

Abstract
Objectives
The term context sensitivity refers to whether a response is in tune with the ever changing demands of the context, while insensitivity is the lack of responding to these cues. To date, we know little about how well patients with pain respond emotionally to changes in the cues provided by the social context, that is, how emotionally context (in)sensitive they are and if this is related to problem severity. The aim of this experimental study was to test a method for determining levels of context sensitivity in individuals with subacute and chronic pain and to explore the link between context (in)sensitivity and pain‐related problems. We operationalized context (in)sensitivity as participants’ emotional responses (observed facial expressions and self‐reported affect) and pain bothersomeness in these contexts and explored the association between these context‐(in)sensitive social‐emotional responses and pain‐related problems.
Methods
Sixty‐two participants with pain were cued to talk openly about three different topics consecutively in a counterbalanced order: (1) their pain, (2) a negative non‐pain topic, and (3) a positive non‐pain topic. We measured the participants’ emotional responses (observed facial expressions and self‐reported affect) and pain bothersomeness across these contexts and explored the effect of social‐emotional responding on pain‐related problems.
Results
The results showed that, irrespective of individuals’ baseline levels of pain bothersomeness, positive affect, and negative affect, those who reacted with more negative affect and pain bothersomeness when prompted to discuss a positive topic had higher levels of pain‐related problems. Moreover, those who showed more negative facial expressions and pain bothersomeness when prompted to discuss a negative non‐pain topic also had higher levels of pain‐related problems.
Conclusions
These findings highlight a link between sensitivity to the social context and the severity of a pain problem. We showed that individuals with greater problem severity were less sensitive to social cues in their emotional responses, as compared to individuals with less pain‐related problems. As predicted, context‐insensitive responding appears to be most strongly associated with pain‐related problems when dealing with negative emotions. Although the cross‐sectional nature of the study prohibits causal conclusions, our findings demonstrate a link and future research is clearly needed to unravel the role of context sensitivity in the development of pain over time.
Statement of contribution.
What is already known on this subject?
Responding to social cues seems to be important for adaptation to pain. The term context sensitivity refers to whether a response is in tune with the provided social cue. To date, we know little about how well patients with persistent pain respond emotionally to changes in the social context, that is, how context (in)sensitive they are and if this is linked to problem severity.
What does this study add?
A test of a method for determining levels of context sensitivity in individuals with persistent pain.
Information about to what extent individuals with chronic pain respond context sensitively.
Knowledge on the link between social context sensitivity and level of pain problems.
Keywords: context sensitivity, social context, flexibility, chronic pain
Background
Context matters: It shapes the way we perceive pain so that an identical noxious stimulus in one situation will be painful, while in a different context, it will not. Early in the history of pain research, Beecher (1946) underscored its relevance in describing how soldiers reacted differently to injuries incurred at war compared to in a safe environment. Context is defined as the collection of cues that signal the probable outcome of a given response (Klein, 1996; Linton, Flink, Schrooten, & Wicksell, 2016). Thus, context is important in learning how to respond to pain in the most advantageous way. Although the context is readily acknowledged as important, there is a lack of research in the field of pain, especially regarding the social context and the link between context‐(in)sensitive responding to social cues and pain.
Responding to social cues seems to be important for adaptation to pain. For example, in some situations social support may be obtained by talking about the pain, while in others, the same behaviour might be punished (Martel, Wideman, & Sullivan, 2012; Shaw, Campbell, Nelson, Main, & Linton, 2013). The term context sensitivity refers to whether a response is in tune with the social context, involving both attending to cues and an ongoing awareness of reinforcement contingencies, while insensitivity is the lack of responding to these cues and an ignorance of current contingencies. Several studies indicate that context sensitivity may be a key in the development of emotional disturbances (Bonanno & Burton, 2013; Coifman & Bonanno, 2010). Similarly, pain coping strategies may be most advantageous when they are sensitive to contextual cues (Linton, 2013; Linton et al., 2016). To date however, we know little about how well patients with pain respond to changes in the social context, that is, how context (in)sensitive they are and if this is related to problem severity.
While research on context (in)sensitivity in pain has been hampered by methodological problems, recent advances from psychopathology now allow for its direct study. The technique was developed in psychological investigations of bereaved adults. Participants who recently lost a loved one were asked to talk about four different topics (loss topic, negative non‐loss topic, positive topic, and current events), each clearly cued by the interviewer (Coifman & Bonanno, 2010). The session was recorded, and sensitivity was determined by studying the correspondence between topic and the participants’ emotional responses. This technique has been tweaked and successfully employed in a sample of medical patients (Harvey, Coifman, Ross, Kleinert, & Giardina, 2016). We draw from these studies, with the purpose of preliminary testing, the value of the concept for understanding pain. We invited people suffering from subacute and chronic pain to talk openly about three different topics consecutively in a counterbalanced order: (1) the pain; (2) a negative non‐pain topic; and (3) a positive topic. In line with the earlier used paradigm (Coifman & Bonanno, 2010), we estimate context sensitivity based on whether participant's expressions of pain and positive/negative affect were congruent with the valence of the cued context. Next, we explored the link between context sensitivity and current levels of pain‐related problems. The purpose of this study then was to test a method for determining levels of context sensitivity in patients suffering from pain and to explore the relationship between context sensitivity, as the predictor variable, and concurrent levels of pain‐related problems, as the outcome.
Method
Overview
In this study, participants suffering from subacute and chronic pain were cued to talk openly about three different topics consecutively, in a counterbalanced order: (1) their pain, (2) a negative non‐pain topic, and (3) a positive non‐pain topic (with the order of topics randomized across participants). We measured participants’ emotional responses (observed facial expressions and self‐reported affect) and pain bothersomeness (self‐reported pain) across these experimental conditions. The degree to which the responses and the valence of the cued topic were in (dis)accordance was used as a proxy for participants’ degree of context (in)sensitivity. In other words, we assumed that the more the responses were in line with the cued topic, the higher the degree of context sensitivity was. Table 1 gives an overview of assumed context‐sensitive and context‐insensitive responding (based on Coifman & Bonanno, 2010) as a reference when analysing the results. First, we analysed the associations between responses and topic. Second, we explored the association between context‐sensitive responding and pain‐related problems while controlling for baseline levels of pain and affect. The study was approved by the Regional Ethical Review Board.
Table 1.
Overview of assumed context‐sensitive and context‐insensitive responding
| Pain topic | Positive non‐pain topic | Negative non‐pain topic | ||||
|---|---|---|---|---|---|---|
| Context sensitive | Context insensitive | Context sensitive | Context insensitive | Context sensitive | Context insensitive | |
| Observed facial expression | Negative facial expression | Positive facial expression | Positive facial expression | Negative facial expression | Negative facial expression | Positive facial expression |
| Subjective rated experience | Pain bothersomeness | Positive affect | Positive affect | Negative affect Pain bothersomeness | Negative affect |
Positive affect Pain bothersomeness |
In the pain topic context, we did not have any assumptions regarding negative affect, as that could both be viewed as context‐sensitive (i.e., part of the pain experience) or context‐insensitive (i.e., not related to pain).
Participants
Figure 1 displays the recruitment process. The study was advertised in local newspapers. Individuals interested in participating contacted the researchers by phone or e‐mail and were informed about the study's general purpose and procedure. Interested individuals underwent a structured screening interview. Inclusion criteria were as follows: (1) sufficient language skills; (2) age = 18–70 years; (3) subacute or chronic back, shoulder, and/or neck pain (>3 weeks); (4) pain intensity the past week ≥ 3 on a scale from 0 (no pain) to 10 (unbearable pain); and (5) pain frequency the past 3 weeks ≥ 5 on a scale from 0 (never) to 10 (always). Exclusion criteria were as follows: (1) severe psychiatric illness that could interfere with participation (e.g., psychosis, substance abuse), (2) severe psychiatric or medical condition at high risk of deterioration in the coming year (e.g., malign cancer), and (3) a planned treatment or surgery in the coming year (e.g., disc surgery). Decisions about eligibility were communicated by phone. Participants were offered snacks and vouchers worth 20 Euros as incentives. Table 2 presents characteristics of the sample.
Figure 1.
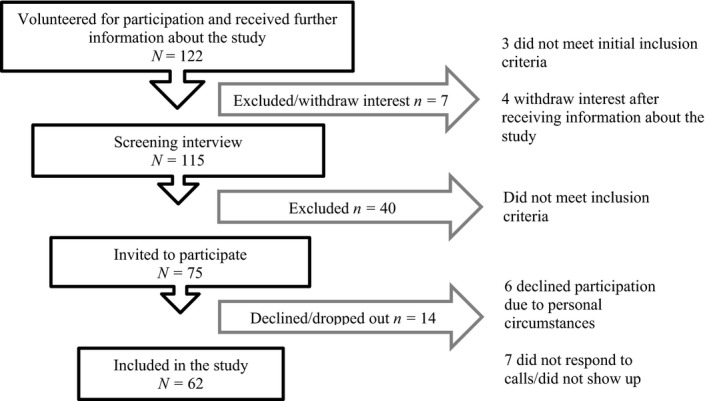
Recruitment process and reasons for exclusion.
Table 2.
Background variables and pain characteristics of the sample (N = 62)
| Age, M (SD) | 55 (12.9) |
| Pain intensity, M (SD) | 5.8 (2.0) |
| ÖMPSQ, M (SD) | 111.3 (29.4) |
| Born in Sweden | 95% |
| Gender, women/men | 77%/23% |
| Married or in a relationship | 71% |
| Pain location (more than one location possible) | |
| Neck | 51% |
| Shoulder | 61% |
| Upper back | 30% |
| Lower back | 72% |
| Arms/legs | 38% |
| Head | 27% |
| Stomach | 15% |
| Pain duration | |
| 1–12 months (acute/subacute) | 8% |
| >12 months (chronic) | 92% |
| Occupation | |
| Employed | 43% |
| Sick leave | 16% |
| Unemployed | 5% |
| Other (e.g., retired) | 36% |
ÖMPSQ = Örebro Musculoskeletal Pain Screening Questionnaire (range 3–210).
Procedure
The protocol was based on the procedure used by Coifman and Bonanno (2010) and was tested in a pilot study (N = 16). The participants were randomly assigned to one of six possible experimental orders (e.g., pain topic – negative non‐pain topic – positive topic, or pain topic – positive topic – negative non‐pain topic) and were contacted by an experiment leader with whom they agreed on a date and a time for participation. The experiment leaders were three female students in clinical psychology who were blind to the hypotheses of the study. All experiments were carried out at the research centre within 3 months after inclusion.
When arriving at the centre, the experiment leader repeated the information about the study and described the experiment more in detail. The participants filled out informed consents, provided demographical data, and completed the self‐ratings regarding pain‐related problems, baseline pain bothersomeness, and positive/negative affect. Subsequently, the experiment leader initiated the video recording and announced the beginning of the first experimental condition (i.e., either the pain topic, the negative non‐pain topic, or the positive topic). The experiment leader read a script informing the participants that they would soon be asked to speak in an open‐ended manner about a certain topic for 2 min. The participants were informed that the experiment leader would remain silent during 2 min and that a timer would announce the end of the 2 min. The experiment leader encouraged the participants to take breaks for reflection if needed. The participants were told to stop talking when the timer signalled, regardless of whether or not they had finished telling their story.
As soon as the participants indicated that they were ready, the experiment leader started a timer set on 2 min and prompted the participants to begin talking. When the timer signalled, the experiment leader thanked the participants for sharing their story. Directly thereafter, the participants rated their experience of pain bothersomeness and positive/negative affect during talking. The second and third experimental conditions were carried out identically to the first experimental condition except for a change in the way interview topics were cued (the independent variable). In between the different topics, there was a short break (5–10 min).
The experiment leaders were instructed to communicate a neutral stance through facial expressions and body language throughout the experiment. The experiment leaders were trained in how to handle typical difficulties during the experiment (e.g., questions, intense emotions, inability to choose a topic to speak about, non‐adherence to the time frame) in a standardized manner. In general, the participants did not have any trouble finding topics, and the experiment leaders did not have to be active during the interviews. The topics varied in content, from more personal ones (e.g., a loss of a loved one, an injury) to daily hassles or positive events (e.g., birthday party, a nice vacation).
Independent variable (cued interview topics)
To create three different controlled social contexts, we varied the verbal instructions (i.e., cues) in the interview situations, based on the paradigm used by Coifman and Bonanno (2010). In the pain topic interview, the general instruction was followed by an invitation to ‘speak about your pain and how it affects your life’. In the negative non‐pain topic interview, the participants were asked to speak about ‘an event or a topic that affects you personally and that is not related to your pain’. Moreover, the participants were told that ‘the event or topic is supposed to be an event or a topic that elicits negative emotions when you think and speak about it. I want you to focus specifically on the aspects eliciting negative emotions’. Finally, the positive topic interview was identical to the negative non‐pain interview except for the fact that the participants were encouraged to speak about a positive event or topic instead of a negative.
Measures and materials
All self‐report instruments were administered through a web‐based survey facility provided by the university. The survey also included demographic questions about age, sex/gender, occupation, country of birth, and civil status.
Experimental assessment of emotional responses and pain bothersomeness
Facial expressions
The system for assessing and coding facial expressions of pain and emotions was based on Coifman and Bonanno (2010). The experiments were video recorded using a Sony Handycam HDR‐CX220 (Sony Corporation, China). The camera was positioned 1 m from the participants and captured the participants from the waist up. The recordings were later viewed by four students in clinical psychology who were blind to the hypotheses and specifics of the study. The coders viewed each experimental condition without sound on a 24‐in. computer screen, according to a randomized order. They were instructed to take into account their total impression of the participant's facial expressions and upper body language. The coders used a 7‐point Likert scale to estimate the participants’ degree of negative affect and positive affect. The inter‐rater reliability was considered as sufficient (intraclass correlation coefficient, .40–.80), except for in the pain interview context where the inter‐rater reliability of negative facial expression was too low. Therefore, facial expressions in this context were excluded from the analyses.
Subjective positive affect and negative affect
Self‐rated positive affect and negative affect were assessed with an instrument specifically developed for the current study in line with the approach used by Coifman and Bonanno (2010), and Coifman, Bonanno, and Rafaeli (2007). The respondents were cued to report on their emotional experience at baseline (‘Reflect on how you are feeling right now and answer the questions below’) as well as immediately after each of the three interview conditions (thinking back and rating how they felt during the interview). They answered eight questions about the extent to which they experienced negative emotions (fear, guilt, distress, and sadness) and positive emotions (happiness, enjoyment, relief, and amusement) (0 = not at all to 7 = very much). Ratings were aggregated for an overall negative affect score and an overall positive affect score (both ranging from 0 to 28). We checked the correspondence between this measure and the Positive and Negative Affect Schedule (PANAS; Watson, Clark, & Tellegen, 1988). As there was satisfactory agreement (correlations between .28 and .63 on negative affect and between .57 and .80 on positive affect), our measure was used in the subsequent analyses. The internal consistency on the items measuring positive affect was good (Cronbach's alpha .89–.95). On the measure of negative affect, it was somewhat lower and questionable (Cronbach's alpha .65–.76), due to a certain degree of floor effect.
Pain bothersomeness
Pain bothersomeness was assessed using an instrument specifically developed and pilot tested for the current study, containing six items. Participants were asked to report their experience at baseline as well as immediately after each of the three interview conditions: They rated five items formulated either as questions (‘How much pain do you have?’ and ‘How much does your pain distract you?’) or statements (‘I find it difficult focusing on anything else than the pain’, ‘I'm restlessly waiting for the pain to decrease’, and ‘The pain I'm experiencing is distressing me’). Items were reformulated to past tense for reporting backward, after each interview condition (e.g., ‘How much pain did you experience?’). The items were rated on a scale from 0 (Not at all or Not true at all) to 7 (Very much or Completely true), resulting in a total score ranging from 0 to 42. The internal consistency of these items was good (Cronbach's alpha .84–.88 depending on condition).
Dependent variable
Pain‐related problems
Problem severity was assessed with the Örebro Musculoskeletal Pain Screening Questionnaire (ÖMPSQ; Linton & Halldén, 1998). The ÖMPSQ was developed to identify patients at risk for developing persistent pain‐related problems, but has also been used to predict future sick leave and perceived health in chronic pain populations (Westman, Linton, Öhrvik, Wahlén, & Leppert, 2008). The instrument consists of 25 items covering various aspects of pain‐related problems such as localization, intensity, frequency, coping behaviour, stress, pain‐related beliefs, and disability. The items are formulated as questions (e.g., ‘Based on all the things you do to cope, or deal with your pain, on an average day, how much are you able to decrease it?’) or statements (e.g., ‘Physical activity makes my pain worse’) and are rated on a scale ranging from 0 (e.g., Can't decrease it at all or Completely disagree) to 10 (e.g., Can decrease it completely or Completely agree). The total score ranges from 3 to 210. A total score between 90 and 105 is commonly interpreted as indicative of a moderate risk for persistent pain and functional impairment, whereas a total score above 105 is interpreted as indicative of a relatively high risk (Linton, 2002). The ÖMPSQ has demonstrated good psychometric properties (Linton & Boersma, 2003).
Data analyses
Positive and negative affect and pain bothersomeness in the three different contexts were considered independent variables in the analyses, and Örebro Musculoskeletal Pain Screening Questionnaire (ÖMPSQ) scores were treated as the outcome, as a proxy for pain‐related problems and risk for future disability. This experimental ordering was applied to minimize the risk of demand characteristics, although it deviates from the usual temporal experimental order (i.e., the ‘outcome’ was assessed before the predictors). Due to skewness on the subjective ratings of emotions and pain bothersomeness, data were summarized using median and interquartile range. As a manipulation check, differences in pain and positive/negative affect were compared across the three interview topics using non‐parametric statistics (Friedman's ANOVA with Wilcoxon signed rank test as post hoc test). To investigate the relation between responses and pain‐related problems, we performed stepwise multiple linear regressions with the ÖMPSQ as dependent variable. Baseline levels of pain bothersomeness, positive affect, and negative affect were controlled for in step 1, and context‐related pain bothersomeness, positive affect, and negative affect were added in step 2 for each interview topic separately. Due to the skewness of the subjective ratings, median splits were used on these variables.
Results
The overall aim was to explore the impact of social‐emotional responding above and beyond the known links between negative affect, pain, and pain‐related problems. To this end, baseline levels were controlled for in the analyses.
Manipulation check
Table 3 shows the associations between interview topics and emotional responses (observed facial expressions and self‐reported affect) and pain bothersomeness on a group level. There were significant differences in emotional responses between the interview topics, except for negative facial expression. The responses were topic congruent, which indicates that overall the manipulation worked, that is, the three contexts triggered different responses. Specifically, pain bothersomeness was significantly higher during the pain topic interview compared to during the positive topic interview. Self‐reported negative affect was significantly higher during the negative non‐pain topic interview compared to during the positive topic, as well as compared to during the pain topic interview. Finally, self‐reported positive affect as well as positive facial expression during the positive topic interview was significantly higher compared to during the negative non‐pain topic interview. Taken together, on average there was congruency between cued topic and response, which indicates that the manipulation worked as intended.
Table 3.
Participants’ median (interquartile range) emotional responses during the interviews with different topics
| Pain topica | Negative non‐pain topicb | Positive non‐pain topicc | Test statistic | |||||
|---|---|---|---|---|---|---|---|---|
| Md | IQR | Md | IQR | Md | IQR | |||
| Pain bothersomeness | 8 | 9.0 | 6 | 10.50 | 4.5 | 10.25 | χ2 F(2) = 17.62b | a > c |
| Self‐rated negative affect | 3 | 7.0 | 6 | 7.0 | 0 | 0 | χ2 F(2) = 62.13b | a < b; b > c; c < a |
| Self‐rated positive affect | 3 | 8.0 | 1 | 3.0 | 20 | 13.0 | χ2 F(2) = 91.43b | b < c; a < c |
| Negative facial expressiona | 4.63 | 2.25 | 4.5 | 1.5 | T = 608.0 | |||
| Positive facial expression | 1.75 | 1.25 | 1.75 | 1.19 | 3 | 2.19 | χ2 F(2) = 64.19b | b < c; a < c |
χ2 F = Friedman's ANOVA; T = Wilcoxon signed rank test.
No data on negative facial behaviour during the pain topic due to low intraclass correlation coefficient.
p < .001.
The relationship between context sensitivity and pain‐related problems
To explore the relationship between the degree of context sensitivity and pain‐related problems, Table 4 shows the predictive value of self‐reported pain and affect during the pain topic interview in explaining variance in pain‐related problems as measured by the ÖMPSQ. As can be seen, controlling for baseline pain bothersomeness, positive affect, and negative affect, high levels of negative affective responding during the pain topic interview were related to higher levels of pain‐related problems.
Table 4.
Prediction of pain‐related problems based on emotional responding and pain bothersomeness during the pain topic interview
| Pain topic (PaT) analysis for subjective emotional responses and pain bothersomeness, F(6, 51) = 4.71** | |||||
|---|---|---|---|---|---|
| Variable | B | SE B | β | R 2 | ΔR 2 |
| Step 1 | |||||
| Baseline pain bothersomeness | 1.22** | 0.43 | .36 | .23 | |
| Baseline negative affect | −0.25 | 0.86 | −.04 | ||
| Baseline positive affect | −1.66** | 0.58 | −.36 | ||
| Step 2 | |||||
| Baseline pain bothersomeness | 0.74 | 0.51 | .22 | .28 | .5# |
| Baseline negative affect | −1.04 | 0.94 | −.16 | ||
| Baseline positive affect | −1.98** | 0.73 | −.42 | ||
| PaT pain bothersomeness | 13.55 | 8.73 | .23 | ||
| PaT negative affect | 16.01* | 7.38 | .27 | ||
| PaT positive affect | 9.20 | 9.33 | .16 | ||
Dependent variable is Örebro Musculoskeletal Pain Screening Questionnaire. No facial behaviour is analysed due to low intraclass correlation coefficient on negative facial behaviour during the pain topic interview.
# p < .10; *p < .05; **p < .01.
Table 5 shows the predictive value of emotional responding (observed facial expressions and self‐reported pain and affect) during the negative non‐pain topic interview in explaining variance in pain‐related problems. As can be seen, while controlling for baseline pain bothersomeness, positive affect, and negative affect, higher levels of self‐reported pain bothersomeness as well as self‐rated and observed negative affect were associated with higher levels of pain‐related problems. Note however that the change in explained variance when adding self‐reported negative affect (step 2) was only significant at p < .10.
Table 5.
Prediction of pain‐related problems based on pain bothersomeness and emotional responding during the negative non‐pain topic interview
| Variable | B | SE B | β | R 2 | ΔR 2 |
|---|---|---|---|---|---|
| Negative non‐pain topic (NT) analysis for subjective emotional responses and pain bothersomeness, F(6, 52) = 5.67** | |||||
| Step 1 | |||||
| Baseline pain bothersomeness | 1.17** | 0.43 | .35 | .22 | |
| Baseline negative affect | −0.50 | 0.84 | −.08 | ||
| Baseline positive affect | −1.78** | 0.57 | −.38 | ||
| Step 2 | |||||
| Baseline pain bothersomeness | 0.17 | 0.56 | .05 | .33 | .11* |
| Baseline negative affect | −0.92 | 0.85 | −.15 | ||
| Baseline positive affect | −2.01** | 0.58 | −.43 | ||
| NT pain bothersomeness | 26.73** | 9.04 | .46 | ||
| NT negative affect | 12.64# | 7.04 | .21 | ||
| NT positive affect | 1.74 | 7.19 | .03 | ||
| NT analysis for facial behaviour, F(5, 53) = 5.62** | |||||
| Step 1 | |||||
| Baseline pain bothersomeness | 1.14** | 0.43 | .34 | .22 | |
| Baseline negative affect | −0.52 | 0.83 | −.08 | ||
| Baseline positive affect | −1.76** | 0.57 | −.38 | ||
| Step 2 | |||||
| Baseline pain bothersomeness | 1.26** | 0.42 | .38 | .29 | .7* |
| Baseline negative affect | −1.05 | 0.82 | −.17 | ||
| Baseline positive affect | −2.16** | 0.56 | −.46 | ||
| NT negative facial behaviour | 17.67** | 6.77 | .30 | ||
| NT positive facial behaviour | 6.41 | 6.74 | .11 | ||
Dependent variable is Örebro Musculoskeletal Pain Screening Questionnaire.
# p < .10; **p < .01.
Finally, Table 6 shows the predictive value of emotional responding (observed facial expressions and self‐reported pain and affect) in explaining variance in pain‐related problems during the positive topic interview, while controlling for baseline pain bothersomeness, positive affect, and negative affect. As can be seen, high levels of negative affective responding and higher experience of pain bothersomeness were related to higher levels of pain‐related problems. No association was found with facial expressions.
Table 6.
Prediction of pain‐related problems based on emotional responding and pain bothersomeness during the positive topic interview
| Variable | B | SE B | β | R 2 | ΔR 2 |
|---|---|---|---|---|---|
| Positive topic (PoT) analysis for subjective emotional responses, F(6, 48) = 6.11** | |||||
| Step 1 | |||||
| Baseline pain bothersomeness | 1.18** | 0.43 | .35 | .26 | |
| Baseline negative affect | −0.60 | 0.87 | −.09 | ||
| Baseline positive affect | −1.99** | 0.59 | −.42 | ||
| Step 2 | |||||
| Baseline pain bothersomeness | 0.51 | 0.49 | .15 | .36 | .10* |
| Baseline negative affect | −1.31 | 0.90 | −.20 | ||
| Baseline positive affect | −2.51** | 0.63 | −.53 | ||
| PoT pain bothersomeness | 17.15* | 8.22 | .29 | ||
| PoT negative affect | 21.23* | 9.48 | .27 | ||
| PoT positive affect | 14.13# | 7.69 | .24 | ||
| PoT analysis for facial behaviour, F(5, 53) = 4.31** | |||||
| Step 1 | |||||
| Baseline pain bothersomeness | 1.16** | 0.43 | .34 | .22 | |
| Baseline negative affect | −0.54 | 0.86 | −.08 | ||
| Baseline positive affect | −1.78** | 0.58 | −.38 | ||
| Step 2 | |||||
| Baseline pain bothersomeness | 1.25** | 0.43 | .37 | .22 | |
| Baseline negative affect | −0.51 | 0.87 | −.08 | ||
| Baseline positive affect | −1.91** | 0.58 | −.41 | ||
| PoT negative facial behaviour | 5.46 | 7.09 | .09 | ||
| PoT positive facial behaviour | 8.87 | 7.06 | .15 | ||
Dependent variable is Örebro Musculoskeletal Pain Screening Questionnaire.
*p < .05; **p < .01; # p >.10.
To clearly picture the association between self‐reported emotional responding and pain‐related problems, it is also graphically depicted in Figure 2. As can be seen, more negative emotional reactivity and pain bothersomeness in social encounters where it was not prompted were clearly related to pain problem level signalling risk for chronicity (ÖMPSQ > 105).
Figure 2.
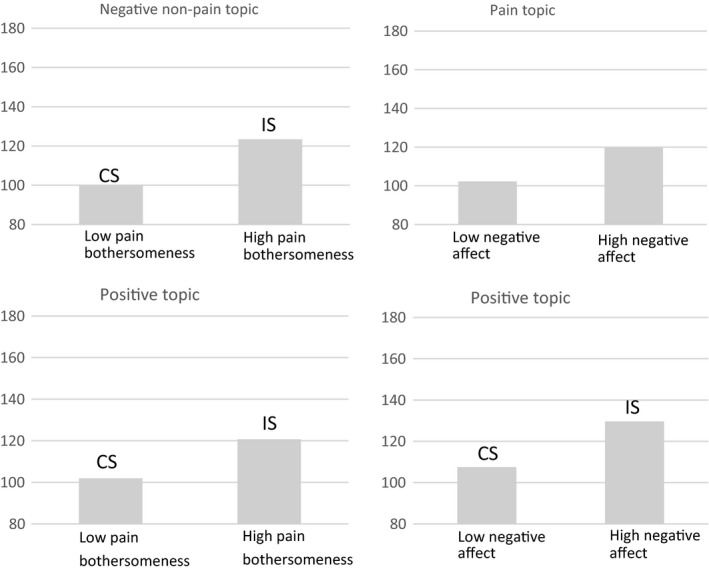
Levels of pain coping problems for participants with context‐sensitive (CS) and context‐insensitive (IS) emotional responses (baseline levels controlled for). Note. The numbers on the y‐axis refer to scores on the Örebro Musculoskeletal Pain Screening Questionnaire (ÖMPSQ; range 3–210), as a proxy for pain‐related problems. Total score 90–105 = moderate risk; >105 = high risk.
This indicates that a larger tendency for context‐insensitive responding was related to high levels of pain‐related problems.
As a summary, all significant associations between context sensitivity versus insensitivity and pain‐related problems are highlighted in Table 7 (typed in bold).
Table 7.
A summary of the identified associations between emotional responding/pain bothersomeness and pain‐related problems in each of the three contexts
| Pain topic | Positive non‐pain topic | Negative non‐pain topic | ||||
|---|---|---|---|---|---|---|
| Context sensitive | Context insensitive | Context sensitive | Context insensitive | Context sensitive | Context insensitive | |
| Observed facial expression | Positive facial expression | Negative facial expression | Negative facial expression | Positive facial expression | ||
| Subjective rated experience | Pain bothersomeness | Positive affect | Positive affect |
Negative affect Pain bothersomeness |
Negative affect |
Positive affect Pain bothersomeness |
All significant associations are typed in bold. In addition to the associations highlighted in this table, self‐rated negative affect during the pain topic was also significantly related to outcome.
Discussion
This is the first study demonstrating a link between emotional responding in a social context and the degree of a pain problem in people suffering from subacute and chronic pain, using an experimental paradigm from the psychopathology literature. Taken as a whole, our findings indicate that context‐insensitive responding to social cues was related to higher levels of pain‐related problems, at least when dealing with negative affect.
Context‐insensitive pain bothersomeness was related to more problems in both the positive and the negative non‐pain interviews. As all participants were selected on the basis of pain, and not on basis of emotional problems, it seems logical that specifically the context‐insensitive pain bothersomeness was important. This corresponds with the extensive literature highlighting the interruptive function of pain and the importance of being able to disengage from pain to cope with it (Eccleston & Crombez, 1999). It has been suggested that catastrophizing may hamper disengagement from pain (Van Damme, Crombez, & Eccleston, 2004). When considering catastrophizing as a feature of inflexibility (Flink, Boersma, & Linton, 2013), it is reasonable that individuals who catastrophize are also context insensitive. However, the link between catastrophizing and context insensitivity needs to be explored empirically to unravel the relationship between these constructs.
When talking about a positive topic, context‐insensitive negative affect was related to more pain‐related problems. This means that individuals with high levels of pain‐related problems were not able to detach from negative feelings when asked to focus on a positive subject. It should be noted that baseline levels of pain and negative affect were controlled for, which strengthens the conclusion that context insensitivity in and of itself was linked to more problems. These results are in line with findings from research on psychopathology, where context‐insensitive expressions of current issues have been related to more psychological problems (Coifman & Bonanno, 2010; Harvey et al., 2016; Southward & Cheavens, 2017), and encourage further research on the importance of context sensitivity in a pain setting.
Context sensitivity is closely related to the theory around discriminative facility, stemming from the field of personality research. Discriminative facility refers to an individuals’ appraisal of situational demands and their ability to adjust behavioural responses depending on present cues (Cheng, Chiu, Hong, & Cheung, 2001; Chiu, Hong, Mischel, & Shoda, 1995). Observations of the value of including situations in the assessment of personality go back to the work of Mischel (1969). Today, this aspect is integrated in the contextualized personality psychology (Mischel, 2004). Discriminative facility is a prerequisite for coping flexibility, conceptualized as a good fit between applied coping strategies and the nature of stressful events (Aldwin, 1994). The importance of behavioural flexibility has been further developed in the theoretical underpinnings of Acceptance and Commitment Therapy (ACT), summarized in the model of psychological flexibility, which has been put forward as central for adaptive coping with pain (McCracken & Morley, 2014). Taken together, context sensitivity clearly overlaps with concepts from personality psychology as well as contemporary learning theories, and more research is required to explore the intricate relation and the unique contribution of these constructs.
Our findings add to the existing literature indicating that particular regulatory strategies are not consistently beneficial or maladaptive; the key is rather to have a flexible use of strategies that respond to the ever changing environment. The regulatory flexibility model (Bonanno & Burton, 2013) identifies three central components of flexibility: sensitivity in reading and evaluating the context, availability of a diverse repertoire of regulatory strategies, and responsiveness to feedback. In our study, we did not isolate the specific components in this model; this may be a mission for future research.
Although the literature may suggest that context sensitivity is linked to a better prognosis and less pain‐related problems (Linton et al., 2016), our findings provide important nuances. Indeed, our findings indicate that individuals with higher levels of pain‐related problems specifically more easily access negative emotional responses, irrespective of social cues. One possibility is that these individuals have a general tendency to easily access negative affect and difficulties in down‐regulating it. This goes in line with the dynamic model of affect, which states that individuals experiencing worsening pain adopt simpler representations of their affective experiences, resulting in easier access to negative experiences as negative affects tend to outcompete positive ones (Zautra, Smith, Affleck, & Tennen, 2001). In other words, pain‐related problems might be linked to emotion regulation difficulties. However, if emotion regulation difficulties explain the identified links, it is not the negative affect per se which is undesirable, but rather that the individuals need to be able to down‐regulate it when it is cued. It is important to note that there was no link whatsoever between context‐insensitive positive affect and pain‐related problems. This corresponds with the findings from Coifman and Bonanno (2010), who found that positive emotions were beneficial regardless of context.
One drawback in the current study is the lack of longitudinal outcome data. Because the study is cross‐sectional in nature, we cannot draw conclusions about causality or the direction of identified links. Another shortcoming is that data on negative facial behaviour in the pain context are missing. Although we based the procedure on an earlier used paradigm (Coifman & Bonanno, 2010), it might have been too difficult for students to code the participants’ facial behaviour resulting in a fairly modest inter‐rater reliability. The difficulties in coding facial behaviour may also explain the evident lack of correspondence between facial behaviour and subjective ratings. Coding verbal content would have been an alternative strategy for exploring context sensitivity and insensitivity. However, as the participants were extremely compliant in following our instructions, detecting differences in verbal content would have required more sophisticated measures and analytical approaches than this study allowed. An additional limitation is the lack of a neutral topic which could have been used as a comparison condition and a more reliable baseline. Future studies would preferably include that.
The data in this study were analysed within each context separately. A shortcoming of this analytical approach is that it precludes conclusions on patterns of responding within individuals. As it is likely that more generalized forms of context insensitivity (e.g., subgroup of persons responding insensitive across several contexts) are more highly related to negative outcome, future, more well‐powered studies, could make use of person‐oriented analytical approaches such as latent profiling or cluster analyses to discern within person patterns of responding. Despite these shortcomings, this study contributes to unique knowledge, emphasizing the link between pain‐related problems and context‐insensitive responding to social cues. Although the results are quite complex, the overall picture indicates that individuals with higher levels of pain‐related problems more easily respond with negative emotionality and pain bothersomeness, irrespective of social cues. A further step is to explore the clinical implications and possibly develop methods for context‐insensitive patients with pain, to facilitate adaption to pain within an interpersonal context.
Taken together, these findings indicate that context sensitivity does matter, at least when dealing with negative affect. Although the longitudinal links need to be explored, this adds to the existing literature, pointing towards context sensitivity as a central feature of adaptation to pain. Future research should explore how context sensitivity is related to development of pain over time, to reveal differences between acute and chronic problems, and delve into the relation between context sensitivity and other well‐known risk factors such as catastrophizing and psychological flexibility.
Conflict of interest
All authors declare no conflict of interest.
Funding
This research was supported by a grant from The Swedish Foundation for Humanities and Social Sciences, grant number P14‐0799:1.
References
- Aldwin, C. (1994). Stress, coping, and development. New York: Guilford Press. [Google Scholar]
- Beecher, H. K. (1946). Pain in men wounded in battle. Annals of Surgery, 123(1), 96 10.1213/00000539-194701000-00005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bonanno, G. A. , & Burton, C. L. (2013). Regulatory flexibility: An individual differences perspective on coping and emotion regulation. Perspectives on Psychological Science, 8, 591–612. 10.1177/1745691613504116 [DOI] [PubMed] [Google Scholar]
- Cheng, C. , Chiu, C. Y. , Hong, Y. Y. , & Cheung, J. S. (2001). Discriminative facility and its role in the perceived quality of interactional experiences. Journal of Personality, 69, 765–785. 10.1111/1467-6494.695163 [DOI] [PubMed] [Google Scholar]
- Chiu, C. Y. , Hong, Y. Y. , Mischel, W. , & Shoda, Y. (1995). Discriminative facility in social competence: Conditional versus dispositional encoding and monitoring‐blunting of information. Social Cognition, 13(1), 49–70. 10.1521/soco.1995.13.1.49 [DOI] [Google Scholar]
- Coifman, K. G. , & Bonanno, G. A. (2010). When distress does not become depression: Emotion context sensitivity and adjustment to bereavement. Journal of Abnormal Psychology, 119, 479 10.1037/a0020113 [DOI] [PubMed] [Google Scholar]
- Coifman, K. G. , Bonanno, G. A. , & Rafaeli, E. (2007). Affect dynamics, bereavement and resilience to loss. Journal of Happiness Studies, 8, 371–392. 10.1007/s10902-006-9014-5 [DOI] [Google Scholar]
- Eccleston, C. , & Crombez, G. (1999). Pain demands attention: A cognitive–affective model of the interruptive function of pain. Psychological Bulletin, 125, 356 10.1037/0033-2909.125.3.356 [DOI] [PubMed] [Google Scholar]
- Flink, I. L. , Boersma, K. , & Linton, S. J. (2013). Pain catastrophizing as repetitive negative thinking: A development of the conceptualization. Cognitive Behaviour Therapy, 42, 215–223. 10.1080/16506073.2013.769621 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harvey, M. M. , Coifman, K. G. , Ross, G. , Kleinert, D. , & Giardina, P. (2016). Contextually appropriate emotional word use predicts adaptive health behavior: Emotion context sensitivity and treatment adherence. Journal of Health Psychology, 21, 579–589. 10.1177/1359105314532152 [DOI] [PubMed] [Google Scholar]
- Klein, S. B. (1996). Learning: Principles and applications (3rd ed.). New York, NY: McGraw‐Hill. [Google Scholar]
- Linton, S. J. (2002). Early identification and intervention in the prevention of musculoskeletal pain. American Journal of Industrial Medicine, 41, 433–442. 10.1002/ajim.10052 [DOI] [PubMed] [Google Scholar]
- Linton, S. J. (2013). A transdiagnostic approach to pain and emotion. Journal of Applied Biobehavioral Research, 18(2), 82–103. 10.1111/jabr.12007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Linton, S. J. , & Boersma, K. (2003). Early identification of patients at risk of developing a persistent back problem: The predictive validity of the Örebro Musculoskeletal Pain Questionnaire. The Clinical Journal of Pain, 19(2), 80–86. 10.1097/00002508-200303000-00002 [DOI] [PubMed] [Google Scholar]
- Linton, S. J. , Flink, I. K. , Schrooten, M. G. , & Wicksell, R. (2016). Understanding co‐occurring emotion and pain: The role of context sensitivity from a transdiagnostic perspective. Journal of Contemporary Psychotherapy, 46(3), 129–137. 10.1007/s10879-016-9323-x [DOI] [Google Scholar]
- Linton, S. J. , & Halldén, K. (1998). Can we screen for problematic back pain? A screening questionnaire for predicting outcome in acute and subacute back pain. The Clinical Journal of Pain, 14, 209–215. 10.1097/00002508-199809000-00007 [DOI] [PubMed] [Google Scholar]
- Martel, M. O. , Wideman, T. H. , & Sullivan, M. J. (2012). Patients who display protective pain behaviors are viewed as less likable, less dependable, and less likely to return to work. PAIN®, 153, 843–849. [DOI] [PubMed] [Google Scholar]
- McCracken, L. M. , & Morley, S. (2014). The psychological flexibility model: A basis for integration and progress in psychological approaches to chronic pain management. The Journal of Pain, 15, 221–234. 10.1016/j.jpain.2013.10.014 [DOI] [PubMed] [Google Scholar]
- Mischel, W. (1969). Continuity and change in personality. American Psychologist, 24, 1012–1018. 10.1037/h0028886 [DOI] [PubMed] [Google Scholar]
- Mischel, W. (2004). Toward an integrative science of the person. Annual Review of Psychology, 55, 1–22. 10.1146/annurev.psych.55.042902.130709 [DOI] [PubMed] [Google Scholar]
- Shaw, W. S. , Campbell, P. , Nelson, C. C. , Main, C. J. , & Linton, S. J. (2013). Effects of workplace, family and cultural influences on low back pain: What opportunities exist to address social factors in general consultations? Best Practice & Research Clinical Rheumatology, 27, 637–648. 10.1016/j.berh.2013.09.012 [DOI] [PubMed] [Google Scholar]
- Southward, M. W. , & Cheavens, J. S. (2017). Assessing the relation between flexibility in emotional expression and symptoms of anxiety and depression: The roles of context sensitivity and feedback sensitivity. Journal of Social and Clinical Psychology, 36, 142 10.1521/jscp.2017.36.2.142 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Van Damme, S. , Crombez, G. , & Eccleston, C. (2004). Disengagement from pain: The role of catastrophic thinking about pain. Pain, 107(1–2), 70–76. 10.1016/j.pain.2003.09.023 [DOI] [PubMed] [Google Scholar]
- Watson, D. , Clark, L. A. , & Tellegen, A. (1988). Development and validation of brief measures of positive and negative affect: The PANAS scales. Journal of Personality and Social Psychology, 54, 1063 10.1037/0022-3514.54.6.1063 [DOI] [PubMed] [Google Scholar]
- Westman, A. , Linton, S. J. , Öhrvik, J. , Wahlén, P. , & Leppert, J. (2008). Do psychosocial factors predict disability and health at a 3‐year follow‐up for patients with non‐acute musculoskeletal pain? A validation of the Örebro Musculoskeletal Pain Screening Questionnaire. European Journal of Pain, 12, 641–649. 10.1016/j.ejpain.2007.10.007 [DOI] [PubMed] [Google Scholar]
- Zautra, A. , Smith, B. , Affleck, G. , & Tennen, H. (2001). Examinations of chronic pain and affect relationships: Applications of a dynamic model of affect. Journal of Consulting and Clinical Psychology, 69, 786 10.1037//0022-006X.69.5.786 [DOI] [PubMed] [Google Scholar]