

Summary
Eculizumab is the first and only medication approved for paroxysmal nocturnal haemoglobinuria (PNH) and atypical haemolytic uraemic syndrome (aHUS) treatment. However, eculizumab safety based on long‐term pharmacovigilance is unknown. This analysis summarises safety data collected from spontaneous and solicited sources from 16 March 2007 through 1 October 2016. Cumulative exposure to eculizumab was 28 518 patient‐years (PY) (PNH, 21 016 PY; aHUS, 7502 PY). Seventy‐six cases of meningococcal infection were reported (0·25/100 PY), including eight fatal PNH cases (0·03/100 PY). Susceptibility to meningococcal infections remained the key risk in patients receiving eculizumab. The meningococcal infection rate decreased over time; related mortality remained steady. The most commonly reported serious nonmeningococcal infections were pneumonia (11·8%); bacteraemia, sepsis and septic shock (11·1%); urinary tract infection (4·1%); staphylococcal infection (2·6%); and viral infection (2·5%). There were 434 reported cases of eculizumab exposure in pregnant women; of 260 cases with known outcomes, 70% resulted in live births. Reporting rates for solid tumours (≈0·6/100 PY) and haematological malignancies (≈0·74/100 PY) remained stable over time. No new safety signals affecting the eculizumab benefit‐risk profile were identified. Continued awareness and implementation of risk mitigation protocols are essential to minimise risk of meningococcal and other Neisseria infections in patients receiving eculizumab.
Keywords: paroxysmal nocturnal haemoglobinuria, atypical haemolytic uraemic syndrome, eculizumab, pharmacovigilance, safety
Paroxysmal nocturnal haemoglobinuria (PNH) and atypical haemolytic uraemic syndrome (aHUS) are rare, chronic, diseases that may be life‐threatening without treatment (Brodsky, 2014; Jang et al, 2016; Loschi et al, 2016; Fakhouri et al, 2017). Both diseases are caused by uncontrolled complement activation, resulting in intravascular haemolysis in PNH and systemic thrombotic microangiopathy (TMA) in aHUS (Noris & Remuzzi, 2009; Brodsky, 2014). Patients are at risk for significant complications, such as thrombosis, haemolytic anaemia, pulmonary hypertension and fatigue in PNH, and haemolytic anaemia and systemic organ impairment or failure in aHUS (Peffault de Latour et al, 2008; Noris & Remuzzi, 2009; Noris et al, 2010; Sallee et al, 2010; Muus et al, 2011; Fremeaux‐Bacchi et al, 2013; Azukaitis et al, 2014; Brodsky, 2014).
Eculizumab (Soliris®; Alexion Pharmaceuticals, Inc., Boston, MA, USA), is the first approved medication for patients with PNH (in 2007) or aHUS (in 2011) (https://www.medicines.org.uk/emc/product/362/smpc/print; http://alexion.com/Documents/Soliris_USPI.aspx), and has been recently approved for refractory generalised myasthenia gravis in Europe (European Medicines Agency, 2017a) and Japan (http://www.soliris.jp/common/pdf/tempu_bunsho.pdf), and generalised myasthenia gravis in the United States. The safety and efficacy of eculizumab therapy in PNH and aHUS were established in several prospective clinical trials, but long‐term post‐marketing safety monitoring in broader populations is essential for orphan drugs. In patients with PNH, treatment with eculizumab was associated with significant reductions in intravascular haemolysis, thromboembolism, transfusion requirements, anaemia, and fatigue, and improved quality of life (Hillmen et al, 2006, 2007, 2013; Brodsky et al, 2008). In patients with aHUS, eculizumab inhibited TMA, improved renal function and haematological outcomes, and improved quality of life (Legendre et al, 2013; Licht et al, 2015; Fakhouri et al, 2016; Greenbaum et al, 2016). Eculizumab therapy has also been associated with improved survival in both clinical settings (Kelly et al, 2011; Johnson et al, 2014).
As a first‐in‐class C5 inhibitor, the long‐term safety of eculizumab was unknown at the time of approval and, given the known increased risk of infection associated with complement deficiency (Figueroa & Densen, 1991), enhanced post‐marketing pharmacovigilance surveillance was established, including patient support programmes and post‐approval observational studies. The purpose was to collect data in a larger and broader patient population in order to ascertain the safety profile of eculizumab, particularly as it relates to rare but potentially clinically significant adverse events (AEs) that would not otherwise be observed in clinical studies. AEs of special interest and other safety outcomes were closely monitored as part of the post‐marketing assessment of eculizumab safety, including meningococcal infections, other serious infections, use in pregnancy and potential for developing malignancies. Since Neisseria meningitidis is primarily cleared by terminal complement components, it has been established that eculizumab‐treated patients are at increased risk for developing meningococcal infections (Figueroa & Densen, 1991; Rother et al, 2007). To minimise this risk, mitigation measures, including meningococcal vaccination, safety cards and educational materials for patients and physicians are implemented worldwide. Use of eculizumab in pregnant patients has been followed in post‐marketing surveillance because pregnancy was an exclusion criterion in the eculizumab registration trials. Historically, pregnancy has been discouraged in patients with PNH, and the management of PNH during pregnancy has been challenging because pregnant patients can have more severe intravascular haemolysis, and morbidity and mortality are higher among pregnant women with PNH versus those with PNH who are not pregnant; these risks continue to be high during the post‐partum period (Kelly et al, 2015). In terms of aHUS, data on pregnancy outcomes is very scarce but due to complement activation, patients have severe manifestations and poor outcomes (Huerta et al, 2018; Kozlovskaya et al, 2018). Assessment of potential risk of malignancy was also a priority even though anti‐tumour immunity is not expected to be affected in patients with late complement deficiency.
The objective of this analysis is to summarise 10 years of post‐marketing safety data collected from spontaneous and solicited reports of patients with PNH and aHUS who were treated with eculizumab. The results from this analysis are also considered in the context of AEs reported in the eculizumab clinical trials.
Methods
Data sources
Safety data regarding eculizumab use in the treatment of PNH and aHUS were collected and recorded in the Alexion pharmacovigilance database. Data were analysed for the period from 16 March 2007 (US Food and Drug Administration and Center for Drug Evaluation and Research, 2007) (the date of first marketing authorization) through 1 October 2016 (for PNH and aHUS patients only). From a pharmacovigilance perspective, an AE can be any unfavourable or unintended sign, symptom or disease temporally related with the use of a medicinal product, whether or not related to the medicinal product (European Medicines Agency, 2017b). AE reports were obtained in a solicited and unsolicited manner. Solicited reports were obtained from organised data collection methods (including, but not limited to, patient support programmes, disease management programmes, surveys of patients by health care providers, observational studies, sales representatives and medical science liaisons). Solicited reports included AEs identified through patient support programmes and from PNH and aHUS registries; solicited sources reported AEs regardless of whether there was causal association with eculizumab. Spontaneous (unsolicited) AEs were voluntarily reported by health care professionals, consumers, and competent authorities worldwide (e.g., US Food and Drug Administration, European Medicines Agency) or retrieved from published scientific literature using a defined search strategy and terms compiled and analysed by the Institute for Scientific and Technical Information, Vandoeuvre‐lès‐Nancy, France (Table SI). Data from Alexion‐sponsored clinical trials of eculizumab were excluded from this analysis.
Data collection
Safety data were structured by individual case safety reports (ICSRs) that included one or more AEs, not by individual patients. Due to confidentiality rules or limited information reported on patients, a given AE may have been reported multiple times from different sources with limited possibility for reconciliation and duplicate removal. Adverse event reports were coded according to preferred terms defined by the Medical Dictionary for Regulatory Activities (MedDRA V18.1).
Database inquiries
All post‐marketing ICSRs were searched using MedDRA preferred terms. ICSRs from solicited sources, where events were clearly considered unrelated to eculizumab treatment by both the reporter and Alexion, were excluded from the analysis. When no causality assessments were reported by a solicited source, events were considered possibly related by default and retained in the analysis.
Data analysis
Data were analysed using summary tables of cumulative AEs and serious AEs generated from the Alexion pharmacovigilance database in order to identify any emerging events, unusual trends or reporting frequencies. Duplicate reports were reconciled whenever possible. Cumulative post‐marketing exposure to eculizumab was calculated by adding the exposure in person‐months of new patients, discontinuing patients and continuing patients for each indication during the analysis period. Rates of AEs were calculated as number of events per 100 patient‐years (PY). Other quantitative data were reported using descriptive statistics.
Data sharing
Qualified academic investigators may request aggregate data contained in relevant sections of the PSUR 14.1 (http://alexion.com/research-development). Further details regarding data availability (including participant‐level clinical data), instructions for requesting information and our data disclosure policy will be available on the Alexion.com website (http://alexion.com/research-development).
Results
Eculizumab exposure and AE reports
The global cumulative post‐marketing exposure to eculizumab from 16 March 2007 to 1 October 2016, was 28 517·7 PY, including 21 015·7 PY in patients with PNH (20 511·3 PY in adults; 504·4 PY in children <18 years of age) and 7501·9 PY in patients with aHUS (5491·4 PY in adults; 2010·5 PY in children). Of the 283·3 reported cumulative AEs per 100 PY collected in the Alexion pharmacovigilance database, 71·1 per 100 PY (25·1%) were from spontaneous reports and 212·2 per 100 PY (74·9%) were from solicited reports. Overall, 36% were serious AEs; 43% of spontaneous AE reports and 33·6% of solicited AE reports were serious. Solicited reports originated mostly from patient support programmes (more than 80%) whose reporters were trained to report all AEs regardless of causality; such AEs would, therefore, include those that reflect disease manifestation as well as those that may be caused by eculizumab.
Most frequently reported AEs
The most frequently reported AEs, which largely reflect disease manifestation, are summarised in Tables 1, 2 and SII. AEs occurring at rates greater than nine events per 100 PY included decreased haemoglobin, fatigue, pyrexia and headache. Deaths occurring during treatment with eculizumab were reported. With the exception of deaths due to meningococcal infections (see below), there were no reports of fatal outcomes with a causal association to eculizumab treatment. Eculizumab was well tolerated and the majority of reported events associated with eculizumab were not serious. No new safety concerns emerged regarding eculizumab‐related infusion reactions (https://www.medicines.org.uk/emc/product/362/smpc/print; http://alexion.com/Documents/Soliris_USPI.aspx).
Table 1.
Most frequently reported AEs (by MedDRA preferred term) in patients with PNH
| MedDRA preferred term | Spontaneous number of AEs per 100 PY | Solicited number of AEs per 100 PY | Total | ||
|---|---|---|---|---|---|
| Serious | Nonserious | Serious | Nonserious | ||
| Haemoglobin decreased | 2·4 | 0·9 | 12·7 | 3·4 | 19·4 |
| Fatigue | 0·4 | 1·7 | 1·6 | 3·9 | 17·6 |
| Pyrexia | 1·6 | 0·9 | 3·9 | 3·3 | 9·7 |
| Headache | 0·6 | 1·0 | 1·4 | 6·2 | 9·2 |
| Haemolysis | 2·7 | 0·5 | 3·5 | 2·3 | 9·0 |
| Dyspnoea | 0·5 | 0·6 | 1·8 | 4·3 | 7·2 |
| Abdominal pain | 0·7 | 0·6 | 2·1 | 3·7 | 7·1 |
| Platelet count decreased | 0·6 | 0·5 | 3·7 | 2·2 | 7·1 |
| Transfusion | 0·6 | 0 | 5·0 | 0·2 | 5·8 |
Incidence rates are expressed as per 100 PY.
AEs, adverse events; MedDRA, Medical Dictionary for Regulatory Activities; PNH, paroxysmal nocturnal haemoglobinuria; PY, patient‐years.
Table 2.
Most frequently reported AEs (by MedDRA preferred term) in patients with aHUS
| MedDRA preferred term | Spontaneous number of AEs per 100 PY | Solicited number of AEs per 100 PY | Total | ||
|---|---|---|---|---|---|
| Serious | Nonserious | Serious | Nonserious | ||
| Haemoglobin decreased | 1·4 | 0·7 | 6·9 | 2·2 | 11·1 |
| Fatigue | 0·2 | 1·1 | 1·0 | 8·2 | 10·5 |
| Death | 2·1 | 0 | 6·5 | 0 | 8·6 |
| Pyrexia | 1·5 | 0·9 | 3·6 | 2·6 | 8·5 |
| Unevaluable event | 0·4 | 0 | 6·7 | 0·4 | 7·6 |
| Headache | 0·5 | 0·8 | 1·1 | 4·6 | 7·1 |
| Platelet count decreased | 0·7 | 0·6 | 3·1 | 1·9 | 6·4 |
| Vomiting | 0·6 | 0·4 | 1·9 | 2·6 | 5·5 |
| Dyspnoea | 0·6 | 0·6 | 2·1 | 2·1 | 5·4 |
| Nausea | 0·4 | 0·5 | 1·3 | 3·0 | 5·2 |
Incidence rates are expressed as per 100 PY.
AEs, adverse events; aHUS, atypical haemolytic uraemic syndrome; MedDRA, Medical Dictionary for Regulatory Activities; PY, patient‐years.
Adverse events of special interest
Meningococcal infections
Seventy‐six cases of meningococcal infection were reported, representing an overall rate of 0·25 reports per 100 PY (0·24 per 100 PY for PNH and 0·29 per 100 PY for aHUS). There were eight fatal meningococcal infection cases (0·03 per 100 PY), all of which occurred in patients with PNH. The rate of meningococcal infections tended to decrease over time, ranging from 0·57 per 100 PY in 2007 to 0·16 per 100 PY in 2016, with no obvious geographical predilection noted (data not shown) and serogroup B remained the most frequently reported meningococcal infection despite introduction of MenB vaccine in 2013. The mortality rate associated with meningococcal infections remained stable over time (Fig 1), with no death observed between 2012 and 2016 (Table 3). No obvious geographical predilection was noted after the introduction of MenB vaccination (data not shown). Demographics and characteristics of patients with meningococcal infection are summarised in Table 4. The majority of reported meningococcal infections occurred in patients aged 16–44 years old. Almost all cases occurred in patients with previous confirmed meningococcal vaccination (vaccination status was not reported in 5% of patients). Importantly, patients were not vaccinated against all serotypes of N. meningitidis because the availability of specific vaccines varied across regions.
Figure 1.
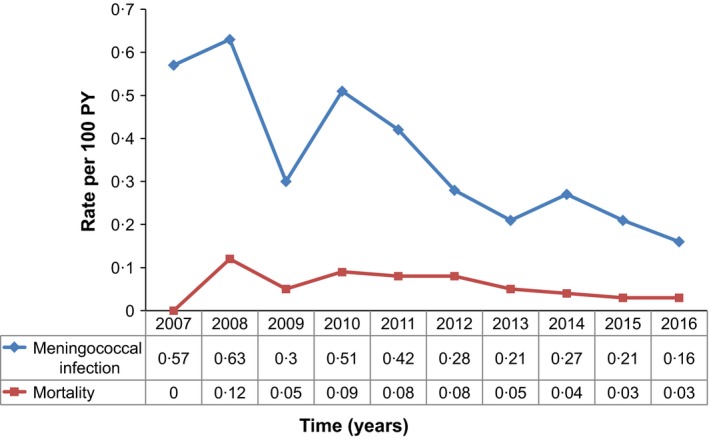
Rates of meningococcal infection and associated mortality per 100 PY from 2007 to 2016. Data are inclusive of both PNH and aHUS (indications approved in March 2007 and September 2011, respectively). Data expressed as cumulative rate per 100 PY. aHUS, atypical haemolytic uraemic syndrome; PNH, paroxysmal nocturnal haemoglobinuria; PY, patient‐years.
Table 3.
Overview of cumulative fatal cases of meningococcal infection.a
| Age (years) | Year of death | Serotype | Confirmed or suspected cause of death | Comments |
|---|---|---|---|---|
| 24 | 2008 | B | MS | Medical History: Budd‐Chiari syndrome, steroid‐use‐induced diabetes, multiple thromboembolic events/thrombosis. Concomitant medications: insulin, warfarin, prednisolone. Patient presented to GP on day 1 with flu symptoms and rash; patient received symptomatic medications and was sent home. Patient safety card was not shown, leading to delayed diagnosis and treatment. Taken to emergency room on day 3 with bluish colour, rash and fever; experienced cardiorespiratory arrest and expired on day 3 |
| 24 | 2010 | B | MB | Medical History: PNH 82% white cell count clone. Patient presented to local clinic with fever, chills, general weakness, myalgia and post‐neck pain on day 1, and refused hospital admission, which delayed appropriate antibiotic treatment. Patient returned and was admitted to intensive care unit on day 2. Condition worsened. On day 4 was intubated and went into coma. Expired on day 31 |
| 27 | 2010 | X | MS | Medical History: No specific risk factors except poor hygienic habits with cocaine abuse. Patient had vomiting on day 1 and presented to his GP with skin spots and cyanosis of ears on day 2 and received symptomatic medications. Taken to emergency room on day 2, was misdiagnosed as anxiety crisis with tachypnea. Experienced cardiac arrest and expired on day 2. Patient safety card was not shown leading to delayed diagnosis and treatment |
| 33 | 2011 | C | MS | Medical History: Minimal information reported. Patient presented to emergency room on day 1 with vomiting, diarrhoea, headache, fever. Diagnosed as gastritis. Expired on day 2 |
| 40 | 2012 | Unknownb | MS | Medical History: Recurrent thrombotic events, no concomitant medications reported. Patient initially experienced malaise and myalgia on day 1 and rapidly progressed to fever, palpable purpura on limbs and severe circulatory shock. Expired on day 1 |
| 22 | 2012 | Unknown | MS | Medical History: Minimal information reported. Patient experienced headache, abdominal pain and fever on day 1 and was admitted to intensive care unit. Antibiotic treatment initiation was delayed for an unknown reason. Patient developed meningococcal sepsis on day 2 and later expired |
| 25 | 2016 | Unknown | ME | Medical History: Cytological abnormality, thromboembolic complication. Patient presented to his GP on day 1 with febrile gastroenteritis for which he received symptomatic medications and was sent home. Patient safety card was not shown. Patient was found dead at home on day 2. However, the diagnosis of ‘suspected meningoencephalitis’ has never been confirmed |
| 29 | 2016 | Y | MS |
Medical History: None reported Twenty days after delivery of a healthy baby, patient experienced fever, chills, hand numbness, sweating, nausea and difficulty drinking water, and presented to hospital (day 1), for which she received symptomatic medication. On day 2, patient experienced purpura and hypotension, diagnosed as septic shock with intravascular coagulation (Neisseria meningitidis and endotoxin), and expired |
Table summarises basic demographic information, a summary narrative of symptom manifestation, treatment intervention, and circumstances of outcome.
GP, general practitioner; MB, meningococcal bacteraemia; ME, meningococcal encephalitis; MS, meningococcal sepsis; PNH, paroxysmal nocturnal haemoglobinuria.
All were vaccinated, spontaneously reported post‐marketing cases, and all occurred in patients with PNH.
Negative for serotypes A, B, C.
Table 4.
Demographics, vaccination status, and identified serotype among patients with meningococcal infection.a
| Patient characteristic | PNH (n = 52) | aHUS (n = 24) | Total (n = 76) |
|---|---|---|---|
| Age group, years, n (%) | |||
| 0–5 | 0 | 2 (8·3) | 2 (2·6) |
| 6–15 | 2 (3·8) | 4 (16·7) | 6 (7·9) |
| 16–25 | 23 (44·2) | 11 (45·8) | 34 (44·7) |
| 26–44 | 18 (34·6) | 5 (20·8) | 23 (30·3) |
| 45–65 | 5 (9·6) | 0 | 5 (6·6) |
| >65 | 1 (1·9) | 0 | 1 (1·3) |
| Not reported | 3 (5·8) | 2 (8·3) | 5 (6·6) |
| Sex | |||
| Female | 29 (55·8) | 14 (58·3) | 43 (56·6) |
| Male | 23 (44·2) | 9 (37·5) | 32 (42·1) |
| Not reported | 0 | 1 (4·2) | 1 (1·3) |
| Time to onset of meningococcal infection after first dose of eculizumab (days), median (range) | 272 (4–2247)a | 502 (43–1481)b | – |
| Vaccination status, n (%) | |||
| All confirmed vaccinationsa | 51 (98·1) | 21 (87·5) | 72 (94·7) |
| Not reported | 1 (1·9) | 3 (12·5) | 4 (5·2) |
| Identified serogroup, n (%) | 30 (57·7) | 15 (62·5) | 45 (59·2) |
| B | 13 (43·3) | 6 (40·0) | 19 (42·2) |
| Y | 6 (20·0) | 3 (20·0) | 9 (20·0) |
| C | 7 (23·3) | 1 (6·7) | 8 (17·8) |
| W | 0 | 4 (26·7) | 4 (8·9) |
| E | 0 | 1 (6·7) | 1 (2·2) |
| X | 1 (3·3) | 0 | 1 (2·2) |
| Z | 1 (3·3) | 0 | 1 (2·2) |
| Noncapsulated apathogenic | 1 (3·3) | 0 | 1 (2·2) |
| Negative in serotypes A, B, C, W135, Y | 1 (3·3) | 0 | 1 (2·2) |
| Unknown serotype, n (%) | 22 (42·3) | 9 (37·5) | 31 (40·8) |
Data expressed as number (percentage) by age group, sex, and vaccination status.
“Unknown” refers to unreported data.
aHUS, atypical haemolytic uraemic syndrome; PNH, paroxysmal nocturnal haemoglobinuria.
Type of vaccine may be unknown; only 34 cases had sufficient information to calculate the median value.
Only 11 cases had sufficient information to calculate the median value. Patients were not vaccinated against all Neisseria meningitidis serogroups; and vaccination is not 100% effective.
Frequencies and outcomes of meningococcal‐related AEs are summarised in Table 5. Sepsis was the most frequently reported presentation of meningococcal infection. In 39 cases (50·8%), patients fully recovered or were improving at the time of report. This includes four patients who recovered with sequelae. Outcomes were unknown or not yet reported in 29 cases (38·1%).
Table 5.
Type of meningococcal disease by MedDRA preferred term and event outcomes
| PNH (n = 61), n (%) | aHUS (n = 24), n (%) | Totala (n = 85), n (%) | |
|---|---|---|---|
| MedDRA preferred terms | |||
| Meningococcal sepsis | 30 (49·2) | 7 (29·2) | 37 (43·5) |
| Meningococcal infection | 13 (21·3) | 8 (33·4) | 21 (24·7) |
| Meningitis meningococcal | 13 (21·3) | 5 (20·8) | 18 (21·2) |
| Meningococcal bacteraemia | 4 (6·6) | 4 (16·7) | 8 (9·4) |
| Encephalitis meningococcal | 1 (1·6) | 0 | 1 (1·2) |
| Outcomes | |||
| Recovered | 19 (36·5) | 10 (41·7) | 29 (38·2) |
| Fatalb | 8 (15·4) | 0 | 8 (10·5) |
| Improvedc | 5 (9·6) | 1 (4·2) | 6 (7·9) |
| Recovered with sequelaed | 3 (5·8) | 1 (4·2) | 4 (4·7) |
| Ongoing | 2 (3·8) | 1 (4·2) | 3 (3·9) |
| Unknown | 15 (28·8) | 11 (45·8) | 26 (34·2) |
Data expressed as percentage for each reported MedDRA term and corresponding outcomes.
Meningococcal infection: generic term, with no location specified.
aHUS, atypical haemolytic uraemic syndrome; MedDRA, Medical Dictionary for Regulatory Activities; PNH, paroxysmal nocturnal haemoglobinuria.
There may be multiple preferred terms per case.
Fatal outcomes occurred with equal distribution worldwide. Main cause of death due to delayed diagnosis.
Not fully recovered.
Sequelae: 1 patient experienced amputation of 7 of 10 distal fingers, 1 patient experienced bilateral forefoot amputation, 1 patient experienced thrombosis of retinal vein and blindness, and 1 patient experienced weakness (which was a pre‐existing condition).
The eight patients (10·5%) with fatal outcomes were 22–40 years of age (Table 3). All eight had received meningococcal vaccination, although not against all serotypes.
Other serious infections
Reported rates of serious, nonmeningococcal infections are provided in Table 6. No age‐related trends were observed within the subgroups with PNH or aHUS. Although there was a higher rate of serious nonmeningococcal infection observed in adults aged 18–65 years, exposure was also higher in this age group compared with paediatric patients. Importantly, this pattern of infection rate corresponds to the age range of patients treated with eculizumab (Tables SIIIA,B).
Table 6.
Overall serious infections in patients treated with eculizumab
| Infections | PNH | aHUS | Total |
|---|---|---|---|
| Rate, per 100 PY | 5·8 | 13·9 | 7·9 |
| Age, mean (range), years | 51·5 (7–94) | 34·2 (0·04–87) | 44·5 (0·04‐94) |
| <18 years, % | 1·8 | 18·9 | 9·7 |
| ≥18 years, % | 86·1 | 51·2 | 70·0 |
| Unknown, % | 12·1 | 29·9 | 20·3 |
| Sex, % | |||
| Female | 51·7 | 58·8 | 55·0 |
| Male | 46·9 | 35·9 | 41·8 |
| Unknown | 1·4 | 5·4 | 3·2 |
| As reported percentage of serious infections by causal organism types | |||
| Causal organism NOS, % | 62·8 | 61·4 | 62·2 |
| All bacterial infections among infections (%) | 22·8 | 19·2 | 21·1 |
| Neisseria a % bacterial infections | 13·3 | 7·2 | 10·8 |
| Enterococcus or E. coli % bacterial infections | 7·6 | 15·1 | 10·8 |
| Streptococcus % bacterial infections | 6·7 | 4·8 | 5·9 |
| Pseudomonas % bacterial infections | 6·5 | 6·9 | 6·7 |
| Klebsiella % bacterial infections | 2·5 | 4·5 | 3·3 |
| Tuberculosis % bacterial infections | 2·2 | 1·9 | 2·2 |
| Haemophilus % bacterial infections | 0·4 | 0·5 | 0·3 |
| Other (%) bacterial infections | 60·8 | 59·1 | 60·0 |
| All viral infections among infections (%) | 11·2 | 13·8 | 12·4 |
| Influenza % viral infections | 21·7 | 26·9 | 24·3 |
| Herpes zoster % viral infections | 11·2 | 12·5 | 11·9 |
| Cytomegalovirus % viral infections | 2·7 | 16·9 | 10·0 |
| BK or JC virus % viral infections | 0 | 6·9 | 1·3 |
| Other % | 64·4 | 36·8 | 52·5 |
| All fungal infections among infections (%) | 2·4 | 4·7 | 3·5 |
| Aspergillus % fungal infections | 14·3 | 32·1 | 24·8 |
| Candida % fungal infections | 8·9 | 11·8 | 10·7 |
| Other % fungal infections | 76·8 | 57·0 | 64·5 |
| All sepsis among infections (%) | 11·7 | 11·9 | 11·8 |
Total incidence rates are expressed as per 100 PY. Breakdown of incidence rates within subgroups are expressed as a percentage of the total incidence rate by age group, sex, or for each type of serious infections.
aHUS, atypical haemolytic uraemic syndrome; NOS, not otherwise specified (causative infective agent was not reported); PNH, paroxysmal nocturnal haemoglobinuria; PY, patient‐years.
Including 1·7% of disseminated gonococcal infections.
Among patients experiencing serious infections, the most commonly reported serious nonmeningococcal infections were pneumonia (11·8%); bacteraemia, sepsis and septic shock (11·1%); urinary tract infection (4·1%); staphylococcal infection (2·6%); and viral infection (not otherwise specified; 2·5%). All patients with serious, nonmeningococcal infections had severe underlying conditions, comorbidities or treatments that could have compromised their immune systems.
Neisseria infections other than N. meningitidis infections also have been reported, including disseminated gonococcal infections (1·7%) and sepsis with other Neisseria species such as Neisseria cinerea, subflava/sicca, or elongata (1·1%).
The overall reporting rate for Aspergillus infection was 0·13 cases per 100 PY (0·39 per 100 PY in aHUS; 0·04 per 100 PY in PNH). All patients had severe and multiple confounding factors, such as recent transplant and immunosuppressive treatment. Sixty‐three percent of the reported cases were fatal.
Outcomes in pregnancy
Eculizumab exposure was reported in a total of 434 women during their pregnancy; 335 patients (77%) with PNH and 99 patients (23%) with aHUS (Table 7). Seventy percent of pregnancies (72% in PNH and 59% in aHUS) with reported outcomes resulted in live births; abortion was induced in 7·8% of pregnancies in PNH and in 20·4% in aHUS. One case of serious infection was reported in a neonate born to a mother treated with eculizumab. However, this infection occurred 12 days post‐delivery and was considered by the treating physician as unlikely to be related to eculizumab. Eculizumab was given as rescue therapy in a patient who was 4 months pregnant experiencing onset of severe aHUS‐related neurological complications and had already received plasma exchanges. She experienced a hospital‐acquired vancomycin‐resistant enterococcus infection. This event was considered unlikely to be related to eculizumab by the treating physician, given the severe underlying conditions with plasma exchanges and catheterization, as well as the high virulence and pathogenicity of nosocomial vancomycin‐resistant enterococcal infections, the most commonly acquired type of hospital infection.
Table 7.
Pregnancy outcomes in women treated with eculizumab
| Reported outcomes | PNH (n = 206), n (%) | aHUS (n = 54), n (%) | Total (n = 260), n (%) |
|---|---|---|---|
| Live birtha | 150 (72·8) | 32 (59·3) | 182 (70·0) |
| Miscarriage or spontaneous abortion | 33 (16·0) | 8 (14·8) | 41 (15·8) |
| Induced abortionb | 16 (7·8) | 11 (20·4) | 27(10·4) |
| Stillbirth or fetal deathc | 6 (2·9) | 3 (5·6) | 9 (3·5) |
| Maternal deathd | 1 (0·5) | 0 | 1 (0·4) |
| Unreported outcomes | PNH ( n = 129), n (%) | aHUS ( n = 45), n (%) | Total ( n = 174), n (%) |
| Pregnant at time of reportinge | 98 (76·0) | 38 (84·4) | 136 (78·2) |
| Lost to follow‐upc | 31 (24·0) | 7 (15·6) | 38 (21·8) |
Table summarises percentage of reported and unreported pregnancy outcomes for each indication and in total.
aHUS, atypical haemolytic uraemic syndrome; PNH, paroxysmal nocturnal haemoglobinuria.
Sixty‐five live births by C‐section.
Abortion was induced for medical reasons (including 1 ectopic pregnancy) or was the patient's decision.
Including 1 ectopic pregnancy.
Patient died of enterococcal infection.
Includes 4 cases where the pregnancy was not confirmed.
Outcomes in breastfeeding mothers
There were 31 patients reported to have breastfed while receiving eculizumab; 20 patients with PNH and 11 patients with aHUS. One patient experienced a painful breast lump, mastitis, sepsis and fever. The remaining 30 patients (and neonates) did not experience any AEs associated with breastfeeding.
Malignancies
Malignancies were reported in patients with PNH (2·6 reports per 100 PY) and aHUS (3·1 reports per 100 PY) (Table 8). The mean time to onset of malignancy after the initial dose of eculizumab was 2·2 years in the 16% of patients with PNH for whom data were available, versus 1·0 years in the 12·5% of patients with aHUS with available data. As expected, the reported haematological pathologies in patients with PNH were higher than in patients with aHUS. The reporting rate of approximately 0·74 per 100 PY remained stable over time. With respect to solid tumours, skin neoplasms were more frequently reported in patients with PNH (15% of solid tumours) than in those with aHUS (5% of solid tumours). Otherwise, no trends were observed regarding specific types of solid tumours. The reporting rate for solid tumours remained stable over time at approximately 0·6 per 100 PY. Reported rates of malignancies stratified by age and sex are summarised in Tables SIVA,B.
Table 8.
Solid tumours and haematological malignancies in patients treated with eculizumab
| PNH | aHUS | Total | |
|---|---|---|---|
| Rate, per 100 PY | 2·6 | 3·1 | 2·7 |
| Age, mean (range), years | 60·6 (9–93) | 51·6 (3–84) | 51·9 (3–93) |
| <18 years, % | 0·9 | 7·4 | 2·8 |
| ≥18 years, % | 84·7 | 59·1 | 77·1 |
| Unknown, % | 14·4 | 33·5 | 20·1 |
| Sex, % | |||
| Female | 46·1 | 53·0 | 48·1 |
| Male | 52·1 | 42·2 | 49·2 |
| Unknown | 1·8 | 4·8 | 2·7 |
| As reported percentage of malignancies by tumour types | |||
| Haematological tumours, % of total malignancies | 53·0a | 22·7 | 43·8 |
| Leukaemia, % of haematological tumours | 90·0 | 40·3 | 82·2 |
| Lymphomas, % of haematological tumours | 6·2 | 35·5 | 10·7 |
| Other NOS, % of haematological tumours | 3·8 | 24·2 | 7·1 |
| Solid tumours, % of total malignancies | 47·0 | 77·3 | 72·8 |
| Gastrointestinal, % of solid tumours | 17·0 | 18·0 | 15·5 |
| Skin, % of solid tumours | 15·2b | 5·2b | 10·4 |
| Reproductive, % of solid tumours | 12·2 | 9·9 | 10·1 |
| Breast, % of solid tumours | 9·2 | 8·5 | 7·9 |
| Other, % of solid tumours (e.g., respiratory, hepatobiliary, CNS, renal; all <5% each) | 46·4 | 58·4 | 56·1 |
Total incidence rates are expressed as per 100 PY. Breakdown of incidence rates within subgroups are expressed as a percentage of the total incidence rate by age group, sex, or for each tumour type.
aHUS, atypical haemolytic uraemic syndrome; CNS, central nervous system; NOS, not otherwise specified; PNH, paroxysmal nocturnal haemoglobinuria; PY, patient‐years.
Of all reported haematological tumours occurring in patients with PNH, 64·5% were myelodysplastic syndromes.
Among skin tumours, 25% were melanomas.
Hepatic dysfunction
Several patients with underlying hepatic dysfunction who were treated with eculizumab, including patients with PNH who had Budd‐Chiari syndrome, cirrhosis or other severe hepatic conditions, were represented in the database. Overall, no clinically relevant differences were observed in the frequency or type of AEs associated with eculizumab treatment in patients with or without a history of liver dysfunction.
Discussion
This report is the largest compilation of pharmacovigilance data on eculizumab exposure to date, including 10 years of post‐marketing surveillance. This analysis reflects 28 518 PY of global cumulative exposure to eculizumab (21 016 PY in PNH and 7502 PY in aHUS) compared with 711 PY of cumulative exposure across clinical trials (Hillmen et al, 2006, 2013; Brodsky et al, 2008; Kanakura et al, 2011; Legendre et al, 2013; Licht et al, 2015; Fakhouri et al, 2016; Greenbaum et al, 2016).
This study has enabled the analysis of long‐term trends in reported AEs, including AEs of special interest, in patients receiving eculizumab. Meningococcal infections are of particular interest because there is a well‐established and predictable risk of infection from Neisseria species that is directly related to the mechanism of action of eculizumab (Rother et al, 2007; McNamara et al, 2017). Overall, the cumulative reporting rate of meningococcal infection in eculizumab‐treated patients tended to decline over time following the initial approval of eculizumab, then remained relatively stable over the most recent 5 years, at approximately 0·25 per 100 PY. The distribution of meningococcal infections by age (16‐ to 25‐year‐olds have a higher infection rate) is also similar to that reported in the general population (Atkinson et al, 2016; Centers for Disease Control and Prevention, 2017). These findings are also consistent with those reported in clinical studies (0·83 events per 100 PY) (Drug Safety and Risk Management Advisory Committee, 2014). Compared with the general population, the incidence rates for meningococcal infections are 8000‐ to 10 000‐fold higher in patients with late complement component deficiency (Figueroa & Densen, 1991; Tedesco, 2008), and ≈1000‐ to 2000‐fold higher in patients receiving eculizumab under the risk mitigation measures (McNamara et al, 2017). It should be noted that those with inherited complement deficiency are at risk from birth, whereas those treated with eculizumab are not at risk before they start complement‐inhibitor therapy. These findings suggest that the current mitigation measures are generally effective. While ≈95% of patients with meningococcal infections were reported to have received vaccinations, patients were not vaccinated against all serotypes. Of note, the vaccine against serogroup B disease was not approved in the European Union until 2013 (European Medicines Agency, 2013), and is not available worldwide. Furthermore, ex vivo data have shown that vaccination may not fully suppress the risk of meningococcal infection due to inhibition of the opsonophagocytic activity and complement‐dependent cytotoxicity required for eradication of Neisseria (Sprong et al, 2003; Konar & Granoff, 2017).
In this analysis, eight deaths occurred in PNH patients with meningococcal infections, largely due to a delay in diagnosis and/or treatment of infection. No deaths due to meningococcal infections were observed in aHUS patients. Importantly, the fatality rate in this analysis (10·5%) was similar to that reported in the general population (8·6%) (Centers for Disease Control and Prevention, 2016). These findings underscore the need for heightened awareness among patients and physicians regarding the risk of meningococcal infection. Information about risk mitigation measures can also be found in patient education and provider certification materials from the Risk Evaluation and Mitigation Strategy programme for eculizumab (www.solirisrems.com). Recommendations from the US Advisory Committee on Immunization Practices encourage vaccination against A, C, W, Y and B serotypes for patients receiving eculizumab (McNamara et al, 2017; O'Leary & Kimberlin, 2017). However, as meningococcal vaccination may not prevent all cases of meningococcal infection in eculizumab‐treated patients (Konar et al, 2016; Konar & Granoff, 2017; McNamara et al, 2017; O'Leary & Kimberlin, 2017), the Centers for Disease Control and Prevention suggests that consideration be given to appropriate use of antibiotic prophylaxis; all patients should be monitored for early signs of meningococcal infection.
The susceptibility to develop serious infections with Neisseria species other than meningococcus was confirmed. Infections with organisms considered to be non‐pathogenic in immunocompetent patients, such as Neisseria sicca/subflava, were observed. Most of the reported gonococcal infections (89%) presented as disseminated gonococcal infections, which are rare in the general population (<1%). This severity might be related to eculizumab treatment that prevents efficient serum bactericidal activity; however, other reasons, such as the underlying pathophysiology of the disease and concomitant medications may also be contributing factors.
Rates of serious nonmeningococcal infections reported herein are consistent with those reported in the clinical trials of eculizumab in PNH (Hillmen et al, 2006, 2013; Brodsky et al, 2008) and aHUS (Legendre et al, 2013; Licht et al, 2015; Fakhouri et al, 2016; Greenbaum et al, 2016). In the only double‐blind, randomised, placebo‐controlled trial of eculizumab in 87 patients with PNH (Hillmen et al, 2006), serious nonmeningococcal infections were reported in similar proportions of eculizumab‐treated and untreated patients with PNH (2% vs. 6%, respectively). Outside of the clinical trial programme, severe infections have been reported in up to 18% (Nishimura et al, 2004) and were identified as the cause of death in 25–40% of mortalities reported in untreated patients with PNH (Jang et al, 2016; Yu et al, 2016). Infections have been identified as precipitating events in patients with aHUS (Noris et al, 2010; Schifferli et al, 2010; Geerdink et al, 2012; Fremeaux‐Bacchi et al, 2013; Campistol et al, 2015); it is important to note that immunosuppression may play a role in these infections because many aHUS patients receive dialysis or renal transplantation (Noris et al, 2010; Schifferli et al, 2010; Geerdink et al, 2012; Fremeaux‐Bacchi et al, 2013; Lok & Foley, 2013; Campistol et al, 2015). Among patients enrolled in the Alexion‐sponsored global aHUS Registry who had no history of treatment with eculizumab, streptococcal pneumonia and influenza were observed in 4% of paediatric and 1% of adult patients (annual interim aHUS Registry analysis – submitted to health authorities along with Periodic Benefit Risk Evaluation Report; unpublished observations). Deaths due to sepsis and Staphylococcus aureus septicaemia have been reported in rare instances in untreated patients with aHUS (Sellier‐Leclerc et al, 2007; Ardissino et al, 2016). The reporting rate for Aspergillus infections was 10‐fold higher in patients with aHUS compared with patients with PNH, as expected in immunosuppressed populations and the comorbidities associated with each disease. All patients with an Aspergillus infection had multiple confounding factors, such as solid organ (renal) transplant or bone marrow transplant, and were receiving immunosuppressive treatment (e.g., high‐dose steroids, mycophenolate mofetil, ciclosporin, tacrolimus). Graft‐versus‐host disease, aplastic anaemia, myelodysplastic syndrome (MDS) and diabetes were also reported in some patients. Together, these reports suggest that the above associated diseases and concomitant treatments that lead to an immunosuppressed state may contribute to the occurrence of serious nonmeningococcal infections in the current analysis, and do not represent a new safety signal for eculizumab (Rother et al, 2007).
Exposure to eculizumab during pregnancy was associated with a comparable rate of live births and a low rate of maternal complications in contrast to reports of elevated maternal mortality rates observed among patients with PNH not receiving eculizumab (Kelly et al, 2015). In aHUS, use of eculizumab in pregnancy and post‐partum is associated with good maternal and fetal outcomes, including normalization of haematological outcomes and renal function (Ardissino et al, 2013; Delmas et al, 2013; Zschiedrich et al, 2013; Canigral et al, 2014; Mussoni et al, 2014; De Sousa Amorim et al, 2015; Demir et al, 2016; Saad et al, 2016; Servais et al, 2016; Tsai & Kuo, 2016; Andries et al, 2017; Bruel et al, 2017; Chua et al, 2017; Gately et al, 2017). The rate of congenital malformation reported in neonates born to mothers treated with eculizumab lies within the range of that reported in the general population (UK Teratology Information Service, 2017). In addition, the overall rate of miscarriage in this study (15·8%) was similar to the rate of pregnancy loss observed in a population of more than 20 000 women in the United States from 1990 to 2011 (19·7%) (Rossen et al, 2018). Thus, the use of eculizumab in pregnancy in patients with PNH or aHUS may be appropriate and safer than discontinuing or not initiating eculizumab treatment.
No teratogenic effects in fetuses have been observed thus far (UK Teratology Information Service, 2017). Teratogenicity is unlikely because eculizumab does not bind Fc receptors (Rother et al, 2007) and has low binding affinity for the neonatal Fc receptor (FcRn), which is a prerequisite for transport of immunoglobulin G antibodies across the maternofetal barrier (Hallstensen et al, 2015). Eculizumab does not accumulate in fetal blood and does not influence fetal/neonatal complement activity (Hallstensen et al, 2015; Servais et al, 2016). Trans‐mammary transportation of antibodies is also an active mechanism requiring binding to FcRn and, therefore, eculizumab is not expected to be found in breast milk (Cui et al, 2014; Kelly et al, 2015). Based on the current limited data and literature, continued treatment appears unlikely to cause adverse effects in infants (Kelly et al, 2015).
The reporting rate for solid and haematological tumours remained stable over the 10‐year assessment period. Importantly, patients with PNH and aHUS may be predisposed to developing malignancies. For example, patients with PNH may also have concurrent bone marrow dysfunction, placing them at increased risk of developing acute leukaemia (Socie et al, 1993; Scheinberg et al, 2014). Thus, haematological malignancy in the setting of PNH is more likely to be a manifestation of underlying abnormalities of haematopoietic function than an effect of eculizumab. Consistent with a potential association between malignancy and disease factors, the current analysis showed diversity in tumour types and age at onset of malignancies for PNH and aHUS, respectively. Particularly low rates of malignancy were reported in paediatric patients with PNH and aHUS, consistent with the rarity of cancer in this age group. Published information on background incidences of malignancies in patients with PNH or aHUS, regardless of treatment, is limited. However, some analyses comparing cohorts of treated and untreated patients showed no difference in cumulative incidence of clonal evolution to MDS or acute myeloid leukaemia (AML) (Loschi et al, 2016). In addition, in a systematic review of published studies in patients with PNH (N = 1665), 5·1% progressed to MDS or AML, and malignancy was the cause of death in 11·9% (Yu et al, 2016). Similar to patients with PNH, patients with aHUS who undergo transplantation or who otherwise receive long‐term immunosuppressive treatment are at increased risk of malignancy, which is unlikely to be related to eculizumab (Villeneuve et al, 2007).
Only 25·1% of AE reports in the current analysis were spontaneous, which implies a higher likelihood of perceived causality by the reporters than in solicited reports. Therefore, due to the solicited nature of most reporting sources, it is likely that many, if not the majority, of the most frequently reported AEs are signs and symptoms of the underlying disease or are confounded by the patients’ other conditions. For example, haemolysis, low haemoglobin and fatigue were among the most frequently reported AEs in patients with PNH and aHUS, and these AEs are similar to common symptoms of PNH and aHUS (Sellier‐Leclerc et al, 2007; Peffault de Latour et al, 2008; Noris & Remuzzi, 2009; Brodsky, 2014). There were no observed meaningful differences in the frequency or type of AEs associated with eculizumab treatment in patients with or without a history of liver dysfunction or history of renal impairment.
There are several limitations of this analysis. First, the AE data were analysed by the frequency of each reported event regardless of causality, and not by patient. Patient identifiers, comparators and denominators were not available for the calculation of AE rates, and it was not possible to perform between‐group statistical comparisons. Second, data in the Alexion pharmacovigilance database are structured by ICSRs, some of which may have contained incomplete information. Third, despite careful checks for duplication of AE information, different sources may have reported some of the same events, and this analysis probably overestimates AE rates. Fourth, although AEs may be underreported in post‐marketing surveillance (Alatawi & Hansen, 2017), this attribute may be mitigated by the effectiveness of patient support programmes and close interactions between physicians and patients. Finally, it was not possible to compare reports by age, sex, concomitant medications or treatment with eculizumab or to perform longitudinal follow‐up of individual patients. Accordingly, pharmacovigilance data are useful for the acquisition of trends or safety signals in treated patients but do not allow for meaningful comparison of incidence rates for malignancies over time.
Conclusions
This analysis is the largest safety data set to date, representing more than 10 years of post‐marketing pharmacovigilance surveillance of eculizumab for the treatment of PNH and aHUS. The overall safety profile of eculizumab is consistent with that reported from clinical trials. No new safety signals affecting the benefit‐risk profile of eculizumab were detected. The use of eculizumab in pregnancy appears to have a favourable benefit‐risk profile. The major risk of eculizumab treatment remains the susceptibility to neisserial infections, most importantly meningococcal infections. Clinicians should rely on careful assessment of the potential benefit and risk of eculizumab for each patient and the implementation of appropriate monitoring to effectively mitigate the risk of meningococcal infection.
Authorship contribution
MPCT and AC had full access to all data in the Alexion pharmacovigilance database, and assume responsibility and accountability for data integrity and accuracy; GS, MPCT, JLM, AC, CLB and PH were responsible for the study concept and design; GS, MPCT, JLM, AC, CLB, CG, AM, PH, JVW and HH were responsible for the acquisition, analysis, and/or interpretation of data and provided critical revision of the manuscript for important intellectual content; GS, MPCT and JLM drafted the manuscript; MPCT and AC were responsible for the statistical analysis; GS, MPCT, CLB and JLM supervised the project. All authors have reviewed and approved the manuscript.
Conflict of interest
GS received speaker fees from, and is a consultant for, Alexion Pharmaceuticals, Inc. MPCT is an employee and shareholder of Alexion Europe SAS. JLM and CLB are former employees and current stockholders of Alexion Pharmaceuticals, Inc. AC and AM are employees and stockholders of Alexion Pharmaceuticals, Inc. CG is an employee and shareholder of Alexion Pharma GmbH. PH, JVW and HH received speaker fees and travel reimbursement, and are consultants for Alexion Pharmaceuticals, Inc.
Supporting information
Table SI. Databases, search concepts, and search strategy.
Table SII. System organ class categories with the most frequently reported AEs, by MedDRA preferred terms.
Table SIII. Demographic characteristics of patients with (A) PNH and (B) aHUS who had serious infections.
Table SIV. Demographic characteristics of patients with (A) PNH and (B) aHUS who had malignancy.
Acknowledgements
The authors acknowledge Peloton Advantage, LLC, which provided editorial and medical writing support by Michael D. Morren, RPh, MBA, with funding from Alexion Pharmaceuticals, Inc. Editorial support was also provided by Åsa Lommelé, PhD (Alexion Pharma GmbH) and Kenneth Pomerantz, PhD (Alexion Pharmaceuticals, Inc.). This study was supported by Alexion Pharmaceuticals, Inc. (US).
References
- Alatawi, Y.M. & Hansen, R.A. (2017) Empirical estimation of under‐reporting in the U.S. Food and Drug Administration Adverse Event Reporting System (FAERS). Expert Opinion on Drug Safety, 16, 761–767. [DOI] [PubMed] [Google Scholar]
- Andries, G. , Karass, M. , Yandrapalli, S. , Linder, K. , Liu, D. , Nelson, J. , Pawar, R. & Chugh, S. (2017) Atypical hemolytic uremic syndrome in first trimester pregnancy successfully treated with eculizumab. Experimental Hematology & Oncology, 6, 4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ardissino, G. , Wally Ossola, M. , Baffero, G.M. , Rigotti, A. & Cugno, M. (2013) Eculizumab for atypical hemolytic uremic syndrome in pregnancy. Obstetrics and Gynecology, 122, 487–489. [DOI] [PubMed] [Google Scholar]
- Ardissino, G. , Salardi, S. , Colombo, E. , Testa, S. , Borsa‐Ghiringhelli, N. , Paglialonga, F. , Paracchini, V. , Tel, F. , Possenti, I. , Belingheri, M. , Civitillo, C.F. , Sardini, S. , Ceruti, R. , Baldioli, C. , Tommasi, P. , Parola, L. , Russo, F. & Tedeschi, S. (2016) Epidemiology of haemolytic uremic syndrome in children. Data from the North Italian HUS network. European Journal of Pediatrics, 175, 465–473. [DOI] [PubMed] [Google Scholar]
- Atkinson, B. , Gandhi, A. & Balmer, P. (2016) History of meningococcal outbreaks in the United States: implications for vaccination and disease prevention. Pharmacotherapy, 36, 880–892. [DOI] [PubMed] [Google Scholar]
- Azukaitis, K. , Loirat, C. , Malina, M. , Adomaitiene, I. & Jankauskiene, A. (2014) Macrovascular involvement in a child with atypical hemolytic uremic syndrome. Pediatric Nephrology, 29, 1273–1277. [DOI] [PubMed] [Google Scholar]
- Brodsky, R.A. (2014) Paroxysmal nocturnal hemoglobinuria. Blood, 124, 2804–2811. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brodsky, R.A. , Young, N.S. , Antonioli, E. , Risitano, A.M. , Schrezenmeier, H. , Schubert, J. , Gaya, A. , Coyle, L. , de Castro, C. , Fu, C.L. , Maciejewski, J.P. , Bessler, M. , Kroon, H.A. , Rother, R.P. & Hillmen, P. (2008) Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria. Blood, 111, 1840–1847. [DOI] [PubMed] [Google Scholar]
- Bruel, A. , Kavanagh, D. , Noris, M. , Delmas, Y. , Wong, E.K.S. , Bresin, E. , Provot, F. , Brocklebank, V. , Mele, C. , Remuzzi, G. , Loirat, C. , Fremeaux‐Bacchi, V. & Fakhouri, F. (2017) Hemolytic uremic syndrome in pregnancy and postpartum. Clinical Journal of the American Society of Nephrology, 12, 1237–1247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Campistol, J.M. , Arias, M. , Ariceta, G. , Blasco, M. , Espinosa, L. , Espinosa, M. , Grinyo, J.M. , Macia, M. , Mendizabal, S. , Praga, M. , Roman, E. , Torra, R. , Valdes, F. , Vilalta, R. & Rodriguez de Cordoba, S. (2015) An update for atypical haemolytic uraemic syndrome: diagnosis and treatment. A consensus document. Nefrologia, 35, 421–447. [DOI] [PubMed] [Google Scholar]
- Canigral, C. , Moscardo, F. , Castro, C. , Pajares, A. , Lancharro, A. , Solves, P. , de la Rubia, J. , Carpio, N. & Sanz, M.A. (2014) Eculizumab for the treatment of pregnancy‐related atypical hemolytic uremic syndrome. Annals of Hematology, 93, 1421–1422. [DOI] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention (2016) Active Bacterial Core Surveillance Report, Emerging Infections Program Network, Neisseria meningitidis, 2016. Centers for Disease Control and Prevention, Atlanta, GA. [Google Scholar]
- Centers for Disease Control and Prevention (2017) Meningococcal Disease: Age as a Risk Factor. Centers for Disease Control and Prevention, Atlanta, GA. [Google Scholar]
- Chua, J. , Paizis, K. , He, S.Z. & Mount, P. (2017) Suspected atypical haemolytic uraemic syndrome in two post‐partum patients with foetal‐death in utero responding to eculizumab. Nephrology (Carlton), 22 (Suppl 1), 18–22. [DOI] [PubMed] [Google Scholar]
- Cui, D. , Zhang, L. , Li, J. , Zhao, Y. , Hu, X. , Dai, Y. , Zhang, R. & Li, N. (2014) Bovine FcRn‐mediated human immunoglobulin G transfer across the milk‐blood barrier in transgenic mice. PLoS ONE, 9, e115972. [DOI] [PMC free article] [PubMed] [Google Scholar]
- De Sousa Amorim, E. , Blasco, M. , Quintana, L. , Sole, M. , Rodriguez de Cordoba, S. & Campistol, J.M. (2015) Eculizumab in pregnancy‐associated atypical hemolytic uremic syndrome: insights for optimizing management. Journal of Nephrology, 28, 641–645. [DOI] [PubMed] [Google Scholar]
- Delmas, Y. , Bordes, C. , Loirat, C. , Fremeaux‐Bacchi, V. & Combe, C. (2013) Post‐partum atypical haemolytic‐uraemic syndrome treated with eculizumab: terminal complement activity assessment in clinical practice. Clinical Kidney Journal, 6, 243–244. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Demir, E. , Yazici, H. , Ozluk, Y. , Kilicaslan, I. & Turkmen, A. (2016) Pregnant woman with atypical hemolytic uremic syndrome delivered a healthy newborn under eculizumab treatment. Case Reports in Nephrology and Dialysis, 6, 143–148. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Drug Safety and Risk Management Advisory Committee (2014) Briefing Document for Soliris® (eculizumab). Alexion Pharmaceuticals, Inc., Cheshire, CT. [Google Scholar]
- European Medicines Agency (2013) Bexsero (meningococcal group B vaccine) [European public assessment report]. Novartis, Siena, Italy. [Google Scholar]
- European Medicines Agency (2017a) Soliris Summary of Opinion (Post Authorisation). European Medicines Agency, London, UK. [Google Scholar]
- European Medicines Agency (2017b) Guideline on Good Pharmacovigilance Practices (GVP) Annex 1 – Definitions (Rev 4). European Medicines Agency, London, UK. [Google Scholar]
- Fakhouri, F. , Hourmant, M. , Campistol, J.M. , Cataland, S.R. , Espinosa, M. , Gaber, A.O. , Menne, J. , Minetti, E.E. , Provot, F. , Rondeau, E. , Ruggenenti, P. , Weekers, L.E. , Ogawa, M. , Bedrosian, C.L. & Legendre, C.M. (2016) Terminal complement inhibitor eculizumab in adult patients with atypical hemolytic uremic syndrome: a single‐arm, open‐label trial. American Journal of Kidney Diseases, 68, 84–93. [DOI] [PubMed] [Google Scholar]
- Fakhouri, F. , Zuber, J. , Fremeaux‐Bacchi, V. & Loirat, C. (2017) Haemolytic uraemic syndrome. Lancet, 390, 681–696. [DOI] [PubMed] [Google Scholar]
- Figueroa, J.E. & Densen, P. (1991) Infectious diseases associated with complement deficiencies. Clinical Microbiology Reviews, 4, 359–395. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fremeaux‐Bacchi, V. , Fakhouri, F. , Garnier, A. , Bienaime, F. , Dragon‐Durey, M.A. , Ngo, S. , Moulin, B. , Servais, A. , Provot, F. , Rostaing, L. , Burtey, S. , Niaudet, P. , Deschenes, G. , Lebranchu, Y. , Zuber, J. & Loirat, C. (2013) Genetics and outcome of atypical hemolytic uremic syndrome: a nationwide French series comparing children and adults. Clinical Journal of the American Society of Nephrology, 8, 554–562. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gately, R. , San, A. , Kurtkoti, J. & Parnham, A. (2017) Life‐threatening pregnancy‐associated atypical haemolytic uraemic syndrome and its response to eculizumab. Nephrology (Carlton), 22(Suppl 1), 32–35. [DOI] [PubMed] [Google Scholar]
- Geerdink, L.M. , Westra, D. , van Wijk, J.A. , Dorresteijn, E.M. , Lilien, M.R. , Davin, J.C. , Komhoff, M. , Van Hoeck, K. , van der Vlugt, A. , van den Heuvel, L.P. & van de Kar, N.C. (2012) Atypical hemolytic uremic syndrome in children: complement mutations and clinical characteristics. Pediatric Nephrology, 27, 1283–1291. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Greenbaum, L.A. , Fila, M. , Ardissino, G. , Al‐Akash, S.I. , Evans, J. , Henning, P. , Lieberman, K.V. , Maringhini, S. , Pape, L. , Rees, L. , van de Kar, N.C. , Vande Walle, J. , Ogawa, M. , Bedrosian, C.L. & Licht, C. (2016) Eculizumab is a safe and effective treatment in pediatric patients with atypical hemolytic uremic syndrome. Kidney International, 89, 701–711. [DOI] [PubMed] [Google Scholar]
- Hallstensen, R.F. , Bergseth, G. , Foss, S. , Jaeger, S. , Gedde‐Dahl, T. , Holt, J. , Christiansen, D. , Lau, C. , Brekke, O.L. , Armstrong, E. , Stefanovic, V. , Andersen, J.T. , Sandlie, I. & Mollnes, T.E. (2015) Eculizumab treatment during pregnancy does not affect the complement system activity of the newborn. Immunobiology, 220, 452–459. [DOI] [PubMed] [Google Scholar]
- Hillmen, P. , Young, N.S. , Schubert, J. , Brodsky, R.A. , Socie, G. , Muus, P. , Roth, A. , Szer, J. , Elebute, M.O. , Nakamura, R. , Browne, P. , Risitano, A.M. , Hill, A. , Schrezenmeier, H. , Fu, C.L. , Maciejewski, J. , Rollins, S.A. , Mojcik, C.F. , Rother, R.P. & Luzzatto, L. (2006) The complement inhibitor eculizumab in paroxysmal nocturnal hemoglobinuria. New England Journal of Medicine, 355, 1233–1243. [DOI] [PubMed] [Google Scholar]
- Hillmen, P. , Muus, P. , Duhrsen, U. , Risitano, A.M. , Schubert, J. , Luzzatto, L. , Schrezenmeier, H. , Szer, J. , Brodsky, R.A. , Hill, A. , Socie, G. , Bessler, M. , Rollins, S.A. , Bell, L. , Rother, R.P. & Young, N.S. (2007) Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria. Blood, 110, 4123–4128. [DOI] [PubMed] [Google Scholar]
- Hillmen, P. , Muus, P. , Roth, A. , Elebute, M.O. , Risitano, A.M. , Schrezenmeier, H. , Szer, J. , Browne, P. , Maciejewski, J.P. , Schubert, J. , Urbano‐Ispizua, A. , de Castro, C. , Socie, G. & Brodsky, R.A. (2013) Long‐term safety and efficacy of sustained eculizumab treatment in patients with paroxysmal nocturnal haemoglobinuria. British Journal of Haematology, 162, 62–73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Huerta, A. , Arjona, E. , Portoles, J. , Lopez‐Sanchez, P. , Rabasco, C. , Espinosa, M. , Cavero, T. , Blasco, M. , Cao, M. , Manrique, J. , Cabello‐Chavez, V. , Suner, M. , Heras, M. , Fulladosa, X. , Belmar, L. , Sempere, A. , Peralta, C. , Castillo, L. , Arnau, A. , Praga, M. & Rodriguez de Cordoba, S. (2018) A retrospective study of pregnancy‐associated atypical hemolytic uremic syndrome. Kidney International, 93, 450–459. [DOI] [PubMed] [Google Scholar]
- Jang, J.H. , Kim, J.S. , Yoon, S.S. , Lee, J.H. , Kim, Y.K. , Jo, D.Y. , Chung, J. , Sohn, S.K. & Lee, J.W. (2016) Predictive factors of mortality in population of patients with paroxysmal nocturnal hemoglobinuria (PNH): results from a Korean PNH registry. Journal of Korean Medical Science, 31, 214–221. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnson, S. , Khursigara, G. , Yen, J. , Wang, J. , Silliman, N. & Bedrosian, C. (2014) Eculizumab improves survival in atypical hemolytic uremic syndrome (aHUS) patients [abstract SP606]. Nephrology, Dialysis, Transplantation, 29(Suppl. 3), iii275. [Google Scholar]
- Kanakura, Y. , Ohyashiki, K. , Shichishima, T. , Okamoto, S. , Ando, K. , Ninomiya, H. , Kawaguchi, T. , Nakao, S. , Nakakuma, H. , Nishimura, J. , Kinoshita, T. , Bedrosian, C.L. , Valentine, M.E. , Khursigara, G. , Ozawa, K. & Omine, M. (2011) Safety and efficacy of the terminal complement inhibitor eculizumab in Japanese patients with paroxysmal nocturnal hemoglobinuria: the AEGIS clinical trial. International Journal of Hematology, 93, 36–46. [DOI] [PubMed] [Google Scholar]
- Kelly, R.J. , Hill, A. , Arnold, L.M. , Brooksbank, G.L. , Richards, S.J. , Cullen, M. , Mitchell, L.D. , Cohen, D.R. , Gregory, W.M. & Hillmen, P. (2011) Long‐term treatment with eculizumab in paroxysmal nocturnal hemoglobinuria: sustained efficacy and improved survival. Blood, 117, 6786–6792. [DOI] [PubMed] [Google Scholar]
- Kelly, R.J. , Hochsmann, B. , Szer, J. , Kulasekararaj, A. , de Guibert, S. , Roth, A. , Weitz, I.C. , Armstrong, E. , Risitano, A.M. , Patriquin, C.J. , Terriou, L. , Muus, P. , Hill, A. , Turner, M.P. , Schrezenmeier, H. & Peffault de Latour, R. (2015) Eculizumab in pregnant patients with paroxysmal nocturnal hemoglobinuria. New England Journal of Medicine, 373, 1032–1039. [DOI] [PubMed] [Google Scholar]
- Konar, M. & Granoff, D.M. (2017) Eculizumab treatment and impaired opsonophagocytic killing of meningococci by whole blood from immunized adults. Blood, 130, 891–899. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Konar, M. , Lujan, E. & Granoff, D. (2016) Effect of complement inhibition by anti‐C5 (eculizumab) or a small molecule inhibitor of factor D (ACH‐4471) on survival of meningococci in blood from vaccinated adults [abstract]. Blood, 128, 2429. [Google Scholar]
- Kozlovskaya, N.L. , Korotchaeva, Y.V. & Bobrova, L.A. (2018) Adverse outcomes in obstetric‐atypical haemolytic uraemic syndrome: a case series analysis. Journal of Maternal‐Fetal & Neonatal Medicine, Apr 1, 1–7. 10.1080/14767058.2018.1450381 [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- Legendre, C.M. , Licht, C. , Muus, P. , Greenbaum, L.A. , Babu, S. , Bedrosian, C. , Bingham, C. , Cohen, D.J. , Delmas, Y. , Douglas, K. , Eitner, F. , Feldkamp, T. , Fouque, D. , Furman, R.R. , Gaber, O. , Herthelius, M. , Hourmant, M. , Karpman, D. , Lebranchu, Y. , Mariat, C. , Menne, J. , Moulin, B. , Nurnberger, J. , Ogawa, M. , Remuzzi, G. , Richard, T. , Sberro‐Soussan, R. , Severino, B. , Sheerin, N.S. , Trivelli, A. , Zimmerhackl, L.B. , Goodship, T. & Loirat, C. (2013) Terminal complement inhibitor eculizumab in atypical hemolytic‐uremic syndrome. New England Journal of Medicine, 368, 2169–2181. [DOI] [PubMed] [Google Scholar]
- Licht, C. , Greenbaum, L.A. , Muus, P. , Babu, S. , Bedrosian, C.L. , Cohen, D.J. , Delmas, Y. , Douglas, K. , Furman, R.R. , Gaber, O.A. , Goodship, T. , Herthelius, M. , Hourmant, M. , Legendre, C.M. , Remuzzi, G. , Sheerin, N. , Trivelli, A. & Loirat, C. (2015) Efficacy and safety of eculizumab in atypical hemolytic uremic syndrome from 2‐year extensions of phase 2 studies. Kidney International, 87, 1061–1073. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lok, C.E. & Foley, R. (2013) Vascular access morbidity and mortality: trends of the last decade. Clinical Journal of the American Society of Nephrology, 8, 1213–1219. [DOI] [PubMed] [Google Scholar]
- Loschi, M. , Porcher, R. , Barraco, F. , Terriou, L. , Mohty, M. , de Guibert, S. , Mahe, B. , Lemal, R. , Dumas, P.Y. , Etienne, G. , Jardin, F. , Royer, B. , Bordessoule, D. , Rohrlich, P.S. , Fornecker, L.M. , Salanoubat, C. , Maury, S. , Cahn, J.Y. , Vincent, L. , Sene, T. , Rigaudeau, S. , Nguyen, S. , Lepretre, A.C. , Mary, J.Y. , Corront, B. , Socie, G. & Peffault de Latour, R. (2016) Impact of eculizumab treatment on paroxysmal nocturnal hemoglobinuria: a treatment versus no‐treatment study. American Journal of Hematology, 91, 366–370. [DOI] [PubMed] [Google Scholar]
- McNamara, L.A. , Topaz, N. , Wang, X. , Hariri, S. , Fox, L. & MacNeil, J.R. (2017) High risk for invasive meningococcal disease among patients receiving eculizumab (Soliris) despite receipt of meningococcal vaccine. MMWR Morbidity and Mortality Weekly Report, 66, 734–737. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mussoni, M.P. , Veneziano, F.A. , Boetti, L. , Tassi, C. , Calisesi, C. , Nucci, S. , Rigotti, A. , Panzini, I. & Ardissino, G. (2014) Innovative therapeutic approach: sequential treatment with plasma exchange and eculizumab in a pregnant woman affected by atypical hemolytic‐uremic syndrome. Transfusion and Apheresis Science, 51, 134–136. [DOI] [PubMed] [Google Scholar]
- Muus, P. , Licht, C. , Goodship, T.H.J. , Greenbaum, L. , Bedrosian, C.L. , Loirat, C. & Legendre, C. (2011) Eculizumab (ECU) significantly improves health‐related quality of life (HRQoL) in patients with atypical hemolytic uremic syndrome (aHUS) [abstract 4772]. Blood, 118, 4772. [Google Scholar]
- Nishimura, J. , Kanakura, Y. , Ware, R.E. , Shichishima, T. , Nakakuma, H. , Ninomiya, H. , Decastro, C.M. , Hall, S. , Kanamaru, A. , Sullivan, K.M. , Mizoguchi, H. , Omine, M. , Kinoshita, T. & Rosse, W.F. (2004) Clinical course and flow cytometric analysis of paroxysmal nocturnal hemoglobinuria in the United States and Japan. Medicine (Baltimore), 83, 193–207. [DOI] [PubMed] [Google Scholar]
- Noris, M. & Remuzzi, G. (2009) Atypical hemolytic‐uremic syndrome. New England Journal of Medicine, 361, 1676–1687. [DOI] [PubMed] [Google Scholar]
- Noris, M. , Caprioli, J. , Bresin, E. , Mossali, C. , Pianetti, G. , Gamba, S. , Daina, E. , Fenili, C. , Castelletti, F. , Sorosina, A. , Piras, R. , Donadelli, R. , Maranta, R. , van der Meer, I. , Conway, E.M. , Zipfel, P.F. , Goodship, T.H. & Remuzzi, G. (2010) Relative role of genetic complement abnormalities in sporadic and familial aHUS and their impact on clinical phenotype. Clinical Journal of the American Society of Nephrology, 5, 1844–1859. [DOI] [PMC free article] [PubMed] [Google Scholar]
- O'Leary, S.T. & Kimberlin, D.W. (2017) Update from the Advisory Committee on Immunization Practices. Journal of the Pediatric Infectious Diseases Society, 6, 311–316. [DOI] [PubMed] [Google Scholar]
- Peffault de Latour, R. , Mary, J.Y. , Salanoubat, C. , Terriou, L. , Etienne, G. , Mohty, M. , Roth, S. , de Guibert, S. , Maury, S. , Cahn, J.Y. & Socie, G. (2008) Paroxysmal nocturnal hemoglobinuria: natural history of disease subcategories. Blood, 112, 3099–3106. [DOI] [PubMed] [Google Scholar]
- Rossen, L.M. , Ahrens, K.A. & Branum, A.M. (2018) Trends in risk of pregnancy loss among US women, 1990‐2011. Paediatric and Perinatal Epidemiology, 32, 19–29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rother, R.P. , Rollins, S.A. , Mojcik, C.F. , Brodsky, R.A. & Bell, L. (2007) Discovery and development of the complement inhibitor eculizumab for the treatment of paroxysmal nocturnal hemoglobinuria. Nature Biotechnology, 25, 1256–1264. [DOI] [PubMed] [Google Scholar]
- Saad, A.F. , Roman, J. , Wyble, A. & Pacheco, L.D. (2016) Pregnancy‐associated atypical hemolytic‐uremic syndrome. American Journal of Perinatology Reports, 6, e125–e128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sallee, M. , Daniel, L. , Piercecchi, M.‐D. , Jaubert, D. , Fremeaux‐Bacchi, V. , Berland, Y. & Burtey, S. (2010) Myocardial infarction is a complication of factor H‐associated atypical HUS. Nephrology, Dialysis, Transplantation, 25, 2028–2032. [DOI] [PubMed] [Google Scholar]
- Scheinberg, P. , Rios, O. , Scheinberg, P. , Weinstein, B. , Wu, C.O. & Young, N.S. (2014) Prolonged cyclosporine administration after antithymocyte globulin delays but does not prevent relapse in severe aplastic anemia. American Journal of Hematology, 89, 571–574. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schifferli, A. , von Vigier, R.O. , Fontana, M. , Sparta, G. , Schmid, H. , Bianchetti, M.G. & Rudin, C. (2010) Hemolytic‐uremic syndrome in Switzerland: a nationwide surveillance 1997‐2003. European Journal of Pediatrics, 169, 591–598. [DOI] [PubMed] [Google Scholar]
- Sellier‐Leclerc, A.L. , Fremeaux‐Bacchi, V. , Dragon‐Durey, M.A. , Macher, M.A. , Niaudet, P. , Guest, G. , Boudailliez, B. , Bouissou, F. , Deschenes, G. , Gie, S. , Tsimaratos, M. , Fischbach, M. , Morin, D. , Nivet, H. , Alberti, C. & Loirat, C. (2007) Differential impact of complement mutations on clinical characteristics in atypical hemolytic uremic syndrome. Journal of the American Society of Nephrology, 18, 2392–2400. [DOI] [PubMed] [Google Scholar]
- Servais, A. , Devillard, N. , Fremeaux‐Bacchi, V. , Hummel, A. , Salomon, L. , Contin‐Bordes, C. , Gomer, H. , Legendre, C. & Delmas, Y. (2016) Atypical haemolytic uraemic syndrome and pregnancy: outcome with ongoing eculizumab. Nephrology, Dialysis, Transplantation, 31, 2122–2130. [DOI] [PubMed] [Google Scholar]
- Socie, G. , Henry‐Amar, M. , Bacigalupo, A. , Hows, J. , Tichelli, A. , Ljungman, P. , McCann, S.R. , Frickhofen, N. , Van't Veer‐Korthof, E. & Gluckman, E. (1993) Malignant tumors occurring after treatment of aplastic anemia. European Bone Marrow Transplantation‐Severe Aplastic Anaemia Working Party. New England Journal of Medicine, 329, 1152–1157. [DOI] [PubMed] [Google Scholar]
- Sprong, T. , Brandtzaeg, P. , Fung, M. , Pharo, A.M. , Hoiby, E.A. , Michaelsen, T.E. , Aase, A. , van der Meer, J.W. , van Deuren, M. & Mollnes, T.E. (2003) Inhibition of C5a‐induced inflammation with preserved C5b‐9‐mediated bactericidal activity in a human whole blood model of meningococcal sepsis. Blood, 102, 3702–3710. [DOI] [PubMed] [Google Scholar]
- Tedesco, F. (2008) Inherited complement deficiencies and bacterial infections. Vaccine, 26 (Suppl 8), I3–I8. [DOI] [PubMed] [Google Scholar]
- Tsai, H.M. & Kuo, E. (2016) From gestational hypertension and preeclampsia to atypical hemolytic uremic syndrome. Obstetrics and Gynecology, 127, 907–910. [DOI] [PubMed] [Google Scholar]
- UK Teratology Information Service (2017) Use of Eculizumab in Pregnancy. UK Teratology Information Service; http://www.medicinesinpregnancy.org/bumps/monographs/USE-OF-ECULIZUMAB-IN-PREGNANCY/ [Google Scholar]
- US Food and Drug Administration & Center for Drug Evaluation and Research (2007) Soliris Approval Letter. US Food and Drug Administration, Silver Spring, MD. [Google Scholar]
- Villeneuve, P.J. , Schaubel, D.E. , Fenton, S.S. , Shepherd, F.A. , Jiang, Y. & Mao, Y. (2007) Cancer incidence among Canadian kidney transplant recipients. American Journal of Transplantation, 7, 941–948. [DOI] [PubMed] [Google Scholar]
- Yu, F. , Du, Y. & Han, B. (2016) A comparative analysis of clinical characteristics of patients with paroxysmal nocturnal hemoglobinuria between Asia and Europe/America. International Journal of Hematology, 103, 649–654. [DOI] [PubMed] [Google Scholar]
- Zschiedrich, S. , Prager, E.P. & Kuehn, E.W. (2013) Successful treatment of the postpartum atypical hemolytic uremic syndrome with eculizumab. Annals of Internal Medicine, 159, 76. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table SI. Databases, search concepts, and search strategy.
Table SII. System organ class categories with the most frequently reported AEs, by MedDRA preferred terms.
Table SIII. Demographic characteristics of patients with (A) PNH and (B) aHUS who had serious infections.
Table SIV. Demographic characteristics of patients with (A) PNH and (B) aHUS who had malignancy.