarized and are presented as mean (standard deviation, SD) or, in the case of skewed data, median (IQR). The analysis of adverse events and serious adverse events was done by tabulation of the incidence and nature. OS was analyzed with actuarial estimates and illustrated with a Kaplan–Meier plot. All analyses were performed using SPSS version 23 (IBM SPSS Statistics for Windows, IBM, Armonk, NY, US) and Stata 14 (Stata Statistical Software, StataCorp LP, College Station, TX, US).
Results
Between February 2015 and April 2017, eleven patients (nine men) and their partners were included in the study. One patient wished to withdraw 1 day after inclusion; another patient was excluded 1 day after inclusion because of refractory epileptic seizures which required intensive care admission. The remaining nine patients started phase A.
The median age of the nine patients included in phase A was 53.8 years (IQR 32).
Patient characteristics are shown in Table 1.
Table 1.
Characteristics of patients included in phase A.
| n = 9 | ||||
| Sex, M (%) | 8 (89) | |||
| Age, years, median (IQR) | 53.8 (22.5) | |||
| Tumor location | Temporal: 4 Occipital: 3 Parietal: 1 Frontal: 1 |
|||
| Tumor resection | Total: 4 Subtotal: 5 |
|||
| IDH 1 mutational status | Negative: 9 Positive: – |
|||
| MGMT promotor methylation status | Positive: – Negative: 2 Unknown: 7 |
|||
| AED use, n, (%) | 7 (78) | |||
| BMI, kg/m2, median (IQR) | Start of study (n = 9): 25 (2.5) | |||
| End of study (n = 6): 24 (4.2) | ||||
|
Time from diagnosis to start KD
weeks, median (IQR) |
3.3 (1.1) | |||
|
REE baseline
median (IQR) |
||||
| Indirect calorimetry | Kcal: 2020 (325) | |||
| Harris–Benedict equation | Kcal: 1713 (389) | |||
|
REE after 6 weeks diet (n = 8)
median (IQR) |
||||
| Indirect calorimetry | Kcal: 1983 (587) | |||
| Harris–Benedict equation | Kcal: 1680 (437) | |||
|
Caloric intake prior to trial per day
median (IQR) |
Kcal: 1996 (382) Carbohydrates: 123 (183) g, (24.6% energy) |
|||
|
Diet phase A: full liquid KD 4:1 per day
median (IQR) |
Kcal: | 2400 (878) | ||
| Protein: | 49 (16) g, (8.2% energy) | |||
| Carbohydrates: | 11 (1.5) g, (2.0% energy) | |||
| Fat: | 237 (69) g, (88.8% energy) | |||
| Diet ratio (fat:carbohydrate+protein): | 4:1 (0) | |||
| Diet phase B: KD with MCT (n = 8) per day, median (IQR) | Kcal: | 2835 (662) | ||
| Protein: | 54 (24) g, (7.6% energy) | |||
| Carbohydrates: | 57 (14) g, (8.0% energy) | |||
| Fat: | 266 (51) g, (84.4% energy) | |||
| Diet ratio (fat:carbohydrate + protein): | 2.2:1 (0.7) | |||
| Physical activity (based on SQUASH) | Start | 6 weeks | End of study | |
| (n = 9) | (n = 8) | (n = 6) | ||
| Normal (n) | 9 | 8 | 6 | |
| Decreased (n) | – | – | – | |
|
Karnofsky Performance Score
median score (IQR) |
Start | End of study | ||
| (n = 9) | (n = 6) | |||
| 95/100 (10) | 90/100 (15) | |||
AEDs, anti-epileptic drugs; BMI, body mass index; IDH 1, isocytrate dehydrogenase type I; IQR, interquartile range; KD, ketogenic diet; M, Male; MCT, medium-chain triglyceride; MGMT, methylguanine deoxyribonucleic acid methyltransferase; REE, resting energy expenditure; SQUASH, short questionnaire to assess health-enhancing physical activity.
Feasibility
During phase A, one patient withdrew after 2 weeks for family reasons (illness of a supporting partner). During phase B, one patient could not tolerate the MCT emulsion and stopped, and one patient was not compliant during the last week of the study and was withdrawn from the study.
Thus, eventually, six out of nine patients (67%) adhered to the KD for the full 14 weeks of the study.
Safety
Seven out of nine patients (78%) suffered from seizures at baseline, and were treated with AEDs. The observed AEs of CTCAE grade 1 were constipation (n = 7), nausea/vomiting (n = 2), hypercholesterolemia (n = 1), hypoglycemia at initiation (n = 1), low carnitine (n = 1), and diarrhea (n = 1). These episodes were mainly transient and could be treated by medication or dietary adjustments. Reported AEs of CTCAE grade 2 included hallucinations (n = 1), allergic reaction (n = 1) and wound infection (n = 1). Other reported severe adverse events were related to seizures (n = 3), ambulatory problems (n = 1) and recurrent wound infection (n = 1).
The lipid profiles showed mainly normal values. One patient experienced hypercholesterolemia (7.4 mmol/l) that normalized with medication (4.5 mmol/l).
One patient had to restart DXM (with a dosage of 8 mg/day) because of neurological deterioration (with ambulatory problems) during the first week of RT and continued using a lower dosage of 1 mg/day for the further duration of the study.
Nine patients reached adequate ketosis (>3 mmol/l) in a mean of 4.5 days (SD 0.91) and had a mean ketone level of 4.3 mmol/l (SD 1.20) during phase A and of 2.9 mmol/l (SD 1.17) during phase B.
The glucose levels of these nine patients were normal with a mean evening glucose level of 4.7 mmol/l (SD 0.17) during phase A and of 5.2 mmol/l (SD 0.70) during phase B. None of the patients showed hyperketosis (defined as ⩾6.5 mmol/l). One patient showed hypoglycemia (defined as ⩽2.5 mmol/l) with a blood glucose level of 2.0 mmol/l once, during KD initiation, due to an extended overnight fast. Table 2 shows treatment characteristics.
Table 2.
Treatment characteristics of all patients (n = 10).
| Patient | Sex | Included
phase A |
Completed
study |
Total
carnitine start, mmol/l |
Lipids
chol, TG start, end study mmol/l |
Lactate
start, end study mmol/l |
IGF-1
start, end study nmol/l |
HbA1c
start, end study mmol/l |
Glucose level
phase A mmol/l mean, SD |
Glucose
level phase B mmol/l mean, SD |
Ketone
level phase A mmol/l mean, SD |
Ketone
level phase B mmol/l mean, SD |
Time on KD
days |
Diet after study
Type of diet |
OS
months |
Age
years |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | M | Yes | No | 50.9 | Chol: 6.20 TG: 0.82 | 1.2 | 16.7 | 36 | 4.5 (NA) | – | 3.50 (NA) | – | 15 | – | 18.4 | 65.5 |
| 2 | M | Yes | No | 33.2 | Chol: 4.3 TG: 0.77 Chol: 4.6 TG: 0.88 |
2.4 0.9 |
– | 32 31 |
4.6 (0.31) | 5.4 (0.76) | 4.98 (0.87) | 3.14 (0.83) |
96 | Modified Atkins Diet |
9.76 | 41.2 |
| 3 | M | Yes | Yes | 57.9 | Chol: 5.2 TG: 1.81 Chol: 4.7 TG: 1.06 |
1.2 0.7 |
17.2 21.9 |
33 23 |
4.6 (0.78) | 5.0 (0.70) | 4.84 (1.07) | 3.69 (1.15) |
97 | KD-MCT | 19.02 | 36.4 |
| 4 | M | Yes | Yes | 28.6 | Chol: 3.9 TG: 1.07 Chol: 4.7 TG: 2.41 |
1.2 1.3 |
30.4 17.9 |
29 25 |
4.4 (0.66) | 5.4 (0.81) | 4.97 (0.83) | 2.44 (1.03) |
97 | KD-MCT | 12.32 | 33.5 |
| 5 | M | Yes | Yes | 34.1 | Chol: 5.9 TG: 1.65 Chol: 5.9 TG: 1.48 |
1.8 1.2 |
12.4 13.2 |
39 31 |
4.8 (0.72) | 5.4 (0.57) | 5.39 (1.05) | 2.51 (0.98) |
98 | Modified Atkins Diet |
15.31 | 53.1 |
| 6 | F | Yes | No | 21.3 | Chol: 6.5 TG: 1.16 | 0.90 | 17.9 | 36 | 4.6 (0.71) | 5.3 (0.30) | 3.50 (0.65) | 1.38 (0.77) |
65 | Modified Atkins Diet |
9.89 | 62.9 |
| 7 | M | No | No | 31.6 | Chol: 4.7 TG:0.83 | 1.5 | 7.2 | – | – | – | – | – | – | – | 10.32 | 55.8 |
| 8 | M | Yes | Yes | 44.5 | Chol: 4.7 TG: 1.61 Chol: 3.9 TG: 1.92 |
– 0.9 |
20.6 35.9 |
40 29 |
4.7 (0.84) | 5.8 (0.59) | 4.47 (1.07) | 3.10 (1.09) |
99 | Modified Atkins Diet |
11.10 | 59.8 |
| 9 | M | Yes | Yes | 51.4 | Chol: 5.8 TG: 0.75 Chol: 7.4 TG: 1.80 |
1.3 – |
15.5 20.0 |
38 31 |
5.2 (0.47) | 5.0 (0.53) | 3.11 (0.66) | 3.27 (1.20) |
95 | KD-MCT | 17.71 | 53.8 |
| 10 | M | Yes | Yes | 34.4 | Chol: 5.9 TG: 0.66 Chol: 6.0 TG: 1.52 |
0.7 1.0 |
22.0 16.8 |
34 36 |
5.0 (0.63) | 5.0 (0.74) | 3.28 (0.84) | 2.19 (0.58) |
104 | KD-MCT | 12.78 | 55.5 |
Legenda:
Chol, cholesterol; F, female; HbA1c, glycated hemoglobulin; IGF-1, insulin growth factor 1; KD, ketogenic diet; M, male; MCT, medium-chain triglycerides; NA, not applicable; OS, overall survival; TG, triglyceride.
Coping
Data from the coping questionnaires indicate that both patients and partners expected hardly any difficulty at start; however, in daily practice they were facing some challenges. The majority of the coping scores ranged from median 3 to median 6 on a 10-point scale at all three timepoints.
Both types of KD were found slightly more difficult to cope with than expected. The introduction of a ketogenic snack was important for adhering to the exclusively fluid KD. In daily practice, preparing suitable menus proved more difficult than expected for the patient but not for the partner.
Patients and partners reported that intensive counseling by the dietician was needed, not only to solve practical problems, but also to stay motivated. Nevertheless, all patients continued using a kind of carbohydrate-restricted diet after the end of the study during the additional 6-month period of cyclic CT; four of them continued the KD with MCT emulsions and had contact with the research team at regular outpatient visits. Data from the coping questionnaires are available as supplemental material.
Quality of life
Data from QoL questionnaires showed normal values as compared with the normative data from the Dutch cohort17 in 13/15 items at baseline versus 12/15 at end of the study. However, the proportion of patients in our study who were fatigued at start and stayed fatigued during the study was higher than normal and this also held true for pain and insomnia after 6 weeks of chemoradiation. Complaints of nausea and vomiting decreased over time, whereas gastrointestinal complaints were reported throughout the whole study period. Table 3 shows QoL data.
Table 3.
Quality-of-life median scores at baseline, after 6 weeks, and end of study.
| Baseline
(%, min–max) (n = 9) |
6 weeks
(%, min–max) (n = 8) |
End of study
(%, min–max) (n = 6) |
Reference
value41 |
||
|---|---|---|---|---|---|
| Global quality of life |
83 (50–92) |
67 (33–83) |
58 (0–75) |
78 | |
| Functioning scales: | Physical | 100 (87–100) |
97 (92–100) |
93 (75–100) |
90 |
| Role | 93 (33–100) |
83 (17–100) |
67 (50–100) |
89 | |
| Emotional | 88 (58–100) |
67 (58–100) |
75 (67–92) |
89 | |
| Cognitive | 83 (50–100) |
83 (67–100) |
83 (67–100) |
92 | |
| Social | 75 (33–100) |
67 (33–100) |
100 (67–100) |
94 | |
| Symptom scales: | Fatigue | 28 (0–56) |
39 (11–44) |
22 (11–67) |
17 |
| Vomiting/nausea | 0 (0–83) |
0 (0–33) |
0 (0–17) |
2.7 | |
| Pain | 0 (0–17) |
0 (0–67) |
0 (0–0) |
15 | |
| Single items: | Dyspnea | 0 (0–0) |
0 (0–0) |
0 (0–33) |
7.1 |
| Insomnia | 0 (0–33) |
0 (0–67) |
0 (0–0) |
14 | |
| Appetite loss | 0 (0–67) |
0 (0–33) |
0 (0–67) |
3.3 | |
| Constipation | 0 (0–33) |
33 (0–67) |
0 (0–67) |
4.8 | |
| Diarrhea | 0 (0–33) |
0 (0–33) |
0 (0–33) |
3.9 | |
| Financial difficulties |
0 (0–67) |
0 (0–33) |
0 (0–33) |
3.1 |
Neurological functioning and functional impairment
On the VASB II, each patient obtained a maximum score on the ‘motor skills’ and ‘communication’ domains at both the start and end of the study. Each patient was slightly impaired on the domains ‘daily living skills’ and ‘socialization’ but scores in these domains did not differ between the start and end of the study for all. The median group KPS decreased from 95 (IQR 10) at the start to 90 (IQR 15) at the end of the study.
Survival
The median OS of the nine patients was 12.8 months (IQR 12.3–17.7, range 9.8–19.0). Two patients survived for 17.7 and 19.0 months, respectively. Figure 2 illustrates the Kaplan–Meier plot of OS.
Figure 2.
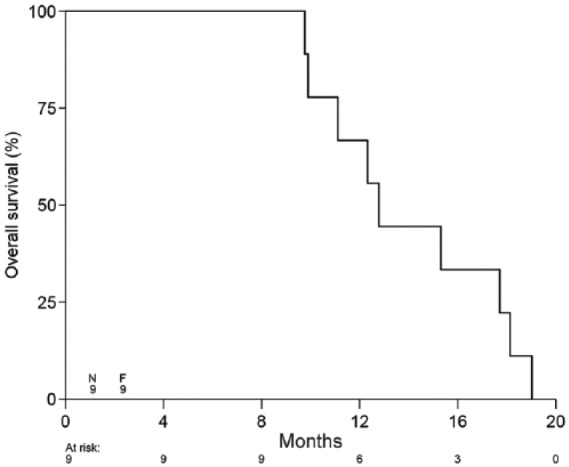
Kaplan–Meier plot of overall survival stratified by time interval between diagnosis and death.
n represents the number of patients at the start of the study; F represents the number of failures.
Nine patients were included into phase A of the study: at 4 months and 8 months after diagnosis, nine had survived; at 12 months after diagnosis, six had survived; at 16 months after diagnosis three had survived; and at 20 months, all had died.
Discussion
In this clinical study, patients with GBM consumed a strict KD in addition to chemoradiation after first surgery. They reached strong ketosis before starting chemoradiation and were able to maintain it during the total study period.
The safety outcomes in this study were in line with those in previous studies.20–24 The reported adverse events were mild and temporary and could be resolved by medical treatment or dietary adjustments. All serious AEs registered during this study were considered not related to dietary treatment.
QoL, neurological functioning and KPS outcomes did not change essentially during the study. The median OS was lower than generally expected, although the cohort consisted of relatively young patients in good performance status who had undergone total or subtotal resection, that is, patients with favorable prognostic characteristics. However, all patients who entered phase A included those who had confirmed IDH 1 wildtype, which is negatively associated with OS.25 The MGMT promotor methylation status, which is a predictor of positive response to TMZ treatment,26 was negative in two patients and unknown in seven. The small sample size precluded correcting for confounding factors, and thus, a definite statement on the efficacy of KD on OS cannot be made.
All patients continued using a carbohydrate-restricted diet after the end of the study, with variable intake of carbohydrates, resulting in substantially decreased ketone levels. Two patients with a prolonged survival duration (17.7 and 19.0 months, respectively) had continued consuming large amounts of MCT emulsions after the study period ended and were able to maintain strong ketosis. It is not clear which factor might have favored this outcome. Currently a subject of interest in cancer research, dietary carbohydrate restriction such as use of KD is thought to help the host fight against this tumor type when ketones become the main fuel for the brain. To date, only limited data from clinical trials in malignant brain tumors are available, based on small cohorts of patients or case reports.20–22,24,27–30 Data from animal studies suggest a KD combined with energy restriction (ERKD, energy restriction range of 30–40%) may prolong survival.31–33 In clinical practice, additional energy restriction is more likely to negatively influence tolerability and adherence to the diet.23,28 In line with this, intermittent fasting might be an alternative.34,35 Because the dietary composition and time of diet onset differ between all studies, it is hard to tell which strategy is most beneficial to OS.
We hypothesized that maintaining strict ketosis during the 6 weeks of chemoradiation was crucial to maximizing the potential beneficial effect of the combined therapies. After these 6 weeks, we allowed liberalization of the diet. The question is whether we chose the right KD modification. Still, other kinds of liberal KDs like the modified Atkins Diet and the Low Glycemic Index Diet (40–60 g carbohydrate/day with a glycemic index > 50, high fat and protein intake)36 would not have produced the high levels of ketones we aimed for in this study. Nevertheless, despite the modification of the KD, our patients and partners had some problems varying the menus and some reported difficulty consuming the large volume of prescribed MCT emulsions. Additionally, the carbohydrate restriction of the KD-MCT used in our study was in line with diets of previous studies.20–22,37
Our study has several strengths. First, in clinical practice, chemoradiation therapy is started soon after surgery and we were able to successfully initiate KD and instruct patients and their partners within this small timeframe because of a strict and well-structured protocol. An adequate state of strong ketosis was reached within less than a week without major side effects and could be sustained during the study period. Second, we included patients with partners who could help them comply with this highly demanding diet. Our study is in line with the lessons learned from Schwartz et al.24 where a supporting partner, apart from intensive coaching by a dietician and nurse practitioner, is of importance for successful implementation and adherence to the diet.
Still, several limitations need to be addressed. First, during a 2-year period, only 10 patients could be included, of whom only 9 were included into phase A. We had expected that many eligible patients confronted with severe brain disease and a poor prognosis would decline participation due to the experimental character of our study. Therefore, probably only those families highly interested in nutrition were likely to participate. Our strict inclusion criteria may also have hampered inclusion of more patients. Although the feasibility study of Martin-McGill et al.29 reported sending questionnaires to 172 patients with brain tumors, only 6 patients with GBM initially started a modified KD, of which 4 completed the study of 12 weeks and no data on survival were reported. Only Rieger et al.22 described a larger cohort of GBM patients (n = 20), of whom only those with secondary tumor progression used the KD, and not those patients receiving regular upfront chemoradiation.
Second, the exclusion of patients needing DXM might have caused selection bias.
Third, although we proved that a 3 mmol/l level of ketosis could be achieved by a very strict full liquid version of the KD under normoglycemia, an association with OS could not be established in this small cohort of patients. The mouse study of Abdelwahab et al.,10 showed a significant difference in OS with adjuvant KD during RT. However, the increased BHB levels (>2 mmol/l) measured in their study were even lower than the levels we achieved, although BHB levels are not to be extrapolated 1:1 from rodents to humans.10 Lastly, as questionnaires for evaluation of the dietary application were not available in the literature, we used a self-designed one, which had not yet been validated.
Conclusion
This study suggests that the use of KD as adjuvant to standard treatment, with chemoradiation after first surgery, is feasible and safe in patients with GBM. The value of this study should be regarded in light of upcoming metabolic therapy trials which will be performed in several types of cancer. Specifically, in GBM, there are three studies ongoing.38–40
Given that the KD proved feasible, future studies should focus on the use of modified versions of the KD, with a nutritional composition that induces at least a moderate level of ketosis. A less-strict diet might be crucial to recruit a cohort large enough to explore if survival in GBM benefits from metabolic therapy when it is combined with other treatment modalities. In future studies, early identification of GBM patients who would particularly benefit form KD as add-on therapy should be systematically explored by studying the mutational and methylation status of the tumor, as well as using imaging techniques to identify relevant tumor biomarkers with rapid response to ketosis.
Supplemental Material
Supplemental material, Supplemental_Materials_coping_patient_and_partner_rebuttal_07032019_JFO for Ketogenic diet treatment as adjuvant to standard treatment of glioblastoma multiforme: a feasibility and safety study by Elles J. T. M. van der Louw, Joanne F. Olieman, Patricia M. L. A. van den Bemt, Jacoline E. C. Bromberg, Esther Oomen-de Hoop, Rinze F. Neuteboom, Coriene E. Catsman-Berrevoets and Arnaud J. P. E. Vincent in Therapeutic Advances in Medical Oncology
Acknowledgments
We would like to thank Yoeri Fransen for his contribution to the data collection; Marten Poley for his advice on data analysis, Nelly van der Meer-van de Velden, Ilse Oosterom and Tessa van de Klundert of the Clinical Trial Center for their contribution to the data collection and study monitoring; and Diane Coule and Marit Eland, Nurse Practitioners at from the Department of Neurosurgery for their valuable patient support.
Footnotes
Funding: This study was in part supported by the Dutch Cancer Society (EMCR 2014-6124) and Danone Nutricia Research BV (ISS15EP89704.1.160922A).
Conflict of interest statement: The authors declare that there is no conflict of interest.
Supplemental material: Supplemental material for this article is available online.
ORCID iD: Elles JTM van der Louw  https://orcid.org/0000-0003-3245-0471
https://orcid.org/0000-0003-3245-0471
Contributor Information
Elles J. T. M. van der Louw, Department of Dietetics, Erasmus MC, University Medical Center, Dr. Molewaterplein 40, Rotterdam, Zuid Holland 3015 GD, The Netherlands.
Joanne F. Olieman, Department of Dietetics Erasmus MC, University Medical Center, Rotterdam, The Netherlands
Patricia M. L. A. van den Bemt, Department of Hospital Pharmacy, University Medical Center, Rotterdam, The Netherlands
Jacoline E. C. Bromberg, Department of Neurology, University Medical Center, Rotterdam, The Netherlands
Esther Oomen-de Hoop, Department of Medical Oncology, University Medical Center, Rotterdam, The Netherlands.
Rinze F. Neuteboom, Department of Neurology, University Medical Center, Rotterdam, The Netherlands
Coriene E. Catsman-Berrevoets, Department of Neurology, University Medical Center, Rotterdam, The Netherlands
Arnaud J. P. E. Vincent, Department of Neurosurgery, University Medical Center, Rotterdam, The Netherlands
References
- 1. Awad AW, Karsy M, Sanai N, et al. Impact of removed tumor volume and location on patient outcome in glioblastoma. J Neurooncol 2017; 135: 161–171. [DOI] [PubMed] [Google Scholar]
- 2. Roslin M, Henriksson R, Bergstrom P, et al. Baseline levels of glucose metabolites, glutamate and glycerol in malignant glioma assessed by stereotactic microdialysis. J Neurooncol 2003; 61: 151–160. [DOI] [PubMed] [Google Scholar]
- 3. Seyfried TN, Flores R, Poff AM, et al. Metabolic therapy: a new paradigm for managing malignant brain cancer. Cancer Lett 2015; 356: 289–300. [DOI] [PubMed] [Google Scholar]
- 4. Woolf EC, Syed N, Scheck AC. Tumor metabolism, the ketogenic diet and beta-hydroxybutyrate: novel approaches to adjuvant brain tumor therapy. Front Mol Neurosci 2016; 9: 122. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Martuscello RT, Vedam-Mai V, McCarthy DJ, et al. A supplemented high-fat low-carbohydrate diet for the treatment of glioblastoma. Clin Cancer Res 2016; 22: 2482–2495. [DOI] [PubMed] [Google Scholar]
- 6. Maurer GD, Brucker DP, Bahr O, et al. Differential utilization of ketone bodies by neurons and glioma cell lines: a rationale for ketogenic diet as experimental glioma therapy. BMC Cancer 2011; 11: 315. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Lussier DM, Woolf EC, Johnson JL, et al. Enhanced immunity in a mouse model of malignant glioma is mediated by a therapeutic ketogenic diet. BMC Cancer 2016; 16: 310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Seyfried TN, Mukherjee P. Targeting energy metabolism in brain cancer: review and hypothesis. Nutr Metab (Lond) 2005; 2: 30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Seyfried TN, Sanderson TM, El-Abbadi MM, et al. Role of glucose and ketone bodies in the metabolic control of experimental brain cancer. Br J Cancer 2003; 89: 1375–1382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Abdelwahab MG, Fenton KE, Preul MC, et al. The ketogenic diet is an effective adjuvant to radiation therapy for the treatment of malignant glioma. PLoS One 2012; 7: e36197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Strowd RE, Cervenka MC, Henry BJ, et al. Glycemic modulation in neuro-oncology: experience and future directions using a modified Atkins diet for high-grade brain tumors. Neurooncol Pract 2015; 2: 127–136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Winter SF, Loebel F, Dietrich J. Role of ketogenic metabolic therapy in malignant glioma: a systematic review. Crit Rev Oncol Hematol 2017; 112: 41–58. [DOI] [PubMed] [Google Scholar]
- 13. Noorlag L, De Vos FY, Kok A, et al. Treatment of malignant gliomas with ketogenic or caloric restricted diets: a systematic review of preclinical and early clinical studies. Clin Nutr 2018; pii: S0261-5614(18)32519-6. [DOI] [PubMed] [Google Scholar]
- 14. Stupp R, Mason WP, Van den Bent MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med 2005; 352: 987–996. [DOI] [PubMed] [Google Scholar]
- 15. National Cancer Institute UDoHaHS. Common Terminology Criteria for Adverse Events. http://ctep.cancer.gov/protocolDevelopment/electronicapplications/ctc.htm (2010).
- 16. Aaronson NK, Ahmedzai S, Bergman B, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst 1993; 85: 365–376. [DOI] [PubMed] [Google Scholar]
- 17. Van de Poll-Franse LV, Mols F, Gundy CM, et al. Normative data for the EORTC QLQ-C30 and EORTC-sexuality items in the general Dutch population. Eur J Cancer 2011; 47: 667–675. [DOI] [PubMed] [Google Scholar]
- 18. Sparrow SS, Cicchetti DV, Balla DA. Vineland adaptive behavior scales second edition: survey forms manual. Circle Pines MN, USA: American Guidance Service; 2005. [Google Scholar]
- 19. Mor V, Laliberte L, Morris JN, et al. The Karnofsky Performance Status Scale. An examination of its reliability and validity in a research setting. Cancer 1984; 53: 2002–2007. [DOI] [PubMed] [Google Scholar]
- 20. Fine EJ, Segal-Isaacson CJ, Feinman RD, et al. Targeting insulin inhibition as a metabolic therapy in advanced cancer: a pilot safety and feasibility dietary trial in 10 patients. Nutrition 2012; 28: 1028–1035. [DOI] [PubMed] [Google Scholar]
- 21. Champ CE, Palmer JD, Volek JS, et al. Targeting metabolism with a ketogenic diet during the treatment of glioblastoma multiforme. J Neurooncol 2014; 117: 125–131. [DOI] [PubMed] [Google Scholar]
- 22. Rieger J, Bahr O, Maurer GD, et al. ERGO: a pilot study of ketogenic diet in recurrent glioblastoma. Int J Oncol 2014; 44: 1843–1852. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Schwartz K, Chang HT, Nikolai M, et al. Treatment of glioma patients with ketogenic diets: report of two cases treated with an IRB-approved energy-restricted ketogenic diet protocol and review of the literature. Cancer Metab 2015; 3: 3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Schwartz KA, Noel M, Nikolai M, et al. Investigating the ketogenic diet as treatment for primary aggressive brain cancer: challenges and lessons learned. Front Nutr 2018; 5: 11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Yan H, Parsons DW, Jin G, et al. IDH1 and IDH2 mutations in gliomas. N Engl J Med 2009; 360: 765–773. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Hegi ME, Genbrugge E, Gorlia T, et al. MGMT promoter methylation cutoff with safety margin for selecting glioblastoma patients into trials omitting temozolomide: a pooled analysis of four clinical trials. Clin Cancer Res. Epub ahead of print 4 December 2018. DOI: 10.1158/1078-0432.CCR-18-3181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Nebeling LC, Miraldi F, Shurin SB, et al. Effects of a ketogenic diet on tumor metabolism and nutritional status in pediatric oncology patients: two case reports. J Am Coll Nutr 1995; 14: 202–208. [DOI] [PubMed] [Google Scholar]
- 28. Zuccoli G, Marcello N, Pisanello A, et al. Metabolic management of glioblastoma multiforme using standard therapy together with a restricted ketogenic diet: case report. Nutr Metab (Lond) 2010; 7: 33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Martin-McGill KJ, Marson AG, Tudur Smith C, et al. The modified ketogenic diet in adults with glioblastoma: an evaluation of feasibility and deliverability within the National Health Service. Nutr Cancer 2018; 70: 643–649. [DOI] [PubMed] [Google Scholar]
- 30. Van der Louw E, Reddingius RE, Olieman JF, et al. Ketogenic diet treatment in recurrent diffuse intrinsic pontine glioma in children: a safety and feasibility study. Pediatr Blood Cancer 2019; 66: e27561. [DOI] [PubMed] [Google Scholar]
- 31. Jiang YS, Wang FR. Caloric restriction reduces edema and prolongs survival in a mouse glioma model. J Neurooncol 2013; 114: 25–32. [DOI] [PubMed] [Google Scholar]
- 32. Mukherjee P, Abate LE, Seyfried TN. Antiangiogenic and proapoptotic effects of dietary restriction on experimental mouse and human brain tumors. Clin Cancer Res 2004; 10: 5622–5629. [DOI] [PubMed] [Google Scholar]
- 33. Shelton LM, Huysentruyt LC, Mukherjee P, et al. Calorie restriction as an anti-invasive therapy for malignant brain cancer in the VM mouse. ASN Neuro 2010; 2: e00038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Safdie F, Brandhorst S, Wei M, et al. Fasting enhances the response of glioma to chemo- and radiotherapy. PLoS One 2012; 7: e44603. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Lee C, Raffaghello L, Brandhorst S, et al. Fasting cycles retard growth of tumors and sensitize a range of cancer cell types to chemotherapy. Sci Transl Med 2012; 4: 124ra27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Miranda MJ, Turner Z, Magrath G. Alternative diets to the classical ketogenic diet–can we be more liberal? Epilepsy Res 2012; 100: 278–285. [DOI] [PubMed] [Google Scholar]
- 37. Nebeling LC, Lerner E. Implementing a ketogenic diet based on medium-chain triglyceride oil in pediatric patients with cancer. J Am Diet Assoc 1995; 95: 693–697. [DOI] [PubMed] [Google Scholar]
- 38. Klein P. Ketogenic diet as adjuvant treatment in refractory/end-stage glioblastoma multiforme: a pilot study. https://clinicaltrials.gov/ct2/show/NCT01865162?term=ketogenic (2013, accessed 30 March 2013).
- 39. Scheck A. Phase I/II prospective trial for newly diagnosed GBM, with upfront gross or subtotal resection, followed by ketogenic diet with radiotherapy and concurrent temodar(R) chemotherapy followed by adjuvant temodar(R) chemotherapy. https://clinicaltrials.gov/ct2/show/NCT02046187?term=ketogenic+diet (2014, accessed 27 January 2014).
- 40. Schwartz K. Pilot study of a metabolic nutritional therapy for the management of primary brain tumors. https://clinicaltrials.gov/ct2/show/NCT01535911?term=ketogenic+diet (2012, accessed 20 February 2012).
- 41. Van de Poll-Franse LV, Mols F, Gundy CM, et al. Normative data for the EORTC QLQ-C30 and EORTC-sexuality items in the general Dutch population. Eur J Cancer 2011; 47(5): 667–675. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplemental material, Supplemental_Materials_coping_patient_and_partner_rebuttal_07032019_JFO for Ketogenic diet treatment as adjuvant to standard treatment of glioblastoma multiforme: a feasibility and safety study by Elles J. T. M. van der Louw, Joanne F. Olieman, Patricia M. L. A. van den Bemt, Jacoline E. C. Bromberg, Esther Oomen-de Hoop, Rinze F. Neuteboom, Coriene E. Catsman-Berrevoets and Arnaud J. P. E. Vincent in Therapeutic Advances in Medical Oncology