

Abstract
Earlier evidence has revealed a bi‐directional causal relationship between anxiety and attention biases in adults and children. This study investigated the prospective and concurrent relations between anxiety and attentional bias in a sample of 89 families (mothers, fathers, and first‐born children). Parents’ and children's attentional bias was measured when children were 7.5 years old, using both a visual probe task and visual search task with angry versus happy facial expressions. Generalized and social anxiety symptoms in parents and children were measured when children were 4.5 and 7.5 years old. Anxiety in parents and children was prospectively (but not concurrently) related to their respective attentional biases to threat: All participants showed a larger attentional bias to threat in the visual search (but not in the visual probe) task if they were more anxious at the 4.5 (but not at the 7.5) year measurement. Moreover, parents’ anxiety levels were prospectively predictive of the visual search attentional bias of their children after controlling for child anxiety. More anxiety in mothers at 4.5 years was related to a faster detection of angry among happy faces, while more anxiety in fathers predicted a faster detection of happy among angry faces in children at 7.5 years. We found no direct association between parental and child attentional biases. Our study contributes to the recently emerging literature on attentional biases as a potential mechanism in the intergenerational transmission of anxiety by showing that parents’ anxiety rather than parents’ attentional bias contributes to the intergenerational transmission of risk for child anxiety.
Keywords: anxiety, attentional bias, fathers, visual probe task, visual search task
RESEARCH HIGHLIGHTS.
Attentional bias to threat is assumed to play a role in the development of anxiety disorders in adults and children, and in its parent‐to‐child transmission.
This study shows that earlier anxiety is related to later attentional biases to threat (in children and in adults/parents).
This study reveals that earlier anxiety in mothers and fathers are related to later attentional biases in children (over and above children's own anxiety).
We conclude that children of anxious parents may develop an attentional bias to threat which may contribute to risk for later anxiety (disorders).
1. INTRODUCTION
Anxiety disorders are among the most prevalent childhood (Polanczyk, Salum, Sugaya, Caye, & Rohde, 2015) and adulthood psychopathologies (Remes, Brayne, van der Linde, & Lafortune, 2016). Anxiety disorders run in families (Beidel & Turner, 1997; Gar, Hudson, & Rapee, 2005): The presence of an anxiety disorder in parents corresponds to up to a sevenfold increase in the anxiety disorders in the offspring (Turner, Beidel, & Costello, 1987; Turner, Beidel, & Epstein, 1991). Both the genetic transmission of anxiety vulnerabilities and the environmental influences derived from growing up with an anxious parent have been found to contribute to the overlap between parents’ and their offspring's anxiety (Eley, McAdams, Rijsdijk, Lichtenstein, Narusyte, Reiss, & Neiderhiser, 2015). However, little is known regarding the specific mechanisms supporting familial aggregation (Rapee, 2002).
Cognitive theories highlight the prioritized processing of threat as a central mechanism in the development of anxiety in children and adults (for a review, see Van Bockstaele, Verschuere, Tibboel, De Houwer, Crombez, & Koster, 2014). More specifically, attentional bias, defined as the preferential allocation of attention to threatening stimuli over other categories of stimuli, may play a central role in anxiety disorders. A first meta‐analysis by Bar‐Haim, Lamy, Pergamin, Bakermans‐Kranenburg, and van IJzendoorn (2007) showed that anxious individuals indeed attend more to threatening information in their environment than non‐anxious individuals. This attentional bias towards threat has been demonstrated in samples of adults and children with different anxiety problems and using different methodologies, although the results of individual studies have been argued to be less consistent (Van Bockstaele et al., 2014). A more recent meta‐analysis from Dudeney, Sharpe, and Hunt (2015) replicated Bar‐Haim et al. (2007) by showing that an attentional bias towards threat is also present in high‐anxious children (for a recent large‐scale study, see Abend et al., 2018; for a more critical view, see Roy, Dennis, & Warner, 2015).
Until recently, little attention was given to the question how development affects information processing biases to threat. Building on the main conceptualizations of development by Ollendick and colleagues (Ollendick, Grills, & King, 2001; Ollendick & Vasey, 1999), Field and Lester (b) described three potential developmental trajectories, namely, integral bias models, moderation models, and acquisition models. While integral bias models assume no developmental influence on attentional biases to threat, Field and Lester argued that moderation and acquisition models were more likely. In these models, development exerts an influence on attention biases, either by moderating the expression of an existing (innate) attentional bias to threat or by leading to later acquisition of these biases. To date, little is known about how development influences attention biases, as well as on how development influences the association between attentional biases and anxiety.
Cognitive theories of anxiety consider attentional bias a vulnerability factor for later anxiety disorders (e.g. Eysenck, 1992; Williams, Watts, MacLeod, & Mathews, 1997), and a review of the literature indicated that the relation between attentional bias and anxiety is likely bi‐directional and mutually reinforcing, so that attentional bias maintains or increases levels of anxiety, and anxiety in turn increases attentional bias (Van Bockstaele et al., 2014). Given that attentional bias in children may thus be a precursor for later anxiety problems, a fine‐grained understanding of the development of attentional bias at young ages is imperative.
In a parallel vein, cognitive‐behavioural models of intergenerational anxiety transmission highlight the transmission of threat‐related information processing biases from parents to children as a central mechanism in familial aggregation (Creswell, Cooper, & Murray, 2010). These models postulate similarities in parents’ and children's processing of threat in the case of parental anxiety. Anxious parents’ biased information processing of threat may also extend to threats in their child's environment, altering parental behaviours. Field and Lester (2010a) suggest that each confrontation of the parent and the child with ambiguity is a trial in a real‐life cognitive bias training by parents. Anxious parents who are, by definition, more likely to see ambiguity as threat are more likely to react with more anxiety to such ambiguity. As such, they may model an anxious information‐processing style and sensitize child information processing to threat (also see Hadwin, Garner, & Perez‐Olivas, 2006).
A number of studies support the idea that children of anxious parents have an attentional bias themselves. Moradi, Neshat‐Doost, Taghavi, Yule, and Dalgleish (1999) found that children of parents with PTSD were slower to name the colours of threat‐related words than neutral words in an emotional Stroop paradigm (Williams, Mathews, & MacLeod, 1996), although they did not differ from a control group in anxiety levels. A more recent study by Schneider, Unnewehr, In‐Albon, and Margraf (2008) did not replicate this finding in children of parents with panic disorder. In a similar paradigm, they found no significant differences in Stroop interference for panic‐related words relative to control words. A study by Montagner et al. (2016) further revealed that the link between parental emotional disorders and child attention biases to threat may differ as a function of child gender. In this study, daughters of mothers with any emotional disorder were shown to have an attentional bias to threat. In turn, an attentional bias to threat was only observed in sons of depressed mothers, while no attentional bias was observed in the sons of mothers with anxiety problems or mothers with comorbid depression and anxiety problems.
Mogg, Wilson, Hayward, Cunning, and Bradley (2012) were the first to compare attentional bias among anxious parents and their children. In a sample of mothers with panic disorder and their daughters versus a control group of mothers without panic disorder and their daughters, they measured attentional bias using a visual probe task (MacLeod, Mathews, & Tata, 1986). In this task, two cue stimuli (words or pictures) were presented simultaneously on different locations on a computer screen, followed by a target stimulus on either location. One of these cues was related to physical threat, while the other cue was neutral. Attentional bias towards threat in the visual probe task is typically inferred from faster reaction times (RTs) on trials where the target appears on the location of the threatening cue (congruent trials) compared to trials where the target appears on the location of the neutral cue (incongruent trials). Although Mogg et al. (2012) found no differences in attentional bias between mothers with lifetime panic disorder and control mothers without panic disorder history, they did find that daughters of mothers with panic disorder had a larger attentional bias towards threat when cues were presented for 1,250 ms (but not when they were presented for 500 ms) than daughters of mothers in the control group. Finally, anxiety measures of mothers were significantly correlated with attentional bias scores of their daughters, although attentional bias scores of mothers and daughters were not correlated. Interesting as these findings are, they are also controversial. Waters, Forrest, Peters, Bradley, and Mogg (2015; for a recent follow‐up, see Waters, Candy, & Candy, 2017) used a similar procedure as Mogg et al. (2012) in a sample of mothers with a history of depression or anxiety disorders and their children. They found no differences in attentional bias between children of mothers with a history of emotional disorders and children of mothers in a control group, and no association between mothers’ anxiety levels and children's attentional bias for threat.
In sum, although the intergenerational transmission of attentional bias and anxiety is an emerging topic, results thus far have been largely inconsistent. One of the main reasons for these inconsistencies likely relates to the paradigms that have been used to measure attentional bias. Both the visual probe task and the emotional Stroop task yield notoriously unreliable attentional bias scores, both in adults (Schmukle, 2005) and children (Brown et al., 2014). Although both tasks could be useful in cross‐sectional designs, they are less suitable for research on individual differences (De Schryver, Hughes, Rosseel, & De Houwer, 2016; Staugaard, 2009).
This study aimed to extend the existing evidence on the links between parent–child anxiety disorders and attentional bias in several ways. First, earlier studies investigating the links between parent and child attention biases were mostly limited to cross‐sectional designs. Considering the potentially mutually reinforcing relation between attention and anxiety, a longitudinal investigation of the prospective and concurrent associations of anxiety in both parents and children with attentional bias is essential to better understand the role of parents’ attention patterns in child anxiety.
Second, as our brief overview of the literature reveals, the available evidence focused almost exclusively on mothers’ anxiety and mothers’ attentional bias to test these relations. To our knowledge, no studies thus far incorporated the crucial role that fathers may play in the development of child anxiety and familial aggregation over and above the mothers’ role. The studies including fathers (Moradi et al., 1999; Schneider et al., 2008) did not address the separate contributions of mothers’ and fathers’ anxiety, likely because the number of participating fathers was too small. Our study thus aimed to shed light on the separate contributions of mothers’ and fathers’ anxiety and attentional bias to child anxiety and attentional bias. The inclusion of maternal and paternal anxiety and attentional bias, in addition to children's profiles, also enabled the comparison of the link between anxiety and attentional bias across parents and children.
Third, in contrast with earlier studies that focused on PTSD and panic disorder, our study aimed to extend the investigation of the parent–child anxiety and attentional bias link to two of the most prevalent anxiety disorders and its precursors, namely, Social Anxiety Disorder (SAD) and Generalized Anxiety Disorder (GAD). Both disorders have early‐onset forms (De Lijster et al., 2017; Hoehn‐Saric, Hazlett, & McLeod, 1993), are fairly stable over the course of development (Wittchen & Fehm, 2003; Wittchen & Hoyer, 2001), and influence patterns of psychopathology into adulthood (Beesdo, Knappe, & Pine, 2009). In addition, attentional bias for negative facial expressions has been demonstrated in both social and generalized anxiety disorders (e.g. Bradley, Mogg, White, Groom, & De Bono, 1999; Mogg, Philippot, & Bradley, 2004).
Finally, as briefly discussed above, previous studies have largely relied on single unreliable attentional bias measures. In our study, we not only assessed attentional bias with the visual probe task but also with a visual search task, which has been shown to yield more reliable estimates of attentional bias (Brown et al., 2014; Van Bockstaele, Salemink, Bögels, & Wiers, 2017; Van Bockstaele et al., submitted).
We assessed attentional bias in a sample of mothers, fathers, and their 7.5‐year‐old children who were part of a longitudinal study on the intergenerational transmission of anxiety (Aktar, Majdandžić, De Vente, & Bögels, 2017; Nikolić, Aktar, Bögels, Colonnesi, & de Vente, 2018). We addressed three research questions (see Figure 1 for an overview): First, we investigated the concurrent and predictive associations between anxiety and attentional bias, and tested whether these associations differed across parents and children. We expected that both parents and children would show a stronger attentional bias to threat if they were more anxious (Bar‐Haim et al., 2007; Dudeney et al., 2015).
Figure 1.
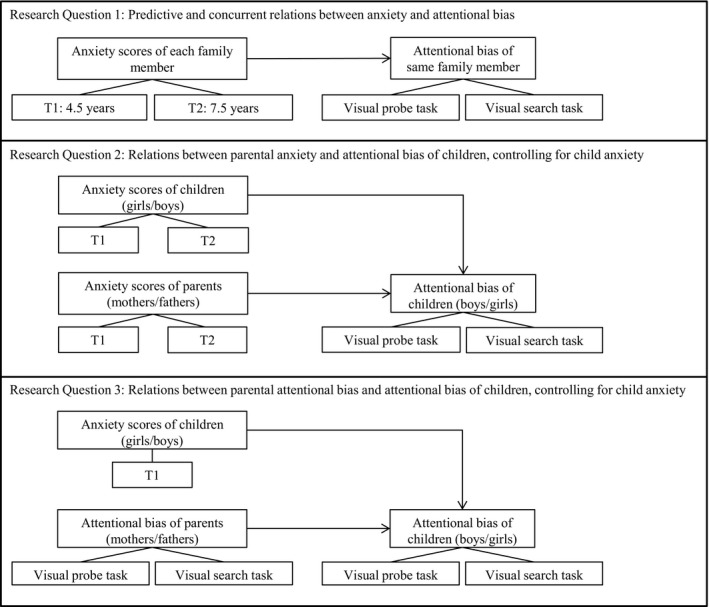
A schematic overview of research questions in this study. T1 refers to measurements when children were 4.5 years old and T2 refers to measurements when children were 7.5 years old.
Second, we investigated both concurrent and prospective links between maternal and paternal anxiety and attentional bias in children, after controlling for child anxiety. Based on cognitive models of anxiety and its intergenerational transmission (Creswell et al., 2010; Field & Lester, 2010a), we expected that children who have more anxious parents and who were more anxious themselves would show a stronger attentional bias to threat. In the light of the evidence revealing differential associations between parent anxiety and child attentional bias for boys and girls (Montagner et al., 2016), we additionally explored the moderation of these links by child gender.
Third, we investigated the direct concurrent link between attentional bias in parents and attentional bias in children. Based on cognitive‐behavioural models of anxiety transmission (Creswell et al., 2010, Field & Lester, 2010a,b), we expected a direct positive association between attentional bias to threat of parents and attentional bias in their children.
2. METHOD
2.1. Participants
The sample consisted of 89 families (89 children: Mean Age = 7.52, SD = 0.08, 47 girls; 89 mothers: Mean Age = 39.12, SD = 4.23; and 89 fathers: Mean Age = 43.04, SD = 9.62) with partially or fully available data for parents and/or children (for numbers of children, mothers, and fathers per task/measure, see Tables 1 and 2). The separate sample sizes from mothers, fathers, and children allow sufficient power for the analyses of individual differences (Maas & Hox, 2005). Participating parents were predominantly Dutch (89.89% of mothers and 96.59% of fathers were born in the Netherlands), had high levels of education (on an 8‐point scale from 1: primary education to 8: university, mean education level was 7.23, SD = 1.00, for mothers, and 6.65, SD = 1.74, for fathers) and employment (on an 11‐point scale from 1: manual labour for which no education is required to 11: labour for which a university degree is required, mean professional level was 8.83, SD = 2.22, for mothers, and 8.38, SD = 2.41, for fathers. 88.37% of mothers and 92.10% of fathers had full‐time or part‐time jobs). The participants were part of a larger community sample, recruited for a longitudinal study on the development of shyness and social anxiety (for a more elaborate description of this longitudinal sample, see Aktar, Majdandžić, de Vente, & Bögels, 2013; De Vente, Majdandžić, Colonnesi, & Bögels, 2011). This longitudinal study started during pregnancy (T0, N = 151), and continued up to the point where children were 7.5 years old. This study makes use of the data from the 4.5‐year‐old and 7.5‐year‐old measurements (referred as T1 and T2 respectively). Data from T0 were only used in the computation of lifetime psychopathology at T1. At T2, children completed a house visit during which the attention tasks were completed. From actively participating families of this sample (N = 117 at T1 and N = 114 at T2), the house visit was conducted with 93 families. Data from four of the families who participated in the house visit were unavailable (the data from the house visit was lost in three families due to experimenter error, and the tasks could not be completed with one family due to time restrictions). Children of families who completed the attention tasks did not differ from the non‐completers on age (p = 0.612) or gender (p = 0.508), and parents did not differ on educational (p = 0.900, and 0.175 for mothers and fathers respectively) or professional (p = 0.504 and 0.441 respectively) level.
Table 1.
Descriptive statistics and raw associations between parents’ and children's anxiety symptoms
| Descriptive statistics | Correlations | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| N | Min. | Max. | M | SD | 1 | 2 | 3 | 4 | 5 | |
| 1. Child anxiety symptoms at T1 | 89 | 0.00 | 3.00 | 0.26 | 0.49 | |||||
| 2. Child anxiety symptoms at T2 | 89 | 1.00 | 2.22 | 1.36 | 0.28 | 0.60** | ||||
| 3. Maternal anxiety symptoms at T1 | 89 | 0.00 | 3.50 | 0.98 | 1.09 | 0.13 | 0.32** | |||
| 4. Maternal anxiety symptoms at T2 | 82 | 1.00 | 2.33 | 1.47 | 0.36 | 0.12 | 0.36** | 0.67** | ||
| 5. Paternal anxiety symptoms at T1 | 89 | 0.00 | 3.75 | 0.87 | 0.99 | 0.19 | 0.11 | 0.39** | 0.24* | |
| 6. Paternal anxiety symptoms at T2 | 69 | 1.00 | 2.28 | 1.31 | 0.31 | 0.04 | 0.07 | 0.31** | 0.25* | 0.60** |
*p ≤ 0.05, **p ≤ 0.01.
Table 2.
Descriptive statistics and correlations between parents’ and children's attentional bias
| Descriptive statistics | Correlations | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| N | Min. | Max. | M | SD | 1 | 2 | 3 | 4 | 5 | |
| 1. Child AB in VPT | 85 | −110 | 133 | −5 | 43 | |||||
| 2. Child AB in VST | 81 | −891 | 2,826 | 670 | 744 | 0.03 | ||||
| 3. Maternal AB in VPT | 88 | −40 | 88 | 4 | 23 | 0.05 | −0.23* | |||
| 4. Maternal AB in VST | 84 | −537 | 876 | 31 | 285 | −0.04 | 0.16 | 0.00 | ||
| 5. Paternal AB in VPT | 84 | −40 | 49 | 1 | 19 | −0.14 | −0.06 | 0.10 | 0.08 | |
| 6. Paternal AB in VST | 82 | −978 | 881 | −21 | 360 | −0.14 | −0.12 | 0.13 | −0.02 | 0.03 |
*p ≤ 0.05, AB = Attentional Bias, VPT = Visual Probe Task, VST = Visual Search Task.
2.2. Instruments
2.2.1. Parental psychopathology
Parents’ current and lifetime SAD and GAD symptoms were measured twice using the Anxiety Disorder Interview Schedule (ADIS; Di Nardo, Brown, & Barlow, 1994), first during pregnancy (T0) and next during the 4.5‐year measurement (T1). Additionally, parents reported their GAD and SAD symptoms in the adult version of the Screen for Child Anxiety Related Emotional Disorders (SCARED‐A: Bögels & Van Melick, 2004) during the 7.5‐year measurement (T2).
Parental psychopathology at T1
Parental psychopathology at T1 was calculated by combining the ADIS data of the pregnancy measurement and the 4.5‐year measurement. The prenatal ADIS data were available for all 89 families who participated in our current study. The inter‐observer reliability of symptom scores at T0 was obtained from 17 mothers and 17 fathers whose recordings were double coded. The intra‐class correlations ranged from 0.98 to 1.00 for mothers’ and fathers’ current and lifetime SAD and GAD symptoms. The intra‐class correlations could not be computed for fathers’ report of current and past GAD in the prenatal measurement due to lack of variance, while the inter‐observer agreement was 100%.
ADIS scores at T1 were available for 87 mothers and 83 fathers. To establish inter‐observer reliability, a trained coder recoded the videos from 20 mothers’ and 15 fathers’ measurements. The intra‐class correlations ranged from 0.94 to 1.00 for mothers’ and fathers’ current and past SAD symptoms. The intra‐class correlations could not be computed for mothers’ and fathers’ report of their own GAD due to lack of variance (i.e. the number of GAD symptoms was 0 for all scores in this randomly selected subsample), while the inter‐observer agreement was 100%.
The measurement of lifetime SAD and GAD at T1 was dependent on T0, such that the lifetime diagnoses at T1 only covered the period from T0 to T1. After aggregating the ADIS data across T0 and T1, in the current sample of 89 families, 40 mothers and 38 fathers had a current and/or lifetime SAD diagnosis at T0 and/or T1, and 13 mothers and 9 fathers had a current and/or lifetime GAD diagnosis. Thus, the prevalence of GAD and SAD in the current sample was substantially higher than in the general Dutch population (Bijl, Ravelli, & Van Zessen, 1998). This is likely due to the fact that families were explicitly informed about the focus of this study on the development of shyness and social anxiety at the time of recruitment. Parents with dispositions for anxiety may have showed a more pronounced interest to be part of this longitudinal study, leading to an overrepresentation in our sample.
In contrast to the commonly used categorical approach to psychopathology focusing on the presence/absence of diagnosis, we adopted a dimensional approach to psychopathology (Brown & Barlow, 2005; Hudziak, Achenbach, Althoff, & Pine, 2007). We used the mean number of SAD and GAD symptoms from the ADIS across the T0 and T1 measurements to compute anxiety scores at T1. This allowed us to preserve the naturally occurring inter‐individual variation in the levels of psychopathology in our community sample. For parents with missing ADIS data at T1, we used the averages of current and lifetime symptoms at T0. GAD and SAD symptoms in parents did not significantly differ between families who completed the attention tasks and non‐completers in this sample (neither at T0 nor at T1, p's ranging from 0.082 to 0.987).
Parental psychopathology at T2
At the 7.5‐year measurement, both parents filled in the adult version of the Screen for Child Anxiety Related Emotional Disorders (SCARED‐A: Bögels & Van Melick, 2004). This questionnaire consists of 58 items measuring anxiety on 3‐point scales. The SAD and GAD subscales each consisted of 9 items, and parental anxiety scores at T2 were operationalized as the average of these two subscales. The SCARED‐A data were available for 82 mothers and 69 fathers. The internal consistency of parental SAD and GAD symptoms ranged between 0.83 and 0.89 in this study.
2.2.2. Child psychopathology
Children's SAD and GAD symptoms were also measured twice, first at T1 using the parent version of Anxiety Disorder Interview Schedule for child psychopathology (ADIS‐C; Silverman & Albano, 1996), and at T2 using parental reports of GAD and SAD in the Screen for Child Anxiety Related Emotional Disorders (SCARED‐P: Birmaher et al., 1999).
Child psychopathology at T1
Both parents completed the ADIS interview for child psychopathology. To establish inter‐observer reliability, a trained coder recoded the videos from the child interview of 20 mothers and 15 fathers. The intra‐class correlations of parent‐reported SAD and GAD symptoms ranged from 0.938 to 1.000. The intra‐class correlations could not be computed for mothers’ report of child GAD due to lack of variance (i.e. the number of child GAD symptoms was 0 for all scores in this randomly selected subsample), while the inter‐observer agreement was 100%. Child psychopathology data were available for 87 mothers and 83 fathers in the current sample. Children of families who completed the current tasks did not significantly differ from non‐completers on SAD and GAD symptoms (neither in mothers’ nor in fathers’ report, p's ranging from 0.172 to 0.955). To obtain the final symptom scores for children, we averaged symptoms reported by mothers and fathers about their child's GAD and SAD symptoms. In cases where the scores were missing from one parent, the scores were obtained by averaging of GAD and SAD symptoms reported by the other parent only.
Child psychopathology at T2
Both parents reported on child psychopathology using the parent version of Screen for Child Anxiety Related Emotional Disorders (SCARED‐P: Birmaher et al., 1999) at T2. The SCARED‐P consisted of 58 items, rated on 3‐point scales. The SAD and GAD subscales each consisted of nine items, and child anxiety scores at T2 were operationalized as the average of these two subscales. The SCARED‐P data on child anxiety were available from 86 mothers and 75 fathers. In cases where the scores were missing from one parent, the scores were obtained by averaging of GAD and SAD symptoms reported by the other parent only. The internal consistency of child SAD and GAD scores in our study ranged from 0.80 to 0.86.[Link]
2.3. Apparatus and materials
The attentional bias tasks were run on an ASUS TP500L laptop with a 15.6‐inch screen. The experiment was programmed using Inquisit 4 (2014). For both the visual probe task and the visual search task, we used the same 96 pictures (happy and angry expression from 24 adult female and 24 adult male actors) from the Karolinska Directed Emotional Faces database (KDEF; Lundqvist, Flykt, & Öhman, 1998). For practice blocks, we selected the angry, happy, and neutral expressions from another four female and four male actors. All pictures in the visual probe task were rescaled to 309 × 419 pixels; all pictures in the visual search task were rescaled to 169 × 229 pixels.
2.4. Visual probe task
Each trial in the visual probe task started with the presentation of a fixation cross in the centre of the screen, flanked by two grey rectangles. The rectangles were 309 pixels wide by 419 pixels high, and the centre of the rectangles was 4.5 cm away from the fixation cross. After 500 ms, the grey rectangles were replaced by a happy and an angry face of the same actor. It should be noted that, unlike most previous studies (e.g. Montagner et al., 2016; Waters, Forrest, Peters, Bradley, & Mogg, 2015; White et al., 2017), we did not compare angry or happy expressions with neutral expressions. After another 500 ms, the faces were masked by the grey rectangles, and 20 ms later the target was presented in the centre of one of the two grey rectangles. The target stimulus was an asterisk (3 mm × 3 mm) and remained on the screen until a response and the corresponding RT was registered. Participants were required to respond as fast and as accurately as possible to the location of the target by pressing the left or right button of a response box. The inter‐trial interval was 850 ms.
On congruent trials, the target appeared on the location of the angry face; on incongruent trials, the target appeared on the location of the happy face. The test block consisted of 48 trials, 24 of which were congruent and 24 were incongruent. Half of the faces in both congruent and incongruent trials were male, the other half were female. Targets appeared equally often in the right and the left location. Prior to the test block, participants completed a practice block, consisting of eight trials in which only neutral faces were presented. In the practice block, error feedback was provided upon incorrect responses. The data of the practice block were not analysed.
2.5. Visual search task
The visual search task was modelled after the task used by Van Bockstaele et al. (2017). Each trial started with the presentation of a white fixation cross against a black background for 500 ms. Next, eight different faces appeared on the screen in a 3 × 3 matrix with the middle position empty. In the first test block, a single angry target face was presented amidst seven happy distractors. In the second test block, a single happy face was presented amidst seven angry distractors. Participants were asked to click as fast as possible on the target face, and the next trial started 500 ms after a response and the corresponding RT was registered. Each individual face was presented equally often, target faces appeared equally often on each of the eight possible locations, and the same face was never presented on several locations within the same trial.
Each test block was preceded by a practice block of eight trials, in which error feedback was provided upon incorrect responses. The data of the practice blocks were not analysed. We created two versions of the test blocks: One for parents and one for children. Each test block in the child version consisted of 24 trials, while each test block in the parent version consisted of 48 trials. Because we were mainly interested in individual differences, the order of the two blocks was not counterbalanced: All participants started with the find‐angry block, followed by the find‐happy block.
2.6. Procedure
The study was conducted in quiet rooms in the participating families’ homes. Test sessions were planned individually to maximize the availability of both parents. In order to minimize method variance and maximize person‐related variance (Perugini, Richetin, & Zogmaister, 2010), the attentional bias tasks were conducted in a fixed order: First, one parent completed the visual probe task, followed by the visual probe measurement of the child, the visual search task for both parents, the visual probe task of the second parent, and the visual search task of the child. While one family member completed an attentional bias task, other members of the family completed the questionnaires or performed other tasks, mostly related to parenting behaviours, which were not part of the current study. The entire procedure was approved by the ethical committee of the University of Amsterdam.
3. RESULTS
3.1. Preliminary analyses
Descriptive statistics and raw associations between parents’ and children's anxiety scores at T1 and T2 are presented in Tables 1 and 2. The amount of individual variation in child anxiety symptom counts in the current sample was relatively low at T1, and did not include more severe forms of child anxiety (range 0–3 symptoms). There was continuity in the anxiety scores, as significant moderate associations appeared between anxiety scores at T1 and T2 (r = 0.60 for children, 0.67 for mothers, and 0.60 for fathers). These associations suggest that both anxiety measures at T1 and T2 are tapping into similar latent constructs. Moreover, there were modest associations between mothers’ reports of their own anxiety at both T1 and T2, and of child anxiety at T2 (r = 0.32 and 0.36 respectively). There were no such significant correlations between fathers’ reports of their own versus their child's anxiety. These findings suggest that a direct link between parents’ and children's anxiety is only visible with mothers. However, this link does include the measurement error coming from using parents’ rating of child anxiety. Earlier evidence (e.g. Najman, Williams, Nikles, Spence, Bor, O'Callaghan, & Andersen, 2000) has shown that mothers’ anxiety status might bias their rating of their children's levels of anxiety, while the lack of a significant association between fathers’ own anxiety and their report of child anxiety suggests that such a bias may not be present in fathers. Finally, there were significant positive associations between mothers’ and fathers’ anxiety (r = 0.39 at T1 and 0.25 at T2) which can be explained by assortative mating (e.g. Luo, 2017).
3.2. Analytic strategy for the main analyses
The data from the visual probe and visual search tasks were processed using the same approach as Van Bockstaele et al. (2017). The details of data processing are presented in the Supplement. Split‐half reliabilities of attentional bias scores in the visual probe task (mean RT on incongruent trials minus mean RT on congruent trials) were poor, with r = 0.02, p = 0.865, for children, and r = 0.18, p = 0.019, for parents.[Link] The split‐half reliability of the attentional bias scores in the visual search task (mean RT on find‐happy block minus mean RT on find‐angry block) was better, with r = 0.39, p < 0.001, for children, and r = 0.53, p < 0.001, for parents.
RTs served as the outcome measure in all analyses. The data had a hierarchical structure with trials, nested in trial type, nested in family members, nested in families, and were analysed in repeated multi‐level regression models. All continuous variables were standardized. The sample size at the highest level of the current hierarchical structure (N = 89 families in the visual probe and 88 in the visual search) was sufficient to generate reliable estimates for the multi‐level models (Maas & Hox, 2005). We used maximum likelihood as the estimation method in all models.
In addition to the main effects, all the theoretically relevant two‐ and three‐way interactions among trial type/block, member, and the anxiety predictor were also included in the initial multi‐level models. Because non‐significant interactions consume additional degrees of freedom in the models, alter the interpretation of the lower‐order effects, and make the models more complex, we aimed to obtain the best fitting and the most parsimonious model by removing non‐significant interaction effects one by one from this model in a backwards fashion, starting with higher p‐values and higher‐order interactions (Field, 2009).
Multi‐level models generate F‐scores tests of fixed effects (in addition to β estimates, see below). Just like in ANOVAs, F‐scores provide tests of significance for overall group differences for the main effect of the categorical variables (such as family member), as well as for the higher‐order interactions including these variables. Inclusion/exclusion of initially tested interactions in the final model was based on the significance of F‐scores. In addition to the inspection of p‐values from these scores, we also checked the improvement in the model fit in each step using −2 log‐likelihood tests. These were fully consistent with our decisions based on p‐values. For conciseness, we only present F‐scores for the interaction terms. The backward method was more favourable than the alternative approach of starting with the simple main effects and adding the theoretically relevant interactions one by one in a forward fashion, as it eliminates the need to make decisions about the sequence of inclusion of separate interactions.
In addition to F‐scores, multi‐level models generate the standardized coefficient estimates β of fixed effects (which can be interpreted as Cohen's d effect size in the current analyses with standardized scores), which provide separate tests for each pair within categories, and were used to interpret the fixed effects of categorical and continuous variables in the final models. Consistent with this, in the Results section, we present the F‐scores for each of the tested interaction effects, and we use the standardized coefficient estimates β, along with the confidence intervals (in text as well as in the Tables) for the interpretation of the effects in the final models. Full models including F‐scores, coefficient estimates β, and covariance parameters appear in the supplementary tables.
3.3. Prospective and concurrent relations between anxiety and attentional bias
This section focuses on the links between participants’ own attention biases and own anxiety. In separate models, anxiety scores at T1 were used to prospectively predict attentional bias at T2, while anxiety scores at T2 were used to address the concurrent relation between anxiety and attentional bias. Both the children and the parents were included to these analyses, categorized as separate members in the models.
To test the relations between anxiety and attentional bias, we fit a three‐level multi‐level model (per task) consisting of repeated observations of trials nested in trial type (level 1), nested in participant (level 2). The intercept was estimated as a random effect. This model contained the fixed main effects of trial type (congruent vs. incongruent for the visual probe task, and search happy vs. search angry in the visual search task), family member (mother vs. father vs. child), and the anxiety predictor. Trial number was added as a control variable in the analyses.
3.3.1. Anxiety at T1 as a predictor of reaction times in the visual probe task at T2
None of the crucial interactions in the initial model with anxiety scores at T1 as the anxiety predictor was significant: The two‐way interactions between family member and trial type, F(2, 11652.05) = 0.65, p = 0.524, between trial type and anxiety, F(1, 11651.99) = 0.340, p = 0.560, between family member and anxiety, F(2, 230.57) = 0.46, p = 0.629, and the three‐way interaction among family member, trial type, and anxiety, F(2, 11652.02) = 0.84, p = 0.434, did not significantly predict RTs. This reduced the final model to a main effects model. The final model (presented in Tables 3 and S1, N = 257, 85 children, 88 mothers, and 84 fathers) did not reveal a significant attentional bias to threat: RTs did not differ between congruent and incongruent trials (β = 0.00, SE = 0.01, p = 0.830, CI = −0.02–0.02, also see Figure 2, upper panel). The overall RT differed across parents and children: Children were overall slower to respond than mothers, β = −1.47, SE = 0.07, p < 0.01, CI = −1.61 to −1.34, as well as than fathers, β = −1.52, SE = 0.07, p < 0.01, CI = −1.66 to −1.39. The link between anxiety and RT was not significant, β = −0.03, SE = 0.03, p = 0.301, CI = −0.91 to 0.28. In sum, anxiety scores at T1 were not predictive of attentional bias as measured with the visual probe task at T2.
Table 3.
Anxiety at T1 as a predictor of RT in the visual probe task at T2 (N = 257)
| Parameter | β | SE | df | t | p | 95% Confidence interval | |
|---|---|---|---|---|---|---|---|
| Lower bound | Upper bound | ||||||
| Intercept | 1.08 | 0.05 | 264.12 | 20.65 | <0.001 | 0.98 | 1.18 |
| Trial type (congruent vs. incongruent) | 0.00 | 0.01 | 11,652.17 | 0.22 | 0.830 | −0.02 | 0.02 |
| Mother (vs. child) | −1.47 | 0.07 | 187.60 | −21.69 | <0.001 | −1.61 | −1.34 |
| Father (vs. child) | −1.53 | 0.07 | 182.55 | −22.47 | <0.001 | −1.66 | −1.39 |
| Trial number | 0.00 | 0.00 | 11,654.08 | −7.26 | <0.001 | 0.00 | 0.00 |
| Anxiety symptoms at T1 | −0.03 | 0.03 | 252.58 | −1.04 | 0.301 | −0.09 | 0.03 |
Figure 2.
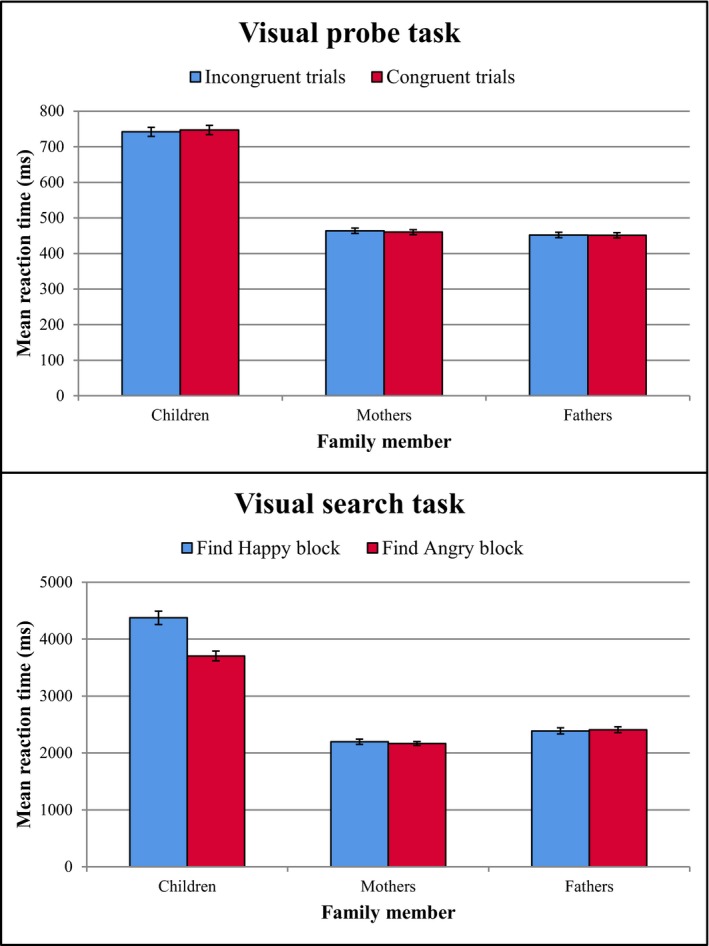
Children's, mothers’, and fathers’ mean reaction times per trial type (visual probe task) or block type (visual search task). Error bars depict ± 1 standard error of the mean.
3.3.2. Anxiety at T2 as a predictor of reaction times in the visual probe task at T2
In the next step, anxiety scores at T2 were tested as a predictor of RTs in visual probe task (N = 231). None of the interactions was significant in this model, with the two‐way interactions between trial type and family member: F(2, 10460.14) = 1.53, p = 0.217; between trial type and anxiety: F(1, 10460.19) = 0.16, p = 0.691; between family member and anxiety: F(2, 212.27) = 0.16, p = 0.849; and the three‐way interaction among trial type, family member, and anxiety: F(1, 10460.18) = 0.43, p = 0.651, reducing the final model to main effects. There was no significant association between participants’ anxiety at T2 and their RTs in the final model consisting of main effects only, β = −0.03, SE = 0.03, p = 0.311, CI = −0.93–0.30. In sum, anxiety scores at T2 were not related to either parents’ or children's attentional biases as measured with the visual probe task at T2.
3.3.3. Anxiety at T1 as a predictor of reaction times in the visual search task at T2
The model with the RTs to find happy versus angry faces as the outcome (N = 247, presented in Tables 4 and S2) revealed a significant three‐way interaction among trial type, family member, and anxiety scores, F(2, 17643.53) = 3.25, p = 0.039, which was retained in the final model: The interaction between trial type and anxiety differed between mothers and children β = −0.13, SE = 0.05, p = 0.011, CI = −0.23 to −0.03, and between fathers and children β = −0.12, SE = 0.05, p = 0.016, CI = −0.23 to −0.02. We further inspected this interaction by running separate analyses per family member, which revealed significant interactions between trial type and ADIS scores for children, n = 81, F(1, 3590.91) = 3.96, p = 0.047, mothers, n = 84, F(1, 7093.90) = 4.11, p = 0.043, and fathers, n = 82, F(1, 6962.74) = 4.40, p = 0.036 (Figure 3). Higher anxiety scores in participants were related to stronger attentional bias to threat, both in parents and children: The difference in RTs to finding happy vs. angry faces became more pronounced as participants’ anxiety increased. A closer inspection of the plots in Figure 3 revealed that the differentiation was mainly driven by an association between more anxiety and longer RTs to find happy faces among angry crowds in fathers and children. As such, it seems that more anxiety in fathers and children is related to more distraction by angry faces in fathers and in children respectively. In contrast, more anxiety symptoms in mothers were related to quicker maternal RTs to detect angry faces among happy crowds. This pattern may reflect enhanced vigilance to threat. In sum, anxiety scores at T1 were significant predictors of attentional bias as measured with the visual search task at T21 in all three family members.
Table 4.
Anxiety at T1 as a predictor of reaction times in the visual search task at T2 (N = 247)
| Parameter | β | SE | df | t | p | 95% Confidence interval | |
|---|---|---|---|---|---|---|---|
| Lower bound | Upper bound | ||||||
| Intercept | 0.72 | 0.06 | 295.79 | 11.62 | <0.001 | 0.60 | 0.84 |
| Trial type (search happy vs. search angry) | 0.55 | 0.03 | 17,646.24 | 16.04 | <0.001 | 0.48 | 0.62 |
| Mother (vs. child) | −1.08 | 0.07 | 226.50 | −14.43 | <0.001 | −1.22 | −0.93 |
| Father (vs. child) | −0.92 | 0.07 | 228.16 | −12.35 | <0.001 | −1.07 | −0.78 |
| Trial number | 0.00 | 0.00 | 17,765.26 | 3.84 | <0.001 | 0.00 | 0.00 |
| Anxiety symptoms at T1 | −0.05 | 0.09 | 288.70 | −0.57 | 0.570 | −0.22 | 0.12 |
| Mother (vs. Child) * trial type | −0.54 | 0.04 | 17,645.34 | −13.79 | <0.001 | −0.61 | −0.46 |
| Father (vs. Child) * trial type | −0.57 | 0.04 | 17,645.52 | −14.47 | <0.001 | −0.64 | −0.49 |
| Mother (vs. Child) * anxiety symptoms at T1 | 0.01 | 0.10 | 279.92 | 0.14 | 0.891 | −0.17 | 0.20 |
| Father (vs. child) * anxiety symptoms at T1 | 0.06 | 0.10 | 273.28 | 0.64 | 0.523 | −0.13 | 0.25 |
| Trial type * anxiety symptoms at T1 | 0.15 | 0.05 | 17,644.51 | 3.18 | 0.001 | 0.06 | 0.25 |
| Mother (vs. Child) * trial type * anxiety symptoms at T1 | −0.13 | 0.05 | 17,644.31 | −2.53 | 0.011 | −0.23 | −0.03 |
| Father (vs. child) * trial type * anxiety symptoms at T1 | −0.12 | 0.05 | 17,644.30 | −2.40 | 0.016 | −0.23 | −0.02 |
Figure 3.
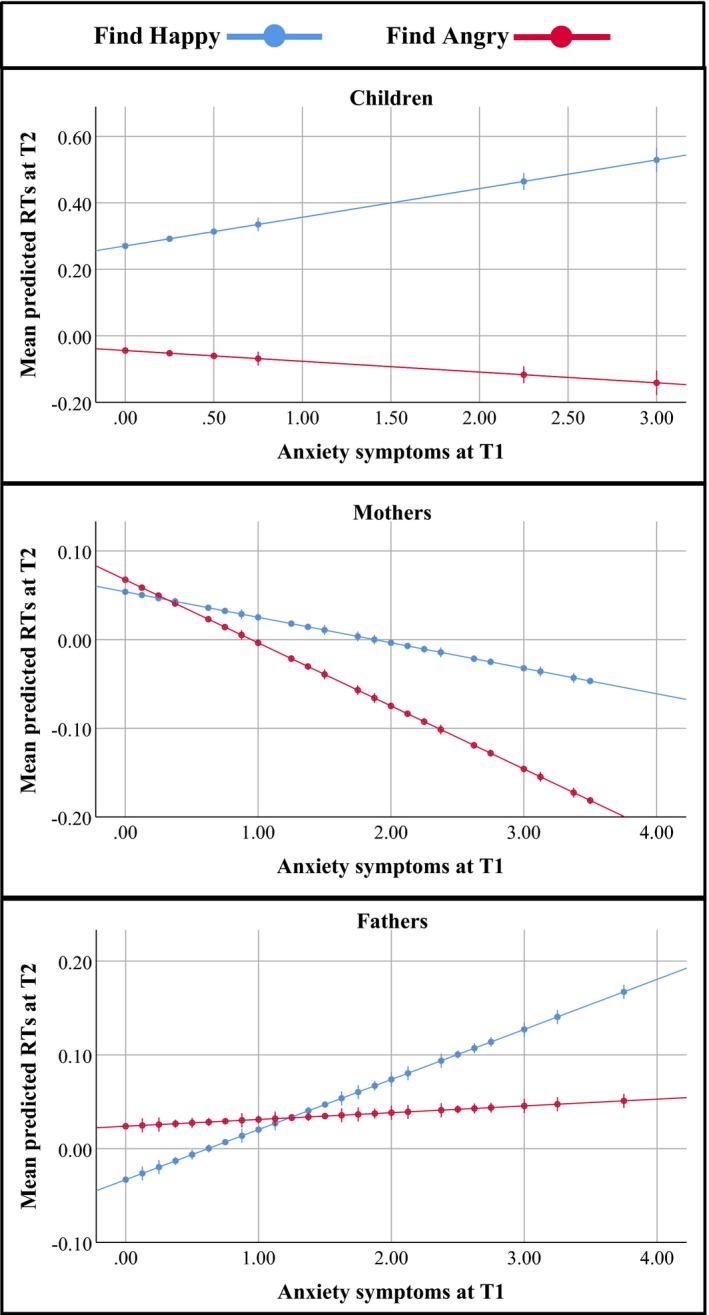
The associations between the average number of anxiety symptoms at T1, and mean predicted reaction times at T2, separately presented for children (top), and mothers (middle), and fathers (bottom). The mean RT is standardized. Error bars represent 95% confidence intervals.
3.3.4. Anxiety at T2 as a predictor of reaction times in the visual search task at T2
In the next step, anxiety at T2 was tested as a predictor of RTs in the visual search task. The initial model revealed that the following interactions were not significant: The two‐way interactions between trial type and anxiety: F(1, 15492.21) = 3.63, p = 0.057, and between family member and anxiety: F(2, 203.71) = 0.79, p = 0.453, and the three‐way interaction among trial type, family member, and anxiety: F(2, 15491.96) = 0.58, p = 0.561. There was a significant interaction between family member and trial type which was retained in the final model (N = 222), F(2, 15493.00) = 127.98, p < 0.001. Separate analyses of this effect in parents and children revealed that only children, n = 81, F(1, 3592.19) = 134.98, p <0.001, but not parents (n = 78, p = 0.435 for mothers and n = 63, p = 0.099 for fathers) showed an attentional bias towards threat in the visual search task (see Figure 2, bottom panel). Current anxiety levels were not associated with RTs in this model. In sum, the concurrent association between anxiety symptoms at T2 and attentional bias as measured with the visual search task at T2 was not significant. Overall, children did show an attentional bias for threat in the visual search task, while adults had no attentional bias.
3.4. Relations of parental anxiety and child anxiety to child attentional bias
This section focuses on the relations among child, maternal, and paternal anxiety and children's attentional biases. To test these effects, we fit an initial three‐level model for each task consisting of repeated observations of trials nested in trial type (level 1), nested in children (level 2). The random intercept was not significant, and was therefore excluded from these models. The initial model contained the fixed main effects of trial type, child gender (girls vs. boys), in addition to maternal, paternal, and child anxiety. All the two‐ and three‐way interactions between these predictors were also tested in the initial model. The main effect of trial number was included as a control variable in the analyses. We used the same strategy as above to reach the best fitting and the most parsimonious model, and tested both anxiety at T1 and anxiety at T2 as predictors of attentional bias in separate models per task.
3.4.1. Parents’ and children's anxiety at T1 as predictors of child reaction times in the visual probe task at T2
In the model with parents’ and children's anxiety scores at T1 as predictors of child attentional bias at T2, none of the tested interactions was significant: The three‐way interactions among the trial type, child gender, and anxiety of the child: F(1, 3812.07) = 0.27, p = 0.605, anxiety of the mother, F(1, 3812.11) = 1.68, p = 0.195, and anxiety of the father: F(1, 3812.14) = 0.11, p = 0.745); the two‐way interactions between trial type and anxiety of the child: F(1, 3812.07) = 0.11, p = 0.742, anxiety of the mother: F(1, 3812.11) = 0.12, p = 0.732, and anxiety of the father: F(1, 3812.14) = 0.31, p = 0.580; the two‐way interactions between child gender and anxiety of the child: (F(1, 84.88) = 0.03, p = 0.864, anxiety of the mother: F(1, 84.84) = 1.34, p = 0.251, and anxiety of the father F(1, 84.91) = 0.12, p = 0.728. The final model, reduced to main effects (N = 85), revealed no significant differences in the RTs of girls versus boys (p = 0.146). The effects of parents’ (mothers: p = 0.304; fathers: p = 0.588) or child anxiety at T1 (p = 0.297) were not significant. In sum, these results show that neither children's nor parental anxiety scores at T1 were predictive of children's attentional bias as measured with the visual probe task at T2.
3.4.2. Parents’ and children's anxiety at T2 as predictors of child reaction times in the visual probe task at T2
The multi‐level models with anxiety scores at T2 as predictors also yielded no main effect or significant interactions that included trial type (congruent vs. incongruent) in the initial model (N = 63). F‐scores for the interactions were as follows: three‐way interactions among the trial type, child gender, and anxiety of the child: F(1, 2829.25) = 0.00, p = 0.965, anxiety of the mother: F(1, 2829.10) = 0.27, p = 0.605, and anxiety of the father: F(1, 2829.11) = 0.15, p = 0.703; two‐way interactions between trial type and anxiety of the child: F(1, 2829.25) = 0.05, p = 0.829, anxiety of the mother: F(1, 2829.10) = 0.34, p = 0.559, and anxiety of the father: F(1, 2829.11) = 0.02, p = 0.888. There was a significant interaction between child gender and paternal anxiety, F(1, 63.011) = 4.24, p = 0.044, which was retained in the final model, β = 0.32, SE = 0.16, p = 0.044, CI = 0.01 to 0.64. We further inspected this interaction by running separate analyses of this association in girls and boys. These revealed that girls (but not boys) had overall slower RTs in the visual probe task if the father had higher levels of anxiety at T2, β = 0.28, SE = 0.10, p = 0.007, CI = 0.08 to 0.48. The main effects of mothers’, p = 0.924 and 0.959, for girls and boys, respectively, and children's, p = 0.630 and 0.499, anxiety at T2 were not significant neither. In sum, T2 anxiety scores of neither parents nor children were not associated with attentional bias of children as measured with the visual probe task at T2.
3.4.3. Parents’ and children's anxiety at T1 as predictors of child reaction times in the visual search task at T2
In the multi‐level model with T1 anxiety scores from parents and children as predictors of child attentional bias in the visual search task (N = 81), only the interactions between trial type and anxiety predictors were significant. F‐scores for the non‐significant interactions were as follows: three‐way interactions among the trial type, child gender, and anxiety of the child: F(1, 3591.20) = 1.90, p = 0.169, and anxiety of the mother: F(1, 3591.20) = 0.13, p = 0.716, and anxiety of the father: F(1, 3591.55) = 0.07, p = 0.787, two‐way interaction between child gender and anxiety of the child, F(1, 80.53) = 0.04, p = 0.853, anxiety of the mother, F(1, 80.27) = 0.63, p = 0.430, anxiety of the father, F(1, 80.36) = 1.37, p = 0.246.
The significant interactions between block and anxiety predictors (from mothers’, fathers’, and children) were retained in the final model presented in Tables 5 and S3. The F‐scores were as follows: the two‐way interactions between trial type (search happy vs. search angry) and mothers’ anxiety, F(1, 3591.11) = 4.22, p = 0.040, trial type and fathers’ anxiety, F(1, 3591.36) = 8.78, p = 0.003, and trial type and children's anxiety, F(1, 3590.84) = 4.56, p = 0.033, see Figure 4. More anxiety in mothers was related to more attentional bias to threat in their children, β = 0.07, SE = 0.03, p = 0.040, CI = 0.00 to 0.13, while more anxiety in fathers was related to less attentional bias to threat in their children, β = −0.09, SE = 0.03, p = 0.003, CI = −0.16 to −0.03. Closer inspection of the plots in Figure 4 reveals that the former result is mainly driven by the finding that children of mothers with higher anxiety levels were quicker to respond to the angry faces, showing an enhanced vigilance in the detection of threat‐relevant facial expressions. In contrast, children with fathers with higher anxiety levels were quicker to find the happy face among angry distractors, suggesting avoidance of threat‐relevant stimuli. In sum, we found that parental levels of anxiety at T1 were predictive of their children's levels of attentional bias as measured with the visual search task at T2, even after taking into account children's own anxiety levels at T1.
Table 5.
Parents’ and children's anxiety at T1 as predictors of child reaction times in the visual search task at T2(N = 81)
| Parameter | β | SE | df | t | p | 95% Confidence interval | |
|---|---|---|---|---|---|---|---|
| Lower bound | Upper bound | ||||||
| Intercept | −0.22 | 0.08 | 108.93 | −2.95 | .004 | −0.38 | −0.07 |
| Trial type (search happy vs. search angry) | 0.35 | 0.03 | 3,592.32 | 11.72 | <0.001 | 0.29 | 0.41 |
| Child gender (girls vs. boys) | −0.08 | 0.09 | 80.34 | −0.79 | 0.430 | −0.26 | 0.11 |
| Trial number | 0.01 | 0.00 | 3,591.26 | 4.21 | <0.001 | 0.00 | 0.01 |
| Child anxiety symptoms at T1 | −0.01 | 0.05 | 96.25 | −0.16 | 0.871 | −0.10 | 0.09 |
| Maternal anxiety symptoms at T1 | −0.07 | 0.05 | 96.08 | −1.37 | 0.174 | −0.18 | 0.03 |
| Paternal anxiety symptoms at T1 | 0.02 | 0.05 | 96.33 | 0.33 | 0.743 | −0.09 | 0.12 |
| Trial type * child anxiety symptoms at T1 | 0.06 | 0.03 | 3,590.84 | 2.13 | 0.033 | 0.01 | 0.12 |
| Trial type * maternal anxiety symptoms at T1 | 0.07 | 0.03 | 3,591.12 | 2.05 | 0.040 | 0.00 | 0.13 |
| Trial type * paternal anxiety symptoms at T1 | −0.09 | 0.03 | 3,591.36 | −2.96 | 0.003 | −0.16 | −0.03 |
Figure 4.
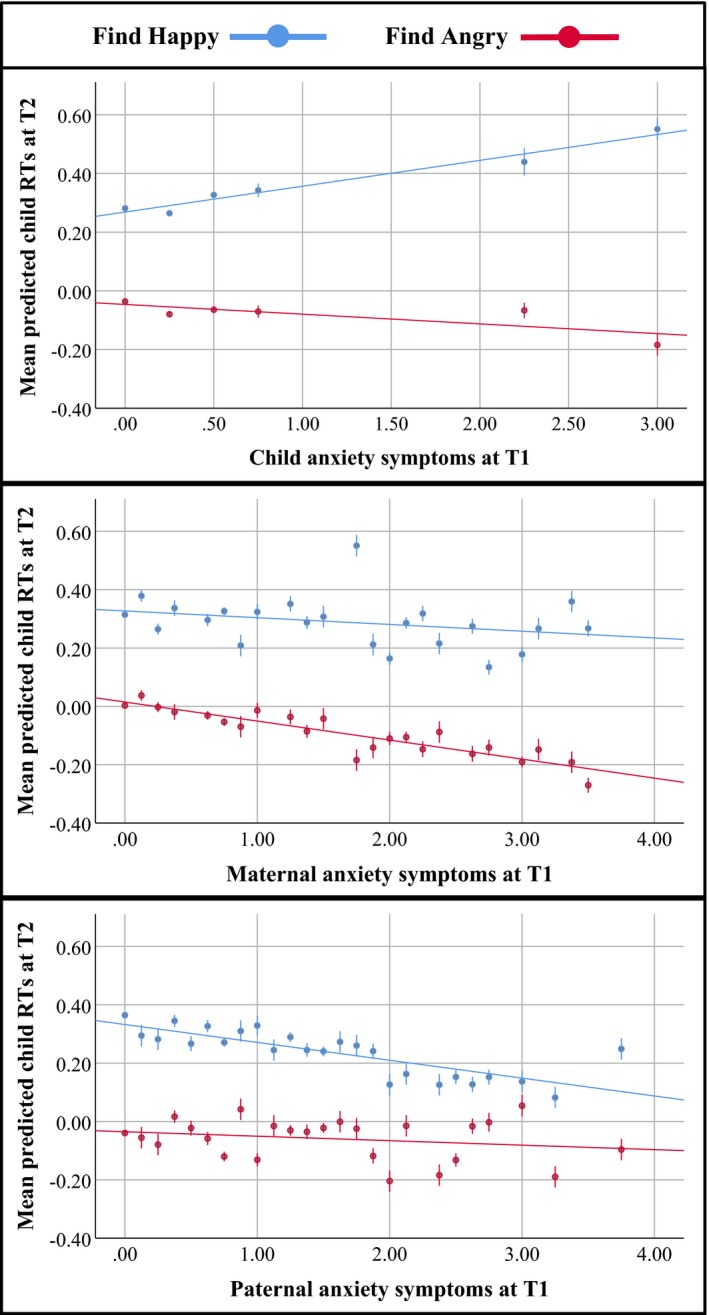
The associations between children's (top), mothers' (middle) and fathers' (bottom) average number of anxiety symptoms T1 and the mean predicted child reaction times at T2. The mean RT is standardized. Error bars represent 95% confidence intervals.
3.4.4. Parents’ and children's anxiety at T2 as predictors of child reaction times in the visual search task at T2
The same multi‐level model with anxiety scores at T2 revealed different effects: Neither the main effects of maternal, paternal, or child anxiety nor the interactions involving trial type and anxiety were significant in the initial model. F‐scores of the interactions were as follows: the three‐way interactions among the trial type, child gender, and anxiety of the child: F(1, 2619.83) = 0.12, p = 0.735, anxiety of the mother: F(1, 2619.94) = 0.44, p = 0.505, and anxiety of the father: F(1, 2619.82) = 0.40, p = 0.843; the two‐way interactions between trial type and anxiety of the child: F(1, 2619.83) = 0.23, p = 0.628, anxiety of the mother: F(1, 2619.94) = 0.01, p = 0.758, and anxiety of the father, F(1, 2619.82) = 2.26, p = 0.133; the two‐way interactions between child gender and anxiety of the child: F(1, 58.26) = 0.08, p = 0.772, anxiety of the mother: F(1, 58.32) = 0.16, p = 0.691, and anxiety of the father: F(1, 58.23) = 1.28, p = 0.262. Neither children's, p = 0.555, nor parental (p = 0.201 for mothers, and p = 0.759 for fathers) levels of anxiety at T2 were related to children's levels of attentional bias as measured with the visual search task at T2 in the final model with main effects.
3.5. Relation between attentional biases of parents and children
This section focuses on the direct associations between parents’ and children's attentional biases. To match parents’ and children's responses in the visual probe task, we first aggregated RTs across trials, separately for congruent and incongruent trials. We investigated the direct associations between parent and child attentional biases using multi‐level models consisting of repeated observations of RTs across different trial types (level 1), nested in children (level 2). Note that trial number was not included as a control variable in this model because the data were aggregated across trials.
In the visual search task, the order of the blocks was fixed. As such, parents’ and children's responses could be matched on the level of trials without averaging per trial type. We therefore matched the first half of parents’ RTs in both blocks with children's responses in these blocks. We investigated the direct association between parent and child attentional biases in an initial multi‐level model consisting of repeated observations of RT in trials, nested in trial type (level 1), nested in children (level 2). Trial number was added as a control variable in the analyses of the visual search task.
The initial models for both tasks contained the fixed main effects of trial type and child gender (girls vs. boys) in addition to maternal and paternal attentional biases and child anxiety. We used anxiety scores at T1 to account for child anxiety, as this was the only anxiety predictor explaining variance in child attentional bias (see above). We also tested all potential interactions of maternal and paternal RTs and child anxiety with trial type and child gender in these models.
3.5.1. Parents’ reaction times as predictors of child reaction times in the visual probe task at T2
None of the tested interactions reached significance in this model. The F‐scores were as follows: the three‐way interactions among trial type, child gender, and maternal RTs: F(1, 80.63) = 1.23, p = 0.271, among trial type, child gender, and paternal RTs: F(1, 83.89) = 0.30, p = 0.588, and among trial type, child gender, and child anxiety: F(1, 80.27) = 0.25, p = 0.618; the two‐way interactions between trial type and maternal RTs: F(1, 80.63) = 1.31, p = 0.256, between trial type and paternal RTs: F(1, 83.89) = 0.00, p = 0.962, between trial type and child anxiety: F(1, 80.27) = 0.33, p = 0.566, between child gender and maternal RTs: F(1, 159.31) = 0.09, p = 0.762, between child gender and paternal RTs: F(1, 149.65) = 0.28, p = 0.598, and between child gender and child anxiety: F(1, 79.86) = 0.00, p = 0.985. As such, the final model was reduced to a main effects model (N = 81). The main effects of mothers’ and fathers’ latencies were not significant in this final model (p = 0.234 and 0.828 for mothers and fathers respectively). As such, we found no evidence for a direct link between parents’ and children's attentional biases in the visual probe task at T2.
3.5.2. Parents’ reaction times as predictors of child reaction times in the visual search task at T2
Among tested interactions in this model, the three‐way interaction among child gender, trial type, and child anxiety was significant and retained in the final model, F(1, 3060.31) = 6.00, p = 0.014. None of the remaining interactions was significant in the first model. F‐scores were as follows in the initial model: the three‐way interactions among trial type, child gender, and maternal RTs: F(1, 3078.76) = 3.46, p = 0.063, among trial type, child gender, and paternal RTs: F(1, 3082.98) = 2.11, p = 0.147; the two‐way interactions between trial type and maternal RTs: F(1, 3078.77) = 0.06, p = 0.808, between trial type and paternal RTs: F(1, 3082.98) = 0.05, p = 0.829, between child gender and maternal RTs: F(1, 3127.25) = 0.916, p = 0.339, and between child gender and paternal RTs: F(1, 3131.83) = 0.14, p = 0.707.
The final model (N = 73) is presented in Tables 6 and S4. Maternal and paternal RTs did not significantly predict child RTs in the final model (p = 0.964 and 0.154 for mothers and fathers respectively). To further inspect the significant three‐way interaction among child gender, trial type, and child anxiety, β = 0.28, SE = 0.11, p = 0.013, CI = 0.06 to 0.51, we conducted separate analyses of girls’ and boys’ attentional biases. These analyses revealed that the link between anxiety and attentional bias was stronger in girls than in boys: The two‐way interaction between trial type and child anxiety was significant for girls, n = 39, F(1, 1636.72) = 5.53, p = 0.019, while it was marginal for boys, n = 34, F(1, 1423.54) = 3.47, p = 0.063. In sum, we found no significant relation between parents’ attentional biases and their children's attentional biases in the visual search task at T2.
Table 6.
Parents’ reaction times as predictors of child reaction times in the visual search task at T2(N = 73)
| Parameter | β | SE | df | t | p | 95% Confidence interval | |
|---|---|---|---|---|---|---|---|
| Lower bound | Upper bound | ||||||
| Intercept | −0.23 | 0.09 | 104.63 | −2.59 | 0.011 | −0.41 | −0.05 |
| Trial type (search happy vs. search angry) | 0.30 | 0.05 | 3,060.36 | 5.86 | <0.001 | 0.20 | 0.41 |
| Child gender (girls vs. boys) | −0.09 | 0.11 | 86.74 | −0.77 | 0.442 | −0.31 | 0.14 |
| Trial number | 0.01 | 0.00 | 3,059.72 | 3.92 | <0.001 | 0.00 | 0.01 |
| Child anxiety symptoms at T1 | −0.02 | 0.18 | 87.18 | −0.14 | 0.890 | −0.37 | 0.32 |
| Maternal RT | 0.00 | 0.02 | 3,125.02 | −0.05 | 0.964 | −0.04 | 0.03 |
| Paternal RT | 0.03 | 0.02 | 3,131.56 | 1.43 | 0.154 | −0.01 | 0.06 |
| Child gender * trial type | 0.06 | 0.07 | 3,060.44 | 0.86 | 0.387 | −0.07 | 0.19 |
| Trial type * child anxiety symptoms at T1 | −0.20 | 0.11 | 3,060.28 | −1.85 | 0.064 | −0.41 | 0.01 |
| Child gender * child anxiety symptoms at T1 | 0.01 | 0.19 | 87.07 | 0.05 | 0.962 | −0.36 | 0.38 |
| Child gender * trial type * child anxiety symptoms at T1 | 0.28 | 0.11 | 3,060.30 | 2.50 | 0.013 | 0.06 | 0.51 |
4. DISCUSSION
This study investigated the prospective and concurrent associations between anxiety and attentional bias, using both a visual probe task and a visual search task, in a sample of mothers, fathers, and 7.5‐year‐old children in a longitudinal design. With the visual probe task, we found no significant effects. With the more reliable visual search task, we found significant prospective associations between anxiety levels in both adults and children at T1 and attentional biases at T2, while concurrent relations between anxiety levels at T2 and attentional biases at T2 were not significant. Demonstrating the intergenerational transmission of anxiety problems, parental anxiety at T1 was predictive of children's attentional bias at T2, even while controlling for children's own levels of anxiety at T1. Finally, we found no significant relations between attentional biases of parents and the attentional bias of their children.
In contrast with earlier meta‐analytic evidence (Bar‐Haim et al., 2007; Dudeney et al., 2015), we found no evidence, either in children or in adults, for the idea that current attentional bias relates to current anxiety. However, our findings revealed that all participants (i.e. parents and their 7.5‐year‐old children) showed a stronger attentional bias to threat only in the visual search task if they were more anxious at 4.5 years; that is, 3 years prior to the attentional bias assessments.2 Our results could be in line with cognitive models of anxiety according in which there is a mutually reinforcing relation between attentional bias and anxiety (see Van Bockstaele et al., 2014). While our data only allowed us to test the hypothesis that anxiety prospectively predicts attentional bias, a mutually reinforcing relation would also entail that current attentional bias measures predict future anxiety problems (e.g. see Pérez‐Edgar et al., 2010, 2011; but see Waters et al., 2018). A future follow‐up assessment of child anxiety in our sample could add empirical weight to this hypothesized relation.
The lack of significant concurrent associations between anxiety and attentional biases in children is in line with a recent longitudinal study from White et al. (2017). They found no significant attentional bias to threat at either 5 or at 7 years using the visual probe task with angry versus neutral faces. In line with our current visual probe task findings, none of their overall concurrent or prospective associations between child attentional biases and child anxiety was significant. White et al. did, however, find a concurrent link between attentional bias to threat and anxiety in a subgroup of children with early temperamental dispositions for anxiety – Behavioural Inhibition (BI). BI is a biologically based temperamental disposition marked by hypervigilance, and high levels of fearful and withdrawn reactions in response to novel/ambiguous stimuli in early childhood years (Fox, Henderson, Marshall, Nichols, & Ghera, 2005). The data therefore suggest a moderating role for attentional bias in the link between early temperamental predispositions and later child anxiety. A similar moderating role of attentional bias was also reported in the relation between early BI and later social withdrawal in adolescents and 5‐year‐old children (Pérez‐Edgar et al., 2010, 2011). Moreover, Morales, Taber‐Thomas, and Pérez‐Edgar (2017) recently reported that stable patterns of attentional bias across tasks were only evident for children with high levels of BI. This may suggest that children at risk for anxiety due to their temperamental dispositions are more likely to show consistent patterns of vigilance and/or to detect ambiguous signals as threat than children without these dispositions. Including the potentially moderating role of BI in future research on the relation between child attentional biases and anxiety may therefore be paramount.
From a developmental perspective, the finding that attentional biases were observed only in children, but not in adults is in line with the idea that attention biases to threat may fade away with development. This finding indirectly supports the idea that development may exert an influence on the attention biases to threat, moderating an existing bias, as suggested by moderation models (Field & Lester,b). In contrast, the link between more anxiety and larger future attentional biases held both for parents and children, suggesting that this mechanism may be more stable and is less affected by developmental influences. Nevertheless, it should be noted that these developmental implications are mostly speculative, and a longitudinal study assessing both attentional bias and anxiety at multiple time points during development is needed to fully address whether attentional bias remains stable over time or whether it is affected by development. In addition, future anxiety measurements in our sample are needed to address whether attentional biases in childhood are predictive of later anxiety.
Children's attentional biases to threat in the visual search task were not only predicted by their own anxiety but also by both maternal and paternal anxiety symptoms at T1, after taking into account children's own anxiety. However, the pattern of results differed between mothers and fathers (see Bögels & Perotti, 2011; Bögels & Phares, 2008). In line with earlier findings with children of parents with PTSD (Moradi et al., 1999, but not with panic disorder, Schneider et al., 2008), more social and generalized anxiety in mothers was related to more attentional bias to threat in children, as evidenced by faster RTs to find angry targets in happy crowds. This suggests that mothers’ anxiety may sensitize children's vigilance and attention to threat, thereby contributing to the risk for child anxiety. In contrast, more anxiety in fathers was related to less attentional bias and more avoidance of threat in children, as evidenced by faster RTs to find happy faces in angry crowds. While this reduced attentional bias could indicate that fathers’ anxiety contributes to resilience for anxiety development in children, attentional avoidance of threat in children has also been related to increased risks of anxiety disorders (Brown et al., 2013) and to vulnerability to PTSD (Briggs‐Gowan et al., 2016; Wald et al., 2011). Again, future measurements of child anxiety in our sample are needed to convincingly answer the question whether vigilance for threat, attentional avoidance of threat, both vigilance and avoidance, or neither vigilance nor avoidance are directly predictive of future child anxiety.
In turn, raw correlations revealed that children's anxiety was only modestly related to mothers’ but not to fathers’ anxiety. The lack of a direct link between fathers’ and children's anxiety is at odds with the predictions of evolutionary models that attribute a more pronounced role to paternal as compared to maternal anxiety in the development of social anxiety disorder (Bögels & Perotti, 2011; Bögels & Phares, 2008). The significant yet modest relation between children's and mothers’ anxiety is in line with earlier evidence from family and twin studies showing a significant familial aggregation (Eley et al., 2015; Turner et al., 1987; Turner et al., 1991). However, given the methodological limitation stemming from using mothers’ reports for their own as well as their child's psychopathology, we refrain from drawing strong conclusions regarding this relation based on our current data.
Contrary to Montagner et al. (2016), none of our crucial findings was influenced by child gender. These diverging findings can be explained in several ways. First, Montagner et al. addressed concurrent relations using a visual probe task with angry‐neutral face pairs, while we compared angry‐happy face pairs. Second, we used a dimensional measure of parental anxiety, while Montagner et al. differentiated among no disorder, anxiety disorder, mood disorder, and comorbid mood and anxiety disorder. It is possible that a diagnosis of depression in one of the parents determines differential patterns of attentional bias in boys and girls.
Finally, in contrast with cognitive‐behavioural models of anxiety transmission (Creswell et al., 2010), we found no significant direct positive association between parental attentional bias to threat and the attentional bias of their children. This finding is in line with the findings of Mogg et al. (2012) who also found no direct link between attention biases in children and their mothers with (vs. without) panic disorder. The absence of a direct relationship between attentional bias to threat in parents’ and their offspring suggests that the relation between parental anxiety and child attentional bias is unlikely to be mediated by parental attentional biases. In other words, parental attentional biases are unlikely to contribute to the development of attentional bias in their children. Instead, other aspects of parenting behaviour (e.g. challenging parenting: Lazarus et al., 2016) and of environmental exposure to parental anxiety (e.g. through social learning: Aktar et al., 2017) may shape children's attentional biases more directly.
Our current findings should be interpreted considering a number of limitations. First, although the longitudinal design is helpful in establishing a developmental time line, our study did not manipulate attentional bias or anxiety in parents or children, precluding direct causal inferences about the associations between anxiety and attentional bias. Moreover, attentional bias measures from parents and children were only available at one time‐point, at 7.5 years. Second, despite a possibly bi‐directional link between parent and child attentional biases and anxiety, we focused on parent‐to‐child effects. As such, we only considered parental anxiety and attentional bias as predictors of child attentional biases, rather than vice versa. Third, child anxiety scores in this study were obtained using parents’ reports. Parents’ own anxiety can bias their perception of their child's anxiety (Najman et al., 2000). Raw associations in the current sample showed moderate associations between children's anxiety at T2 and mothers’ (but not fathers’) anxiety scores at T1 and T2. Future research may counter this issue by including measures of child anxiety that do not rely on parent reports, such as observational data. Moreover, the prevalence of the SAD and GAD in the current sample of parents was higher than in the general population, whereas the inter‐individual variation in anxiety symptoms was limited in children, and consisted only of mild levels of anxiety. This does limit the generalizability of our findings, and calls for future studies including more anxious children, for instance, through preselection or screening. Such an approach was not feasible in our current study, as the sample was selected before the children were born.
Fourth, our study did not include the potential interplay of attention biases with other anxiety vulnerabilities such as BI (Pérez‐Edgar et al., 2010, 2011), nor did we differentiate between social and generalized anxiety disorder symptoms. Our choice to combine these disorders was mainly driven by statistical as well as practical considerations: Because our sample was not preselected, combining symptoms of the two disorders increased the variance in anxiety scores, and using emotional facial expressions in the attentional bias tasks is common in both social and generalized anxiety. However, we cannot exclude the possibility that the results are driven by either social or generalized anxiety alone. Future studies, comparing preselected samples suffering from social versus generalized anxiety disorders, could shed more light on this issue.
Finally, our significant findings were based only on the visual search data, and we found no significant effects in the visual probe data. The lack of significant effects in the visual probe data may be due to our choice to use angry–happy face pairs instead of angry‐neutral face pairs. A more fundamental explanation for the lack of significant findings in the visual probe task relates to its poor reliability. This poor reliability is a well‐documented finding in both adults and children (e.g. Brown et al., 2014; Schmukle, 2005). Recently, several different ways to improve the reliability of the visual probe task, including the development of so‐called attentional bias variability indices (e.g. Iacoviello et al., 2014), have been proposed (for elaborate discussions on this topic, see Price et al., 2015; Rodebaugh et al., 2016). Future research will need to elucidate whether or not these new developments will result in a consistent improvement of the reliability of the visual probe task, and if so, whether or not previous findings (including our own null findings) are replicated using these new indices.
Despite these limitations, this study increases our understanding of the intergenerational transmission of attentional bias and anxiety in several ways. To our knowledge, our study is the first longitudinal investigation of both prospective and concurrent associations between anxiety in mothers, fathers, and children and attentional biases to threat. Our findings raise important questions about the direction of causality between attentional biases and anxiety in the intergenerational transmission of anxiety. They are consistent with the idea that earlier anxiety problems in both parents and children influence the development of attentional bias at a later age, and thus counter theories suggesting that attentional bias is involved in the aetiology of anxiety disorders in a strict linear cause–effect model (e.g. Bar‐Haim et al., 2007). Our data can be reconciled with the idea that attentional bias and anxiety are mutually reinforcing (Van Bockstaele et al., 2014), with anxiety levels at T1 influencing attentional biases at T2, and attentional biases at T2 further affecting anxiety at T3 and so on. As argued earlier, this time course would be supported if our current attentional bias scores prove predictive of follow‐up measurements of anxiety at later ages. Further longitudinal investigations of the temporal relation between anxiety and attention are thus essential for a better understanding of the role of attention in anxiety.
Most importantly, we found that parental anxiety levels predict attentional bias as measured with the visual search task in their children, even after correcting for children's own anxiety levels. Furthermore, moving beyond earlier studies that almost exclusively focused on mothers’ anxiety and attentional bias to test this relation, this was the first study that examined the role fathers’ anxiety and attention may play in the development of child anxiety. We found separate and inverse relations of mothers relative to fathers’ anxiety and child attentional biases: Mothers’ anxiety predicted enhanced vigilance for threat, while fathers’ anxiety predicted enhanced attentional avoidance of threat. Our findings illustrate the importance of including both parents in future studies, as they may play different roles in increasing or reducing the risk of their children developing anxiety disorders.
5. CONCLUSIONS
In this study, we found that anxiety levels in both parents and children were prospectively (but not concurrently) related to their respective attentional biases to threat as measured in the visual search task. In addition, parental anxiety was prospectively predictive of visual search attentional bias of their children, after controlling for child anxiety. This finding suggests that children of anxious parents may come to develop an attentional bias to threat, which may be a risk factor for future anxiety (disorders). Finally, parental attentional bias was unrelated to attentional bias of their children, suggesting that it is parents’ anxiety rather than parents’ attentional bias that is involved in the intergenerational transmission of risk for child anxiety.
Supporting information
Aktar E, Van Bockstaele B, Pérez‐Edgar K, Wiers RW, Bögels SM. Intergenerational transmission of attentional bias and anxiety. Dev Sci. 2019;22:e12772 10.1111/desc.12772
Funding information
Bram Van Bockstaele is a postdoctoral researcher of the Research Priority Area Yield of the University of Amsterdam. This study was financed by the Dutch National Science Foundation (grant number VICI 453‐09‐001, awarded to Susan Bögels, and grant number Rubicon 446‐16‐021 awarded to Evin Aktar).
ENDNOTES
Parents additionally reported child psychopathology in a clinical interview at T2 in this longitudinal study (SCID‐Junior: Braet, Wante, Bögels, & Roelofs, 2015, see Post‐hoc Analyses). We used SCARED scores as the main anxiety predictor at T2 (child SAD and GAD symptoms obtained from SCID‐Junior at T2 were considered in post hoc analyses).
Split‐half correlations can be interpreted as effect sizes, with values from 0.10, 0.30, and 0.50 reflecting small, medium, and large effects respectively (Cohen, 1992).
It is possible that the current findings showing significant prospective but not concurrent associations between anxiety and attention biases are accounted for by the methodological differences in the way we measured anxiety at T1 versus T2 (i.e. clinical interviews at T1, and questionnaires at T2). To further address this possibility, we explored the link between child attention biases and child anxiety using parents’ reports of child psychopathology in a clinical interview at T2 (SCID). These post hoc analyses were limited to children, as parental anxiety scores were only measured with questionnaires at T2. There was no significant concurrent association between parents’ report of child anxiety symptoms from SCID and child attentional bias (see section post hoc analyses in the supplement for more detail). Thus, the lack of significant concurrent associations between child anxiety and attention biases cannot be explained by this difference in the measurement of anxiety in this study.
The differential concurrent and prospective links between anxiety and attentional biases observed in this study were not accounted for by the methodological differences in the measurement of anxiety at T1 versus T2.
REFERENCES
- Abend, R. , de Voogd, L. , Salemink, E. , Wiers, R.W. , Pérez‐Edgar, K. , Fitzgerald, A. ··· Bar‐Haim, Y. (2018). Association between attention bias to threat and anxiety symptoms in children and adolescents. Depression and Anxiety, 35, 229–238. 10.1002/da.22706 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Aktar, E. , Majdandžić, M. , de Vente, W. , & Bögels, S.M. (2013). The interplay between expressed parental anxiety and infant behavioural inhibition predicts infant avoidance in a social referencing paradigm. Journal of Child Psychology and Psychiatry, 54, 144–156. 10.1111/j.1469-7610.2012.02601.x [DOI] [PubMed] [Google Scholar]
- Aktar, E. , Majdandžić, M. , De Vente, W. , & Bögels, S.M . (2017). Parental expressions of anxiety and child temperament in toddlerhood jointly predict preschoolers’ avoidance of novelty. Journal of Clinical Child and Adolescent Psychology. 10.1080/15374416.2017.1371029 [DOI] [PubMed] [Google Scholar]
- Bar‐Haim, Y. , Lamy, D. , Pergamin, L. , Bakermans‐Kranenburg, M.J. , & van IJzendoorn, M.H. (2007). Threat‐related attentional bias in anxious and nonanxious individuals: A meta‐analytic study. Psychological Bulletin, 133, 1–24. 10.1037/0033-2909.133.1.1 [DOI] [PubMed] [Google Scholar]
- Beesdo, K. , Knappe, S. , & Pine, D.S. (2009). Anxiety and anxiety disorders in children and adolescents: Developmental issues and implications for DSM‐V. Psychiatric Clinics of North America, 32, 483–524. 10.1016/j.psc.2009.06.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beidel, D.C. , & Turner, S.M. (1997). At risk for anxiety: I. Psychopathology in the offspring of anxious parents. Journal of the American Academy of Child & Adolescent Psychiatry, 36, 918–924. 10.1097/00004583-199707000-00013 [DOI] [PubMed] [Google Scholar]
- Bijl, R.V. , Ravelli, A. , & Van Zessen, G. (1998). Prevalence of psychiatric disorder in the general population: Results of the Netherlands Mental Health Survey and Incidence Study (NEMESIS). Social Psychiatry and Psychiatric Epidemiology, 33, 587–595. 10.1007/s001270050098 [DOI] [PubMed] [Google Scholar]
- Birmaher, B. , Brent, D.A. , Chiappetta, L. , Bridge, J. , Monga, S. , & Baugher, M. (1999). Psychometric properties of the Screen for Child Anxiety Related Emotional Disorders (SCARED): A replication study. Journal of the American Academy of Child and Adolescent Psychiatry, 38(10), 1230–1236. [DOI] [PubMed] [Google Scholar]
- Bögels, S.M. , & Perotti, E.C. (2011). Does father know best? A formal model of the paternal influence on childhood social anxiety. Journal of Child and Family Studies, 20, 171–181. 10.1007/s10826-010-9441-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bögels, S. , & Phares, V. (2008). Fathers’ role in the etiology, prevention and treatment of child anxiety: A review and new model. Clinical Psychology Review, 28, 539–558. 10.1016/j.cpr.2007.07.011 [DOI] [PubMed] [Google Scholar]
- Bögels, S.M. , & Van Melick, M. (2004). The relationship between child‐ report, parent self‐report, and partner report of perceived parental rearing behaviors and anxiety in children and parents. Personality and Individual Differences, 37, 1583–1596. 10.1016/j.paid.2004.02.014 [DOI] [Google Scholar]
- Bradley, B.P. , Mogg, K. , White, J. , Groom, C. , & De Bono, J. (1999). Attentional bias for emotional faces in generalized anxiety disorder. British Journal of Clinical Psychology, 38, 267–278. 10.1348/014466599162845 [DOI] [PubMed] [Google Scholar]
- Braet, C. , Wante, L. , Bögels, S.M. , & Roelofs, J . (2015). SCID‐Junior. Unpublished manuscript.
- Briggs‐Gowan, M.J. , Grasso, D. , Bar‐Haim, Y. , Voss, J. , McCarthy, K.J. , Pine, D.S. , & Wakschlag, L.S. (2016). Attention bias in the developmental unfolding of post‐traumatic stress symptoms in young children at risk. Journal of Child Psychology and Psychiatry, 57, 1083–1091. 10.1111/jcpp.12577 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brown, T.A. , & Barlow, D.H . (2005). Dimensional versus categorical classification of mental disorders in the fifth edition of the Diagnostic and statistical manual of mental disorders and beyond: Comment on the special section. Journal of Abnormal Psychology, 114, 551–556. 10.1037/0021-843x.114.4.551 [DOI] [PubMed] [Google Scholar]
- Brown, H.M. , Eley, T.C. , Broeren, S. , Macleod, C. , Rinck, M. , Hadwin, J.A. , & Lester, K.J. (2014). Psychometric properties of reaction time based experimental paradigms measuring anxiety‐related information‐processing biases in children. Journal of Anxiety Disorders, 28, 97–107. 10.1016/j.janxdis.2013.11.004 [DOI] [PubMed] [Google Scholar]
- Brown, H.M. , McAdams, T.A. , Lester, K.J. , Goodman, R. , Clark, D.M. , & Eley, T.C. (2013). Attentional threat avoidance and familial risk are independently associated with childhood anxiety disorders. Journal of Child Psychology and Psychiatry, 54, 678–685. 10.1111/jcpp.12024 [DOI] [PubMed] [Google Scholar]
- Cohen, J. (1992). A power primer. Psychological Bulletin, 112, 155–159. 10.1037/0033-2909.112.1.155 [DOI] [PubMed] [Google Scholar]
- Creswell, C. , Cooper, P. , & Murray, L . (2010). Intergenerational transmission of anxious information processing biases In Hadwin J.A. & Field A.P. (Eds.), Information processing biases and anxiety: A developmental perspective (pp. 280–295). Chichester: John Wiley and Sons; 10.1002/9780470661468.ch12 [DOI] [Google Scholar]
- De Lijster, J.M. , Dierckx, B. , Utens, E.M. , Verhulst, F.C. , Zieldorff, C. , Dieleman, G.C. , & Legerstee, J.S. (2017). The age of onset of anxiety disorders: A meta‐analysis. The Canadian Journal of Psychiatry, 62, 237–246. 10.1177/0706743716640757 [DOI] [PMC free article] [PubMed] [Google Scholar]
- De Schryver, M. , Hughes, S. , Rosseel, Y. , & De Houwer, J. (2016). Unreliable yet still replicable: A comment on LeBel and Paunonen. Frontiers in Psychology, 6, 2039 10.3389/fpsyg.2015.02039 [DOI] [PMC free article] [PubMed] [Google Scholar]
- De Vente, W. , Majdandžić, M. , Colonnesi, C. , & Bögels, S.M. (2011). Intergenerational transmission of social anxiety: The role of paternal and maternal fear of negative child evaluation and parenting behaviour. Journal of Experimental Psychopathology, 2, 509–530. 10.5127/jep.018811 [DOI] [Google Scholar]
- Di Nardo, P.A. , Brown, T.A. , & Barlow, D.H. (1994). Anxiety Disorders Interview Schedule for DSM‐IV: Lifetime version (ADIS‐1V‐L). San Antonio, TX: Psychological Corporation. [Google Scholar]
- Dudeney, J. , Sharpe, L. , & Hunt, C. (2015). Attentional bias towards threatening stimuli in children with anxiety: A meta‐analysis. Clinical Psychology Review, 40, 66–75. 10.1016/j.cpr.2015.05.007 [DOI] [PubMed] [Google Scholar]
- Eley, T.C. , McAdams, T.A. , Rijsdijk, F.V. , Lichtenstein, P. , Narusyte, J. , Reiss, D. ··· Neiderhiser, J.M. (2015). The intergenerational transmission of anxiety: A children‐of‐twins study. American Journal of Psychiatry, 172, 630–637. 10.1176/appi.ajp.2015.14070818 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eysenck, M.W. (1992). Anxiety: The cognitive perspective. Hove: Lawrence Erlbaum. [Google Scholar]
- Field, A.P. (2009). Discovering statistics using SPSS (3rd edn). London: Sage publications. [Google Scholar]
- Field, A.P. , & Lester, K.L . (2010a). Learning of information processing biases in anxious children and adolescents In Hadwin J.A. & Field A.P. (Eds.), Information processing biases and anxiety: A developmental perspective (pp. 253–278). Chichester: John Wiley& Sons; 10.1002/9780470661468.ch11 [DOI] [Google Scholar]
- Field, A.P. , & Lester, K.J. (2010b). Is there room for ‘development’ in developmental models of information processing biases to threat in children and adolescents? Clinical Child and Family Psychology Review, 13, 315–332. [DOI] [PubMed] [Google Scholar]
- Fox, N.A. , Henderson, H.A. , Marshall, P.J. , Nichols, K.E. , & Ghera, M.M. (2005). Behavioural inhibition: Linking biology and behaviour within a developmental framework. Annual Review of Psychology, 56, 235–262. 10.1146/annurev.psych.55.090902.141532 [DOI] [PubMed] [Google Scholar]
- Gar, N.S. , Hudson, J.L. , & Rapee, R.M. (2005). Family factors and the development of anxiety disorders In Hudson J.L. & Rapee R.M. (Eds.), Psychopathology and the family (pp. 125–145). Oxford: Elsevier. [Google Scholar]
- Hadwin, J.A. , Garner, M. , & Perez‐Olivas, G. (2006). The development of information processing biases in childhood anxiety: A review and exploration of its origins in parenting. Clinical Psychology Review, 26, 876–894. 10.1016/j.cpr.2005.09.004 [DOI] [PubMed] [Google Scholar]
- Hoehn‐Saric, R. , Hazlett, R.L. , & McLeod, D.R. (1993). Generalized anxiety disorder with early and late onset of anxiety symptoms. Comprehensive Psychiatry, 34, 291–298. 10.1016/0010-440X(93)90013-T [DOI] [PubMed] [Google Scholar]
- Hudziak, J.J. , Achenbach, T.M. , Althoff, R.R. , & Pine, D.S. (2007). A dimensional approach to developmental psychopathology. International Journal of Methods in Psychiatric Research, 16, S16–S23. 10.1002/mpr.217 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Iacoviello, B.M. , Wu, G. , Abend, R. , Murrough, J.W. , Feder, A. , Fruchter, E. … Charney, D.S. (2014). Attention bias variability and symptoms of posttraumatic stress disorder. Journal of Traumatic Stress, 27, 232–239. 10.1002/jts.21899 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Inquisit 4 [Computer software]. (2014). Available from http://www.millisecond.com
- Lazarus, R.S. , Dodd, H.F. , Majdandžić, M. , De Vente, W. , Morris, T. , Byrow, Y. ··· Hudson, J.L. (2016). The relationship between challenging parenting behaviour and childhood anxiety disorders. Journal of Affective Disorders, 190, 784–791. 10.1016/j.jad.2015.11.032 [DOI] [PubMed] [Google Scholar]
- Lundqvist, D. , Flykt, A. , & Öhman, A. (1998). The Karolinska Directed Emotional Faces – KDEF, Psychology CD ROM from Department of Clinical Neuroscience section. Karolinska Institutet. [Google Scholar]
- Luo, S. (2017). Assortative mating and couple similarity: Patterns, mechanisms, and consequences. Social and Personality Psychology Compass, 11(8), e12337 10.1111/spc3.12337 [DOI] [Google Scholar]
- Maas, C.J. , & Hox, J.J. (2005). Sufficient sample sizes for multilevel modeling. Methodology, 1, 86–92. 10.1027/1614-1881.1.3.86 [DOI] [Google Scholar]
- MacLeod, C. , Mathews, A. , & Tata, P. (1986). Attentional bias in emotional disorders. Journal of Abnormal Psychology, 95, 15–20. 10.1037/0021-843X.95.1.15 [DOI] [PubMed] [Google Scholar]
- Mogg, K. , Philippot, P. , & Bradley, B.P. (2004). Selective attention to angry faces in clinical social phobia. Journal of Abnormal Psychology, 113, 160–165. 10.1037/0021-843X.113.1.160 [DOI] [PubMed] [Google Scholar]
- Mogg, K. , Wilson, K.A. , Hayward, C. , Cunning, D. , & Bradley, B.P. (2012). Attentional biases for threat in at‐risk daughters and mothers with lifetime panic disorder. Journal of Abnormal Psychology, 121, 852–862. 10.1037/a0028052 [DOI] [PubMed] [Google Scholar]
- Montagner, R. , Mogg, K. , Bradley, B.P. , Pine, D.S. , Czykiel, M.S. , Miguel, E.C. ··· Salum, G.A. (2016). Attentional bias to threat in children at‐risk for emotional disorders: Role of gender and type of maternal emotional disorder. European Journal of Child and Adolescent Psychiatry, 25, 735–742. 10.1007/s00787-015-0792-3 [DOI] [PubMed] [Google Scholar]
- Moradi, A. R. , Neshat-Doost, H. T. , Taghavi, R. , Yule, W. , & Dalgleish, T. (1999). Performance of children of adults with PTSD on the Stroop colour-naming task. Journal of Traumatic Stress, 12, 663–672. 10.1023/A:1024721218869 [DOI] [PubMed] [Google Scholar]
- Morales, S. , Taber‐Thomas, B.C. , & Pérez‐Edgar, K.E . (2017). Patterns of attention to threat across tasks in behaviorally inhibited children at risk for anxiety. Developmental Science, 20 10.1111/desc.12391 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Najman, J.M. , Williams, G.M. , Nikles, J. , Spence, S. , Bor, W. , O'Callaghan, M. … Andersen, M.J. (2000). Mothers’ mental illness and child behavior problems: Cause‐effect association or observation bias? Journal of the American Academy of Child & Adolescent Psychiatry, 39, 592–602. 10.1097/00004583-200005000-00013 [DOI] [PubMed] [Google Scholar]
- Nikolić, M. , Aktar, E. , Bögels, S.M. , Colonnesi, C. , & de Vente, W. (2018). Bumping heart and sweaty palms: Physiological hyperarousal as a risk factor for child social anxiety. Journal of Child Psychology and Psychiatry, 59, 119–128. 10.1111/jcpp.12813 [DOI] [PubMed] [Google Scholar]
- Ollendick, T.H. , Grills, A.E. , & King, N.J. (2001). Applying developmental theory to the assessment and treatment of childhood disorders: Does it make a difference? Clinical Psychology & Psychotherapy, 8, 304–314. [Google Scholar]
- Ollendick, T.H. , & Vasey, M.W. (1999). Developmental theory and the practice of clinical child psychology. Journal of Clinical Child Psychology, 28, 457–466. [DOI] [PubMed] [Google Scholar]
- Pérez‐Edgar, K. , Bar‐Haim, Y. , McDermott, J.M. , Chronis‐Tuscano, A. , Pine, D.S. , & Fox, N.A. (2010). Attention biases to threat and behavioral inhibition in early childhood shape adolescent social withdrawal. Emotion, 10, 349–357. 10.1037/a0018486 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pérez‐Edgar, K. , Reeb‐Sutherland, B.C. , McDermott, J.M. , White, L.K. , Henderson, H.A. , Degnan, A.A. … Fox, N.A. (2011). Attention biases to threat link behavioral inhibition to social withdrawal over time in very young children. Journal of Abnormal Child Psychology, 39, 885–895. 10.1007/s10802-011-9495-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Perugini, M. , Richetin, J. , & Zogmaister, C. (2010). Prediction of behavior In Gawronski B. & Payne B.K. (Eds.), Handbook of Implicit Social Cognition: Measurement, theory, and applications (pp. 255–277). New York, NY: Guilford press. [Google Scholar]
- Polanczyk, G.V. , Salum, G.A. , Sugaya, L.S. , Caye, A. , & Rohde, L.A. (2015). Annual research review: A meta‐analysis of the worldwide prevalence of mental disorders in children and adolescents. Journal of Child Psychology and Psychiatry, 56, 345–365. 10.1111/jcpp.12381 [DOI] [PubMed] [Google Scholar]
- Price, R.B. , Kuckertz, J.M. , Siegle, G.J. , Ladouceur, C.D. , Silk, J.S. , Ryan, N.D. … Amir, N. (2015). Empirical recommendations for improving the stability of the dot‐probe task in clinical research. Psychological Assessment, 27, 365–376. 10.1037/pas0000036 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rapee, R.M. (2002). The development and modification of temperamental risk for anxiety disorders: Prevention of a lifetime of anxiety? Biological Psychiatry, 52, 947–957. 10.1016/S0006-3223(02)01572-X [DOI] [PubMed] [Google Scholar]
- Remes, O. , Brayne, C. , van der Linde, R. , & Lafortune, L. (2016). A systematic review of reviews on the prevalence of anxiety disorders in adult populations. Brain and Behavior, 6, e00497 10.1002/brb3.497 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rodebaugh, T.L. , Scullin, R.B. , Langer, J.K. , Dixon, D.J. , Huppert, J.D. , Bernstein, A. … Lenze, E.J. (2016). Unreliability as a threat to understanding psychopathology: The cautionary tale of attentional bias. Journal of Abnormal Psychology, 125, 840–851. 10.1037/abn0000184 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roy, A.K. , Dennis, T.A. , & Warner, C.M. (2015). A critical review of attentional threat bias and its role in the treatment of pediatric anxiety disorders. Journal of Cognitive Psychotherapy, 29, 171–184. 10.1891/0889-8391.29.3.171 [DOI] [PubMed] [Google Scholar]
- Schmukle, S. (2005). Unreliability of the dot probe task. European Journal of Personality, 19, 595–605. 10.1002/per.554 [DOI] [Google Scholar]
- Schneider, S. , Unnewehr, S. , In‐Albon, T. , & Margraf, J. (2008). Attention bias in children of patients with panic disorder. Psychopathology, 41, 179–186. 10.1159/000120986 [DOI] [PubMed] [Google Scholar]
- Silverman, W.K. , & Albano, A.M. (1996). The Anxiety Disorders Interview Schedule for Children for DSM‐IV: (Child and Parent Versions). San Antonio, TX: Psychological Corporation. [Google Scholar]
- Staugaard, S.R. (2009). Reliability of two versions of the dot‐probe task using photographic faces. Psychology Science Quarterly, 51, 339–350. [Google Scholar]
- Turner, S.M. , Beidel, D.C. , & Costello, A. (1987). Psychopathology in the offspring of anxiety disorder patients. Journal of Consulting and Clinical Psychology, 55, 229–235. 10.1037//0022-006X.55.2.229 [DOI] [PubMed] [Google Scholar]
- Turner, S.M. , Beidel, D.C. , & Epstein, L.H. (1991). Vulnerability and risk for anxiety disorders. Journal of Anxiety Disorders, 5, 151–166. 10.1016/0887-6185(91)90026-P [DOI] [Google Scholar]
- Van Bockstaele, B. , Lamens, L. , Salemink, E. , Wiers, R.W. , Bögels, S.M. , & Nikolaou, K . (manuscript submitted for publication). Reliability and validity of measures of attentional bias towards threat in unselected student samples: Seek, but will you find? [DOI] [PubMed]
- Van Bockstaele, B. , Salemink, E. , Bögels, S.M. , & Wiers, R.W. (2017). Limited generalization of changes in attentional bias following attentional bias modification with the visual probe task. Cognition and Emotion, 31, 369–376. 10.1080/02699931.2015.1092418 [DOI] [PubMed] [Google Scholar]
- Van Bockstaele, B. , Verschuere, B. , Tibboel, H. , De Houwer, J. , Crombez, G. , & Koster, E.H.W. (2014). A review of current evidence for the causal impact of attentional bias on fear and anxiety. Psychological Bulletin, 140, 682–721. 10.1037/a0034834 [DOI] [PubMed] [Google Scholar]
- Wald, I. , Shechner, T. , Bitton, S. , Holoshitz, Y. , Charney, D.S. , Muller, D. … Bar‐Haim, Y. (2011). Attention bias away from threat during life threatening danger predicts PTSD symptoms at one‐year follow‐up. Depression and Anxiety, 28, 406–411. 10.1002/da.20808 [DOI] [PubMed] [Google Scholar]
- Waters, A.M. , Forrest, K. , Peters, R.M. , Bradley, B.P. , & Mogg, K. (2015). Attention bias to emotional information in children as a function of maternal emotional disorders and maternal attention biases. Journal of Behavior Therapy and Experimental Psychiatry, 46, 158–163. [DOI] [PubMed] [Google Scholar]
- Waters, A.M. , Candy, E.M. , & Candy, S.G. (2017). Attention bias to threat in mothers with emotional disorders predicts increased offspring anxiety symptoms: A joint cross‐sectional and longitudinal analysis. Cognition and Emotion, 32, 892–903. 10.1080/02699931.2017.1349650 [DOI] [PubMed] [Google Scholar]
- Waters, A.M. , Forrest, K. , Peters, R. , Bradley, B.P. , & Mogg, K. (2015). Attention bias to emotional information in children as a function of maternal emotional disorders and maternal attention biases. Journal of Behavior Therapy and Experimental Psychiatry, 46, 158–163. 10.1016/j.jbtep.2014.10.002 [DOI] [PubMed] [Google Scholar]
- White, L.K. , Degnan, K.A. , Henderson, H.A. , Pérez‐Edgar, K. , Walker, O.L. , Shechner, T. ··· Fox, N.A. (2017). Developmental relations among behavioral inhibition, anxiety, and attention biases to threat and positive information. Child Development, 88, 141–155. 10.1111/cdev.12696 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williams, J.M.G. , Mathews, A. , & MacLeod, C. (1996). The emotional Stroop task and psychopathology. Psychological Bulletin, 120, 3–24. 10.1037/0033-2909.120.1.3 [DOI] [PubMed] [Google Scholar]
- Williams, J.M.G. , Watts, F.N. , MacLeod, C. , & Mathews, A. (1997). Cognitive psychology and the emotional disorders (2nd edn.). New York, NY: Wiley. [Google Scholar]
- Wittchen, H.U. , & Fehm, L. (2003). Epidemiology and natural course of social fears and social phobia. Acta Psychiatrica Scandinavica, 108(s417), 4–18. 10.1034/j.1600-0447.108.s417.1.x [DOI] [PubMed] [Google Scholar]
- Wittchen, H.U. , & Hoyer, J. (2001). Generalized anxiety disorder: Nature and course. Journal of Clinical Psychiatry, 62, 15–21. [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials