

Abstract
Background
A recent Center for Medicare and Medicaid Innovation report evaluated the four‐year Strong Start for Mothers and Newborns Initiative, which sought to improve maternal and newborn outcomes through exploration of three enhanced, evidence‐based care models. This paper reports the socio‐demographic characteristics, care processes, and outcomes for mothers and newborns engaged in care with American Association of Birth Centers (AABC) sites.
Methods
The authors examined data for 6424 Medicaid or Children's Health Insurance Program (CHIP) beneficiaries in birth center care who gave birth between 2013 and 2017. Using data from the AABC Perinatal Data Registry™, descriptive statistics were used to evaluate socio‐behavioral and medical risks, and core perinatal quality outcomes. Comparisons are made between outcomes in the AABC sample and national data during the study period.
Results
Childbearing mothers enrolled at AABC sites had diverse socio‐behavioral risk factors similar to the national profile. The AABC sites exceeded national quality benchmarks for low birthweight (3.28%), preterm birth (4.42%), and primary cesarean birth (8.56%). Racial disparities in perinatal indicators were present within the Strong Start sample; however, they were at narrower margins than in national data. The enhanced model of care was notable for use of midwifery‐led prenatal, labor, and birth care and decreased hospital admission.
Conclusions
Birth center care improves population health, patient experience, and value. The model demonstrates the potential to decrease racial disparity and improve population health. Reduction of regulatory barriers and implementation of sustainable reimbursement are warranted to move the model to scale for Medicaid beneficiaries nationwide.
Keywords: birth centers/birthing centers, midwifery, Strong Start
1. INTRODUCTION
Medicaid finances approximately one‐half of all births in the United States.1 The Center for Medicare and Medicaid Innovation (CMMI) Strong Start for Mothers and Newborns Initiative was designed to determine whether enhanced prenatal care models could reduce preterm birth and other poor outcomes of pregnancy for mothers and infants while improving quality and lowering costs.2, 3 Three models of prenatal care were evaluated during the 4‐year initiative: centering or group prenatal care, maternity care home, and birth center care.
Studies of freestanding birth centers have consistently demonstrated safe, high‐quality care with fewer medical interventions during labor than usual care, while achieving lower cesarean birth rates.4, 5, 6, 7, 8, 9, 10, 11 Neonatal outcomes have been similar to those of lower‐risk mothers in usual care.7, 8, 9
Previous birth center study populations were mostly white, non‐Hispanic, college‐educated, and middle‐ and higher‐income mothers, making it difficult to generalize findings to all lower‐risk childbearing mothers in the United States.8, 9 Preliminary evaluation of American Association of Birth Centers (AABC) Medicaid beneficiaries enrolled at Strong Start sites demonstrated population diversity and high‐quality outcomes responsive to the enhanced, wellness‐oriented model of care.4, 10
The purpose of this research was to explore the medical and social risk factors, care processes, and quality outcomes of Medicaid beneficiaries in the AABC Strong Start sample compared with publicly reported US data in order to inform future research and Medicaid policy reform.
2. METHODS
This descriptive analysis includes all 6424 Medicaid beneficiaries enrolled and giving birth with the 45 AABC Strong Start birth center sites in 19 states between 2013 and 2017. The sample includes women who received prenatal care in AABC Strong Start sites with planned birth locations of birth center, home, and hospital, both elective and medically indicated, as well as women requiring transfer to the hospital during labor. The AABC birth center model provides enhanced primary maternity care that is integrated into the overall perinatal care system (Figure 1). This midwifery‐led model (Figure 2) includes structured relationship building, time‐intensive care, and individualized education, all of which have been demonstrated to improve outcomes for socially at‐risk communities.4, 5, 10, 11
Figure 1.
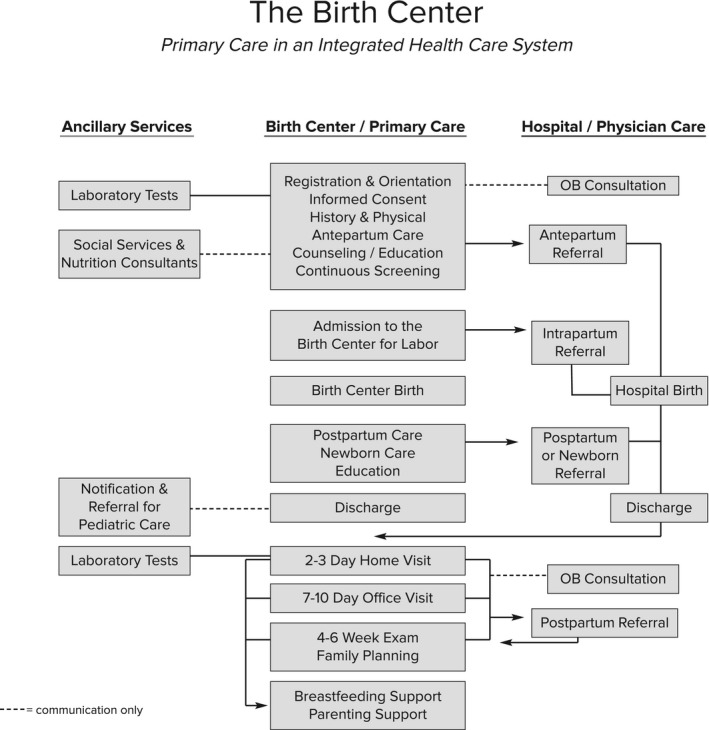
The birth center: primary care in an integrated health care system
Figure 2.
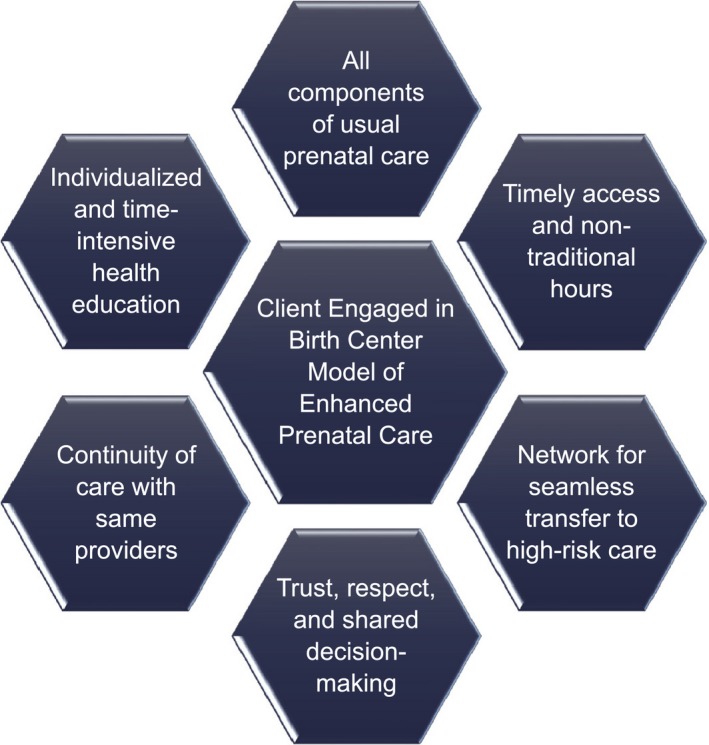
Birth center model of enhanced prenatal care [Color figure can be viewed at wileyonlinelibrary.com]
Clients are fully engaged in their care with birth center midwives providing support, respect, and shared decision‐making. Prenatal visits last longer than in medical model care, and clients are encouraged to develop relationships with midwife providers. Educational components of prenatal care are individualized depending on each client's needs and include discussion of the benefits of physiologic pregnancy, labor, birth, postpartum, and newborn care. In addition, birth centers work with a network of referral providers; thus, consultations or referrals are available if needed. Birth may occur in the birth center or hospital, although in some birth centers choice of hospital birth involves using a different provider who may be a physician. In some birth center practices, home birth is an option. This model differs from usual US maternity care that is predominantly provided in the medical model with birth occurring in the hospital, involving relatively high levels of intervention, and attended by physicians.
We analyzed data from the American Association of Birth Centers Perinatal Data Registry (AABC PDR™), version 3.0, one of the largest observational, prospective, de‐identified, perinatal data registries in the United States. The PDR measures demographic, descriptive, and process‐and‐outcome indicators while adhering to the registry guidelines from the Agency for Healthcare Research and Quality.12 Quality assurance mechanisms are in place to ensure systematic client enrollment, timely completion of data, minimization of loss of follow‐up, and data consistency checks through verification with medical record numbers by the site. Data definitions are embedded within the data set, published in the user manual, and reviewed during mandatory user trainings. A validation study conducted in 2010 found a high level of consistency between registry data and matched medical records, exceeding birth certificate capabilities with 100% consistency for 10 variables.13 Childbearing mothers signed a consent form to participate in the Strong Start program and to be included in the data registry after their first prenatal visit. Perinatal attrition was tracked and included medical attrition such as spontaneous abortions and elective or medically indicated pregnancy terminations, and elective transfers of care and migration.
Using SPSS, version 25, core perinatal outcomes were analyzed, including outcomes for mothers and newborns transferred after admission in labor. Distinct processes of care were summarized, and a preliminary exploration of racial disparities was conducted. A descriptive analysis of socio‐demographic and medical characteristics of the sample was compared with publicly available national birth certificate data.14 For variables that are not collected or reported in birth certificate data, other national sources were chosen as a point of reference such as CDC Perinatal Risk Assessment Monitoring System (PRAMS),15 Centers for Medicare and Medicaid Services,16 and Centers for Disease Control and Prevention's National Immunization Survey.17 The AABC PDR research protocol has been ruled exempt by New England IRB as research involving the study of existing data and recorded in such a manner that participants cannot be identified directly or through identifiers linked to the participants.
3. RESULTS
The sample includes data from all 6424 Medicaid beneficiaries enrolled for care in 45 AABC Strong Start practices in 19 states between 2013 and 2017. No participating birth centers were excluded from the sample; all sites had complete data, defined as no more than 5% incomplete records. Missing data for each variable were excluded before calculating percentages.
3.1. Socio‐demographic characteristics
The AABC sample has a socio‐demographic profile similar to that of total US birth certificate data during the study time period (Table 1).14, 15 Compared with national data, women in the AABC sample had slightly more births to teen mothers (7.8% vs 5.4%), and fewer births to mothers aged 35 and older (9.0% vs 17.0%). The AABC sample had more unmarried women (52.6% vs 39.8%), whereas educational status was similar between the two groups. Women within the AABC sample mirrored US percentages of Hispanic and Native American ethnicity and were less likely to be Asian or Pacific Islander (1.5% vs 7.6%) or non‐Hispanic black (11.9% vs 14.2%), compared with national data. Ethnicity was not a mandatory field when the study began; thus, the number of records with missing data for this variable was a limitation.
Table 1.
Socio‐demographic and risk characteristics for the American Association of Birth Centers Strong Start Sample—2013‐2017, compared with nationally reported data
|
AABC Strong Start births N = 6424a n (%) |
National datab
N = 3 945 875 n (%) |
|
|---|---|---|
| Socio‐demographic characteristics | ||
| Age | ||
| <20 | 502 (7.8) | 212.062 (5.4) |
| 20‐34 | 5342 (83.2) | 3 064 142 (77.7) |
| 35+ | 580 (9.0) | 669 671 (17.0) |
| Unmarried | 3379 (52.6) | 1 569 796 (39.8) |
| High school degree/GED or higher | 5489 (85.5) | 3 401 344 (86.2) |
| Race/ ethnicity | ||
| Non‐Hispanic white | 2362 (56.2) | 2 056 332 (52.1) |
| Hispanic | 1169 (23.2) | 918 447 (23.3) |
| Non‐Hispanic black | 764 (11.9) | 558 622 (14.2) |
| American Indian or Alaskan Native | 65 (1.0) | 43 555 (1.1) |
| Asian or Pacific Islander | 94 (1.5) | 302 283 (7.6) |
| Medical risk factors | ||
| History of depression | 678 (10.6) | 4273 (10.5)c |
| History of previous preterm birth | 365 (5.7) | 122 042 (3.1) |
| Pre‐pregnancy BMI | ||
| Overweight (BMI 25.0‐29.9) | 1603 (25.8) | 997 615 (26.0) |
| Obese (BMI >30.0) | 1492 (24.0) | 1 001 452 (26.1) |
| Psychosocial risk factors | ||
| Interval since last live birth <18 mo | 334 (5.2) | 35.839 (1.6) |
| Unplanned or unwanted pregnancy | 2207 (34.4) | 11 607 (34.2)c |
| Smoking | 766 (11.9) | 284 103 (7.2) |
| Domestic violence | 252 (3.9) | 855 (2.1)c |
Missing data were excluded before percentages were computed.
Martin, Hamilton, Osterman, Driscoll, & Drake, Final Birth Data for 2016, 2018.
CDC, Centers for Disease Control, nd.
Compared with national data for the same time period, women in the AABC sample had similar psychosocial and behavioral risk factors. Women in the AABC sample were more likely to have a history of preterm birth, smoking, and a history of domestic violence. The most common psychosocial risk factors were unplanned or unwanted pregnancy (34.4%), smoking (11.9%), chronic stress (11.0%), history of depression (10.6%), and interpregnancy interval between viable pregnancies <18 months (5.2%), all of which have been linked to increased risk of preterm birth. National data show that about 3.0% of pregnant Medicaid beneficiaries reported illicit drug use in the past month.18 In the AABC sample, 318 (5.0%) reported current illicit drug use on presentation to prenatal care.
3.2. Core perinatal outcomes
When we examined perinatal outcomes, the Medicaid beneficiaries in the AABC Strong Start sample exceeded national benchmarks for several perinatal quality indicators (Table 2).14, 17, 19, 20 Preterm birth and low‐birthweight rates were less than half those in national data, 4.4% vs 9.9% and 3.7% vs 8.2%, respectively. The total cesarean birth rate was 12.3%, less than half the national rate (31.9%), and the primary cesarean rate was 8.7% compared to a national rate of 21.8%. The nulliparous, term, singleton, vertex (NTSV) cesarean rate in the AABC sample was 14.7%, compared with a rate of 25.7% in the national data and a Healthy People 2020 target of 23.9%.21
Table 2.
Perinatal quality indicators for the American Association of Birth Centers Strong Start Sample—2013‐2017, compared with nationally reported data
| Perinatal quality indicator |
AABC Strong Start births N = 6424a n (%) |
National datab
N = 3 945 875 n (%) |
|---|---|---|
| Total induction of labor | 1052 (16.4) | 967 811 (24.5) |
| Primary cesarean | 558 (8.7) | 860 200 (21.8) |
| Total cesarean | 792 (12.3) | 1 258 734 (31.9) |
| Nulliparous term singleton vertex cesarean | 328 (14.7) | 1 014 090 (25.7) |
| Low birthweight | 232 (3.7) | 322 377 (8.2) |
| Exclusive breastfeeding at discharge | 5107 (87.0) | 41.5c |
| Any breastfeeding at discharge | 5453 (92.9) | 3 279 022 (83.1) |
| Exclusive breastfeeding at 1 mo | 3149 (65.7) | 10 090 (59.1)d |
| Any breastfeeding at 1 mo | 4224 (88.1) | 13 511 (79.0)d |
| NICU admission all newborns | 182 (2.9) | 344 454 (8.7) |
| NICU admission newborns >2500 g | 116 (1.8) | 4.3%e |
| Postpartum contraception | 3457 (85.1) | 40 641 (78.4)d |
Missing data were excluded before percentages were computed.
Martin et al, Final Birth Data for 2016, 2018.
National Quality Forum, 2012.
CDC, Centers for Disease Control, 2017.
Harrison & Goodman, 2015.
The AABC Strong Start participants had excellent breastfeeding outcomes, a marker for life course health of both the mother and baby (Table 2). Overall, 5106 (87.0%) AABC Strong Start mothers were exclusively breast milk feeding at discharge, compared to 41.5% in the last national report of this endorsed quality metric.19 Similarly, 92.9% of AABC Strong Start participants reported feeding “any” breast milk at the time of discharge from the birth facility, compared to 83.1% nationally.14 At discharge, 415 newborns (6.5%) were exclusively formula feeding and 347 (1.3%) of newborns received formula supplementation. This compares favorably with Healthy People 2020 targets of 81.9% of infants who are ever breastfed and 14.2% of newborns receiving formula supplementation within the first two days of life.17 These favorable breastfeeding rates persisted at 4‐6 weeks, with 65.7% of AABC Strong Start mothers still exclusively breastfeeding and 88.1% reporting any breastfeeding.
3.3. Care use patterns
To better understand high leverage characteristics of the model that may be responsible for improved clinical outcomes, we examined the care use patterns within the AABC Strong Start sample (Table 3).14, 23, 24, 25, 26, 27 Notably, the use of midwives as primary care providers in the population was different from nationally reported patterns during the study period. The majority of Medicaid beneficiaries within the AABC Strong Start sample experienced midwifery‐led prenatal care (95.9%) and midwife‐attended birth (64.5%). During this same time period, physicians attended 89.7% of births nationwide.14
Table 3.
Selected process of care variables for the American Association of Birth Centers Strong Start Sample—2013‐2017, compared with nationally reported data
| Effective care variables |
AABC Strong Start N = 6424 n (%)a |
National data N = 3 945 875b n (%) |
|---|---|---|
| Adequacy of prenatal care | ||
| Attended prenatal care in 1st trimesterc | 4551 (81.7) | 1 111 526 (68.1)d |
| Adequate plus prenatal care (APNCU Index)c | 4210 (68.0) | 526 639 (32.5)d |
| Primary provider for prenatal care | ||
| Nurse‐midwife/certified midwife | 4942 (76.9) | – |
| Certified professional midwife or licensed midwife | 1218 (19.0) | – |
| Physicianc | 264 (4.1) | 75.7e |
| Care in labor | ||
| Intermittent auscultation only | 2735 (42.6) | 264 (11.0)f |
| Epidural analgesia in labor | 942 (29.1) | 2 901 486 (73.5) |
| Primary attendant for birth | ||
| Certified nurse‐midwife/certified midwife | 3495 (54.4) | 389 892 (8.5) |
| Certified professional midwife or licensed midwife | 649 (10.1) | 32 841 (0.8) |
| Physician | 1989 (31.0) | 3 572 527 (89.7) |
| Place of birth | ||
| Hospital | 3374 (52.5) | 3 883 255 (98.4) |
| Birth center | 2797 (43.5) | 19 767 (0.5) |
| Planned homeg | 176 (2.7) | 38 830 (1.0) |
| En route or unplanned home | 77 (1.2) | |
| Postpartum care | ||
| Attended postpartum visitc | 5479 (85.5) | 54%h |
Missing data were excluded before percentages were computed.
Martin, et. Al. Final Birth Data for 2016, 2018.
Women with Medicaid or CHIP as source of payment.
Osterman & Martin, 2018.
Uddin, Simon, & Myrick, 2014.
Declercq, et al, 2013.
Planned and unplanned home births are not distinguished in all state birth certificate data.
Centers for Medicare & Medicaid Services, 2017.
The model demonstrated early use and access to prenatal care with 81.7% presenting to care in the first trimester, compared to 68.1% reported in national data for mothers whose source of payment was Medicaid.23 Six sites had <70% of their clients presenting for care in first trimester. The Healthy People 2020 target for first‐trimester presentation to prenatal care is 77.9%. Eighty‐nine (1.6%) of AABC Strong Start participants first presented to prenatal care in third trimester, in contrast to 8.6% of Medicaid recipients nationally with late or no prenatal care.23 Mothers presenting with no prenatal care are not appropriate for birth center care in labor, and a few birth centers do not enroll mothers presenting for care in third trimester.
The AABC Strong Start sites demonstrated notably different patterns of resource use regarding prevalence of hospitalization among Medicaid beneficiaries. Among 4278 mothers intending to give birth at home or at a birth center in third trimester, 3179 (74.3%) were admitted to their intended site in labor, and 2797 (65.4%) gave birth without being hospitalized. A total of 17.7% of women who had planned a birth center or home birth were admitted to or transferred to the hospital during labor. Of mothers admitted to birth center or home, 381 (8.9%) required transfer to the hospital during labor. Another 377 (8.8%) of mothers planning to give birth at home or in the birth center required transfer to hospital care when they were first evaluated on presentation in labor. The findings regarding site of birth contrast with the predominant model of care during this time period in which 98.5% of US births occurred in hospitals.14
Use of the appropriate level of care is further demonstrated by fetal surveillance in labor in which nearly half (42.6%) experienced intermittent auscultation as the sole form of fetal surveillance after admission in labor. In Listening to Mothers III: New Mothers Speak Out, 89% of women reported that their fetus was monitored using an electronic fetal monitor either continuously (66%) or intermittently in combination with a handheld device (23%).26 This is in contrast to research demonstrating intermittent auscultation as the appropriate level of care for medically low‐risk childbearing women.28
Overall, 182 (2.8%) AABC Strong Start newborns were admitted to neonatal intensive care unit (NICU), compared to a national rate of 8.7%.14 Among newborns ≥2500 g, 116 (1.8%) experienced NICU admission. Strong Start newborns were almost twice as likely to be admitted to NICU after a hospital birth (1.2%) than after a birth center birth (0.7%), possibly reflecting the conditions that prompted either a planned hospital birth or transfer to the hospital from the birth center during labor. The rate of NICU admissions in a US population‐based study for newborns ≥2500 g was 4.3%.20
Finally, length of stay is relatively short in the AABC Strong Start sample, with 2839 (57.4%) of mother/newborn dyads staying 24 hours or less; 759 (15.4%) mothers remained longer than 48 hours after a vaginal birth and 333 (6.7%) longer than 72 hours after a cesarean birth. A population study of new mothers in California reports a median length of stay of 2 days for mothers experiencing a vaginal birth.29 The close follow‐up of families in the birth center model, with over 30% receiving at least one home visit after discharge, provides ongoing care and screening after discharge, contributing to few readmissions of mother (1.1%) or newborn (1.9%).
3.4. Racial and ethnic disparities
The preterm birth rate for white, non‐Hispanic women within the AABC sample was 4.2% compared to 9.0% in national data. Preterm birth for non‐Hispanic black women within the AABC sample was 5.1%, less than one‐half of the national rate (13.8%), showing a narrowing in racial disparity for this measure (Table 4).14 Low birthweight and cesarean birth occurred at lower rates compared with national data, but with persisting racial disparities (Table 4). Non‐Hispanic black women enrolled in the AABC Strong Start program experienced cesarean at less than one‐half of the national rate (15.1% vs 35.9%), whereas non‐Hispanic white women had a cesarean birth rate of 10.6% compared to 30.9% nationally.
Table 4.
National quality indicators by race and ethnicity for the American Association of Birth Centers Strong Start Sample—2013‐2017, compared with nationally reported data
|
AABC Strong Start N = 6424 n (%)a |
United States birthsb
N = 3 945 875 n (%) |
|
|---|---|---|
| All races and ethnicities | 6424 (100) | 3 945 875 (100) |
| White, non‐Hispanic | 2362 (56.2) | 2 056 332 (52.1) |
| Hispanic | 1169 (23.2) | 918 447 (23.2) |
| Black, non‐Hispanic | 764 (11.9) | 558 622 (14.2) |
| Low birthweight | ||
| All races and ethnicities | 232 (3.7) | 321 838 (8.2) |
| White, non‐Hispanic | 31 (1.3) | 143 254 (7.0) |
| Hispanic | 13 (2.9) | 67 210 (7.3) |
| Black, non‐Hispanic | 45 (5.9) | 76 299 (13.7) |
| Preterm birth <37 wk | ||
| All races and ethnicities | 284 (4.4) | 388 218 (9.9) |
| White, non‐Hispanic | 99 (4.2) | 185 854 (9.0) |
| Hispanic | 32 (7.0) | 86 691 (9.5) |
| Black, non‐Hispanic | 39 (5.1) | 76 834 (13.8) |
| Cesarean birth | ||
| All races and ethnicities | 792 (12.3) | 1 258 581 (31.9) |
| White, non‐Hispanic | 250 (10.6) | 635 558 (30.9) |
| Hispanic | 61 (13.4) | 290 832 (31.7) |
| Black, non‐Hispanic | 115 (15.1) | 200 460 (35.9) |
| Ever breastfed c | ||
| All races and ethnicities | 5453 (92.2) | 17 673 (83.2) |
| White, non‐Hispanic | 1787 (91.0) | 9907 (85.9) |
| Hispanic | 321 (91.2) | 3723 (84.6) |
| Black, non‐Hispanic | 632 (89.1) | 1607 (69.4) |
Missing data were excluded before percentages were computed.
Martin, et al, Final Birth Data for 2016, 2018.
CDC National Immunization Survey, 2009‐2015.
Consistent with national data, racial and ethnic disparities were also noted in breastfeeding rates. Among non‐Hispanic black mothers, 559 (78.8%) were exclusively breastfeeding at discharge, with 315 (59.1%) of non‐Hispanic black mothers exclusively breastfeeding at 6 weeks postpartum and 449 (84.2%) providing some breast milk. Despite disparities within the AABC Strong Start beneficiaries, breastfeeding rates in the AABC sample were consistently higher than available national rates for all races and ethnicities, with 83.2% US overall, 85.9% white, non‐Hispanic, 84.6% Hispanic, and 69.4% non‐Hispanic black mothers reporting having ever breastfed their infant.17
4. DISCUSSION
From 2013 to 2017, 6424 Medicaid beneficiaries enrolled in prenatal care in AABC Strong Start birth centers and giving birth with the birth center midwives or their collaborative physicians in birth center, hospital, and home. Strong Start enrollees exhibited a similar socio‐behavioral risk profile to mothers giving birth in the United States during the study period, with enrollees experiencing slightly higher rates of tobacco use, domestic violence, chronic stress, and drug use. Outcomes achieved in birth centers suggest that similar outcomes could be achieved nationwide with spread and scale of this enhanced care model. The AABC model demonstrated lower rates of induction of labor, low birthweight, preterm birth, and cesarean birth than rates reported nationally. The outcomes demonstrate higher success with health protective factors, like breastfeeding, and a narrowing of health disparities, which warrants further evaluation. Breastfeeding rates at 6 weeks are lower among mothers who are Medicaid beneficiaries, as were all Strong Start participants, as compared with commercial payers, with one study reporting rates of 30.2.% exclusive breastfeeding and 48.4% any breastfeeding at 6‐8 weeks postpartum.22
Racial disparities are known to exist in outcomes among childbearing mothers, with institutional racism understood to be a factor.39 Analysis of AABC Strong Start data by the Urban Institute demonstrated that birth center prenatal care was associated with lower rates of preterm birth, low birthweight, and cesarean delivery for non‐Hispanic black and Hispanic women.2, 3 These disparity reductions were confirmed using comparison groups of Medicaid beneficiaries with similar risk levels receiving usual care. More research is needed to better understand the potential for the model to reduce racial and ethnic disparities in birth outcomes.
Enhanced prenatal care provided by birth centers achieved excellent outcomes that warrant regulation and reimbursement reform to facilitate increased access. The processes of care and outcomes require a notably different workforce composition with different workflows than traditional prenatal care. The high leverage components of enhanced birth center care, such as midwifery‐led care, peer counselor support, longer provider visits, and facilitated educational sessions, require reliable funding mechanisms. This requires a shift away from payment for procedures, which is known to drive cost and decrease quality. Steps toward the transformation of the current system outlined in the Blueprint for Advancing High‐Value Maternity Care through Physiologic Childbearing include improving access to birth center care by reducing various regulatory barriers.30 Developing sustainable reimbursement by Medicaid for time‐intensive care is recommended.
Increased investment in birth center model prenatal care will lead to significant cost savings with healthier mothers and infants. Strong Start care in birth centers demonstrates substantial cost savings, with lower cesarean rates and fewer medical interventions, and when prenatal care is provided by the birth center, reductions in preterm, and low‐birthweight births.2, 3 The estimate of Medicaid savings from the cesareans prevented per 10 000 births is $4.35 million.8 Estimated savings reduction in preterm births prevented per 10 000 births is $24.25 million.40 Higher rates of breastfeeding and lower rates of NICU admissions also contribute to cost savings from this care.20, 32 Cost savings are also affected by shorter length of stay for both mother and newborn, with 57.4% of mother/newborn dyads staying <24 hours.
The processes of care and outcomes for socially at‐risk Medicaid beneficiaries were markedly different than those nationally reported. Comparative effectiveness research is feasible using CMMI Strong Start data as other arms of the study included traditional medical settings that were physician‐led. The current system of high‐tech care drives high cost and poor quality.30, 31, 32, 33, 34, 35, 36, 37, 38 The midwifery‐led wellness model of care provided within birth center practices continues to demonstrate improved outcomes. System‐level accountability to the preferences of Medicaid beneficiaries is an important step to ensuring a safe, family‐centered maternity care system.
4.1. Strengths and limitations
This is a descriptive study of the demographics, processes, and outcomes of women participating in Strong Start with prenatal care provided in birth centers, compared with national data. Strengths of the study include a relatively large sample, geographic diversity of birth centers collecting data, and a sample with demographic and psychosocial risk profile similar to that of the national population of childbearing mothers. Data were collected by care providers during course of care, with findings from the previous validation study and the consistency of data across sites suggesting that the data are reliable.13 The design of the data collection platform, with users unable to submit the data form unless required variables are completed, results in minimal missing data for all key variables.
To best inform public policy, risk‐adjusted analysis, using propensity scoring and weighted comparative effectiveness research through the Center for Medicare and Medicaid Innovation, needs to be conducted because it best controls for medical risk factors while quantifying care use, outcomes, and cost. Although this sample population was more diverse and had more risk factors than populations in previous large observational studies of birth center care, selection bias of those choosing to enroll in prenatal care at a Strong Start birth center may make the AABC sample different from national birth certificate data in ways that have an impact on outcomes. More research is needed on women's choices about where they receive maternity care and plan to give birth. This should include research on lower‐risk women who choose hospital birth. Comparison of breastfeeding data is limited by the fact that the nationally endorsed quality measure of exclusive breastfeeding is not reported in birth certificate data for the study period.
4.2. Conclusions
The AABC birth center model provides primary maternity care appropriate for Medicaid beneficiaries nationwide. This study demonstrates that the model can serve a socio‐demographically diverse population with significant social risks while improving perinatal outcomes. Continued expansion of access to the birth center model of care among childbearing Medicaid beneficiaries offers promise in improving population health, mothers’ experience of care, and the value of care.
HHS‐DISCLAIMER
The project described was supported by Funding Opportunity Number CMS‐1D1‐12‐001 from the Centers for Medicare & Medicaid Services, Center for Medicare & Medicaid Innovation. The contents do not necessarily represent the official views of HHS or any of its agencies. This project does not limit a fee‐for‐service Medicare, Medicaid, or CHIP patient's freedom to choose a particular health care provider.
ACKNOWLEDGMENTS
The authors wish to thank the women who enrolled in Strong Start, all of the birth centers that participated in this study, and American Association of Birth Centers Foundation for their ongoing support of research of enhanced care in the birth center. We thank Ruth and Bill Lubic who work tirelessly to improve access to birth center care for more mothers who are Medicaid beneficiaries.
Biographies
Jill Alliman was Project Director for the AABC Strong Start for Mothers and Newborns Initiative. She teaches Master's and Doctoral students at Frontier Nursing University.
Susan R. Stapleton is the former Chair of the AABC Research Committee and Data Coordinator for AABC Strong Start for Mothers and Newborns Initiative.
Jennifer Wright is AABC Perinatal Data Registry™ (PDR) Manager, and was Research Associate for Strong Start for Mothers and Newborns Initiative.
Kate Bauer is the Executive Director of the American Association of Birth Centers.
Kate Slider is the Associate Director of the American Association of Birth Centers and was Sites Coordinator for the AABC Strong Start for Mothers and Newborns Initiative.
Diana Jolles is the Chair of the Research Committee for the American Association of Birth Centers and is a current contributor to the PDR™ registry.
Alliman J, Stapleton SR, Wright J, Bauer K, Slider K, Jolles D. Strong Start in birth centers: Socio‐demographic characteristics, care processes, and outcomes for mothers and newborns. Birth. 2019;46:234–243. 10.1111/birt.12433
Funding information
Research Funding Source: Funding was awarded to American Association of Birth Centers, Inc. for Strong Start for Mothers and Newborns Initiative, to conduct research on freestanding birth center care as a model of enhanced prenatal care. Funding #1D1CMS331135‐04‐01 from February 2013 to July, 2017. Writing Funding Source: Funding came from a grant from the American Association of Birth Centers Foundation to support writing time for this manuscript in 2018.
REFERENCES
- 1. Markus AR, Andres E, West KD, Garro N, Pellegrini C. Medicaid covered births, 2008 through 2010, in the context of the implementation of health reform. Womens Health Issues. 2013;23(5):e273‐e280. [DOI] [PubMed] [Google Scholar]
- 2. Hill I, Dubay L, Courtot B, et al. Strong start for mothers and newborns evaluation: year 5 project synthesis, Vol 1. https://downloads.cms.gov/files/cmmi/strongstart-prenatal-finalevalrpt-v1.pdf. Updated 2018. Accessed September 2, 2018.
- 3. Hill I, Dubay L, Courtot B, et al. Strong start for mothers and newborns evaluation: year 5 project synthesis, Vol 2. Awardee‐Specific Reports. https://downloads.cms.gov/files/cmmi/strongstart-prenatal-finalevalrpt-v2.pdf. Updated 2018. Accessed September 2, 2018.
- 4. Jolles DR, Langford R, Stapleton S, Cesario S, Koci A, Alliman J. Outcomes of childbearing Medicaid beneficiaries engaged in care at strong start birth center sites between 2012 and 2014. Birth. 2017;44(4):298‐305. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Sandall J, Soltani H, Gates S, Shennan A, Devane D. Midwife‐led continuity models versus other models of care for childbearing women. Cochrane Database Syst Rev. 2015;9:CD004667. [DOI] [PubMed] [Google Scholar]
- 6. Alliman J, Phillippi JC. Maternal outcomes in birth centers: an integrative review of the literature. J Midwifery Womens Health. 2016;61(1):21‐51. [DOI] [PubMed] [Google Scholar]
- 7. Phillippi JC, Danhausen K, Alliman J, Phillippi RD. Neonatal outcomes in the birth center setting: a systematic review. J Midwifery Womens Health. 2018;63(1):68‐89. [DOI] [PubMed] [Google Scholar]
- 8. Stapleton SR, Osborne C, Illuzzi J. Outcomes of care in birth centers: demonstration of a durable model. J Midwifery Womens Health. 2013;58(1):3‐14. [DOI] [PubMed] [Google Scholar]
- 9. Rooks JP, Weatherby NL, Ernst E, Stapleton S, Rosen D, Rosenfield A. Outcomes of care in birth centers: the National Birth Center study. N Engl J Med. 1989;321(26):1804‐1811. [DOI] [PubMed] [Google Scholar]
- 10. Benatar S, Garrett AB, Howell E, Palmer A. Midwifery care at a freestanding birth center: a safe and effective alternative to conventional maternity care. Health Serv Res. 2013;48(5):1750‐1768. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Howell E, Palmer A, Benatar S, Garrett B. Potential Medicaid cost savings from maternity care based at a freestanding birth center. Medicare Medicaid Res Rev. 2014;4(3):E1‐E13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Gliklich RE, Dreyer NA, Leavy MB. Registries for evaluating patient outcomes: a user’s guide. [Agency for Healthcare Research and Quality Report No. 13]. https://www.ncbi.nlm.nih.gov/books/NBK208616/. Updated 2014. Accessed April 28, 2019. [PubMed]
- 13. Stapleton SR. Validation of an online data registry for midwifery practices: a pilot project. J Midwifery Womens Health. 2011;56(5):452‐460. [DOI] [PubMed] [Google Scholar]
- 14. Martin JA, Hamilton BE, Osterman MJK, Driscoll AK, Drake P. Births: final data for 2016 [National Vital Statistics Report 67(1)]. https://www.cdc.gov/nchs/data/nvsr/nvsr67/nvsr67_01.pdf. Updated 2018. [PubMed]
- 15. Centers for Disease Control . Prevalence of selected maternal and child health indicators for all PRAMS sites: Pregnancy Risk Assessment Monitoring System (PRAMS): 2012‐2015. https://www.cdc.gov/prams/pramstat/pdfs/mch-indicators/PRAMS-All-Sites-2012-2015-508.pdf. Updated n.d. Accessed September 2, 2018.
- 16. Centers for Medicare & Medicaid Services . Quality of care for adults in Medicaid: finding from the 2016 Adult Core Set – Chart Pack. https://www.medicaid.gov/medicaid/quality-of-care/downloads/performance-measurement/2017-adult-chart-pack.pdf. Published 2017. Updated 2017. Accessed May 21, 2018.
- 17. Centers for Disease Control and Prevention . Breastfeeding among U.S. children born 2009–2015: CDC National Immunization Survey. https://www.cdc.gov/breastfeeding/data/nis_data/rates-any-exclusive-bf-socio-dem-2015.htm. Updated 20172018.
- 18. Center for Behavioral Health Statistics and Quality . 2016 national survey on drug use and health: detailed tables. Substance Abuse and Mental Health Services Administration. https://www.samhsa.gov/data/sites/default/files/NSDUH-DetTabs-2016/NSDUH-DetTabs-2016.pdf. Updated 2017. Accessed September 2, 2018.
- 19. National Quality Forum . Perinatal and reproductive health: endorsement maintenance technical report. http://www.qualityforum.org/Publications/2012/06/Perinatal_and_Reproductive_Health_Endorsement_Maintenance.aspx. Updated 2012. Accessed March 21, 2019.
- 20. Harrison W, Goodman D. Epidemiologic trends in neonatal intensive care, 2007–2012. JAMA Pediatr. 2015;169(9):855‐862. [DOI] [PubMed] [Google Scholar]
- 21. Centers for Disease Control and Prevention . Healthy people 2020 midcourse review, Chapter 26. Centers for Disease Control and Prevention Web site. https://www.cdc.gov/nchs/data/hpdata2020/HP2020MCR-C26-MICH.pdf. Published January 11, 2017. Updated January 11, 2017. Accessed February 14, 2019.
- 22. Mercier RJ, Burcher TA, Horowitz R, Wolf A. Differences in breastfeeding among Medicaid and commercially insured patients: a retrospective cohort study. Breastfeed Med. 2018;13(4):286‐291. [DOI] [PubMed] [Google Scholar]
- 23. Osterman M, Martin JA. Timing and adequacy of prenatal care in the United States, 2016. Natl Vital Stat Rep. 2018;67(3):1‐14. [PubMed] [Google Scholar]
- 24. Uddin SG, Simon AE, Myrick K. Routine prenatal care visits by provider specialty in the United States, 2009‐2010. https://www.cdc.gov/nchs/data/databriefs/db145.pdf. Updated 2014. Accessed September 2, 2018. [PubMed]
- 25. Declercq ER, Sakala C, Corry MP, Applebaum S, Herrlich A. Listening to mothers™ III: pregnancy and birth [Report of the third national U. S. Survey of Women’s childbearing experiences]. http://transform.childbirthconnection.org/wp-content/uploads/2013/06/LTM-III_Pregnancy-and-Birth.pdf. Updated 2013. Accessed February 6, 2019
- 26. Declercq ER, Sakala C, Corry MP, Applebaum S, Herrlich A. Listening to mothers III: new mothers speak out. New York: Childbirth Connection, June 2013. https://transform.childbirthconnection.org/wp-content/uploads/2013/06/LTM-III_NMSO.pdf. Accessed April 1, 2019.
- 27. Centers for Medicare and Medicaid Services . Prenatal and postpartum care: postpartum care [scorecard by state 2014‐2015]. https://www.medicaid.gov/state-overviews/scorecard/state-health-system-performance/communication-and-coordination/prenatal-postpartum/index.html. Updated n.d. Accessed February 6, 2019.
- 28. Devane D, Lalor JG, Daly S, McGuire W, Cuthbert A, Smith V. Cardiotocography versus intermittent auscultation of fetal heart on admission to labour ward for assessment of fetal wellbeing. Cochrane Database Syst Rev. 2017;(1):CD005122 10.1002/14651858.CD005122.pub5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Sakala C, Declercq ER, Turon JM, Corry MP. Listening to mothers in California: a population‐based survey of women's childbearing experiences. https://chcf.org/wp-content/uploads/2018/09/ListeningMothersCAFullSurveyReport2018.pdf. Updated 2018. Accessed February 6, 2019.
- 30. Avery MD, Bell AD, Bingham D, et al. Blueprint for advancing high‐value maternity care through physiologic childbearing. http://www.nationalpartnership.org/our-work/resources/health-care/maternity/blueprint-for-advancing-high-value-maternity-care.pdf. Updated 2018. Accessed February 6, 2019. [DOI] [PMC free article] [PubMed]
- 31. Kennedy HP, Kozhimannil KB, Sakala C. Using the blueprint for advancing high‐value maternity care for transformative change. Birth. 2018;45(4):331‐335. [DOI] [PubMed] [Google Scholar]
- 32. Bartick MC, Jegier BJ, Green BD, Schwarz EB, Reinhold AG, Stuebe AM. Disparities in breastfeeding: impact on maternal and child health outcomes and costs. J Pediatr. 2017;181:49‐55.e6. [DOI] [PubMed] [Google Scholar]
- 33. Kozhimannil KB, Muoto I, Darney BG, Caughey AB, Snowden JM. Early elective delivery disparities between non‐Hispanic black and white women after statewide policy implementation. Womens Health Issues. 2018;28(3):224‐231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Attanasio L, Kozhimannil KB. Relationship between hospital‐level percentage of midwife‐attended births and obstetric procedure utilization. J Midwifery Womens Health. 2018;63(1):14‐22. [DOI] [PubMed] [Google Scholar]
- 35. Kozhimannil KB, Law MR, Virnig BA. Cesarean delivery rates vary tenfold among US hospitals; reducing variation may address quality and cost issues. Health Aff. 2013;32(3):527‐535. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Miller S, Abalos E, Chamillard M, et al. Beyond too little, too late and too much, too soon: a pathway towards evidence‐based, respectful maternity care worldwide. Lancet. 2016;388(10056):2176‐2192. [DOI] [PubMed] [Google Scholar]
- 37. Morton CH, Henley MM, Seacrist M, Roth LM. Bearing witness: United States and Canadian maternity support workers’ observations of disrespectful care in childbirth. Birth. 2018;45(3):263‐274. [DOI] [PubMed] [Google Scholar]
- 38. Shaw D, Guise J, Shah N, et al. Drivers of maternity care in high‐income countries: can health systems support woman‐centred care? Lancet. 2016;388(10057):2282‐2295. [DOI] [PubMed] [Google Scholar]
- 39. Alhusen JL, Bower KM, Epstein E, Sharps P. Racial discrimination and adverse birth outcomes: an integrative review. J Midwifery Womens Health. 2016;61(6):707‐720. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Institute of Medicine (IOM) and National Research Council (NRC) , ed. An Update on Research Issues in the Assessment of Birth Settings: Workshop Summary . Washington, DC: The National Academies Press; 2013. [PubMed] [Google Scholar]