

Abstract
As the older adult population grows and becomes more diverse, so will their needs and preferences for living environments. Many adults over 65 years of age require assistance in their living environment (Administration on Aging, 2009), however it is important for their feelings of well-being that the assistance does not restrict their autonomy (e.g., Barkay & Tabak, 2002). Moreover, autonomy enhancement may improve older adults’ functionality (e.g., Greiner et al., 1996). This paper provides an overview of older adults’ diverse living situations and an assessment of their needs for assistance with activities of daily living (ADLs) and instrumental activities of daily living (IADLs) when living in the community or in a long-term care residence, such as assisted living or skilled nursing. We also examine older adults’ residential mobility patterns to understand potential unmet needs for assistance. This needs assessment highlights the specific areas that could benefit from human factors interventions to support older adults in making choice-driven decisions about where they live.
INTRODUCTION
In 2009, adults age 65 and older comprised nearly 13% of the U.S. population and this group is expected to comprise almost 20% of the U.S. population in 2030 (Administration on Aging, 2009). As it grows, the older adult population is also becoming more culturally diverse. By 2050, the distribution of the ethnic population 65 and older in the U.S. is projected to be Hispanic (20%), African American (16.1%), and Asian American (15%) (Angel & Hogan, 2004). The growth and increase in diversity of the older adult population will likely translate to a wider range of lifestyle needs and preferences.
Housing options are one aspect of an older adults’ lifestyle that has grown in recent years. Housing types range from the traditional (e.g., remaining in original home, moving in with relatives, or moving to a skilled nursing residence) to the more recent options (e.g., moving to an assisted living residence or continuing-care retirement community). Moreover, within each housing type there is often a wide range of care levels. Individuals may be living in their original home with very little assistance or with substantial assistance from informal and formal caregivers. Likewise, individuals residing in a skilled nursing residence may be receiving various types and levels of assistance.
Diverse needs for assistance are one of the factors driving housing market changes for older adults. Approximately 37% of adults 65 and older report having a severe disability, ranging from difficulty in hearing, vision, and cognition to difficulty with ambulation, self-care, and independent living (Administration on Aging, 2009). Moreover, the number of people reporting a severe disability increases to 56% for adults over 80 years of age. Some needs for assistance can be met where older adults choose to live, whereas other needs may necessitate an undesired relocation to a long-term care residence.
Older adults’ preferences for living environments vary as well, although most prefer to remain in their own homes as they age (AARP, 2000). Nevertheless, some older adults voluntarily relocate to assisted living residences (Kostka, & Jachimowicz, 2010), in anticipation of future needs for assistance or for the amenities offered. There are also ethnic differences in housing preferences. For example, Asian, African American, and Hispanic seniors are more likely to live in multigenerational homes than Caucasian seniors (AARP, 2001). Given the growing senior ethnic population, these findings suggest the number of older adults living in multigenerational homes will increase.
Regardless of where older adults live, research suggests they want to preserve their autonomy and that this preservation has substantial benefits. Autonomy refers to the “experience of choice” (Ryan & Deci, 2006) and is related to independence. Nursing home policies supporting autonomy are associated with higher resident well-being, less use of support services, and more participation in social activities (Barkay & Tabak, 2002; Rodin, 1986), whereas autonomy-restricting policies are associated with mental and physical decline (e.g., Boyle, 2005). Overall, evidence from cross-sectional, longitudinal, and experimental studies on autonomy present a powerful message suggesting that losses in autonomy may have harmful consequences, including increased morbidity and mortality (Schulz & Brenner, 1977); enhancements in autonomy may improve health status, psychological well-being, and activity level (see Sikorska-Simmons & Wright, 2007, for a review).
Research has shown that even people who reside in assisted living facilities value personal autonomy (Ball et al., 2004). However, some older adults may not prefer to preserve their autonomy (Rodin, 1986) and some may not benefit from autonomy enhancement. One study found that greater autonomy was only associated with reduced rates of hospitalization and mortality for nursing home residents without functional impairment; those with functional impairment did not experience such benefits (Menec & Chipperfield, 1997). Hence, while the majority of older adults may want to maintain their autonomy, there is a subset of older adults whose needs for assistance may surpass or reduce their preference for autonomy.
Needs for assistance can also override preference for housing type. An individual may want to remain in their home, yet their needs require them to move to a long-term care residence. The distinction between choice-driven (i.e., planned) and unplanned moves is important given that older adults who plan their admission to skilled nursing residences may adjust at a faster rate than those with unplanned admissions (Wilson, 2008).
The aforementioned findings emphasize the importance of accommodating older adults’ needs for assistance, and preferences for housing and autonomy. Currently, these data are not integrated in the literature making it difficult to understand what such accommodations should be. Thus, this article provides an analysis of needs for assistance, taking into consideration different living environments. These findings can provide guidance for designers of technologies that enable older adults to live where they choose to live.
WHERE IS HOME?
Adults 65 years of age and older live in a variety of housing arrangements. As shown in Table 1, most live in the community (i.e., the general populace) with a spouse, however many live alone. The likelihood of living alone is higher for those 85 and older and for women. Close to 50% of woman who are 75 and over live alone. About 32% of adults 65 and older live with other relatives, such as in a multigenerational household (20%, Pew, 2009). Nearly 11% of adults 65 and older live in the community with informal care (U.S. Census, 2005) and almost 5% live in the community with formal care (DHHS, 1998).
Table 1.
Living Arrangements for Older Adults in the United States (% of the U.S. population)
| Age | Community Alonea |
Community with Spouseb |
Community with Other Relativesb |
Long-Term Care (Institutional Living)c |
|---|---|---|---|---|
| 65–74 | 21.9 | 63.0 | 10.9 | 1.3 |
| 75–84 | 31.2 | 48.2 | 13.4 | 3.8 |
| 85+ | 38.7 | 27.3 | 23.0 | 15.4 |
Note. Pew (2008),
Administration on Aging (2009). Rows do not equal 100 because living arrangement categories are not comprehensive and table includes data from multiple sources.
Some older adults move into long-term care residences, such as those that offer skilled nursing, assisted living, or continuous care. One notable trend is that the likelihood of living in a long-term care residence increases dramatically for those 85 years of age and older. Adults 85 and older are almost 12 times more likely to live in a skilled nursing residence than those less than 85 years of age. The ramifications of this trend are significant given that those aged 85 and over are the most rapidly growing group of older adults (U.S. Census, 1995).
An increasing number of older adults are living in assisted living residences. In 1999 it was estimated that 811,000 people 65 and older were living in assisted care residences (U.S. Census, 2005). However, given this is a relatively new type of housing, it has not been well researched or defined well enough to make research possible (e.g., Mitchell & Kemp, 2000).
ADL AND IADL ASSISTANCE
Examining the provision and utilization of assistive services can provide insight into older adults’ needs for assistance in different living environments. To understand the needs of older adults living in the community, we explored survey findings regarding assistance from informal caregivers (e.g., partners, adult children, other relatives, friends and neighbors) and formal caregivers (i.e., subsidized or paid professionals). In the U.S., almost 40% of adults 65 and older report having some type of disability (U.S. Census Bureau, 2008). Approximately 96% of those who are disabled (i.e., difficulty in hearing, vision, cognition, ambulation, self-care, or independent living) report receiving assistance from informal caregivers for an average of nearly 29 hours a week (DHHS, 1998).
In one national survey, 1,002 informal caregivers identified the activities of daily living (ADLs) and instrumental activities of daily living (IADLs) for which they provide assistance (Donelan et al., 2002). Many respondents (30%) reported assisting with three or more ADLs. The ADLs that respondents assisted with most frequently included dressing (42%), transfer (40%), ambulation (34%), bathing/showering (26%), feeding (17%), and managing incontinence (related to toileting ADL; 17%). The most commonly reported IADLs for which assistance was provided were errands (85%), transportation (76%), housework (71%), making phone calls (59%), preparing meals (59%) and managing medications (39%). This distribution of responses reflects that informal caregivers assist with IADLs more often than with ADLs, a finding that is consistent with other studies (e.g., Hopp, 1999).
Approximately 35% of disabled older adults use formal home care, although only 5.4% rely entirely on formal caregivers. The use of formal caregivers is greater among those with moderate to severe levels of disability. In fact, approximately half of older adults who require assistance with three or more ADLs rely to some extent on assistance from formal caregivers. Approximately 44% of home health care patients received assistance with personal care, including ADLs and IADLs (DHHS, 2000). Over half of these patients received help with at least one ADL (51%). The most frequent ADLs for which older adults received assistance were bathing/showering, dressing and transfer (see Figure 1). The most common IADL for which assistance was received was housework (see Figure 2). These data reflect a disparity between the type of caregiving tasks provided by informal caregivers, who are more likely to provide assistance with IADLs, and formal caregivers, who are more likely to provide assistance with ADLs.
Figure 1.
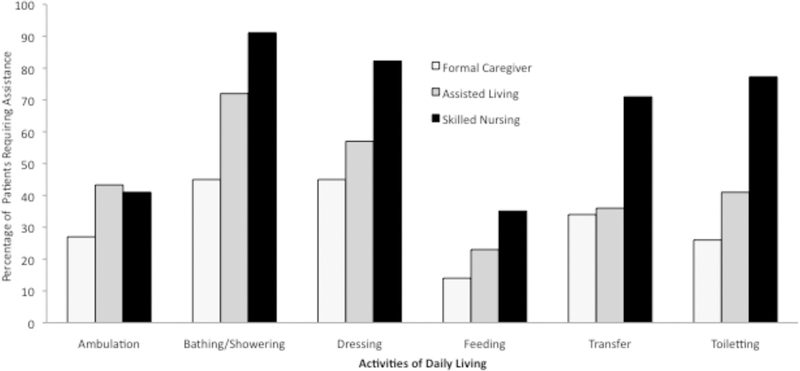
Distribution of support across caregiver type. Percentage of patients requiring ADL assistance.
Figure 2.
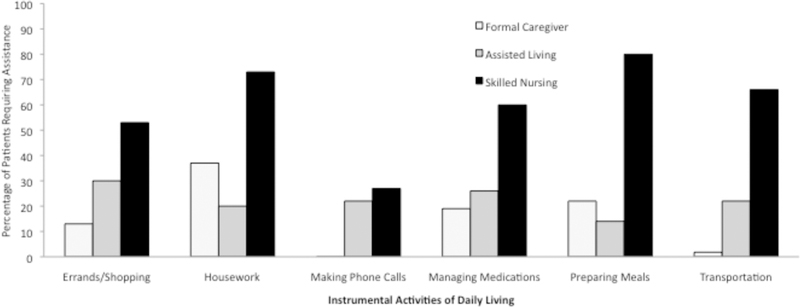
Distribution of support across caregiver type. Percentage of patients requiring IADL assistance.
To understand the needs of older adults living in long-term care residences, we explored data on provision of assistance in long-term care residences. There is general agreement that assisted living is a special type of housing, not licensed as a skilled nursing home, that offers supportive and health care services for individuals who require help with daily activities. Other terms used to describe assisted living include personal care homes and residential care, both of which offer assistive services in a homelike environment (Lewin, 1996).
The average number of ADL limitations for assisted living residents is 2.8 (Cohen & Miller, 2000), and survey findings showed the most common assistance need was for bathing/showering and dressing (NCAL, 2000). Assistance needs for assisted living residents was more equally dispersed for IADLs. Figures 1 and 2 demonstrate a continued shift toward greater provision/need for ADL assistance as the level and availability of care increases in living environment (i.e., comparing community living with formal care services versus assisted living). Assistance with transfer is an exception to this trend in that the need of assistance for this ADL is comparable across community living with formal care services and assisted living.
The average number of ADL limitations increases for skilled nursing residents to 4.7 (Cohen & Miller, 2000), and they most frequently included bathing/showering, dressing, toileting, and transfer (in and out of bed or chairs). Note that the frequency of ambulation limitations is similar for assisted living and skilled nursing residents. Otherwise, not only do needs for assistance with ADLs increase for residents in skilled nursing residences compared to those in assisted living residences, needs for assistance with IADLs increase as well. The most commonly reported IADLs for which assistance was required in skilled nursing residences were preparing meals, transportation, medication management, shopping/errands and housework. Making phone calls was the only IADL for which under 40% of nursing home residents were reported to have limitations.
RESIDENTIAL MOBILITY PATTERNS
The behavioral model of health service utilization (Andersen, 1995), suggests three mechanisms drive utilization of formal health services: 1) predisposing variables, 2) enabling conditions, and 3) need characteristics. Predisposing variables include person characteristics that are correlated with greater use of health services (e.g., age, race). Enabling conditions include variables that make health services more accessible (e.g., income). Need characteristics include impairment and illness-related factors (e.g., limitations in ADLs and IADLs) that necessitate the use of formal services. Need characteristics are often the most immediate and strongest predictors of the utilization of formal health services (Bookwala et al., 2004). Below we discuss need characteristics most predictive of transitions to assisted living and skilled nursing care.
Older adults who live independently often require assistance with IADLs, and those IADL needs can precipitate transitions to assisted living. For example, difficulties performing tasks such as walking outside, doing heavy housework, doing laundry, and going shopping may be predictors of transitions to assisted living (Finlaysona, Mallinsonb, & Barbosac, 2005). Difficulty managing medications has also been found to be a significant reason older adults move into assisted living (Lieto & Schmidt, 2005). This finding is understandable given that on average residents take approximately six medications and 25% take nine or more (Armstrong, Rhodes, & Meiling, 2001). Hence, the need for assistance with IADLs appears to be an important variable impacting whether a person transitions to an assisted living residence. However, the literature in this area is sparse. More systematic, empirical research is needed that carefully examines the relative contributions of various need characteristics in precipitating transitions to assisted living residences.
Predictors of transitions to skilled nursing residences have been researched to a greater extent than those of transitions to assisted living. Whereas transitions to assisted living may be precipitated more by IADL assistance needs, transitions to skilled nursing may be more often predicted by needs for ADL assistance. For example, the percentage of nursing home residents having either complete or partial ADL function dependence may be as high as 97% (Gabriel, 2000). Inability to take a bath independently was the most common dependency in this study. However, other findings suggest that the need for IADL assistance may be a stronger predictor than the need for ADL assistance for skilled nursing transitions. In a study of 4,066 older adults, IADL dependence and bowel incontinence independently predicted skilled nursing residence admission, whereas poor cognitive status, number of chronic conditions, ADL deficits, urinary incontinence, behavioral disturbances, and duration of program operation did not (Friedman, Steinwachs, Rathouz, Burton, & Mukamel, 2005). Together, these findings suggest that ADL and IADL assistance needs are strongly tied to transitions to long-term care facilities. Therefore, ADL and IADL supports are important areas for assistive technology developers to target.
DISCUSSION
The growing aging population has diverse needs, including requirements of assistance with ADLs and IADLs. In some cases these needs necessitate a transition to a living environment that offers greater levels of assistance. However, given that older adults have preferences about where they live and there are significant benefits from maintaining autonomy, there is a need to understand how to support choice-driven living environment decisions.
We reviewed existing research exploring predictors of transitions to long-term care. However, more research is needed, particularly converging evidence on the relative contributions of IADL and ADL assistance needs as predictors. Nevertheless, data are available documenting the provision and utilization of assistance in different living environments. By supporting older adults’ needs, unwanted transitions to higher levels of care may be reduced.
Critical Opportunities for Assistive Technologies
Our needs analysis highlights activities for which older adults receive or require assistance in different living environments. Those residing in the community were more likely to be assisted in performing IADLs, whereas older adults in long-term care residences were more likely to receive assistance for ADLs and IADLs. Given that these declines could precipitate unwanted transitions to residences with higher levels of care, it is crucial that further research focuses on understanding the pattern of these declines.
In a longitudinal study, 47.6% of individuals 75 years of age and older (N=1,344) who reported no difficulty with ADLs at an initial assessment reported some loss in ability to perform ADLs independently at a later assessment (approx. every 20 months; Jagger, Arthur, Spiers, & Clarke, 2001). This pattern reflects the nature of ADLs to decline with age. The order of decline in activities, across gender and age groups, was bathing, mobility, toileting, dressing, transfers from bed and chair, and feeding. The authors concluded that losses in lower-extremity strength (bathing, mobility, toileting) precede losses in upper-extremity strength (dressing, feeding).
Findings such as these are essential for pinpointing the progression of decline in independent functioning. Jaggar and colleagues’ (2001) findings are consistent with the data we presented regarding ADL and IADL assistance in different living environments. Bathing, dressing, toileting and transfer (often a component of toileting) appear to be the ADLs that are in most need of assistance, particularly when greater levels of care are necessitated. Assistance appears to be needed with most of the IADLs, particularly for those who reside at home with informal caregivers and in skilled nursing. Although assistive devices exist for these activities, they may not be used universally, the reason for which is an area in need of exploration. Future assistive technologies for these ADLs and IADLs, designed to be used in home environments, could support older adults’ preferences for aging in place.
Our needs assessment integrated data from various literatures to a degree that has not been done previously. A comprehensive needs assessment, such as this, is an essential first step in understanding where human factors interventions are necessary. This needs assessment can feed directly into a requirements analysis from which to guide design (Beith, 2001). Future directions relevant to human factors professionals includes assessing the usability of currently available assistive devices (e.g., for bathing, dressing, toileting, transfer) and understanding the existing needs for emerging and future assistive technologies.
ACKNOWLEDGEMENTS
This research was supported in part by a grant from the National Institutes of Health (National Institute on Aging) Grant P01 AG17211 under the auspices of the Center for Research and Education on Aging and Technology Enhancement (CREATE; www.create-center.org). The report was inspired by our collaboration with Willow Garage (www.willowgarage.com) who selected the Georgia Institute of Technology as a beta PR2 site for research (www.willowgarage.com/blog/2010/06/07/spotlight-georgia-tech).
REFERENCES
- Administration on Aging (2009). A Profile of Older Americans: 2009 Retrieved January 8, 2011, from http://www.aoa.gov/aoaroot/aging_statistics/Profile/index.aspx
- Andersen RM (1995). Revisiting the behavioral model and access to medical care: does it matter? Journal of Health and Social Behavior, 36, 1–10. [PubMed] [Google Scholar]
- Angel J, & Hogan D (2004). Population aging and diversity in a new era. In Whitfield K (Ed.), Closing the gap: improving the health of minority elders in the new millennium. Washington, DC: Gerontological Society of America. [Google Scholar]
- American Association of Retired Persons (AARP). (2000). Fixing to stay: A national survey of housing and home modification issues. Retrieved January 11, 2011, from assets.aarp.org/rgcenter/il/home_mod.pdf
- American Association of Retired Persons (AARP). (2001). In the middle: A report on multicultural boomers coping with family and aging issues. Retrieved January 11, 2011, from assets.aarp.org/rgcenter/il/in_the_middle.pdf
- Armstrong EP, Rhoads M, & Meiling F (2001). Medication usage patterns in assisted living facilities. Consulting Pharmacist, 6, 65–69. [Google Scholar]
- Ball M, Perkins M, Whittington FJ, Hollingsworth, King S, & Combs B (2004). Independence in assisted living. Journal of Aging Studies, 18, 467–483. [Google Scholar]
- Barkay A, & Tabak N (2002). Elderly residents’ participation and autonomy within a geriatric ward in a public institution. International Journal of Nursing Practice, 8, 198–209. [DOI] [PubMed] [Google Scholar]
- Beith B (2001). Needs and requirements in health care for the older adult: Challenges and opportunities for the new millennium Human factors interventions for the health care of older adults (pp. 13–30). Mahwah, NJ US: Lawrence Erlbaum Associates Publishers. [Google Scholar]
- Bookwala J, Zdaniuk Z, Burton L, Lind B, Jackson S, & Schulz R (2004). Concurrent and long-term predictors of older adults’ use of community-based long-term care services: the caregiver health effects study. Journal of Aging and Health, 16(1), 88–115. [DOI] [PubMed] [Google Scholar]
- Cohen MA, & Miller J (2000). The use of nursing home and assisted living facilities among privately insured and non-privately insured disabled elders. Retrieved January 20, 2011, from http://aspe.hhs.gov/daltcp/reports/2000/nhalfues.htm
- Donelan K, Hill CA, Hoffman C, Scoles K, Feldman PH, Levine C, & Gould D (2002). Challenged to care: informal caregivers in a changing health system. Health Affairs, 21(4), 222–231. [DOI] [PubMed] [Google Scholar]
- Finlayson M, Mallinson T, & Barbosa VM (2005). Activities of daily living (ADL) and instrumental activities of daily living (IADL) items were stable over time in a longitudinal study on aging. Journal of Clinical Epidemiology, 58, 338–349. [DOI] [PubMed] [Google Scholar]
- Friedman SM, Steinwachs DM, Rathouz PJ, Burton LC, & Mukamel DB (2005). Characteristics predicting nursing home admission in the program of all-inclusive care for elderly people. The Gerontologist, 45(2), 157–166. [DOI] [PubMed] [Google Scholar]
- Gabriel CS (2000). Characteristics of elderly nursing home current residents and discharges: data from the 1997 national nursing home survey. Advanced Data, 25(312), 1–15. [PubMed] [Google Scholar]
- Greiner PA, Snowdon DA, & Schmitt FA (1996). The loss of independence in activities of daily living: The role of low normal cognitive function in elderly nuns. American Journal of Public Health, 86, 62–66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hopp FH (1991). Patterns and Predictors of Formal and Informal Care Among Elderly Persons Living in Board and Care Homes. The Gerontologist, 39(2), 167–176 [DOI] [PubMed] [Google Scholar]
- Jagger C, Arthur AJ, Spiers NA, & Clarke M (2001). Patterns of onset of disability in activities of daily living with age. Journal of the American Geriatrics Society, 49(4), 404–9. [DOI] [PubMed] [Google Scholar]
- Kostka T, & Jachimowicz V (2010). Relationship of quality of life to dispositional optimism, health locus of control and self-efficacy in older subjects living in different environments. Quaity of Life Research, 19, 351–361. [DOI] [PubMed] [Google Scholar]
- Lewin-VHI, Inc. (1996). National study of assisted living for the frail elderly: Literature review update Office of the Assistant Secretary for Planning and Evaluation and Administration on Aging, U.S. Department of Health and Human Services. [Google Scholar]
- Lieto JM, & Schmidt KS (2005). Reduced ability to self-administer medication is associated with assisted living placement in a continuing care retirement community. Journal of the American Medical Directors Association, 6(4), 246–9. [DOI] [PubMed] [Google Scholar]
- Menec VH, & Chipperfield JG (1997). The interactive effect of perceived control and functional status on health and mortality among young-old and old-old adults. Journal of Gerontology B Psychological Sciences and Social Sciences, 52, 118–126. [DOI] [PubMed] [Google Scholar]
- Mitchell JM, & Kemp BJ (2000). Quality of life in assisted living homes: A multidimensional analysis. Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 55, P117–P127. [DOI] [PubMed] [Google Scholar]
- Rodin J (1986). Aging and health: Effects of the sense of control. Science, 233, 1271–1276. [DOI] [PubMed] [Google Scholar]
- Ryan RM, & Deci EL (2006). Self-regulation and the problem of human autonomy: Does psychology need choice, self-determination, and will? Journal of Personality, 74(6), 1557–1585. [DOI] [PubMed] [Google Scholar]
- Schulz R, & Brenner J (1977). Relocation of the aged: A review and theoretical analysis. Journal of Gerontology, 32, 323–333. [DOI] [PubMed] [Google Scholar]
- Sikorska-Simmons E, & Wright JD (2007). Determinants of resident autonomy in assisted living facilities: A review of the literature. Care Management Journals, 8(4), 187–193. [DOI] [PubMed] [Google Scholar]
- National Center for Assisted Living (NCAL) (2000). The Assisted Living Sourcebook. Retrieved January 18, 2011, from www.ahcancal.org/ncal/resources/Documents/alsourcebook2001.pdf
- Census US (1995). Sixty-five plus in the United States. Retrieved February 8, 2011, from http://www.census.gov/population/socdemo/statbriefs/agebrief.html
- U.S. Census (2003). America’s families and living arrangements: 2003. Retrieved February 13, 2011, from http://www.census.gov/prod/2004pubs/p20-553.pdf
- U.S. Census (2005). 65+ in the United States: 2005. Retrieved January 20, 2011, from www.census.gov/prod/2006pubs/p23-209.pdf
- U.S. Census (2008). American community survey. Retrieved January 20, 2011, from www.census.gov/compendia/statab/2011/tables/11s0035.pdf
- U.S. Department of Health and Human Services (DHHS) (2000). National home and hospice survey: Current home health care patients. Retrieved January 7, 2008, from http://www.cdc.gov/nchs/data/nhhcsd/curhomecare00.pdf
- U.S. Department of Health and Human Services (DHHS) (1998). Informal Caregiving: Compassion in Action. Retrieved January 7, 2011, from http://aspe.hhs.gov/daltcp/reports/carebro2.pdf
- Wilson SA (2008). The transition to nursing home life: a comparison of planned and unplanned admissions. Journal of Advanced Nursing, 26(5), 864–871. [DOI] [PubMed] [Google Scholar]