

Abstract
Background:
After North Carolina (NC) fire inspectors detected unsafe carbon monoxide (CO) levels inside several waterpipe cafés, the state fire code was amended to include provisions regulating waterpipe cafés, adding a requirement for air ventilation. These regulations apply to new buildings constructed after January 1, 2016, but can be enforced for older buildings where there exists a distinct hazard to life. We measured air quality at a sample of waterpipe cafés before and after the starting date of this regulation and collected information on presence of air ventilation.
Methods:
Air quality (CO, PM2.5) monitoring was conducted inside and outside of six waterpipe cafés in NC in September of 2015 (time 1) and September of 2016 (time 2). In addition, questionnaires were administered to managers from each waterpipe café at time 2 to determine presence of air ventilation systems.
Results:
Elevated levels of CO and PM2.5 were found inside waterpipe cafés at time 1 (Median CO= 42 ppm; Median PM2.5=379.3 μg/m3) and time 2 (Median CO= 65 ppm; Median PM2.5= 484.0 μg/m3), with no significant differences between time periods (p>0.05). Indoor levels were significantly higher than levels outside cafés at both time periods (p<0.05). All waterpipe cafés reported having an air ventilation system that was installed prior to time 1 air monitoring.
Conclusions:
Unsafe levels of CO and PM2.5 were observed in waterpipe cafés in NC, despite reported use of air ventilation systems. Prohibiting indoor waterpipe smoking may be necessary to ensure clean air for employees and patrons.
Keywords: secondhand smoke, waterpipe smoking, hookah smoking, air quality, policy
INTRODUCTION
Effective January 2, 2010, North Carolina’s (NC) smokefree law prohibited smoking in restaurants and bars.1 However, tobacco smoking, including waterpipes, is permitted in establishments that do not sell alcohol or prepare food onsite.2 Thus, employees and non-smoking patrons remain exposed to secondhand smoke (SHS) in waterpipe cafés (WCs) in NC.
In 2014, fire marshals in NC became concerned with SHS exposure in WCs due to elevated levels of CO.3 After unsafe CO levels were detected at several WCs, the NC Building Code Council approved adding new regulations for WCs to the state fire code. Section 310.9 of the updated fire code states that “An approved ventilation system is required” for all WCs.4 The regulation applies to buildings constructed after January 1, 2016, but can be applied to older buildings where there exists a distinct hazard to life or property (personal correspondence, Dan Austin, North Carolina Department of Insurance).
To determine if WCs use air ventilation systems and whether these adequately control secondhand smoke levels, we conducted air monitoring in a sample of WCs in NC. Air monitoring was conducted during two time periods – before and after January 1, 2016 – to assess changes due to the regulation.
METHODS
Internet searches (i.e., Google, Google Maps, Yelp) identified 14 WCs in the Research Triangle area (i.e., Raleigh, Durham, Chapel Hill) of NC. Calls were made to each business: two businesses could not be reached, one business was confirmed closed, and one business no longer offered waterpipe smoking. The remaining 10 WCs were visited in September of 2015 for time 1 monitoring. During time 1 monitoring, one WC only offered outdoor waterpipe smoking, and no waterpipe smoking was found at a second café. Thus, time 1 monitoring was conducted in eight WCs. The same WCs were revisited in September of 2016 for time 2 monitoring. During time 2 monitoring, we observed that one café had permanently closed, and a second café was avoided due to safety concerns that arose during time 1 monitoring. The analytic sample (i.e., monitoring conducted at both times 1 and 2) included six WCs. Monitoring was also conducted within a smokefree control (pizza restaurant). All WC monitoring was conducted on Friday and Saturday evenings, when WCs are typically busiest.5
PM2.5 levels were measured using the TSI SidePak AM510 Personal Aerosol Monitor (TSI Inc, USA). A calibration factor of 0.38 was applied.6 CO levels were measured using a EL-USB-CO300 (Lascar Electronics Inc; USA). Both devices were set to one-minute logging. Devices were concealed to prevent influencing smoking behaviors. Monitoring was conducted for a minimum of 30 minutes inside each café, and approximately five minutes was spent monitoring outdoor air before café entry and after exit.
Observations were made inside each café for number of people and waterpipes in use at 0, 15, and 30 minutes. Other information that could influence air quality, (e.g., cigarette smoking) were also recorded.
During time 2 monitoring, we asked a manager from each WC whether the café had air ventilation, and when it was installed. IRBs at Wake Forest School of Medicine and University of North Carolina exempted this study from review.
Wilcoxon rank-sum tests were used to compare mean indoor and outdoor levels of CO and PM2.5. Wilcoxon matched-pairs signed-rank tests were used to test for differences in CO and PM2.5 levels between times 1 and 2 measures inside each café, and number of waterpipes and people at times 1 and 2. One-sample Wilcoxon signed rank tests were used to test for differences between the median indoor CO and PM2.5 levels inside WCs and the mean indoor CO and PM2.5 levels inside the smokefree control at times 1 and 2.
RESULTS
Supplement 1 lists the mean number of people and waterpipes in use inside each café at times 1 and 2. There were no significant differences observed in number of waterpipes (p=0.173) or people (p=0.293) between time periods.
Mean indoor CO levels at time 1 ranged from 2.0–141.4 ppm (median=46.2 ppm), and were significantly higher than outdoor levels (p=0.030). Mean indoor PM2.5 levels at time 1 ranged from 18.0–1891.9 μg/m3 (median=379.3 μg/m3), and were significantly higher than outdoor levels (p=0.010).
At time 2 monitoring, mean CO levels inside ranged from 3.7–239.7 ppm (median=64.6 ppm), and were significantly higher than outdoor levels (p=0.016). Mean PM2.5 levels at time 2 ranged from 73.7–1886.3 μg/m3 (median=484.0 μg/m3), and were significantly higher than outdoor levels p=0.004). As a reference, the mean annual PM2.5 concentrations reported by the U.S. Environmental Protection Agency (EPA) for Raleigh, NC ranged from 6.9–10.6μg/m3 in 2015 and 7.6–9.9 μg/m3 in 2016.7
Figures 1a and 1b display box plots of mean CO and PM2.5 levels between times 1 and 2, respectively. No significant differences were found for indoor CO levels (p=0.173) and PM2.5 levels (p=0.116) between the times 1 and 2 visits. Figures 1a and 1b also include EPA’s National Ambient Air Quality Standards for CO (8-hour average: 9 ppm and 1-hour average: 35 ppm) and the EPA’s Ambient Air Quality Index’s (AQI) “good” (12 μg/m3) and “hazardous” (250.5 μg/m3) levels for PM2.5 for outdoor air.8,9 At times 1 and 2, mean PM2.5 levels in all venues exceeded the EPA’s AQI’s “good” level, while levels in four out of six cafés exceeded the “hazardous” level. Mean CO levels exceeded the EPA’s 8-hour limit for CO in five of six cafés and the 1-hour limit for CO in three of six cafés during visits 1 and 2.
Figure 1.
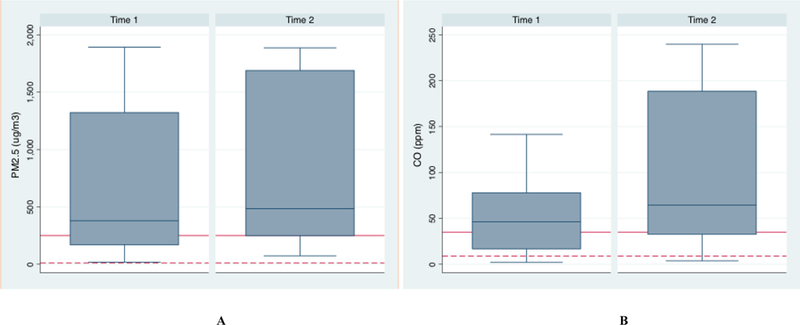
Box and whisker plots of mean PM2.5 levels (A) at time 1 and time 2 and mean CO levels (B) at time 1 and time 2 inside six waterpipe cafés in North Carolina. Top, middle and lower ends of boxes represent 75%, 50%, and 25% percentiles, respectively. Whiskers represent maximum and minimum mean levels. Solid horizontal lines represent the EPA’s Ambient Air Quality index’s “hazardous” level for PM2.5 (250.5 μg/m3) and EPA’s 1-hour time weighted average exposure limit for CO (35 ppm) for panels A and B, respectively. Dashed horizontal lines represents the EPA’s Ambient Air Quality Index’s “good” level for PM2.5 (12 μg/m3) and the EPA’s 8-hour time weighted average exposure limit for CO (9 ppm) for panels A and B, respectively.
At time 1, mean CO levels inside and outside of the control venue were 0.0 ppm and 0.4 ppm, respectively. At time 2, mean CO levels were 0.0 ppm inside and outside of the smokefree control. Mean PM2.5 levels were 2.9 μg/m3 inside and 5.7 μg/m3 outside of the control venue at time 1. At time 2, mean PM2.5 levels were 4.5 μg/m3 inside and 4.1 μg/m3 outside of the control venue. Median CO and PM2.5 levels inside of the WCs were significantly higher than the mean CO and PM2.5 levels inside the smokefree control at times 1 and 2 (p=0.016)
All managers indicated having air ventilation installed before time 1 monitoring.
DISCUSSION
This is the first known study to measure indoor air quality inside WCs and inquire about presence of air ventilation systems. Unsafe levels of CO and PM2.5 were detected at both visits, despite all cafés reportedly having ventilation systems. These findings underscore the potential dangers of waterpipe SHS and the need for additional protections for employees and the public.
The elevated levels of CO detected are consistent with previous research conducted in Canada10, USA11,12, and Egypt.13 At times 1 and 2, mean CO levels in 50% of cafés exceeded the EPA’s recommended exposure limit (35 ppm). Further, 50% of cafes had levels exceeding 100 ppm, a level that may induce CO poisoning symptoms.14 In the US, >75% of waterpipe smokers report smoking for ≥30 minutes.15 Thus, given the high levels of CO and length of time typically spent smoking, both patrons and workers may be at risk for CO poisoning.
Similarly, 50% of cafés had mean PM2.5 levels exceeding the EPA’s AQI’s “hazardous” level. Further, all cafés exceeded the EPA’s AQI’s “good” level. The overall median PM2.5 level across all cafés and both visits (399.2 μg/m3) was 33-times the EPA’s AQI’s “Good” level. These findings are similar to studies conducted elsewhere.16,17
Concerns about unsafe CO levels in WCs have been expressed through the modification of the fire code to include a provision to regulate WCs.4 However, these findings indicate that, to date, this modification has resulted in no significant reductions in CO levels within a sample of WCs. This study did not assess whether local fire marshals have inspected WCs for compliance with the new fire code requirements, or if they plan to enforce these regulations in the future.
Previous research has found that ventilation cannot clear smoke-filled air and is not a substitute for smoking bans.18 The American Society of Heating, Refrigerating, and Air-Conditioning Engineers (ASHRAE) has concluded that adverse health effects of tobacco smoke exposure in a room with smoking cannot be controlled with ventilation.19 In the 2006 US Surgeon General’s Report on the dangers of SHS20, the effectiveness of ventilation on improving indoor air contaminated by smoking was reviewed. The report concluded that current air ventilation systems used in residential and commercial buildings “cannot fully control exposures to secondhand smoke unless a complete smoking ban is enforced.”20 The results of this study confirm that conclusion as hazardous levels of CO and PM2.5 were measured, despite WCs indicating the use of ventilation systems.
This study is limited by its small sample size, and the responses by managers may be subject to social desirability bias. Further, we could not confirm the presence of air ventilation systems, whether the system was properly functioning, or the ventilation rate. Differences in how frequently cafés replace charcoal, or store burning charcoal, likely impacted air quality, and were not measured. We attempted to estimate interior volume by having two researchers independently pace the length and width of the interior environment and estimate ceiling height. But due to the presence of irregular-shaped rooms, slanted and pointed ceilings, and physical obstacles (e.g., patrons, furniture) that blocked pacing, these data are not reported.
In conclusion, unsafe levels of CO and PM2.5 were measured within a sample of WCs in NC, despite the reported presence of air ventilation. Prohibiting indoor waterpipe smoking may be required to ensure clean air for employees and customers.
Supplementary Material
Mean number of waterpipes in use, total number of people, mean CO levels, mean PM2.5 levels, and other factors potentially influencing air quality observed at time 1 and time 2 within six waterpipe cafés and one control venue in North Carolina.
WHAT THIS PAPER ADDS.
Indoor waterpipe smoking generates dangerous levels of CO and PM2.5.
While previous research has shown that air ventilation systems cannot fully control exposures to harmful chemicals in cigarette secondhand smoke, little research has been conducted on the impact of the presence of air ventilation systems on waterpipe secondhand smoke.
The present study measured indoor CO and PM2.5 in a sample of waterpipe cafés in North Carolina, USA, where new regulations have been enacted for waterpipe cafés. We found unsafe levels of CO and PM2.5, despite all cafés reporting the use of air ventilation systems. These findings suggest that additional measures are needed to protect employees and the public from the dangers of waterpipe secondhand smoke.
ACKNOWLEDGEMENTS
ABS is supported by the UNC Lineberger Cancer Control Education Program (T32 CA057726). MJT was supported by the Roswell Park Comprehensive Cancer Center and National Cancer Institute (NCI) grant P30CA016056.
REFERENCES
- 1.General Assembly of North Carolina. An act to prohibit smoking in certain public places and certain places of employment. Session Law 2009–27; House Bill 2.. [Google Scholar]
- 2.Tobacco Prevention and Control Branch North Carolina Health and Human Services. SmokefreeNC: FAQs. http://www.tobaccopreventionandcontrol.ncdhhs.gov/smokefreenc/faq.htm. Accessed March 8, 2018.
- 3.Steimer J Charlotte steps up scrutiny, regulation of hookah bars. Charlotte Observer. July 19, 2015. http://www.charlotteobserver.com/news/business/article27550105.html, March 8, 2018. [Google Scholar]
- 4.North Carolina State Building Code: Fire Prevention Code (2012): Third Printing, May 2017. https://cdn-codes-pdf.iccsafe.org/public/getpdf/9456/2012_NC_Fire.pdf. Accessed May 13, 2018.
- 5.Zhou S, Behrooz L, Weitzman M, et al. Secondhand hookah smoke: an occupational hazard for hookah bar employees. Tob Control. 2017;26(1):40–45. [DOI] [PubMed] [Google Scholar]
- 6.Travers MJ, Kulak JA, Vogl L. Waterpipe cafes are hazardous to your health: Determination of a waterpipe specific calibration factor. Int J Hyg Environ Health. 2018;221(1):48–53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.United States Environmental Protection Agency. Outdoor Air Quality Data - Monitor Values Report. https://www.epa.gov/outdoor-air-quality-data/monitor-values-report. Accessed March 8, 2018.
- 8.U.S. Environmental Protection Agency. (2013). National ambient air quality standards for particulate matter; final rule. Federal Register, 78(10), 3086–3287. [Google Scholar]
- 9.United States Environmental Protection Agency. NAAQS Table. https://www.epa.gov/criteria-air-pollutants/naaqs-table. Accessed March 8, 2018.
- 10.Zhang B, Haji F, Kaufman P, Muir S, Ferrence R. ‘Enter at your own risk’: a multimethod study of air quality and biological measures in Canadian waterpipe cafes. Tob Control. 2015;24(2):175–181. [DOI] [PubMed] [Google Scholar]
- 11.Zhou S, Weitzman M, Vilcassim R, et al. Air quality in New York City hookah bars. Tob Control 2015;24(e3):e193–198. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Torrey CM, Moon KA, Williams DA, et al. Waterpipe cafes in Baltimore, Maryland: Carbon monoxide, particulate matter, and nicotine exposure. J Expo Sci Environ Epidemiol. 2015;25(4):405–410. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Moon KA, Magid H, Torrey C, et al. Secondhand smoke in waterpipe tobacco venues in Istanbul, Moscow, and Cairo. Environ Res. 2015;142:568–574. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Iowa State University. Carbon monoxide concentrations https://www.abe.iastate.edu/extension-and-outreach/carbon-monoxide-concentrations-table-aen-172/. Accessed March 8, 2018.
- 15.Salloum RG, Thrasher JF, Getz KR, Barnett TE, Asfar T, Maziak W. Patterns of Waterpipe Tobacco Smoking Among U.S. Young Adults, 2013–2014. Am J Prev Med. 2017;52(4):507–512. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Al Mulla A, Fanous N, Seidenberg AB, Rees VW. Secondhand smoke emission levels in waterpipe cafes in Doha, Qatar. Tob Control. 2015;24(e3):e227–231. [DOI] [PubMed] [Google Scholar]
- 17.Cobb CO, Vansickel AR, Blank MD, Jentink K, Travers MJ, Eissenberg T. Indoor air quality in Virginia waterpipe cafes. Tob Control. 2013;22(5):338–343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.KC RJJ. Can Displacement Ventilation Control Secondhand ETS? ASHRAE IAQ Applications. 2006;7(4):2–6. [Google Scholar]
- 19.American Society of Heating R, and Air-Conditionaing Engineers,. Environmental Tobacco Smoke: Position Document. 2005. [Google Scholar]
- 20.US Department of Health Human Services. The health consequences of involuntary exposure to tobacco smoke: a report of the Surgeon General. Atlanta, GA: US Department of Health and Human Services, Centers for Disease Control and Prevention, Coordinating Center for Health Promotion, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 2006;709. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Mean number of waterpipes in use, total number of people, mean CO levels, mean PM2.5 levels, and other factors potentially influencing air quality observed at time 1 and time 2 within six waterpipe cafés and one control venue in North Carolina.