

Abstract
Proximal metatarsal stress fractures are common at base of the second metatarsal, typically seen in repetitive impact athletes, dancers, and those with cavus feet. It is caused by increased bone resorption rather than formation in a state of abrupt increased physical activity or intensity, leading to repetitive microfractures and eventually stress fracture. It is characterized by swelling and tenderness of a prolonged duration. We report a case of a 40-year-old female having left foot pain diagnosed with stress fracture on Tc-99m HDP single-photon emission computed tomography (SPECT)-CT. We emphasize the use of SPECT/CT in allocating active source of pain in the feet.
Keywords: Foot pain, stress fracture, Tc-99m HDP single-photon emission computed tomography-computed tomography
A 40-year-old female presented with a 1-month history of left ankle and feet pain. Pain started after new-fangled strenuous exercise. Clinical examination shows mild swelling and tenderness. Plain X-ray is normal. Three-phase bone scintigraphy is performed by injecting 22 mCi of Tc-99m HDP intravenously. Dynamic flow and blood pool images showed increased flow and hyperemia at the left midtarsal region. The delayed whole body show focal area of increase tracer uptake at the base of left second metatarsal bone [Figure 1]. Noncontrast computed tomography (CT) coronal, sagittal, and transaxial images show fracture line with corresponding increased uptake on fused images [Figure 2]. Tc-99m HDP single-photon emission computed tomography (SPECT)-CT images better delineate the uptake at base of the second metatarsal bone which may present a source of pain, suggestive of stress fracture.
Figure 1.

Dynamic flow and blood pool images showing increased flow and hyperemia at the left midtarsal region. The delayed whole body showing focal area of increase tracer uptake at the base of left second metatarsal bone. Right foot is unremarkable
Figure 2.
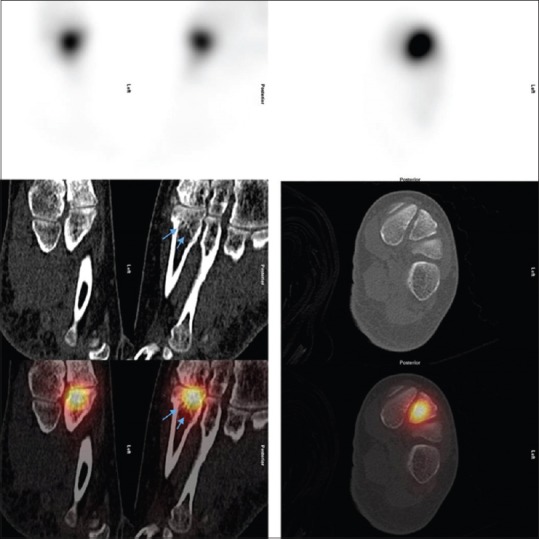
Noncontrast computed tomography sagittal, coronal, and transaxial images showing fracture line with corresponding increased uptake on fused images
Proximal metatarsal fractures occur most commonly at the base of the second metatarsal and are characterized by swelling and tenderness. A proximal stress fracture in the second metatarsal is less as compared to nonproximal stress fracture; however, it is frequently seen with dancers that particularly often performed “en pointe” position, repetitive impact athletes, and those with canvus feet.[1,2] There is loss of bone integrity seen in a stress fracture develop after cyclical, submaximal loading that occurs in a state of usually abrupt increased in physical activity and intensity, leading to bone weakening and eventually stress fracture.[3] Diagnosis is reached through a proper history collection and physical examination followed by imaging with X-ray. In the first few weeks following the onset of symptoms, X-ray images are likely to be normal; thus, if highly suspicious of stress fracture, CT scan or magnetic resonance imaging (MRI) is performed. CT scan can accurately locate the fracture line whereas MRI is the preferred sensitive diagnostic tool of choice.[4] Similarly, bone scintigraphy can show evidence of stress fracture on few days of the onset of symptoms. It has been known as a highly sensitive modality with limited specificity in imaging of metatarsal stress fractures.[5] The addition of SPECT-CT increased the specificity of bone scintigraphy making it compatible with MRI study.[6] SPECT-CT allows precise anatomical localization of bone turnover abnormalities.[7] SPECT-CT is reportedly useful for localizing active disease in foot and ankle pathology.[8,9] In our case, SPECT-CT helps in localizing the source of pain and diagnosing the stress fracture with confidence.
Management of proximal metatarsal stress fractures is mainly conservative with abstinence from the causative activity and wearing the proper supportive footwear and cast.[10] The amount of mobilization limitation required to achieve healing is dependent on the severity of symptoms and etiology of the fracture. In some cases, nonunion occurs and may require surgical intervention.[1]
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Kaiser PB, Guss D, DiGiovanni CW. Stress fractures of the foot and ankle in athletes. Foot Ankle Orthop. 2018;3:1–11. doi: 10.1177/24730114231195045. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Chuckpaiwong B, Cook C, Pietrobon R, Nunley JA. Second metatarsal stress fracture in sport: Comparative risk factors between proximal and non-proximal locations. Br J Sports Med. 2007;41:510–4. doi: 10.1136/bjsm.2006.033571. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Simons SM. Foot injuries in the runner. In: O'Connor FG, Wilder RP, editors. Textbook of Running Medicine. New York: McGraw-Hill; 2001. pp. 213–26. [Google Scholar]
- 4.Albisetti W, Perugia D, De Bartolomeo O, Tagliabue L, Camerucci E, Calori GM, et al. Stress fractures of the base of the metatarsal bones in young trainee ballet dancers. Int Orthop. 2010;34:51–5. doi: 10.1007/s00264-009-0784-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Brukner P, Bennell K. Stress fractures in female athletes. Diagnosis, management and rehabilitation. Sports Med. 1997;24:419–29. doi: 10.2165/00007256-199724060-00006. [DOI] [PubMed] [Google Scholar]
- 6.Mohan HK, Strobel K, van der Bruggen W, Gnanasegaran G, Kampen WU, Kuwert T, et al. The role of hybrid bone SPECT/CT imaging in the work-up of the limping patient: A symptom-based and joint-oriented review. Eur J Hybrid Imaging. 2018;2:8. doi: 10.1186/s41824-018-0026-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Pelletier-Galarneau M, Martineau P, Gaudreault M, Pham X. Review of running injuries of the foot and ankle: Clinical presentation and SPECT-CT imaging patterns. Am J Nucl Med Mol Imaging. 2015;5:305–16. [PMC free article] [PubMed] [Google Scholar]
- 8.Huellner MW, Strobel K. Clinical applications of SPECT/CT in imaging the extremities. Eur J Nucl Med Mol Imaging. 2014;41(Suppl 1):S50–8. doi: 10.1007/s00259-013-2533-5. [DOI] [PubMed] [Google Scholar]
- 9.Mohan HK, Gnanasegaran G, Vijayanathan S, Fogelman I. SPECT/CT in imaging foot and ankle pathology-the demise of other coregistration techniques. Semin Nucl Med. 2010;40:41–51. doi: 10.1053/j.semnuclmed.2009.08.004. [DOI] [PubMed] [Google Scholar]
- 10.Brukner P, Bradshaw C, Bennell K. Managing common stress fractures: Let risk level guide treatment. Phys Sportsmed. 1998;26:39–47. doi: 10.3810/psm.1998.08.1104. [DOI] [PubMed] [Google Scholar]