

Abstract
Background
We report a rare case in which an epiphyseal injury of the distal radius caused entrapment and rupture of the index extensor digitorum communis tendon during conservative treatment.
Case presentation
A 16-year-old girl suffered epiphyseal injury of the right distal radius with palmar displacement during playing judo. Closed reduction and application of a short arm cast were performed. 4 weeks after injury, movement of her index finger was limited. Extensor tendons adhesion at the fracture site was suspected. It was found that the index extensor digitorum communis tendon had become trapped and ruptured at the site of epiphyseal injury, then reconstruction was done by tendon transfer. At 12 months after surgery, the patient had resumed judo at the same level as before the injury.
Conclusions
The present case suggested that there is a risk of extensor tendon entrapment associated with closed reduction.
Keywords: Epiphyseal injury of the distal radius, Extensor digitorum communis tendon, Tendon entrapment, Palmar displacement
Background
The distal radius is the most common site of epiphyseal injury, accounting for about 40% of all epiphyseal plate injuries [1]. Generally, reasonable closed reduction of the fracture can be achieved, and the outcome is usually satisfactory after immobilization for several weeks. Tendon rupture is a well-recognized complication of Smith's fracture, and Franz reported entrapment of the extensor pollicis longus (EPL) tendon associated with this type of fracture [2]. The mechanism of entrapment has been described in a cadaver model, based on the assumption that Smith's fracture results from forced excessive pronation of the forearm, after which supination of the proximal fragment shifts the EPL tendon towards the ulna and it becomes trapped at the fracture site [3].
We report a rare case in which an epiphyseal injury of the distal radius caused entrapment and rupture of the extensor digitorum communis (EDC) tendon to the index finger during conservative treatment.
Case presentation
A 16-year-old girl suffered epiphyseal injury of the right distal radius with palmar displacement during playing judo (Fig. 1A and B). Closed reduction and application of a short arm cast were performed, with radiographs showing satisfactory reduction. After removal of the cast at 4 weeks after injury, the patient complained that movement of her index finger was limited. The range of wrist motion with the index finger extended was flexion of 85° and extension of 85°, while the range of wrist motion with the index finger flexed was flexion of 20° and extension of 85°, since the tenodesis effect limited wrist flexion (Fig. 2A and B). Pronation and supination were not restricted, with both having a range of 85°. Grip strength was 24 kg on the right and 30 kg on the left. The Visual Analog Scale (VAS), Quick Disabilities of the Arm, Shoulder and Hand (Q-DASH) score, and Cooney score were 5/10, 4.55/100, and 90/100, respectively. Radiography showed that the fracture had healed but dorsal epiphyseal displacement persisted. CT scans clearly revealed the displacement (Fig. 3A–C). These findings led to a diagnosis of extensor tendon adhesion at the fracture site, and tenolysis surgery was planned.
Fig. 1.
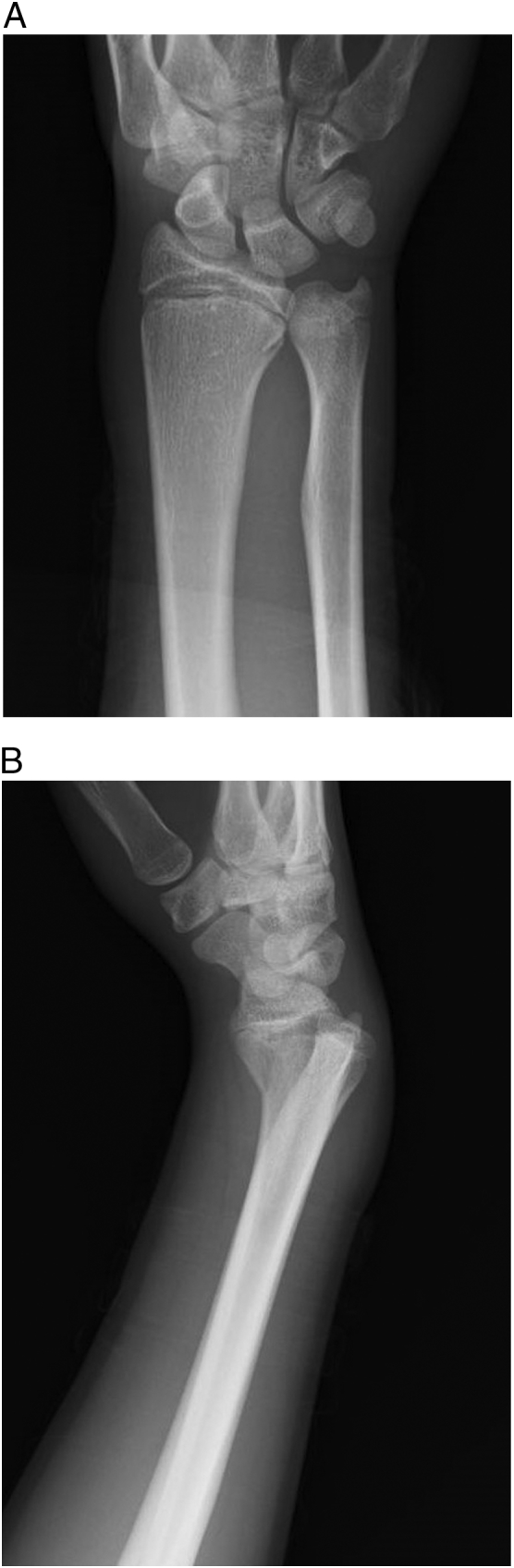
Radiographs obtained at the time of injury, showing epiphyseal fracture of the right distal radius with palmar displacement.
A: Antero-posterior view.
B: Lateral view.
Fig. 2.

Range of wrist motion with the index finger extended and flexed.
With the index finger extended, the range of wrist motion was 85°of flexion and 85°of extension (A). With the index finger flexed, the range of wrist motion was 20° of flexion and 85° of extension (B).
Fig. 3.

Preoperative radiographs and CT scan.
Radiographs showed healing of the fracture with persistent dorsal displacement of the epiphyseal fragment (A: Antero-posterior view, B: Lateral view). CT clearly showed the displacement (C).
A 3–4 transseptal approach was used, passing through the extensor retinaculum in the septum between the third and fourth compartments, after which the extensor retinaculum was retracted to the ulnar side. It was found that the index finger EDC tendon had become trapped and ruptured at the site of epiphyseal injury (Fig. 4A). Reconstruction was done by transfer of the distal end of the index finger EDC tendon to the middle finger EDC tendon (Fig. 4B). Finally, the extensor tendons were protected with extensor retinaculum at the site of epiphyseal injury (Fig. 4C).
Fig. 4.

Intraoperative findings.
A: The index finger EDC tendon was trapped and ruptured at the epiphyseal fracture site.
B: Reconstruction of the index finger EDC tendon was done by transfer of its distal end to the middle finger EDC tendon.
C: The extensor tendons were protected with extensor retinaculum at the site of epiphyseal injury.
At 12 months after surgery, the range of wrist motion with the index finger extended was as follows: flexion of 75°, extension of 90°, supination of 90°, and pronation of 90° (Fig. 5A–D). Grip strength was 28 kg on the right and 26 kg on the left, while the VAS, Q-DASH score, and Cooney score were 0/10, 0/100, and 100/100, respectively. The patient had resumed judo at the same level as before the injury.
Fig. 5.

Range of wrist motion at 12 months after surgery.
With the index finger extended, the range of wrist motion was 75° of flexion (A), 90° of extension (B), 90° of supination (C), and 90° of pronation (D).
Discussion
Rupture of the EPL tendon is a well-recognized complication of epiphyseal injury at the distal radius [2]. Injury to the EPL tendon generally occurs due to irritation by fractures with a dorsal roof bone fragment and Lister's tubercle functions as a pulley for the tendon [4]. In contrast, entrapment of the long extensor tendons to the fingers has been described in several patients with Smith's fracture of the distal radius [[5], [6], [7]]. Tendon entrapment was previously reported in pediatric patients who had Salter-Harris type 2 fracture of the distal radius with palmar displacement, and our case showed displacement in the same direction [8,9]. It was previously reported that tendon entrapment should be suspected if it is impossible achieve anatomical reduction [10].
In our patient, adequate reduction of the distal fragment was obtained despite entrapment of the tendon and limitation of finger motion was not noted during immobilization. The patient only became aware that index finger motion was limited after removal of the cast. Okazaki reported extensor tendon entrapment in 8 out of 633 patients with acute fracture of the distal radius. Seven of these 8 patients had a fracture with palmar displacement, and one patient had dorsal displacement. The EPL, extensor indicis proprius (EIP), and EDC tendons were affected in the 7 patients with palmar displacement, while entrapment of the flexor digitorum profundus tendon was seen in the patient with dorsal displacement [8]. Our case seems to be rare, since entrapment only affected the index finger EDC tendon. Although it is unclear why the superficially located index finger EDC tendon was entrapped rather than the deeper EIP tendon, it may have occurred due to pressure on the extensor tendon from the dorsal side during manual reduction of the palmar displaced fragment.
Tendon rupture due to entrapment at a fracture site can be treated by three surgical options, which are tenolysis, reconstruction using a tendon graft, or reconstruction by tendon transfer. In this young patient, there was no degeneration or adhesion of the unaffected tendons and we wanted to maintain the extension function of index finger. Therefore, reconstruction was performed by transferring the distal end of the index finger EDC tendon to the middle finger EDC tendon.
Funding
No funding was required in preparation of the manuscript.
Availability of data and materials
Not applicable.
Ethics approval and consent to participate
The study was carried out in accordance with the Declaration of Helsinki and the appropriate ethical framework. The patient and her parents provided informed consent for the publication of her clinical data and radiographs within the context of this case report.
Consent for publication
Not applicable.
Declaration of Competing Interest
None.
Acknowledgements
Not applicable.
References
- 1.Bailey D.A., Wedge J.H., McCulloch R.G., Martin A.D., Bernhardson S.C. Epidemiology of fractures of the distal end of the radius in children as associated with growth. J. Bone Joint Surg. Am. 1989;71:1225–1231. [PubMed] [Google Scholar]; .D.A. Bailey, J.H. Wedge, R.G. McCulloch, A.D Martin, S.C. Bernhardson, Epidemiology of fractures of the distal end of the radius in children as associated with growth, J Bone Joint Surg Am 71 (1989) 1225–1231. [PubMed]
- 2.Franz T. Entrapment of extensor pollicis longus tendon after volar plating of a Smith type pediatric distal forearm fracture. J. Hand Surg. Asian Pac. Vol. 2016;21:253–256. doi: 10.1142/S2424835516720085. [DOI] [PubMed] [Google Scholar]; T. Franz, Entrapment of Extensor Pollicis Longus Tendon after Volar Plating of a Smith Type Pediatric Distal Forearm Fracture, J Hand Surg Asian Pac Vol 21 (2016) 253-256. [DOI] [PubMed]
- 3.Hunt D.D. Dislocation of the extensor pollicis longus tendon in Smith's fracture of the radius. A case report. J. Bone Joint Surg. Am. 1969;51:991–994. [PubMed] [Google Scholar]; D.D. Hunt, Dislocation of the extensor pollicis longus tendon in Smith'’s fracture of the radius. A case report, J Bone Joint Surg Am 51 (1969) 991-994. [PubMed]
- 4.Naito K., Sugiyama Y., Dilokhuttakarn T. A survey of extensor pollicis longus tendon injury at the time of distal radius fractures. Injury. 2017;48:925–929. doi: 10.1016/j.injury.2017.02.033. [DOI] [PubMed] [Google Scholar]; K. Naito, Y. Sugiyama, T. Dilokhuttakarn, et al, A survey of extensor pollicis longus tendon injury at the time of distal radius fractures, Injury 48 (2017) 925-929. [DOI] [PubMed]
- 5.Shively J.L., Lesnick D.S. Distal radius fracture with tendon entrapment. Orthopedics. 1982;10:1330–1332. doi: 10.3928/0147-7447-19821001-08. [DOI] [PubMed] [Google Scholar]; J.L. Shively, D.S. Lesnick, Distal radius fracture with tendon entrapment, Orthopedics 10 (1982) 1330-1332. [DOI] [PubMed]
- 6.Kumar A.A., Kelly C.P. Extensor pollicis longus entrapment after Smith's fracture. Injury. 2003;34:75–78. doi: 10.1016/s0020-1383(02)00083-9. [DOI] [PubMed] [Google Scholar]; .A. A Kumar, C.P. Kelly, Extensor pollicis longus entrapment after Smith's fracture, Injury 34 (2003) 75-78. [DOI] [PubMed]
- 7.Cavanilles Walker J.M., Masferrer Pino A., Alberti Fito G. Entrapment of the extensor pollicis longus tendon after a radial fracture in a child. J. Hand Surg. Eur. Vol. 2012;37:182–183. doi: 10.1177/1753193411430028. [DOI] [PubMed] [Google Scholar]; J.M. Cavanilles Walker, A. Masferrer Pino, G. Alberti Fito, Entrapment of the extensor pollicis longus tendon after a radial fracture in a child, J Hand Surg Eur 37 (2012) 182-183. [DOI] [PubMed]
- 8.Okazaki M., Tazaki K., Nakamura T., Toyama Y., Sato K. Tendon entrapment in distal radius fractures. J. Hand Surg. Eur. Vol. 2009;34:479–482. doi: 10.1177/1753193408100960. [DOI] [PubMed] [Google Scholar]; M. Okazaki, K. Tazaki, T. Nakamura, Y. Toyama, K. Sato, Tendon entrapment in distal radius fractures, J Hand Surg Eur 34 (2009) 479-482. [DOI] [PubMed]
- 9.Karlsson J., Appelqvist R. Irreducible fracture of the wrist in a child. Entrapment of the extensor tendons. Acta Orthop. Scand. 1987;58:280–281. doi: 10.3109/17453678709146485. [DOI] [PubMed] [Google Scholar]; J. Karlsson, R. Appelqvist, Irreducible fracture of the wrist in a child. Entrapment of the extensor tendons, Acta Orthop Scand 58 (1987) 280-281. [DOI] [PubMed]
- 10.Thomas W.G., Kershaw C.J. Entrapment of extensor tendons in a Smith's fracture: brief report. J. Bone Joint Surg. (Br.) 1988;70 (:491. doi: 10.1302/0301-620X.70B3.3372582. [DOI] [PubMed] [Google Scholar]; W.G. Thomas, C.J. Kershaw, Entrapment of extensor tendons in a Smith's fracture: brief report, J Bone Joint Surg Br 70 (1988) 491. [DOI] [PubMed]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Not applicable.