

Abstract
Objective
Angle stable interlocking intramedullary nail (ASIN), a novel technique, has rarely been used for treatment of tibial plateau fractures (TPF). This retrospective study was designed to introduce this novel technique, ASIN, as well as to describe the initial experience and verify the effectiveness when ASIN was used for the management for TPF.
Methods
A cohort of 19 cases with closed TPF aged from 18–70 years with at least 23 months follow‐up from November 2008 to September 2013 was analyzed retrospectively. All patients underwent the ASIN procedure, which was performed by the same group of surgeons. Perioperative and postoperative parameters like the measurement of radiographic pictures, surgical data, and clinical function were recorded including the changes in treatment. A modified Hohl–Luck radiological and functional score combined with the Hospital for Special Surgery (HSS) score were applied to evaluate the final results and to provide reliable data through the whole procedure when applying the ASIN procedure.
Results
The patients were followed up regularly for an average of 26.3 (range, 23–34) months. All patients achieved a bony union at an average of 15.1 weeks with no incidences of malunion, nonunion, or infection. Anatomical reduction of the articular surface was obtained in 16 patients. No secondary failure of fixation occurred. The mean postoperative knee flexion was 122.9°. The modified Hohl–Luck radiological and functional score was excellent and good, respectively, in 16 patients. The mean HSS score was 89.4.
Conclusion
The angle stable interlocking intramedullary nail system turned out to be a viable alternative protocol in the treatment of tibia plateau fractures and provided satisfactory results, with good fracture reduction, biomechanical fixation, low rates of complications, and passable postoperative knee function.
Keywords: Intra‐articular fracture, Intramedullary nailing, Plateau fracture, Tibia
Introduction
Tibial plateau fractures (TPF) are commonly high‐energy injuries that have been estimated to account for 1.2% of all fractures1. These fractures often involve instability, compressive articular surface, and severe soft‐tissue injury. The surgical treatment of these fractures continues to remain a challenge for most surgeons.
Several methods, including open reduction and internal fixation (ORIF), minimally invasive percutaneous plate osteosynthesis (MIPPO), and external fixation, have been described for the management of TPF, and each technique has both advantages and disadvantages2, 3, 4. However, the fracture patterns and the associated complications have contributed to contradictory results regarding the optimal treatment. Currently, ORIF with plates and screws is the most commonly used method in the management for TPF5. Nevertheless, this method exhibits disadvantages of secondary damage to soft tissues and devascularizing the fracture site, increasing the risk of infection, and exposing the implant. In addition, the plate–screw fixation cannot maintain the position of the fragment effectively, leading to the failure of replacement and implant2.
The intramedullary nail (IMN) has the advantages of decreasing the soft‐tissue disruption as well as preventing the plate prominence in patients with a poor soft‐tissue envelope, and, thus, has become the gold standard of diaphyseal fracture management6, 7, 8, 9. However, IMN is technically challenging in patients with metaphyseal fractures. With the updates in design, the indications of IMN have been extended to tibia metaphyseal fractures, as well as intra‐articular fractures10, 11, 12, 13. Garnavos and Lasanianos14, 15 and Lasanianos et al.16 reported on the IMN available in TPF. In these studies, a proposal implementing intramedullary nailing and compression bolts for the management of selected complex fractures of the tibial plateau was presented. Furthermore, Garnavos and Lasanianos14,15 suggests that the proposed technique could be biomechanically advantageous. In comparison to other traditional techniques this biomechanical study was confirmed.
The tibial locked intramedullary nail is suitable for tibial shaft fracture fixation, but there are technical difficulties in relation to the proximal tibial fracture. The postoperative reduction loss rate was 58% to 84%17. The first reason for this is there are few locking holes in the proximal part of the tibial locked intramedullary nail and there is no multi‐direction locking function. The second reason is that there is no “angular stability” between the main nail and the locking nail, and the locking nail itself does not have the effect of cancellous bone locking screws. In addition, in the case of intraarticular fractures, on the basis of restrictive locking fixation, non‐restrictive elastic screw fixation is needed, which is “raft” nail fixation, so that intraarticular fractures could be converted to extraarticular fractures. With the recognition of the “angle stability” technique between the primary nail and the locking nail, a biomechanical study on the cadaveric bone shows that the mechanical effect of tibial intramedullary nail fixation on the metaphysis fracture is better than that of plate screw fixation.
This is a retrospective study that describes the initial experience and verifies the effectiveness of the newly‐designed angle stable interlocking intramedullary nail (ASIN) combined with higher‐threaded cancellous screws in the management of type‐B/C (AO/OTA classification) TPF. The purpose of this study was: (i) to introduce the newly designed intramedullary implant, the ASIN; and (ii) to assess the clinical effect of the ASIN used in the management of type‐B/C TPF.
Materials and Methods
Patients
Inclusion and Exclusion Criteria
With approval of the Institutional Review Board and in accordance with the Declaration of Helsinki in ethical standards, this retrospective study of patients who met the following inclusion criteria was performed: (i) age between 18 and 70 years at the time of injury; (ii) fresh and closed TPF (AO/Schatzker classification); (iii) treated with ASIN; and (iv) available follow‐up records of at least 23 months postoperatively. Exclusion criteria were as follows: (i) severe cognitive dysfunction which may have hindered postoperative rehabilitation; (ii) history of previous knee surgery on either side; (iii) severe articular comminution, neurovascular injuries and pathologic fracture; (iv) concomitant fractures of other areas; and (v) absence of independent walking capability prior to trauma. Informed consent was obtained from all participants included in the study.
Baseline Data
A cohort of 19 cases with closed TPF treated by the new method, ASIN, from November 2008 to September 2013 was analyzed retrospectively. Perioperative and postoperative parameters like the measurement of radiographic pictures, surgical data, and clinical function were recorded including the changes in treatment. The primary outcome measures were the modified Hohl–Luck radiological and function score and the hospital for special surgery (HSS) functional score.
Treatment
Introduction of Angle Stable Interlocking Intramedullary Nail
All fractures were treated by the ASIN system that was performed by the same group of orthopedic surgeons. The ASIN (Fig. 1) was designed for tibial shaft fractures as well as metaphyseal fractures, TPF, and pilon fractures11. The system consisted of nails and non‐restrictive and restrictive screws. Based on the anatomical morphology, an 8° radius of the proximal end (80 mm) eased the insertion and extraction of the nail and provided optimal stability for the TPF. For proximal locking, four options were possible: two oblique options with thread for locking screws located at 18 and 24 mm from the proximal end, respectively, thereby providing the locking function in proximity to the locking plate and the other two mediolateral locking options at the far proximal end. Two kinds of locking screws, known as restrictive screws, are used in ASIN: cancellous bone lag locking screws with a gentle slope and cancellous bone locking screws with a higher thread. The other locking screws, known as the non‐restrictive screws, which are cancellous bone lag locking screws, are excluded from ASIN.
Figure 1.

Multiple locking options in different planes and locking screws at the proximal end of angle stable interlocking intramedullary nail (ASIN). a Restrictive screws cancellous bone locking screws with a gentle slope. b Restrictive screws cancellous bone locking screws with higher thread.
Surgical Technique
The patient is placed in a supine position with the ability to bring the affected knee to >100° of flexion. In the case of 2 patients with minimal intra‐articular displacement, a closed reduction was used. A straight parapatellar incision was fashioned in 6 patients with bicondylar fractures with severe displacement. In 11 cases, a medial or lateral oblique incision facilitated reduction. All fractures were classified according to the AO11/Schatzker et al.18 classification. The fracture was reduced temporarily with pointed reduction forceps, manual pressure, or Kirschner wires, followed by the usage of 1–2 non‐restrictive screws to fix the medial and lateral condylar according to the AO dogma: the C‐type fractures have to be converted to the A‐type fractures (Fig. 2). Positioning of the non‐restrictive screw was followed by the fixation of IMN. To provide maximum support and fixation strength, all proximal locking screws must be inserted. In addition, 1–2 non‐restrictive screws were used, if necessary, to improve the strength of fixation. None of the interlocking screws were applied to the distal nail in all cases except for 1 patient who also presented with tibia shaft fractures. We used non‐reamed nails.
Figure 2.
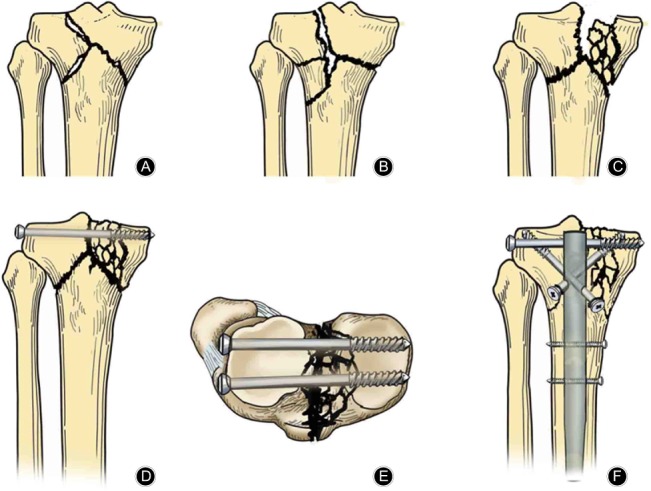
Diagram of reduction and internal fixation of C‐type tibial plateau fractures. (A–C) Preoperative morphology of C‐type tibial plateau fracture (A: C1‐type, B: C2‐type, C: C3‐type). (D, E) After reduction and leveling of tibial plateau fracture, the front (D) and upper (E) view of internal joint fracture were fixed by a “raft” type of cancellous screw, turning C‐type fracture into A‐type fracture. (F) Installation of angle stable interlocking intramedullary nail (ASIN), enabling the fixation of large fracture pieces with restrictive cancellous tension nailing while supporting the non‐restrictive cancellous pull screw. The main nail of ASIN, the restrictive high thread locking nail, the restrictive cancellous bone tension locking nail and the unrestrictive cancellous bone tension screw together form the jail technique 3‐D fixation.
Postoperative Management
We used a hinged external fixation brace to support the affected limb and to maintain the alignment immediately after surgery. All patients received antibiotic prophylaxis within 24 h postoperatively. The active and passive motion of the toes’ flexion–extension and isometric contraction of the quadriceps was initiated on day 1. All patients were advised to non‐weight‐bear with the assistance of crutches within 1 week. Active painless knee flexion–extension functional exercise started at 2–3 weeks, progressing to partial‐weight‐bearing at 12 weeks, followed by full‐weight‐bearing subsequently.
All patients underwent radiographical and clinical follow‐up at 1, 4, and 12 weeks until the fracture was healed, every 6 months, and then, before and after the removal of the nail. The clinical functions and radiological evaluation in patients with TPF were estimated using the modified Hohl–Luck score (Tables 1, 2)19. The malunion was defined as a loss of fracture reduction, resulting in >3 mm articular step‐off or varus/valgus malalignment >5°20. The functional outcomes were evaluated by the HSS functional score21 (range, 0–100 points) at the latest follow‐up. A score from 85–100 was considered excellent, 70–84 good, 60–69 fair, and 0–59 poor.
Table 1.
Modified Hohl–Luck score system (functional grading used in the evaluation)
| Grades | Lack of extension (degrees) | Range of movement (degrees) | Valgus or varus instability (degrees) | Walking distance (m) | Pain |
|---|---|---|---|---|---|
| Excellent (all of the following) | 0 | ≥120 | <5 | ≥3000 | None |
| Good (not more than one of the following) | >0 | <90 | >5 | <1000 | Mild on activity |
| Fair (not more than two of the following) | ≥10 | <75 | >5 | <100 | Moderate on activity or intermittent at rest |
| Poor | All results worse than fair | ||||
Table 2.
Modified Hohl–Luck score system (radiographical grading used in the evaluation)
| Grade | Valgus/varus deformity (degrees) | Depression of articular surface (mm) | Osteoarthritis |
|---|---|---|---|
| Excellent (all of the following) | ≤5 | <5 | None |
| Good (not more than one of the following) | >5 | >5 | Minimal |
| Fair (not more than two of the following) | >10 | >5 | Moderate |
| Poor | All results worse than fair | ||
Statistical Analysis
The normally distributed quantitative variables were presented as the means ± standard deviations and analyzed by Student's t test. The non‐normally distributed quantitative data were presented as medians with interquartile ranges and analyzed using the Wilcoxon rank‐sum test. The enumeration variables were presented as absolute numbers with percentages and analyzed using the χ2 and Fisher exact tests. The significance was set at P < 0.05. The statistical analysis was conducted using SPSS software (version 17.0; SPSS, USA).
Results
The patients were followed up regularly for an average of 26.3 (range, 23–34) months. The patients’ variables are listed in (Appendix I). All patients achieved a bony union within an average duration of 15.1 (range, 12–20) weeks. The operative parameters included a mean operation time of 105 (range, 60–150) min and a mean estimated blood loss of 115.3 (range, 30–250) mL. All patients were treated using ASIN combined with 1–2 non‐restrictive locking screws.
Nevertheless, the complications were minimal. Seven patients exhibited swelling and drainage of operation incision, requiring periodic dressing. These patients healed without other complications. One patient presented a loss of alignment into 20° varus during healing. None of the cases displayed any infection, non‐union, stiffness, and nail and screw fracture.
Modified Hohl–Luck Radiological Score
The radiological score was excellent in 11 (57.9%) patients, good in 5 (26.3%), fair in 2 (10.5%), and poor in 1 (5.3%) patient. Anatomical reduction of the articular surface was obtained in 16 (84.2%) patients. Three (15.8%) patients showed a step‐off <3 mm. Seventeen (89.5%) patients showed good alignment, and 1 (%) showed a varus malalignment of <5°. In contrast, 1 (5.3%) patient exhibited a malalignment >15°, which was due to ignoring the doctor's advice against leaving bed and walking until 1 week postoperatively. Eight patients presented post‐traumatic arthritis; of these, 4 patients were diagnosed with osteoarthritis preoperatively. Figs 2C and D show the radiographs of patients treated with the ASIN presenting good radiological outcome.
Modified Hohl–Luck Functional Score
Ten patients had an excellent score, 6 good, 1 fair, and 2 poor. None of the patients either showed instability at the follow‐up or had an extension lag. The average knee flexion was 122.9°, and the range of movement varied from 70° to 145°. Two patients exhibited a flexion range < 110°, 6 experienced slight pain while walking and climbing stairs, whereas 2 acknowledged moderate pain during similar activities.
Hospital for Special Surgery Score
At the final follow‐up, the mean HSS score was 89.4 (range, 64–97). The HSS score was >85 points in 13 (68.4%) patients, 70–84 in 5 (26.3%), and 60–69 in 1 (5.3%) patient. The rate of excellent and good was 94.7%.
Discussion
In this study, we described an alternative technique of ASIN for the management of TPF. Furthermore, we compared the outcomes to the fracture reduction and the rate of complications presented in the literature using the ORIF method with one or two plates. The 17 (89.5%) patients in this series satisfied with the therapeutic effect returned to their normal routine. The ASIN technique demonstrated similar or superior advantages with respect to stability and complications.
In recent years, the indication for the use of the IMN was expanded to the treatment of TPF10, 14, 15. This advanced technique of the ASIN system involves multi‐directional locking options in different planes at the proximal end. The tight fit between the locking screws and the nail has angular stability and a locking function that enhances the stability of fracture fragments. Owing to the modified designs described above, the ASIN system has advantages similar to or greater than the plates while managing the TPF. Several biomechanical studies have shown that IMN combined with free screws fixed TPF, thereby demonstrating an elastic behavior and an absolute stability similar to or greater than to the plates16, 22. In addition, non‐restrictive screws were inserted to fix the intra‐articular fracture fragments in all patients. The positions and orientations of the screws were random such that they would not interfere with ASIN and the insertion of locking screws. These screws in combination with restrictive screws function similarly to the jail technique23, 24, which prevents the secondary loss of reduction and enhances the stability of the fracture fragments. Simultaneously, if the non‐restrictive screw is tangent to the nail, it also functions as the poller screw25. All these design modifications might allow an alternative technique for the treatment of TPF.
Anterior knee pain and motion limitation are common complications following intramedullary nailing of tibial shaft fractures. In our experience, the precise nail tip position is more than 5.5 mm from the tibial plateau and more than 2.5 mm from the tibial tuberosity26.
The anatomical reconstruction and alignment are critical issues in the treatment of TPF, and the quality is associated with obtaining an adequate clinical outcome27. Previously, the rate of malunion among TPF via ORIF ranged from 9.1% to 20%28. Reportedly, the malreduction occurs in 15%–23% of TPF via the LISS (less invasive stabilization system) plating system29, 30. In this study, 16 (84.2%) patients achieved excellent and good results according to the modified Hohl–Luck radiological score; only 1 patient presented a malunion. None of the patients exhibited non‐union, stiffness, or implant failures, and 18 (94.7%) patients achieved excellent and good rates of HSS. Moreover, a majority of malalignments and articular step‐offs with this new technique were acceptable20, and they had a similar or greater advantage in maintaining alignment and stability as compared to ORIF. Thus, ASIN ensures that the alignment can be maintained and stability can be preserved.
Soft tissue complications pose a serious issue in the treatment of TPF. ORIF with one or two plates often involves extensive exposure of soft tissue of the fracture site. In addition, severe soft‐tissue injury is an adverse factor in soft tissue complications. The literature demonstrates that the rate of infection among TPF treated with ORIF ranges from 4.7% to 14.2%31. In recent years, MIPPO has become widely accepted as the operative treatment of choice for TPF, with satisfactory early results. Reportedly, the rate of infection of TPF treated with LISS was between 3.7% and 13.3%32, 33, 34. Cole et al. reviewed 77 patients with or without intra‐articular tibial proximal fractures treated with LISS and reported infection in 4% patients35. IMN is a minimally invasive treatment method and can adequately resolve the issue of extensive soft‐tissue stripping. The infection rate was lower after IMN as compared to the plates36. In our series, most patients were treated by open reduction; however, none of the patients exhibited any infection. In this study, the sole aim of incision was reduction without any dissection.
Despite comparable results to the literature in the treatment of ORIF via plates, our study was not without its limitations. First, the ASIN technique has its limitations for optional dynamization of the nail in the non‐union shaft cases. We can improve the design of the ASIN, which could have a dynamization hole at the end of the nail. The proximal locking screws in the nail have just four directions, which are not enough to fix all the fractured fragments. Second, the small number of cases were treated via IMN and the data collected in a retrospective manner were subject to bias. However, this is a novel technique for TPF. Thus, a prospective, randomized trial or even a prospective, randomized, case‐comparative study is essential to evaluate the efficacy of this treatment. Third, we could not assess the condition of post‐traumatic arthritis, and surgeons may require extensive experience with the IMN technique to obtain good clinical outcomes15.
In conclusion, the new ASIN technique provides excellent reduction and fixation and permits good results in the treatment of TPF. Therefore, we consider this technique as a viable alternative protocol for the fixation of the TPF.
Supporting information
Appendix I Preoperative and postoperative profile of the patients (n = 19).
Additional appendix may be found in the online version of this article on the publisher's web‐site:
Appendix I Preoperative and postoperative profile of the patients (n = 19).
Disclosure: The authors declare that they have no competing interests.
References
- 1. Ariffin HM, Mahdi NM, Rhani SA, Baharudin A, Shukur MH. Modified hybrid fixator for high‐energy Schatzker V and VI tibial plateau fractures. Strategies Trauma Limb Reconstr, 2011, 6: 21–26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Phisitkul P, McKinley TO, Nepola JV, Marsh JL. Complications of locking plate fixation in complex proximal tibia injuries. J Orthop Trauma, 2007, 21: 83–91. [DOI] [PubMed] [Google Scholar]
- 3. Stevens DG, Beharry R, McKee MD, Waddell JP, Schemitsch EH. The long‐term functional outcome of operatively treated tibial plateau fractures. J Orthop Trauma, 2001, 15: 312–320. [DOI] [PubMed] [Google Scholar]
- 4. Stamer DT, Schenk R, Staggers B, Aurori K, Aurori B, Behrens FF. Bicondylar tibial plateau fractures treated with a hybrid ring external fixator: a preliminary study. J Orthop Trauma, 1994, 8: 455–461. [PubMed] [Google Scholar]
- 5. Biggi F, Di Fabio S, D'Antimo C, Trevisani S. Tibial plateau fractures: internal fixation with locking plates and the MIPO technique. Injury, 2010, 41: 1178–1182. [DOI] [PubMed] [Google Scholar]
- 6. Schmidt AH, Finkemeier CG, Tornetta P 3rd. Treatment of closed tibial fractures. Instr Course Lect, 2003, 52: 607–622. [PubMed] [Google Scholar]
- 7. Drosos GI, Bishay M, Karnezis IA, Alegakis AK. Factors affecting fracture healing after intramedullary nailing of the tibial diaphysis for closed and grade I open fractures. J Bone Joint Surg Br, 2006, 88: 227–231. [DOI] [PubMed] [Google Scholar]
- 8. Bhandari M, Guyatt GH, Swiontkowski MF, et al Surgeons' preferences for the operative treatment of fractures of the tibial shaft. An international survey. J Bone Joint Surg Am, 2001, 83: 1746–1752. [DOI] [PubMed] [Google Scholar]
- 9. Bhandari M, Guyatt GH, Swiontkowski MF, Schemitsch EH. Treatment of open fractures of the shaft of the tibia. J Bone Joint Surg Br, 2001, 83: 62–68. [DOI] [PubMed] [Google Scholar]
- 10. Kuhn S, Hansen M, Rommens PM. Extending the indications of intramedullary nailing with the Expert Tibial Nail. Acta Chir Orthop Traumatol Cech, 2008, 75: 77–87. [PubMed] [Google Scholar]
- 11. Hansen M, ElAttal R, Blum J, Blauth M, Rommens PM. Intramedullary nailing of the tibia with the expert tibia nail. Oper Orthop Traumatol, 2009, 21: 620–635. [DOI] [PubMed] [Google Scholar]
- 12. Kubiak EN, Camuso MR, Barei DP, Nork SE. Operative treatment of ipsilateral noncontiguous unicondylar tibial plateau and shaft fractures: combining plates and nails. J Orthop Trauma, 2008, 22: 560–565. [DOI] [PubMed] [Google Scholar]
- 13. Nork SE, Barei DP, Schildhauer TA, et al Intramedullary nailing of proximal quarter tibial fractures. J Orthop Trauma, 2006, 20: 523–528. [DOI] [PubMed] [Google Scholar]
- 14. Garnavos C, Lasanianos NG. The management of complex fractures of the proximal tibia with minimal intra‐articular impaction in fragility patients using intramedullary nailing and compression bolts. Injury, 2011, 42: 1066–1072. [DOI] [PubMed] [Google Scholar]
- 15. Garnavos C. Retropatellar nailing and condylar bolts for complex fractures of the tibial plateau: technique, pilot study and rationale. Injury, 2014, 45: 1099–1104. [DOI] [PubMed] [Google Scholar]
- 16. Lasanianos NG, Garnavos C, Magnisalis E, Kourkoulis S, Babis GC. A comparative biomechanical study for complex tibial plateau fractures:nailing and compression bolts versus modern and traditional plating. Injury, 2013, 44: 1333–1339. [DOI] [PubMed] [Google Scholar]
- 17. Eastman J, Tseng S, Lo E, Li CS, Yoo B, Lee M. Retropatellar technique for intramedullary nailing of proximal tibia fractures: a cadaveric assessment. J Orthop Trauma, 2010, 24: 672–676. [DOI] [PubMed] [Google Scholar]
- 18. Schatzker J, McBroom R, Bruce D. Tibial plateau fracture. Clin Orthop, 1979, 138: 94–104. [PubMed] [Google Scholar]
- 19. Fracture and dislocation compendium. Orthopaedic Trauma Association Committee for Coding and Classification. J Orthop Trauma, 1996, 10 (Suppl. 1): v–ix 1–154. [PubMed] [Google Scholar]
- 20. Jensen DB, Rude C, Duus B, Bjerg‐Nielsen A. Tibial plateau fractures. A comparison of conservative and surgical treatment. J Bone Joint Surg Br, 1990, 72: 49–52. [DOI] [PubMed] [Google Scholar]
- 21. Ali AM, El‐Shafie M, Willett KM. Failure of fixation of tibial plateau fractures. J Orthop Trauma, 2002, 16: 323–329. [DOI] [PubMed] [Google Scholar]
- 22. Insall JN, Ranawat CS, Aglietti P, Shine J. A comparison of four models of total knee‐replacement prostheses. J Bone Joint Surg Am, 1976, 58: 754–765. [PubMed] [Google Scholar]
- 23. Hogel F, Hoffmann S, Panzer S, Wimber J, Buhren V, Augat P. Biomechanical comparison of intramedullar versus extramedullar stabilization of intra‐articular tibial plateau fractures. Arch Orthop Trauma Surg, 2013, 133: 59–64. [DOI] [PubMed] [Google Scholar]
- 24. Weimann A, Heinkele T, Herbort M, Schliemann B, Petersen W, Raschke MJ. Minimally invasive reconstruction of lateral tibial plateau fractures using the jail technique: a biomechanical study. BMC Musculoskelet Disord, 2013, 14: 120. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Doht S, Lehnert T, Frey S, et al Effective combination of bone substitute and screws in the jail technique: a biomechanical study of tibial depression fractures. Int Orthop, 2012, 36: 2121–2125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Daraboš N, Banić T, Lubina Z, Daraboš A, Bilić V, Sabalić S. Precise nail tip positioning after tibial intramedullary nailing prevents anterior knee pain. Int Orthop, 2013, 37: 1527–1531. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Krettek C, Stephan C, Schandelmaier P, Richter M, Pape HC, Miclau T. The use of Poller screws as blocking screws in stabilising tibial fractures treated with small diameter intramedullary nails. J Bone Joint Surg Br, 1999, 81: 963–968. [DOI] [PubMed] [Google Scholar]
- 28. Marsh JL, Buckwalter J, Gelberman R, et al Articular fractures: does an anatomic reduction really change the result?. J Bone Joint Surg Am, 2002, 84: 1259–1271. [PubMed] [Google Scholar]
- 29. Lee MH, Hsu CJ, Lin KC, Renn JH. Comparison of outcome of unilateral locking plate and dual plating in the treatment of bicondylar tibial plateau fractures. J Orthop Surg Res, 2014, 9: 62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Gosling T, Schandelmaier P, Muller M, Hankemeier S, Wagner M, Krettek C. Single lateral locked screw plating of bicondylar tibial plateau fractures. Clin Orthop Relat Res, 2005, 439: 207–214. [DOI] [PubMed] [Google Scholar]
- 31. Gosling T, Schandelmaier P, Marti A, Hufner T, Partenheimer A, Krettek C. Less invasive stabilization of complex tibial plateau fractures: a biomechanical evaluation of a unilateral locked screw plate and double plating. J Orthop Trauma, 2004, 18: 546–551. [DOI] [PubMed] [Google Scholar]
- 32. Choo KJ, Morshed S. Postoperative complications after repair of tibial plateau fractures. J Knee Surg, 2014, 27: 11–19. [DOI] [PubMed] [Google Scholar]
- 33. Cole PA, Zlowodzki M, Kregor PJ. Less invasive stabilization system (LISS) for fractures of the proximal tibia: indications, surgical technique and preliminary results of the UMC clinical trial. Injury, 2003, 34(Suppl. 1): A16–A29. [DOI] [PubMed] [Google Scholar]
- 34. Schutz M, Kaab MJ, Haas N. Stabilization of proximal tibial fractures with the LIS‐system: early clinical experience in Berlin. Injury, 2003, 34(Suppl. 1): A30–A35. [DOI] [PubMed] [Google Scholar]
- 35. Stannard JP, Wilson TC, Volgas DA, Alonso JE. Fracture stabilization of proximal tibial fractures with the proximal tibial LISS: early experience in Birmingham, Alabama (USA). Injury, 2003, 34 (Suppl. 1): A36–A42. [DOI] [PubMed] [Google Scholar]
- 36. Cole PA, Zlowodzki M, Kregor PJ. Treatment of proximal tibia fractures using the less invasive stabilization system: surgical experience and early clinical results in 77 fractures. J Orthop Trauma, 2004, 18: 528–535. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Appendix I Preoperative and postoperative profile of the patients (n = 19).