An official website of the United States government
Here's how you know
Official websites use .gov
A
.gov website belongs to an official
government organization in the United States.
Secure .gov websites use HTTPS
A lock (
) or https:// means you've safely
connected to the .gov website. Share sensitive
information only on official, secure websites.
As a library, NLM provides access to scientific literature. Inclusion in an NLM database does not imply endorsement of, or agreement with,
the contents by NLM or the National Institutes of Health.
Learn more:
PMC Disclaimer
|
PMC Copyright Notice
1Respiratory Medicine, Nuffield Department of Medicine, University of Oxford, Oxford, United Kingdom
2Lymington New Forest Hospital, Lymington, Hampshire, United Kingdom
✉
Corresponding Author: Richard E.K. Russell, Respiratory Medicine, Nuffield Department of Medicine, University of Oxford, United Kingdom; Lymington New Forest Hospital, Lymington, Hampshire, United Kingdom, E-mail: richard.russell@ndm.ox.ac.uk
✉
Corresponding author.
Received 2018 Dec 20; Accepted 2019 Mar 4; Issue date 2019 Jul.
The use of inhaled corticosteroids (ICS) has been accepted as standard practice following early landmark studies. These demonstrated a reduction in the risk of acute exacerbations of COPD (AECOPD). However, these studies were performed at a time when other therapies were not available and now our standards of care have changed. Other data has emerged which have also raised concerns as to an increase in the incidence of pneumonia in COPD patients taking inhaled corticosteroids. It is thus timely to evaluate the evidence. We present the two sides of this debate and consider the evidence both for the use of ICS as the best therapy to reduce the risk of AECOPD and also the evidence for the use of bronchodilators as a more effective and safer alternative. It is clear that as we approach an age of personalised medicine taking a “one size fits all” approach is both intellectually and medically wrong. We present the evidence that will help clinicians make better decisions for each of their patients.
Recently there has been a reappraisal of the use of inhaled corticosteroids (ICS) in patients with COPD mainly driven by two factors: the recognition that treatment is associated with important adverse events, best documented in clinical trials as an approximately doubling of the risk of pneumonia [1]; and the demonstration in a large and influential clinical trial that combined long acting beta2 agonist (LABA) and long acting antimuscarinic (LAMA) treatment has a larger positive impact on exacerbations, symptoms and lung function and is less likely to be associated with pneumonia than treatment with LABA/ICS [2]. As a result GOLD 2017 recommends LABA/LAMA as a primary exacerbation reduction strategy and a more restricted role for ICS [3]. I argue that this recommendation was premature and inappropriate and that a more reasonable approach would be to recommend treatment in a biomarker defined subgroup.
It has been known for some time that eosinophils are increased in the airways in a significant proportion of patients with COPD and that the short and longer-term beneficial effects of corticosteroid treatment are greater in patients with this feature [4–6]. An important advance has been the identification of the peripheral blood eosinophil count as a reliable and clinically accessible biomarker of eosinophilic airway inflammation [7]. A blood eosinophil count of <2% has been shown to have a high negative predictive value, meaning that the 40–50% of patients with COPD with a blood eosinophil count below this threshold can be reasonable assumed to not have a risk of exacerbation related to eosinophilic airway inflammation [7–9]. Demographic variables such as bronchodilator reversibility, atopy or asthma-COPD overlap are not related to the blood eosinophil count [8,10]. The reproducibility of blood eosinophils numbers appears to be good and ICS have little suppressive effect [11], meaning that low blood eosinophil counts retain their predictive value in an ICS treated patient.
Three large retrospective analyses of studies of patients with COPD and a past history of exacerbations have shown that exacerbation numbers increase with increasing blood eosinophil counts in patients not treated with ICS [11–13]. These studies have also shown that the beneficial effect of inhaled corticosteroids on exacerbation frequency increase progressively with increasing blood eosinophil counts. There is no evidence of efficacy against this outcome at counts below 100 cells/mm3 or a differential count of <2%. The effects of inhaled corticosteroids on FEV1 and QOL are also associated with blood eosinophil count although the findings are more variable [11–13]. Other important outcomes may also be related to the blood eosinophil count as a reanalysis of the ISOLDE study showed that the rate of decline in FEV1 was more rapid in patients with a blood eosinophil count >2% and that ICS effectively prevented this excess decline [14].
Two prospective studies of the utility of this method in stratifying the response to additional ICS therapy in COPD has been published recently. This showed clear benefit of fixed triple therapy vs tiotropium [15] alone or combined LABA/LAMA [16] in patients with a blood eosinophil count >2% but not <2%. This evidence seems sufficient to make definitive recommendations about the need to routinely measure blood eosinophil count when adding an ICS to other therapy in forthcoming guidelines.
I argue that the only criteria for use of ICS in COPD is possession of the biological process that corticosteroids modify: eosinophilic airway inflammation. Blanket, one size fits all management approaches should be replaced by a new precision medicine, biomarker directed approach. In the blood eosinophil count we have a predicative biomarker offering for the first time the prospect of a new precision medicine, biomarker directed approach to management (Figure 1).
Proposed management of COPD incorporating two major treatable traits: symptoms due to airflow limitation and risk assessed using the blood eosinophil count. Risk refers to future risk of exacerbation and decline in FEV1. Treatments with a trait specific effect are included. Rescue short acting bronchodilators (SABA or SAMA) could be used in all situations and patient categories, as required
Footnotes
Peer-review: Externally peer-reviewed.
Conflict of Interest: The author have no conflicts of interest to declare.
Financial Disclosure: We are funded by the Oxford Respiratory Biomedical Research Unit, part of the National Institue of Health Research.
REFERENCES
1.Calverley PM, Anderson JA, Celli B, et al. Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. N Engl J Med. 2007;356:775–89. doi: 10.1056/NEJMoa063070. [DOI] [PubMed] [Google Scholar]
2.Wedzicha JA, Banerji D, Chapman KR, et al. Indacaterol-Glycopyrronium versus Salmeterol-Fluticasone for COPD. N Engl J Med. 2016;374:2222–34. doi: 10.1056/NEJMoa1516385. [DOI] [PubMed] [Google Scholar]
3.From the Global Strategy for the Diagnosis, Management and Prevention of COPD, Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2017. 2017. Available from: http://goldcopd.org.
4.Pizzichini E, Pizzichini MM, Gibson P, et al. Sputum eosinophilia predicts benefit from prednisone in smokers with chronic obstructive bronchitis. Am J Respir Crit Care Med. 1998;158:1511–7. doi: 10.1164/ajrccm.158.5.9804028. [DOI] [PubMed] [Google Scholar]
5.Brightling CE, Monteiro W, Ward R, et al. Sputum eosinophilia and short-term response to prednisolone in chronic obstructive pulmonary disease: a randomised controlled trial. Lancet. 2000;356:1480–5. doi: 10.1016/S0140-6736(00)02872-5. [DOI] [PubMed] [Google Scholar]
6.Siva R, Green RH, Brightling CE, et al. Eosinophilic airway inflammation and exacerbations of COPD: a randomised controlled trial. Eur Respir J. 2007;29:906–13. doi: 10.1183/09031936.00146306. [DOI] [PubMed] [Google Scholar]
7.Bafadhel M, McKenna S, Terry S, et al. Acute exacerbations of chronic obstructive pulmonary disease: identification of biologic clusters and their biomarkers. Am J Respir Crit Care Med. 2011;184 doi: 10.1164/rccm.201104-0597OC. [DOI] [PubMed] [Google Scholar]
8.Singh D, Kolsum U, Brightling CE, et al. Eosinophilic inflammation in COPD: prevalence and clinical characteristics. Eur Respir J. 2014;44:1697–700. doi: 10.1183/09031936.00162414. [DOI] [PubMed] [Google Scholar]
9.Negewo NA, McDonald VM, Baines KJ, et al. Peripheral blood eosinophils: a surrogate marker for airway eosinophilia in stable COPD. Int J Chron Obstruct Pulmon Dis. 2016;11:1495–504. doi: 10.2147/COPD.S100338. [DOI] [PMC free article] [PubMed] [Google Scholar]
10.Pavord ID, Lettis S, Locantore N, et al. Blood eosinophils and inhaled corticosteroid/long-acting beta-2 agonist efficacy in COPD. Thorax. 2016;71:118–25. doi: 10.1136/thoraxjnl-2015-207021. [DOI] [PMC free article] [PubMed] [Google Scholar]
11.Pascoe S, Locantore N, Dransfield MT, et al. Blood eosinophil counts, exacerbations, and response to the addition of inhaled fluticasone furoate to vilanterol in patients with chronic obstructive pulmonary disease: a secondary analysis of data from two parallel randomised controlled trials. Lancet Respir Med. 2015;3:435–42. doi: 10.1016/S2213-2600(15)00106-X. [DOI] [PubMed] [Google Scholar]
12.Siddiqui SH, Guasconi A, Vestbo J, et al. Blood Eosinophils: A Biomarker of Response to Extrafine Beclomethasone/Formoterol in Chronic Obstructive Pulmonary Disease. Am J Respir Crit Care Med. 2015;192:523–5. doi: 10.1164/rccm.201502-0235LE. [DOI] [PMC free article] [PubMed] [Google Scholar]
13.Bafadhel M, Peterson S, De Blas MA, et al. Predictors of exacerbation risk and response to budesonide in patients with chronic obstructive pulmonary disease: a post-hoc analysis of three randomised trials. Lancet Respir Med. 2018;6:117–26. doi: 10.1016/S2213-2600(18)30006-7. [DOI] [PubMed] [Google Scholar]
14.Barnes NC, Sharma R, Lettis S, et al. Blood eosinophils as a marker of response to inhaled corticosteroids in COPD. Eur Respir J. 2016;47:1374–82. doi: 10.1183/13993003.01370-2015. [DOI] [PubMed] [Google Scholar]
15.Vestbo J, Papi A, Corradi M, et al. Single inhaler extrafine triple therapy versus long-acting muscarinic antagonist therapy for chronic obstructive pulmonary disease (TRINITY): a double-blind, parallel group, randomised controlled trial. Lancet. 2017;389:1919–29. doi: 10.1016/S0140-6736(17)30188-5. [DOI] [PubMed] [Google Scholar]
16.Lipson DA, Barnhart F, Brealey N, et al. Once-Daily Single-Inhaler Triple versus Dual Therapy in Patients with COPD. N Engl J Med. 2018;378:1671–80. doi: 10.1056/NEJMoa1713901. [DOI] [PubMed] [Google Scholar]
It is important to be clear about what an exacerbation is, what triggers it and what are the underlying mechanisms that lead to the symptoms and the clinical sequalae [1]. This is often not addressed and blanket recommendations are made which are non-specific and thus for an individual patient are unhelpful. I intend to address this and demonstrate how Broncho-dilators are the most effective therapies to prevent exacerbations as they address all of the changes which occur at an exacerbation, much more so that cortico-steroids which are given to patients in an indiscriminate manner in standard COPD practice.
Let’s start which what causes exacerbations. The three most significant factors are bacteria, viruses and airborne pollutants [2] hospital admissions, and mortality, and strongly influence health-related quality of life. Some patients are prone to frequent exacerbations, which are associated with considerable physiologic deterioration and increased airway inflammation. About half of COPD exacerbations are caused or triggered primarily by bacterial and viral infections (colds, especially from rhinovirus]. These can all trigger a cascade of immune response which leads to broncho-constriction, airway oedema and a reduction in lung function. This leads to symptoms. There are also systemic consequences of the response, leading to systemic inflammation and increasing the potential for the development of co-morbidities [3,4] though relationships between exacerbation recovery, recurrent exacerbation and inflammation have not been previously reported. In the present study, inflammatory changes at COPD exacerbations were related to clinical nonrecovery and recurrent exacerbations within 50 days. Serum interleukin (IL).
Our definitions of exacerbations of COPD are non-specific and often solely patient reported [5,6]. We urgently require a more scientific definition of AECOPD which is multi-dimensional and thus captures: causality, host response, physiological consequences and of course symptoms and patient impact. When different responses have been used in the past it has been interesting to see that dual broncho-dilator therapy (with Long acting anti-muscarinic treatment (LAMA), or long acting beta agonists (LABA)) has proved superior to an inhaled cortico-steroid (ICS) containing therapy. This was irrespective of the definition of AECOPD used [7].
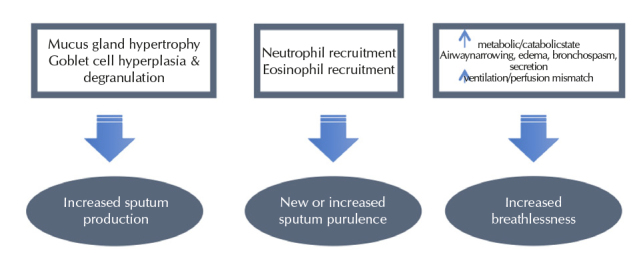
Symptoms are the driver for patients when detecting and declaring an AECOPD. So, what underpins the production of symptoms? Using the Anthonisen criteria our patients may suffer from an increase in sputum production, an increase in sputum purulence and an increase in breathlessness from baseline [6]. Figure 1 demonstrates the pathological effects which contribute to each of these three changes.
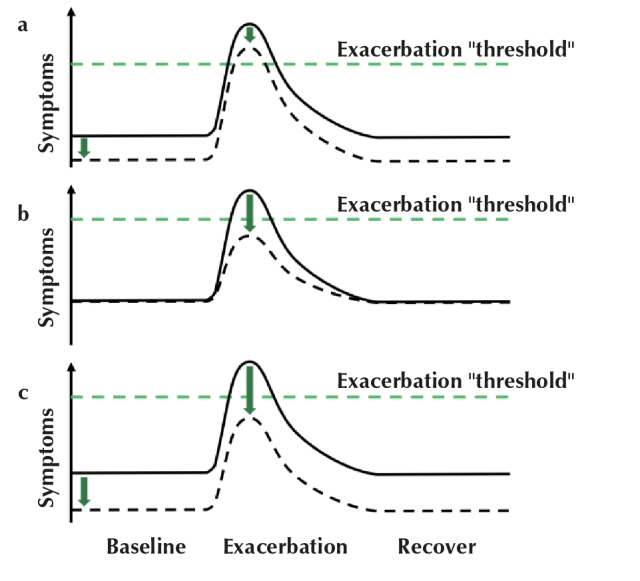
Overall, to detect an AECOPD then a patient must have an increase in their symptom load. It is therefore obvious that dual bronchodilators (long acting beta agonists combined with anti-muscarinic) will be effective. By either improving the patients baseline symptoms to a level whereby an AECOPD does not increase symptoms enough to be detectable or by raising the threshold whereby an AECOPD will be detected this approach to treatment will prove successful (Figure 2). This has been demonstrated to be an effective approach to the prevention of AECOPD in the Flame study, directly comparing LABA/LAMA therapy with LABA/ICS. In a similar group of patients, the LABA/LAMA treated patients had a lower risk of exacerbations, irrespective of exacerbation frequency, compared to ICS/LABA [7].
The pathological changes which lead to the symptoms of an acute exacerbation of COPD as described by Anthonisen et al. (6), adapted by author
So, how might this combination treatment reduce AECOPD and what evidence is there that they are effective against the underlying mechanisms? LABA/LAMA therapy reduces lung hyperinflation [8–10] a long-acting muscarinic antagonist indicated for maintenance treatment of chronic obstructive pulmonary disease (COPD), improves inspiratory capacity, reduces airway resistance and sputum production as well as potentially reducing lung inflammation and having anti-viral properties [11–13] with a preference of long-acting over short-acting drugs. Bronchodilators are classified into two classes based on distinct modes of action, i.e., long-acting antimuscarinics (LAMA, once-daily and twice-daily). These effects are all plausible mechanisms for the prevention of AECOPD [14] and others have shown that combinations of long-acting beta2-adrenergic agonists (LABAs).
Taking each in turn.
Lung hyperinflation. Classic studies of respiratory physiology have demonstrated that during an AECOPD hyperinflation increases. This in turn will cause the normal inspiratory and expiratory loop of breathing to be pushed further towards vital capacity due to the increase in residual volume. This in turn will lead to an increased work of breathing. LABA/LAMA therapy has been demonstrated to reduce hyperinflation with effects on the functional residual capacity and residual volume leading to reduced gas trapping [9,15] there is substantial use in individuals at lower risk. This raises the question of the comparative effectiveness of this combination as maintenance treatment in this group compared to other combination regimens. OBJECTIVE: The study aimed to assess the effect on lung function of once-daily tiotropium + olodaterol versus twice-daily salmeterol + fluticasone propionate in all participants with Global initiative for chronic Obstructive Lung Disease 2 or 3 (moderate to severe). These effects (of up to nearly 1000 mL) are much greater than any changes seen in FEV1. These effects are measured using plethysmography. Studies have also demonstrated significant effects on inspiratory capacity which may be considered as a surrogate measure [8].
Effects on mucus. Early studies on LABA therapy have demonstrated increase mucus clearance due to an enhanced mucociliary clearance. LAMAs are by their very nature anti-cholinergic and so will mediate, via the parasympathetic nervous system, an inhibition of mucus production. This can cause a problem for patients with a particularly dry mouth, but in the context of AECOPD with a productive cough, this effect may be useful [16].
Studies of inflammatory markers in sputum have shown that in those treated with tiotropium there is a reduction in sputum myeloperoxidase (MPO) and the cytokine CXCL-8 (IL-8) [16]. There is a lack of clarity as to the mechanism of these changes and if they are clinically relevant. Nonetheless the findings are intriguing and may lead to further developments later. More mechanistic studies in murine models have also demonstrated an effect of tiotropium (LAMA) on the inflammatory patterns. In mouse exposed to cigarette smoke the use of tiotropium led to a reduction in the overall number of inflammatory cells collected via broncho-alveolar lavage, with a particular effect on the levels of lavage neutrophils [17].
GOLD 2019 clearly states that bronchodilators are the mainstay of therapy and are effective in the prevention of AECOPD [18]. The GOLD evidence statements also confirm that dual therapy is more effective than a single long -acting agent. I would strongly recommend that we take a dual bronchodilator approach to our COPD patients. We will this optimize their lung function, reduce their symptoms and reduce the risk of future exacerbation.
At present we treat many of our patients with inhaled medications which contain inhaled cortico-steroids. This may have detrimental effects on our focus on the prevention of AECOPD. Doctors have assumed that inhaled corticosteroids (ICS) are effective in all patients and we must prescribe them to fully treat the patient. This may lead to complacency and the concern that we will not consider other interventions which are more effective. Smoking cessation must be paramount, and this is closely followed by the provision of effective pulmonary rehabilitation and in some cases palliative care. By giving ICS we may be deluded that we have done enough, we can never do enough. Dual broncho-dilators are really where we must start.
Possible effect of broncho-dilators (LABA/LAMA) to reduce the rate of exacerbations by changing the threshold for symptoms to develop and detect an AECOPD. (a) Broncho-dilators reduce symptoms at all times and thus reduce the level of symptoms which develop at an exacerbation, making it milder. (b) As an exacerbation develops the broncho-dilators may reduce the level of symptoms to that below the exacerbation threshold. (c) Broncho-dilators may reduce the overall symptom burden of the patient to such a degree at both baseline and exacerbation, so the exacerbation does not reach the threshold required for detection
Footnotes
Peer-review: Externally peer-reviewed.
Conflict of Interest: The author have no conflicts of interest to declare.
Financial Disclosure: We are funded by the Oxford Respiratory Biomedical Research Unit, part of the National Institue of Health Research.
REFERENCES
1.Rodriguez-Roisin R. Toward a consensus definition for COPD exacerbations. Chest. 2000;117(5 Suppl 2):398S–401S. doi: 10.1378/chest.117.5_suppl_2.398S. [DOI] [PubMed] [Google Scholar]
3.Perera WR, Hurst JR, Wilkinson TM, et al. Inflammatory changes, recovery and recurrence at COPD exacerbation. Eur Respir J. 2007;29:527–34. doi: 10.1183/09031936.00092506. [DOI] [PubMed] [Google Scholar]
4.Hurst JR. Exacerbation phenotyping in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2011;184:625–6. doi: 10.1164/rccm.201106-1136ED. [DOI] [PubMed] [Google Scholar]
5.Kessler R1, Ståhl E, Vogelmeier C, et al. Patient understanding, detection, and experience of COPD exacerbations: an observational, interview-based study. Chest. 2006;130:133–42. doi: 10.1378/chest.130.1.133. [DOI] [PubMed] [Google Scholar]
6.Anthonisen NR, Manfreda J, Warren CP, et al. Antibiotic therapy in exacerbations of chronic obstructive pulmonary disease. Ann Intern Med. 1987;106:196–204. doi: 10.7326/0003-4819-106-2-196. [DOI] [PubMed] [Google Scholar]
7.Wedzicha JA, Banerji D, Chapman KR, et al. Indacaterol-Glycopyrronium versus Salmeterol-Fluticasone for COPD. N Engl J Med. 2016;374:2222–34. doi: 10.1056/NEJMoa1516385. [DOI] [PubMed] [Google Scholar]
8.Beeh KM, Watz H, Puente-Maestu L, et al. Aclidinium improves exercise endurance, dyspnea, lung hyperinflation, and physical activity in patients with COPD: a randomized, placebo-controlled, crossover trial. BMC Pulm Med. 2014;14:209. doi: 10.1186/1471-2466-14-209. [DOI] [PMC free article] [PubMed] [Google Scholar]
9.Beeh KM, Derom E, Echave-Sustaeta J, et al. The lung function profile of once-daily tiotropium and olodaterol via Respimat(®) is superior to that of twice-daily salmeterol and fluticasone propionate via Accuhaler(®) (ENERGITO(®) study) Int J Chron Obstruct Pulmon Dis. 2016;11:193–205. doi: 10.2147/COPD.S95055. [DOI] [PMC free article] [PubMed] [Google Scholar]
10.Vogelmeier CF, Criner GJ, Martinez FJ, et al. Chronic obstructive pulmonary disease. Eur Respir J. 2017;12:433–8. [Google Scholar]
11.Beeh KM. The Role of Bronchodilators in Preventing Exacerbations of Chronic Obstructive Pulmonary Disease. Tuberc Respir Dis (Seoul) 2016;79:241–7. doi: 10.4046/trd.2016.79.4.241. [DOI] [PMC free article] [PubMed] [Google Scholar]
12.Trevethick M, Clarke N, Strawbridge M, et al. Inhaled muscarinic antagonists for COPD--does an anti-inflammatory mechanism really play a role? Curr Opin Pharmacol. 2009;9:250–5. doi: 10.1016/j.coph.2009.02.003. [DOI] [PubMed] [Google Scholar]
14.Beeh KM, Burgel PR, Franssen FME, et al. How Do Dual Long-Acting Bronchodilators Prevent Exacerbations of Chronic Obstructive Pulmonary Disease? Am J Respir Crit Care Med. 2017;196:139–49. doi: 10.1164/rccm.201609-1794CI. [DOI] [PubMed] [Google Scholar]
15.Watz H, Troosters T, Beeh KM, et al. ACTIVATE: the effect of aclidinium/formoterol on hyperinflation, exercise capacity, and physical activity in patients with COPD. Int J Chron Obstruct Pulmon Dis. 2017;12:2545–58. doi: 10.2147/COPD.S143488. [DOI] [PMC free article] [PubMed] [Google Scholar]
16.Powrie DJ, Wilkinson TM, Donaldson GC, et al. Effect of tiotropium on sputum and serum inflammatory markers and exacerbations in COPD. Rev Port Pneumol. 2008;14:573–6. doi: 10.1016/S0873-2159(15)30264-6. [DOI] [PubMed] [Google Scholar]