

Abstract
Background
Impairments in social cognition have been described in several psychiatric and neurological disorders. Given the importance of the relationship between social cognition and functioning and quality of life in these disorders, there is a growing interest in social cognition remediation interventions. The aim of this study was to carry out a systematic mapping review to describe the state of the art in social cognition training and remediation interventions.
Methods
Publications from 2006 to 2016 on social cognition interventions were reviewed in four databases: Scopus, PsycINFO, PubMed and Embase. From the initial result set of 3229 publications, a final total of 241 publications were selected.
Results
The study revealed an increasing interest in social cognition remediation interventions, especially in the fields of psychiatry and psychology, with a gradual growth in the number of publications. These were frequently published in high impact factor journals and underpinned by robust scientific evidence. Most studies were conducted on schizophrenia, followed by autism spectrum disorders. Theory of mind and emotional processing were the focus of most interventions, whilst a limited number of studies addressed attributional bias and social perception. Targeted interventions in social cognition were the most frequent practice in the selected papers, followed by non-specific treatment interventions and broad-based interventions.
Conclusions
Research in social cognition remediation interventions is growing. Further studies are needed on attributional bias and social perception remediation programs, while the comparative efficacy of different interventions also remains unclear.
Introduction
Social cognition refers to the mental operations involved in social interactions, including processes of perceiving, interpreting, and generating responses to the intentions, dispositions, and behaviors of others [1–6]. Social cognition is a key determinant of the proper functioning and development of human beings. Although various disorders, such as autism [7–9], affective disorders [10–13] and eating disorders [14], have been associated with deficits in social cognition, schizophrenia has frequently been the focus of investigation in social cognition [15–17]. The fact that schizophrenia acquired an early paradigmatic position in psychiatry might partly explain this. Nevertheless, some pragmatic reasons may also be identified: (a) A significant number of patients with schizophrenia present deficits in quality of life and functioning; (b) There is an early onset of these deficits and they persist throughout life; (c) The personal, familiar and economic burden of this disorder is very high. (d) Social cognition impairments appear to make an important contribution to deficits in quality of life and functioning [7,18–21].
The last decade has seen a significant increase in research on social cognition and the strategies for its pharmacological and psychosocial treatment. A recent systematic mapping review of pharmacological interventions in social cognition deficits [22] shows an increase in the number of publications, with a significant number studying hypothalamic hormones (especially oxytocin), with a much less frequent focus on antipsychotics, amphetamines, and sex hormones, in that order.
Several non-pharmacological approaches designed to enhance social cognition abilities have also been developed. Some treatment interventions approach social cognition as a unitary construct, but emphasis has recently been placed on a multidimensional structure of social cognition. Initiatives such as the Social Cognition Psychometric Evaluation (SCOPE) study have defined social cognition as a multidimensional construct that includes four core domains: emotional processing, social perception, attributional style/bias, and theory of mind [23–25]. In this sense, specific remediation interventions have been developed to improve each of the domains of social cognition, either as the main intervention of the program, or as part of a broader training program targeting a variety of dimensions of the illness. Finally, other psychosocial interventions which do not specifically target social cognition, such as social skills training [26–27], have been shown to have a positive impact on social cognition.
Although several reviews have focused on the usefulness of different social cognition remediation interventions [28–31], to our knowledge, no prior systematic mapping review has examined social cognition remediation programs. A systematic mapping review is a secondary empirical study that provides an overview of the state of the art in a field, identifying venues and topics addressed in the literature. Furthermore, this type of review is a systematic approach to understanding the “map” of a field of knowledge, research question, or practice [32], by identifying linkages rather than results [33]. The presence of this type of study in different fields of medicine has increased, especially in recent years, although systematic mapping reviews are still scarce in psychiatry [34–38].
The aim of the present study was to describe the state of the art in social cognition remediation interventions following a systematic mapping review approach, to provide researchers and clinicians with a global picture on social cognition remediation interventions for psychiatric and other medical conditions.
Methods
Research methodology
Research interest
The present mapping review has been conducted for several reasons. The first is to perform a broad analysis of the literature on social cognition remediation interventions, with the aim of providing an overview of existing proposals according to a classification criterion. The second is, if possible, to identify existing research gaps in social cognition rehabilitation intervention programs to plan future research, while the third is to identify topics and areas for future systematic literature reviews focused on smaller research areas.
The steps described in the Template for a Mapping Study Protocol [39–40] were followed to conduct this study. A mapping review protocol includes three distinct phases: (a) Research directives defines the study protocol and identifies the dimensions to be analyzed and the research questions to be answered. (b) Data collection gathers relevant papers in accordance with the inclusion and exclusion criteria defined in the protocol. Finally, (c) Results maps the existing literature in line with the defined criteria and answers the research questions. Note that the PRISMA checklist [41] has not been used in this paper as it does not in fact fit recommendations for systematic mapping studies. Therefore, a checklist for the Template for a Mapping Study Protocol is provided in S1 Table (see supplementary material online).
Research directives
In this section, the definition of the research protocol and the description of the research questions is presented. The protocol included the study topic (social cognition remediation interventions); its rationale (previously mentioned); preliminary research questions; and search strategy, selection criteria, and data extraction form. Finally, the protocol included an overview of selected papers in terms of their publication venues and years.
The four research questions (RQ) for this systematic mapping review and their rationale were:
RQ1. How many papers have been published on social cognition remediation interventions? Is there any temporal trend? What is their level of scientific evidence?
As previously discussed, deficits in social cognition are commonly found in psychiatric disorders such as autism, depressive disorder, bipolar disorder, and schizophrenia. Due to the prevalence and/or severity of these disorders, and the limited efficacy of pharmacological interventions [42–43], the number of papers published on non-pharmacological social cognition remediation interventions was studied. Second, the possible presence of a temporal trend (increasing or decreasing) was analyzed. Finally, the study of their level of scientific evidence provided complementary information regarding the quality of published studies.
RQ2. In what areas of medical knowledge and related disciplines has research on social cognition remediation programs been conducted?
Deficits in social cognition are not exclusive to psychiatric disorders. Several neurological disorders such as behavioral-variant frontotemporal dementia [44], traumatic brain injury [45], or Parkinson’s disease [46] are characterized by impairments in social cognition [47]. Other disorders with central nervous system involvement such as tuberous sclerosis [48], fragile X syndrome [49], Prader Willi syndrome [50], or Wilson’s disease [51] have also been related to social cognition impairments. Therefore, it seems interesting to study which areas of knowledge are developing research on social cognition remediation, including medicine and related fields such as psychology and neuroscience.
RQ3. Which domains of social cognition are the focus of research in social cognition remediation?
Social cognition is considered a multidimensional construct. There is some consensus regarding critical domains of social cognition as four partially overlapping domains (theory of mind/mental state attribution, social perception, attributional bias/style, and emotional processing) [24–25]:
Theory of mind is defined as the ability to recognize intentions, dispositions, and beliefs in oneself and others [52]. Theory of mind includes understanding special ways of communication, such as hints, deception, metaphors or irony, by making inferences about the feelings of others, beliefs, and intentions, and/or by representing human mental states [53–54]. Theory of mind is also known as mentalizing, mental state attribution, or cognitive empathy [55].
Social perception consists of the ability to identify social rules, roles, and goals [56–57]. Social perception is also defined as the ability to correctly interpret the behaviors of other people by means of context and social information [58–59].
Attributional bias/style describes the way in which individuals explain or interpret different social facts or infer the causes of social events [3]. Attributions are external (to others) or internal (to oneself) and may be categorized further by dimensions such as ambiguity of the context or positive vs. negative outcome.
Emotional processing refers to the ability to perceive, recognize and manage emotional information [3]. Emotional processing is also defined as the ability to identify, facilitate, regulate, understand and manage emotions [60–61].
Interventions on social cognition remediation may be focused on one or several social cognition domains. Thus, identifying the most frequently studied domains will help researchers recognize the domains that might need further investigation.
RQ4. What types of interventions are employed in social cognitive remediation?
Although various forms of interventions may potentially improve social cognition, three main types of training and remediation interventions have been distinguished [31]:
Targeted interventions specifically directed at improving one or more domains of social cognition. Targeted interventions are often subcategorized, including “targeted” and “comprehensive” interventions. “Targeted” refers to brief interventions for a single aspect of social cognition. “Comprehensive” refers to programs that leverage all the elements of an extended training program in order to improve multiple domains of social cognition, typically including practice for the generalization of acquired skills for everyday life. Notice that the present work does not provide this subclassification.
Broad-based interventions, including social cognition training in a broader approach oriented towards improving social cognition, neurocognition and/or social skills.
Non-specific interventions, which do not target social cognition but may produce a positive effect on one or more of its domains.
Classifying published papers according to three main types of interventions facilitates an overview of the specificity of the interventions in social cognition remediation.
Data collection
With the aim of including relevant and excluding irrelevant papers, the search strategy of this study involved querying reference databases with customized search strings, followed by manual filtering of the query results using predefined inclusion and exclusion criteria. Five researchers were involved in executing the search strategy.
Source selection and search string
To minimize the risk of missing relevant papers on social cognition remediation, four reference databases were queried: Scopus (Elsevier), PsycINFO (American Psychological Association), PubMed (American Psychological Association) and Embase (Elsevier).
The keywords for the search string were identified by following mainly research questions RQ3 and RQ4. The first part of the search string was composed of words related to social cognition, using the nomenclature described under RQ3, while the second part included remediation and its synonyms (rehabilitation, therapy, training, treatment and enhancement) related to the types of interventions deduced from RQ4. Finally, all items in our search string were interleaved with or/and statements, to make sure that all relevant papers were retrieved. The final search string was: ("affect perception" OR "affect recognition" OR “attributional bias” OR "attributional style" OR “emotional processing” OR "emotion recognition" OR "mentalizing" OR "theory of mind" OR "social cognition" OR “social perception”) AND (“rehabilitation” OR “remediation” OR “therapy” OR “treatment” OR “training” OR “enhancement”). It should be highlighted that no truncation was used in the terms of the final search string for the following reasons: First, not all reference databases enable this option, and using it would drastically deviate the number of records obtained of some database in comparison to others. Second, in the case of Scopus database, for instance, the number of initial results would become intractable (around 27,000 records). In each reference database, the complete string was queried in the title, abstract, and keywords fields.
Inclusion and exclusion criteria
The selection criteria of published studies comprised the following inclusion and exclusion criteria:
- Inclusion criteria:
- I1. Papers focusing on social cognition deficits and their treatment.
- I2. Papers published between January 1, 2006, and December 31, 2016.
- I3. Papers focusing on social cognition training and remediation interventions.
- Exclusion criteria:
- E1. Grey literature, because of their unclear peer review process: editorials, extended abstracts, tutorials, tool demos, doctoral symposium papers, research abstracts, book chapters, proceedings, keynote talks, workshop reports, and technical reports.
- E2. Systematic reviews (including meta-analyses) and survey papers were not considered eligible for inclusion. We were only interested in first-hand experimental research work.
- E3. Papers from venues other than medicine, psychology, neuroscience and/or biomedicine (e.g. agriculture, environmental sciences, business, veterinary, physics, earth sciences, economy, and energy).
- E4. Papers not related to research with human subjects.
- E5. Papers based on pharmacological interventions for social cognition deficits.
Inclusion criterion I2 deserves an explanation. It is usual to consider publications published within the last ten in similar systematic mapping studies. Therefore, we started our study with publications from 2006, which provided around 150 papers as the starting point of the search. Moreover, there are two reasons to end the study in 2016. First, systematic mappings study complete years, and it is not feasible to close a year before the third quarter of the following one, mainly due to delays inherent to data management in search engines. Thus, work on the study was started during the final months of 2017. Second, performing this systematic mapping study was a vast task that continued into 2018.
In relation to exclusion criterion E1, let us highlight that it does not limit the potential to determine interest in the topic, as we have verified the same tendency in the growth of the number of publications including and excluding grey literature. For the under study, grey literature represents around 22% of annual publications.
Search process
The steps described in Fig 1 were followed for the process of extracting and selecting articles. The search string was used on each of the four reference databases. After merging the references from each database and implementing the filters on the papers (according to inclusion and exclusion criteria), a total of 3571 papers were obtained. After eliminating repeated articles (n = 342), two researchers filtered the remaining 3229 papers independently through the screening of title, abstract and keywords. If the researcher was unsure whether to include a paper, the introduction and conclusion sections of the full content paper were read. If, despite this, the researcher was still not sure, or there was no agreement between the two researchers, the paper was presented to the other researchers and the clinical coordinator of the study for discussion and a consensus decision. This step resulted in 1233 references.
Fig 1. Steps for the process of extracting and selecting articles.

At this point, the 1233 references were filtered again by the same two researchers, who independently screened the full content of each paper. As in the preceding step, when a researcher was unsure whether to keep or remove a paper, or there was no agreement between the two researchers, the paper was presented in another session for discussion and a final decision. This step thus produced the final set of 241 references. To ensure that no references were missed during the process, a series of earlier [62–63] and more recent review papers [30–31,64], including a highly recent systematic literature review [65] were carefully studied. A full-text screening of all these papers revealed no undiscovered publications.
Results
A final number of 241 papers (see on-line material, S1 File for a complete list of selected papers) were extracted following the previously described process. Here, the four previously presented research questions will be answered with reference to the selected literature.
RQ1. How many papers have been published on social cognition remediation interventions? Is there any temporal trend? What is their level of scientific evidence?
As shown in Fig 2A, over the period of study, an increase was observed in the number of published papers on social cognition remediation and training programs. There was an overall progressive increase from 2006, growing from 9 papers published in 2006, to 45 papers in 2016. The greatest increase in the number of published papers was found over the last four years.
Fig 2.

(a) Number of selected papers over publication years. (b) Number of references per year and level of scientific evidence.
An overview of selected papers in terms of their level of scientific evidence provided data regarding the quality of published studies. As defined by the US Agency for Healthcare Research and Quality [66], 106 references presented IB level of evidence (evidence obtained from at least one randomized clinical trial), and 41 papers presented IIA level (obtained from at least one well-designed, non-randomized controlled prospective study). Among the remaining references, 50 studies were classified as IIB (scientific evidence obtained from at least one well-designed, quasi-experimental study), while 29 papers presented III level of evidence (well-designed observational studies). The remaining 15 papers were classified as IV (documents or opinions of expert committees and/or clinical experiences of key opinion leaders). An increase in the number of published papers on social cognition remediation and training programs with IB level of evidence was seen in the period studied, as can be seen in the IB trend line (see Fig 2B).
Regarding publication venues, Schizophrenia Research journal was the most popular venue, with 19 papers, followed by Journal of Autism and Developmental Disorders with 10 papers, Psychiatry Research with 8 published papers, Behavioural and Cognitive Psychotherapy with 7 papers, PLoS ONE with 6 papers, Schizophrenia Bulletin with 5 papers, and BMC Psychiatry and Developmental Psychology with 4 papers each. Each of the remaining journals had 3 or fewer published papers (see on-line material, S2 Table for a complete list).
RQ2. In what areas of medical knowledge and related disciplines has research on social cognition remediation programs been conducted?
According to the area of knowledge of the publishing journal, 132 of the 241 included papers were published in journals classified as related to medicine. As shown in Table 1, papers on medicine were mostly in the field of psychiatry, according to the EUMS (European Union of Medical Specialists) (89 papers of a total of 132 in medical specialties). Other areas of knowledge were child and adolescent psychiatry and psychotherapy (22 papers), neurology (6 papers), physical medicine and rehabilitation (6 papers), and public health medicine (4 papers).
Table 1. References by EUMS medical specialties.
| EUMS Medical Specialty | Ref. |
|---|---|
| Psychiatry | P5, P6, P10, P16, P23, P24, P26, P30, P31, P32, P34, P36, P39, P40, P43, P44, P45, P46, P47, P48, P59, P60, P61, P62, P63, P64, P65, P67, P70, P71, P73, P79, P80, P83, P84, P86, P93, P94, P100, P101, P102, P103, P104, P109, P110, P112, P113, P117, P121, P122, P130, P131, P132, P133, P136, P140, P143, P144, P146, P148, P149, P153, P156, P158, P159, P161, P164, P172, P179, P181, P185, P186, P189, P191, P192, P202, P204, P206, P209, P212, P215, P225, P226, P230, P231, P232, P237, P238, P240 |
| Child and Adolescent Psychiatry and Psychotherapy | P7, P8, P11, P12, P13, P18, P19, P52, P77, P81, P107, P116, P123, P124, P125, P155, P194, P201, P208, P216, P219, P235 |
| Neurology | P2, P76, P145, P157, P165, P171 |
| Physical Medicine and Rehabilitation | P1, P50, P174, P183, P199, P218 |
| Public Health Medicine | P25, P126, P227, P241 |
| Geriatrics | P120 |
| Laboratory Medicine / Medical Biopathology | P198 |
| Pediatrics | P90 |
| Non-Specific | P51, P99 |
Furthermore, as can be seen in Table 2, according to the area of knowledge of the publishing journal, the second most frequent studied knowledge area after medicine was psychology, which included 93 papers. The remaining 16 papers were included in science, neuroscience, and education journals.
Table 2. References by journal knowledge area.
| Knowledge Area | Ref. |
|---|---|
| Medicine | P1, P2, P5, P6, P7, P8, P10, P11, P12, P13, P16, P18, P19, P23, P24, P25, P26, P30, P31, P32, P34, P36, P39, P40, P43, P44, P45, P46, P47, P48, P50, P51, P52, P59, P60, P61, P62, P63, P64, P65, P67, P70, P71, P73, P76, P77, P79, P80, P81, P83, P84, P86, P90, P93, P94, P99, P100, P101, P102, P103, P104, P107, P109, P110, P112, P113, P116, P117, P120, P121, P122, P123, P124, P125, P126, P130, P131, P132, P133, P136, P140, P143, P144, P145, P146, P148, P149, P153, P155, P156, P157, P158, P159, P161, P164, P165, P171, P172, P174, P179, P181, P183, P185, P186, P189, P191, P192, P194, P198, P199, P201, P202, P204, P206, P208, P209, P212, P215, P216, P218, P219, P225, P226, P227, P230, P231, P232, P235, P237, P238, P240, P241 |
| Psychology | P3, P4, P9, P14, P15, P17, P20, P21, P22, P28, P29, P33, P35, P37, P38, P41, P42, P49, P54, P55, P56, P57, P58, P69, P72, P74, P75, P78, P82, P85, P87, P88, P89, P91, P92, P95, P96, P97, P98, P105, P106, P108, P114, P118, P119, P127, P134, P135, P137, P138, P141, P147, P150, P151, P152, P154, P160, P162, P166, P167, P168, P169, P170, P173, P175, P176, P177, P178, P180, P182, P184, P187, P188, P190, P195, P196, P200, P205, P210, P211, P213, P214, P217, P220, P221, P222, P223, P224, P228, P229, P233, P234, P239 |
| Science | P66, P68, P111, P129, P142, P163, P193, P197, P203, P207, P236 |
| Neuroscience | P27, P53, P128, P139 |
| Education | P115 |
RQ3. Which domains of social cognition are the focus of research in social cognition remediation?
Theory of mind was the most frequently studied domain with 146 publications, followed by 131 articles in emotional processing, 60 articles in attributional bias and 33 papers in social perception (see Fig 3). Although most studies focus on a single domain of social cognition, some evaluate two or more domains of social cognition, as shown in Fig 3. In this case, the most frequent combination was the pair formed by theory of mind and emotional processing (23 papers), as well as the triad of theory of mind, attributional bias and emotional processing (22 papers).
Fig 3. References by domains of social cognition.
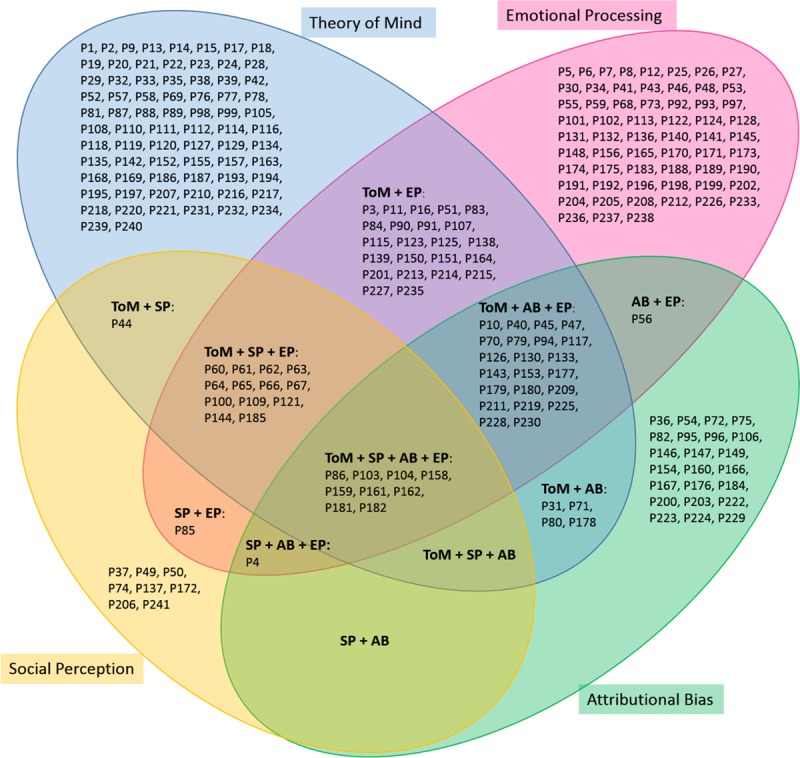
Venn diagram with four sets.
Studies with IB level of evidence were the most frequently found for each domain of social cognition. As can be observed in Fig 4, the greatest number focused on theory of mind and on emotional processing with IB level of evidence.
Fig 4. Categorization of papers in terms of social cognition domain and level of scientific evidence.

As a result of classifying publications according to domains of social cognition and the mental disorder they focus on, most publications in all four domains alluded to schizophrenia spectrum and other psychotic disorders. Autism spectrum disorder was the second most studied disorder (see Table 3).
Table 3. Mental disorders for each domain in social cognition.
| Social Cognition Domain | |
|---|---|
| Mental Disorder | Ref. |
| Emotion Processing | |
| Schizophrenia Spectrum and Other Psychotic Disorders | P4, P10, P16, P30, P34, P45, P46, P47, P48, P59, P60, P61, P62, P63, P64, P65, P66, P67, P70, P79, P83, P84, P85, P86, P92, P94, P100, P101, P102, P103, P104, P109, P121, P122, P128, P130, P131, P132, P133, P136, P138, P140, P143, P144, P148, P153, P158, P159, P161, P162, P164, P165, P173, P177, P179, P180, P181, P182, P185, P188, P189, P191, P192, P202, P204, P209, P225, P226, P227, P228, P230, P237, P238 |
| Autism Spectrum Disorder | P5, P7, P8, P11, P12, P26, P27, P41, P56, P93, P107, P115, P122, P123, P124, P125, P126, P175, P183, P190, P198, P201, P213, P214, P215, P219, P233, P235 |
| Depressive Disorders | P6, P73 |
| Feeding and Eating Disorders | P141, P212 |
| Anxiety Disorders | P113 |
| Attention Deficit / Hyperactivity Disorder | P43 |
| Bipolar and Related Disorders, and Schizoaffective Disorder | P117 |
| Disruptive, Impulse-Control, and Conduct Disorders | P51 |
| Personality Disorders | P40 |
| Theory of Mind | |
| Schizophrenia Spectrum and Other Psychotic Disorders | P9, P10, P14, P15, P16, P17, P28, P33, P39, P44, P45, P47, P60, P61, P62, P63, P64, P65, P66, P67, P70, P71, P79, P80, P83, P84, P86, P94, P98, P100, P103, P104, P108, P109, P121, P130, P133, P138, P142, P143, P144, P152, P153, P158, P159, P161, P162, P164, P177, P178, P179, P180, P181, P182, P185, P209, P220, P225, P227, P228, P230 |
| Autism Spectrum Disorder | P2, P11, P13, P18, P19, P24, P42, P52, P69, P77, P81, P88, P99, P107, P110, P114, P115, P116, P123, P125, P126, P134, P135, P155, P168, P193, P194, P201, P213, P214, P215, P216, P219, P235, P239 |
| Borderline Personality Disorder | P32, P232 |
| Personality Disorders | P40, P57 |
| Attention Deficit / Hyperactivity Disorder | P23 |
| Bipolar and Related Disorders, and Schizoaffective Disorder | P117 |
| Communication Disorders | P197 |
| Delusional Disorder | P31 |
| Disruptive, Impulse-Control, and Conduct Disorders | P51 |
| Intellectual Disabilities | P1 |
| Trauma- and Stressor-Related Disorders | P112 |
| Attributional Bias | |
| Schizophrenia Spectrum and Other Psychotic Disorders | P4, P10, P45, P47, P70, P71, P79, P80, P86, P94, P103, P104, P130, P133, P143, P153, P158, P159, P161, P162, P177, P178, P179, P180, P181, P182, P209, P225, P228, P230 |
| Anxiety Disorders | P72, P147, P203, P223, P224 |
| Depressive Disorders | P106, P149, P160, P200, P229 |
| Autism Spectrum Disorder | P56, P126, P219 |
| Bipolar and Related Disorders, and Schizoaffective Disorder | P117 |
| Delusional Disorder | P31 |
| Feeding and Eating Disorders | P36 |
| Personality Disorders | P40 |
| Social Perception | |
| Schizophrenia Spectrum and Other Psychotic Disorders | P4, P44, P60, P61, P62, P63, P64, P65, P66, P67, P74, P85, P86, P100, P103, P104, P109, P121, P137, P144, P158, P159, P161, P162, P172, P181, P182, P185, P206, P241 |
| Autism Spectrum Disorder | P50 |
| Intellectual Disabilities | P49 |
RQ4. What types of interventions are employed in social cognitive remediation?
As previously stated, on the basis of previous reviews and meta-analyses, three types of programs can be distinguished [31]: targeted interventions, broad-based interventions, and non-specific interventions. The latter may influence social cognition, but do not address it directly. According to this classification, targeted interventions were the focus of the largest number of publications with 156 papers, followed by non-specific therapies with 59 publications, and broad-based interventions with 26 publications (see on-line material, S3 Table, for a complete list).
Among targeted interventions, Social Cognition and Interaction Training (SCIT) was the focus of 16 publications, followed by Training of Affect Recognition (TAR) and Conversation-Based Intervention, both with 7 papers, Mind Reading and SummerMAX with 6 publications each, and Mentalization-Based Therapy (MBT), Micro-Expression Training Tool (METT) and The Theory of Mind Training with 4 publications each (see Table 4). The complete list of targeted interventions can be found as on-line material (S3 Table).
Table 4. Targeted interventions in social cognitive remediation.
| Targeted Interventions | Refs |
|---|---|
| Social Cognition and Interaction Training (SCIT) [67] | P10, P40, P45, P47, P94, P117, P126 (SCIT-Aa), P153, P177, P179, P180, P209 (F-SCITb), P211 (IFW-SCIT c), P219 (SCIT-Aa), P228, P230 |
| Training of Affect Recognition (TAR) [68] | P59, P92, P128, P191, P204, P237, P238 |
| Conversation-Based Intervention [69] | P21, P22, P38, P118, P119, P120, P186 |
| Mind Reading [70] | P88, P115, P116, P215, P216, P233 |
| SummerMAX [71] | P123, P124, P125, P183, P213, P214 |
| Mentalization-Based Therapy (MBT) [72] | P32, P221, P231, P232 |
| Micro-Expression Training Tool (METT) [73] | P131, P132, P188, P189 |
| The Theory of Mind Training [74] | P18, P19, P81, P99 |
a SCIT-A: Social Cognition and Interaction Training Modified for High Functioning Autism
b F-SCIT: Social Cognition and Interaction Training Modified for Family-Assisted
c IFW-SCIT: Social Cognition and Interaction Training Modified for Inpatient Forensic Wards
In the group of broad-based interventions, the most frequently studied therapy was Cognitive Enhancement Therapy (CET) with 11 publications, as shown in Table 5. The second most studied therapy was Integrated Psychological Therapy (IPT) with 4 articles. Auditory Training with Cognitive Social Training plus Social Cognition Training (AT + SCT) followed with 3 papers, and Cognitive Pragmatic Treatment (CPT) and REHACOP with 2 papers each. The rest of the papers on broad-based interventions are available in the supplementary material online (S3 Table).
Table 5. Broad-based interventions in social cognitive remediation.
| Broad-Based Interventions | Refs |
|---|---|
| Cognitive Enhancement Therapy (CET) [75] | P60, P61, P62, P63, P64, P65, P66, P67, P100, P109, P121 |
| Integrated Psychological Therapy (IPT) [76] | P74, P172, P206, P241 |
| Auditory-Based Cognitive Training plus Social-Cognition Training (AT+ SCT) [77] | P101, P102, P192 |
| Cognitive Pragmatic Treatment (CPT) [78] | P28, P76 |
| REHACOP (Programa de REHAbilitación COgnitiva en Psicosis) [79] | P157, P158 |
Finally, in the group of non-specific interventions on social cognition (see S3 Table), the largest number of publications referred to Cognitive and Behavioral Therapies with 28 papers, followed by Neurocognition Training with 5 publications, and Mindfulness and Art Therapy with 4 papers each. The rest of the papers on non-specific interventions are available in the supplementary material online (see S3 Table).
Among the studies analyzed, 61 were based on computerized training versus 180 that used no new technologies, but rather interpersonal modality (see Table 6). It could be interesting to carry out studies comparing the effectiveness of these two types of intervention as future work.
Table 6. Computerized vs. in-person interventions.
| Computerized interventions | |
| Targeted Interventions | P5, P26, P27, P41, P46, P48, P53, P56, P59, P88, P92, P97, P107, P115, P116, P128, P131, P132, P138, P144, P145, P160, P161, P162, P164, P165, P173, P181, P182, P185, P188, P189, P190, P191, P196, P198, P199, P202, P204, P208, P215, P216, P225, P233, P236, P237, P238 |
| Broad-Based Interventions | P34, P70, P101, P102, P122, P192 |
| Non-Specific Interventions | P12, P23, P39, P49, P93, P147, P149, P203 |
| In-person interventions | |
| Targeted Interventions | P1, P2, P3, P10, P14, P16, P17, P18, P19, P20, P21, P22, P24, P25, P32, P33, P35, P36, P38, P40, P42, P43, P44, P45, P47, P51, P58, P69, P71, P72, P79, P80, P81, P82, P83, P84, P85, P86, P87, P90, P91, P94, P95, P96, P98, P99, P103, P104, P105, P108, P110, P117, P118, P119, P120, P123, P124, P125, P126, P127, P130, P133, P134, P137, P141, P150, P151, P152, P153, P154, P155, P156, P168, P169, P170, P171, P177, P178, P179, P180, P183, P186, P187, P194, P195, P197, P201, P209, P211, P212, P213, P214, P217, P218, P219, P220, P221, P222, P223, P224, P227, P228, P230, P231, P232, P234, P239, P240 |
| Broad-Based Interventions | P15, P28, P60, P61, P62, P63, P64, P65, P66, P67, P74, P76, P100, P109, P121, P143, P157, P158, P172, P206, P241 |
| Non-Specific Interventions | P4, P6, P7, P8, P9, P11, P13, P29, P30, P31, P37, P50, P52, P54, P55, P57, P68, P73, P75, P77, P78, P89, P106, P111, P112, P113, P114, P129, P135, P136, P139, P140, P142, P146, P148, P159, P163, P166, P167, P174, P175, P176, P184, P193, P200, P205, P207, P210, P226, P229, P235. |
Discussion
This is the first systematic mapping review carried out on remediation interventions for the enhancement of social cognition deficits. The study included papers published over a period of eleven years (2006–2016). The results show the current situation of this field of knowledge, both with the areas that have received more attention, as well as those that show little research development. The present study adds to the recently published systematic mapping review on pharmacological interventions for social cognition improvement [22], providing a global overview of the current state of knowledge in the field of social cognition remediation interventions.
A total of 241 papers were selected from the initial 3229 non-repeated publications obtained from four databases (Scopus, PsycINFO, PubMed, Embase). The number of papers published per year on social cognition training and remediation interventions clearly increased throughout the studied period, especially in the last four years. This is an indicator of the growing interest in social cognition non-pharmacological treatment approaches, which may be related to the scant effectiveness of pharmacological treatments in improving social cognition deficits.
In terms of the level of scientific evidence as defined by the US Agency for Healthcare Research and Quality Agency [66], of the 241 selected papers, 106 were classified as having IB level of evidence (evidence obtained from at least one randomized clinical trial) and 41 as IIA (obtained from at least one well-designed, non-randomized controlled prospective study). According to the social cognitive domain studied, studies with IB and IIA level of evidence were the most frequently found in the four domains of social cognition. IB was the highest level of evidence that could be found in our mapping review because we excluded papers with IA level of evidence (namely, meta-analyses of randomized clinical trials). Thus, publications with a high level of evidence were predominant, as an indicator of the quality of the research in the field. Moreover, given the high proportion of studies with IB level and their associated important economic costs, current interest in the subject is evident, both for researchers and different public and private funding agencies.
Referring to publication venues, it is interesting to note that most studies were disseminated in journals with a high impact factor. Journals with the highest number of papers on this topic were two journals in the first quartile of their area of knowledge: Schizophrenia Research with 19 papers (IF 3.986; Q1-Psychiatry), and Journal of Autism and Developmental Disorders with 10 papers (IF 8.321; Q1-Psychology, Developmental). Moreover, of the top eight most popular publication venues, five (comprising 42 of the 62 papers) were first-quartile journals. The fact that papers were published in high-impact journals may be related to the high level of scientific evidence previously indicated.
Regarding areas of medical knowledge and related disciplines with research on social cognition training and remediation, most publications belonged to the field of Medicine, especially to Adult Psychiatry, followed by Child and Adolescent Psychiatry and Psychotherapy. Psychology was the discipline with the second-greatest number of publications in social cognition remediation. The fact that impairments in social cognition frequently appear in numerous psychiatric disorders might explain why most studies belong to Adult and Child/Adolescent areas of Psychiatry and Psychology.
Concerning social cognition domains, most of the published papers targeted theory of mind, followed by emotional processing. Previously published reviews centered on schizophrenia and other related disorders showed that emotional processing was the focus of most publications [28–31,63]. Nevertheless, the fact that the present systematic mapping review included papers in disorders other than schizophrenia, such as autism spectrum disorders, might explain this difference. In fact, after schizophrenia and related disorders, autism spectrum disorders were the focus of most of the selected papers in this systematic mapping review. As deficits in theory of mind is a core problem in autism [80], a significant number of papers focused on this domain [64]. Much less frequent was the study of attributional bias, followed by research on social perception training. A feasible explanation for this may be related to the fact that assessment instruments for theory of mind and emotional processing may be considered more objective and less influenced by cultural aspects, as opposed to social perception assessment [81], and less influenced by some symptoms of the disorder itself, as opposed to, for example, attributional bias in patients with paranoid ideation. On the other hand, it has previously been suggested that improvements in attributional bias and social perception might be more difficult to achieve than in theory of mind and social perception [30,63]. More empirical work is needed to determine whether interventions on attributional bias and social perception can produce changes and whether these changes can be objectively measured.
The results regarding the types of social cognition training and remediation interventions show that the majority of publications refer to targeted interventions. This finding is in line with previous publications showing a greater number of papers related to targeted interventions compared to other types of interventions [31]. In the group of targeted interventions, the greatest number of papers were on Social Cognition and Interaction Training (SCIT). SCIT targets three domains of social cognition: theory of mind, emotional processing and attributional bias [67]. Other targeted interventions were Training of Affect Recognition (TAR) [68], Conversation-Based Intervention [69], Mind Reading [70], SummerMAX [71], Mentalization-Based Therapy (MBT) [72], Micro-Expression Training Tool (METT) [73], and The Theory of Mind Training [74]. Among broad-based interventions, the therapy with the largest number of papers was Cognitive Enhancement Therapy (CET) [75]. CET consists of computer-assisted neurocognitive and social cognitive group training to improve theory of mind, social perception and emotional processing [82]. Other less frequently published broad-based interventions were Integrated Psychological Therapy (IPT) [76], Auditory Training with Cognitive Social Training plus Social Cognition Training (AT + SCT) [77] and REHACOP [79]. Finally, in the group of non-specific interventions, the largest number of publications was in Cognitive and Behavioral Therapies. Nevertheless, although publications on certain interventions were more numerous than others, the results show the existence of a considerable number of different interventions for improving social cognition. This may be partly due to the existence of different domains of social cognition, but also due to the limited number of comparative studies.
The present systematic mapping review has some risks and limitations. One of the risks implied in all systematic mapping reviews is related to selective reporting bias [83]. To minimize this risk, four different databases were used as the source for the search process: PsycINFO, PubMed, Embase and Scopus. These provide a comprehensive list of articles encompassing the different aspects of this mapping review. Nevertheless, we should acknowledge that the decision not to truncate search terms may have led to some important articles being overlooked. It is also worth noting that it was decided to exclude grey literature (e.g. theses, internal reports, etc.) from the study. This may have impinged on the validity of the study, but it should be stressed that grey literature is generally published without a rigorous review process. Another possible risk that could have affected this mapping review is the selection bias. This is related to the criteria used to select the articles to be analyzed during the study. In order to mitigate such a risk, both the inclusion and exclusion criteria were clearly defined.
Finally, the risk of likely inaccuracy in data extraction and misclassification was mitigated as classification and extraction data processes were performed independently by two researchers, and a consensus decision including the study coordinator was made in the event of no agreement between these two researchers.
Conclusions
To our knowledge, this is the first systematic mapping review describing social cognition remediation interventions. Our results show a growing interest in non-pharmacological treatments of social cognition, as can be demonstrated by the increase in the number of papers published over the studied period, their high level of scientific evidence, and their dissemination in journals with a high impact factor. Most studies are from the fields of psychiatry and psychology, with schizophrenia spectrum disorders and autism spectrum disorders being the two most studied conditions. Theory of mind was the most frequently studied domain of social cognition, followed by emotional processing. Targeted interventions were the most frequently studied, especially SCIT. Future research should be conducted on attributional bias and domains of social perception, with the comparative efficacy of different social cognition interventions also being an interesting future line of research.
Supporting information
(PDF)
(PDF)
(PDF)
(PDF)
Data Availability
All relevant data are within the manuscript and its Supporting Information files.
Funding Statement
This work was partially supported by Spanish Instituto de Salud Carlos III under PI16/00359 grant, and Spanish Ministerio de Ciencia, Innovación y Universidades, Agencia Estatal de Investigación (AEI) / European Regional Development Fund (FEDER, UE) under DPI2016-80894-R and TIN2015-72931-EXP grants, by Madrid Regional Government (R&D activities in Biomedicine S2017/BMD-3740 (AGES-CM 2-CM)) and Structural Funds of the European Union, by Castilla-La Mancha Regional Government / FEDER, UE under SBPLY/17/180501/000192 grant, and by the Centro de Investigación Biomédica en Red de Salud Mental (CIBERSAM) of the Instituto de Salud Carlos III. These funding sources have not been involved in study design; collection, analysis and interpretation of data; writing of the report; nor in the decision to submit the paper for publication.
References
- 1.Brothers L. The neural basis of primate social communication. Motiv Emot. 1990. June;14(2):81–91. [Google Scholar]
- 2.Fiske ST, Taylor SE. Social Cognition. New York, NY: McGraw-Hill Education; 1991. [Google Scholar]
- 3.Green MF, Penn DL, Bentall R, Carpenter WT, Gaebel W, Gur RC, et al. Social cognition in schizophrenia: an NIMH workshop on definitions, assessment, and research opportunities. Schizophr Bull. 2008. August 20;34(6):1211–20. 10.1093/schbul/sbm145 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Kunda Z. Social Cognition: Making Sense of People Cambidge, MA: The MIT Press; 1999. [Google Scholar]
- 5.Ostrom TM. The sovereignty of social cognition In: Wyer RS, Srull TK, editors. Handbook of Social Cognition; Hillsdale, NJ; 1984. p. 1–37. [Google Scholar]
- 6.Penn DL, Corrigan PW, Bentall RP, Racenstein JM, Newman L. Social cognition in schizophrenia. Psychol Bull. 1997;121(1):114–32. [DOI] [PubMed] [Google Scholar]
- 7.Pinkham AE, Hopfinger JB, Pelphrey KA, Piven J, Penn DL. Neural bases for impaired social cognition in schizophrenia and autism spectrum disorders. Schizophr Res. 2008. February;99(1–3):164–75. 10.1016/j.schres.2007.10.024 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Lai M-C, Lombardo M V, Baron-Cohen S. Autism. Lancet. 2014. March;383(9920):896–910. 10.1016/S0140-6736(13)61539-1 [DOI] [PubMed] [Google Scholar]
- 9.Leekam S. Social cognitive impairment and autism: what are we trying to explain? Philos Trans R Soc B Biol Sci. 2016. January 19;371(1686):20150082. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Bylsma LM, Morris BH, Rottenberg J. A meta-analysis of emotional reactivity in major depressive disorder. Clin Psychol Rev. 2008. April;28(4):676–91. 10.1016/j.cpr.2007.10.001 [DOI] [PubMed] [Google Scholar]
- 11.Samamé C. Social cognition throughout the three phases of bipolar disorder: A state-of-the-art overview. Psychiatry Res. 2013. December;210(3):1275–86. 10.1016/j.psychres.2013.08.012 [DOI] [PubMed] [Google Scholar]
- 12.Vlad M, Raucher-Chéné D, Henry A, Kaladjian A. Functional outcome and social cognition in bipolar disorder: Is there a connection? Eur Psychiatry. 2018. August;52:116–25. 10.1016/j.eurpsy.2018.05.002 [DOI] [PubMed] [Google Scholar]
- 13.Bo Q, Mao Z, Li X, Wang Z, Wang C, Ma X. Use of the MATRICS consensus cognitive battery (MCCB) to evaluate cognitive deficits in bipolar disorder: A systematic review and meta-analysis. McKenna PJ, editor. PLoS One. 2017. April 24;12(4):e0176212 10.1371/journal.pone.0176212 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Bora E, Köse S. Meta-analysis of theory of mind in anorexia nervosa and bulimia nervosa: a specific impairment of cognitive perspective taking in anorexia nervosa? Int J Eat Disord. 2016. August;49(8):739–40. 10.1002/eat.22572 [DOI] [PubMed] [Google Scholar]
- 15.Pinkham AE. Social cognition in schizophrenia. J Clin Psychiatry. 2014. May;75(suppl 2):14–9. [DOI] [PubMed] [Google Scholar]
- 16.Green MF, Horan WP, Lee J. Social cognition in schizophrenia. Nat Rev Neurosci. 2015. September 16;16(10):620–31. 10.1038/nrn4005 [DOI] [PubMed] [Google Scholar]
- 17.van Donkersgoed RJM, Wunderink L, Nieboer R, Aleman A, Pijnenborg GHM. Social cognition in individuals at ultra-high risk for psychosis: A meta-analysis. van Amelsvoort T, editor. PLoS One. 2015. October 28;10(10):e0141075 10.1371/journal.pone.0141075 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Hofer A, Baumgartner S, Bodner T, Edlinger M, Hummer M, Kemmler G, et al. Patient outcomes in schizophrenia II: the impact of cognition. Eur Psychiatry. 2005. August;20(5–6):395–402. 10.1016/j.eurpsy.2005.02.006 [DOI] [PubMed] [Google Scholar]
- 19.Couture SM, Penn DL, Roberts DL. The functional significance of social cognition in schizophrenia: a review. Schizophr Bull. 2006. August 18;32(Supplement 1):S44–63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Schmidt SJ, Mueller DR, Roder V. Social cognition as a mediator variable between neurocognition and functional outcome in schizophrenia: empirical review and new results by structural equation modeling. Schizophr Bull. 2011. September 1;37(suppl 2):S41–54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Shmukler AB, Gurovich IY, Agius M, Zaytseva Y. Long-term trajectories of cognitive deficits in schizophrenia: A critical overview. Eur Psychiatry. 2015. November;30(8):1002–10. 10.1016/j.eurpsy.2015.08.005 [DOI] [PubMed] [Google Scholar]
- 22.Fernández-Sotos P, Navarro E, Torio I, Dompablo M, Fernández-Caballero A, Rodriguez-Jimenez R. Pharmacological interventions in social cognition deficits: a systematic mapping review. Psychiatry Res. 2018;270:57–67. 10.1016/j.psychres.2018.09.012 [DOI] [PubMed] [Google Scholar]
- 23.Healey KM, Bartholomeusz CF, Penn DL. Deficits in social cognition in first episode psychosis: A review of the literature. Clin Psychol Rev. 2016. December;50:108–37. 10.1016/j.cpr.2016.10.001 [DOI] [PubMed] [Google Scholar]
- 24.Pinkham AE, Penn DL, Green MF, Buck B, Healey K, Harvey PD. The social cognition psychometric evaluation study: results of the expert survey and RAND panel. Schizophr Bull. 2014. July;40(4):813–23. 10.1093/schbul/sbt081 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Pinkham AE, Penn DL, Green MF, Harvey PD. Social cognition psychometric evaluation: results of the initial psychometric study. Schizophr Bull. 2016. March;42(2):494–504. 10.1093/schbul/sbv056 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Baghdadli A, Brisot J, Henry V, Michelon C, Soussana M, Rattaz C, et al. Social skills improvement in children with high-functioning autism: a pilot randomized controlled trial. Eur Child Adolesc Psychiatry. 2013. July 16;22(7):433–42. 10.1007/s00787-013-0388-8 [DOI] [PubMed] [Google Scholar]
- 27.Baghdadli A, Brisot-Dubois J, Picot M-C, Michelon C. Comparaison de l’effet de deux interventions prosociales sur l’évolution des capacités d’identification des expressions faciales et du raisonnement social d’enfants avec un syndrome d’Asperger ou autisme de haut niveau. Neuropsychiatr Enfance Adolesc. 2010. November;58(8):456–62. [Google Scholar]
- 28.Fiszdon JM, Reddy LF. Review of social cognitive treatments for psychosis. Clin Psychol Rev. 2012. December;32(8):724–40. 10.1016/j.cpr.2012.09.003 [DOI] [PubMed] [Google Scholar]
- 29.Grant N, Lawrence M, Preti A, Wykes T, Cella M. Social cognition interventions for people with schizophrenia: a systematic review focussing on methodological quality and intervention modality. Clin Psychol Rev. 2017. August;56:55–64. 10.1016/j.cpr.2017.06.001 [DOI] [PubMed] [Google Scholar]
- 30.Kurtz MM, Gagen E, Rocha NBF, Machado S, Penn DL. Comprehensive treatments for social cognitive deficits in schizophrenia: a critical review and effect-size analysis of controlled studies. Clin Psychol Rev. 2016. February;43:80–9. 10.1016/j.cpr.2015.09.003 [DOI] [PubMed] [Google Scholar]
- 31.Tan B-L, Lee S-A, Lee J. Social cognitive interventions for people with schizophrenia: a systematic review. Asian J Psychiatr. 2016. September; [DOI] [PubMed] [Google Scholar]
- 32.Perryman CL. Mapping studies. J Med Libr Assoc. 2016. January;104(1):79–82. 10.3163/1536-5050.104.1.014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Cooper ID. What is a “mapping study?” J Med Libr Assoc. 2016. January;104(1):76–8. 10.3163/1536-5050.104.1.013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Forsman AK, Ventus DBJ, van der Feltz-Cornelis CM, Wahlbeck K. Public mental health research in Europe: a systematic mapping for the ROAMER project. Eur J Public Health. 2014. December;24(6):955–60. 10.1093/eurpub/cku055 [DOI] [PubMed] [Google Scholar]
- 35.Evans-Lacko S, Courtin E, Fiorillo A, Knapp M, Luciano M, Park A-L, et al. The state of the art in European research on reducing social exclusion and stigma related to mental health: A systematic mapping of the literature. Eur Psychiatry. 2014. August;29(6):381–9. 10.1016/j.eurpsy.2014.02.007 [DOI] [PubMed] [Google Scholar]
- 36.Fernandez A, Black J, Jones M, Wilson L, Salvador-Carulla L, Astell-Burt T, et al. Flooding and mental health: A systematic mapping review. Ebi KL, editor. PLoS One. 2015. April 10;10(4):e0119929 10.1371/journal.pone.0119929 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Bantjes J, Iemmi V, Coast E, Channer K, Leone T, McDaid D, et al. Poverty and suicide research in low- and middle-income countries: systematic mapping of literature published in English and a proposed research agenda. Glob Ment Heal. 2016. December 13;3:e32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.McDaniel Peters BC, Wood W. Autism and equine-assisted interventions: A systematic mapping review. J Autism Dev Disord. 2017. October 21;47(10):3220–42. 10.1007/s10803-017-3219-9 [DOI] [PubMed] [Google Scholar]
- 39.EBSE-RG. Template for a mapping study protocol [Internet]. 2009 [cited 2002 Jul 20]. Available from: http://www.dur.ac.uk/ebse/resources/templates/MappingStudyTemplate.pdf
- 40.Kitchenham B. Procedures for performing systematic reviews. Tech. rep. TR/SE-0401, version 2.3. Keele University. 2004.
- 41.Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009. July 21;6(7):e1000097 10.1371/journal.pmed.1000097 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Gauthier C, Doyen C, Amado I, Lôo H, Gaillard R. Applications thérapeutiques de l’ocytocine dans l’autisme: premiers résultats et pistes de recherche. Encephale. 2016. Feb;42(1):24–31. 10.1016/j.encep.2015.07.006 [DOI] [PubMed] [Google Scholar]
- 43.Kucharska-Pietura K, Mortimer A. Can antipsychotics improve social cognition in patients with schizophrenia? CNS Drugs. 2013. May 27;27(5):335–43. 10.1007/s40263-013-0047-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Henry JD, Phillips LH, von Hippel C. A meta-analytic review of theory of mind difficulties in behavioural-variant frontotemporal dementia. Neuropsychologia. 2014. April;56:53–62. 10.1016/j.neuropsychologia.2013.12.024 [DOI] [PubMed] [Google Scholar]
- 45.Xiao H, Jacobsen A, Chen Z, Wang Y. Detecting social-cognitive deficits after traumatic brain injury: an ALE meta-analysis of fMRI studies. Brain Inj. 2017. June 19;1–9. [DOI] [PubMed] [Google Scholar]
- 46.Palmeri R, Lo Buono V, Corallo F, Foti M, Di Lorenzo G, Bramanti P, et al. Nonmotor symptoms in Parkinson disease: a descriptive review on social cognition ability. J Geriatr Psychiatry Neurol. 2017. March 11;30(2):109–21. 10.1177/0891988716687872 [DOI] [PubMed] [Google Scholar]
- 47.Kennedy DP, Adolphs R. The social brain in psychiatric and neurological disorders. Trends Cogn Sci. 2012. November;16(11):559–72. 10.1016/j.tics.2012.09.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.de Vries P, Humphrey A, McCartney D, Prather P, Bolton P, Hunt A. Consensus clinical guidelines for the assessment of cognitive and behavioural problems in tuberous sclerosis. Eur Child Adolesc Psychiatry. 2005. July;14(4):183–90. 10.1007/s00787-005-0443-1 [DOI] [PubMed] [Google Scholar]
- 49.Turkstra LS, Abbeduto L, Meulenbroek P. Social cognition in adolescent girls with fragile X syndrome. Am J Intellect Dev Disabil. 2014. July;119(4):319–39. 10.1352/1944-7558-119.4.319 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Lo ST, Siemensma E, Collin P, Hokken-Koelega A. Impaired theory of mind and symptoms of autism spectrum disorder in children with Prader–Willi syndrome. Res Dev Disabil. 2013. September;34(9):2764–73. 10.1016/j.ridd.2013.05.024 [DOI] [PubMed] [Google Scholar]
- 51.Peyroux E, Santaella N, Broussolle E, Rigard C, Favre E, Brunet A-S, et al. Social cognition in Wilson’s disease: A new phenotype? Pavlova MA, editor. PLoS One. 2017. April 6;12(4):e0173467 10.1371/journal.pone.0173467 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Baron-Cohen S, Wheelwright S, Hill J, Raste Y, Plumb I. The “Reading the Mind in the Eyes” test revised version: a study with normal adults, and adults with Asperger syndrome or high-functioning autism. J Child Psychol Psychiatry. 2001. February;42(2):241–51. [PubMed] [Google Scholar]
- 53.Frith CD. The Cognitive Neuropsychology of Schizophrenia. Hove, UK: Laurence Erlbaum Associates; 1992. [Google Scholar]
- 54.Penn DL, Addington J, Pinkham A. Social cognitive impariments In: Lieberman JA, Stroup TS, Perkins DO, editors. The American Psychiatric Publishing Textbook of Schizophrenia. Arlington, VA: American Psychiatric Publishing, Inc.; 2006. p. 261–74. [Google Scholar]
- 55.Shamay-Tsoory SG. The neural bases for empathy. Neurosci. 2011. February 11;17(1):18–24. [DOI] [PubMed] [Google Scholar]
- 56.Addington J, Saeedi H, Addington D. Influence of social perception and social knowledge on cognitive and social functioning in early psychosis. Br J Psychiatry. 2006. October 1;189(4):373–8. [DOI] [PubMed] [Google Scholar]
- 57.Toomey R, Schuldberg D, Corrigan P, Green MF. Nonverbal social perception and symptomatology in schizophrenia. Schizophr Res. 2002. January 1;53(1–2):83–91. [DOI] [PubMed] [Google Scholar]
- 58.Corrigan PW, Green MF. Schizophrenic patients’ sensitivity to social cues: the role of abstraction. Am J Psychiatry. 1993. April;150(4):589–94. 10.1176/ajp.150.4.589 [DOI] [PubMed] [Google Scholar]
- 59.Penn DL, Ritchie M, Francis J, Combs D, Martin J. Social perception in schizophrenia: the role of context. Psychiatry Res. 2002. March 15;109(2):149–59. [DOI] [PubMed] [Google Scholar]
- 60.Mayer JD, Salovey P, Caruso DR, Sitarenios G. Emotional intelligence as a standard intelligence. Emotion. 2001. September;1(3):232–42. [PubMed] [Google Scholar]
- 61.Salovey P, Sluyter DJ. Emotional Development and Emotional Intelligence. New York, NY: Basic Books; 1997. [Google Scholar]
- 62.Choi JH, Kim JH, Lee J, Green MF. Social cognition training for individuals with schizophrenia: a review of targeted interventions. Clin Psychopharmacol Neurosci. 2009;7(2):29–38. [Google Scholar]
- 63.Kurtz MM, Richardson CL. Social cognitive training for schizophrenia: a meta-analytic investigation of controlled research. Schizophr Bull. 2012. September 1;38(5):1092–104. 10.1093/schbul/sbr036 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Bishop-Fitzpatrick L, Minshew NJ, Eack SM. A systematic review of psychosocial interventions for adults with autism spectrum disorders. J Autism Dev Disord. 2013. March 24;43(3):687–94. 10.1007/s10803-012-1615-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Vass E, Fekete Z, Simon V, Simon L. Interventions for the treatment of theory of mind deficits in schizophrenia: Systematic literature review. Psychiatry Res. 2018. September;267:37–47. 10.1016/j.psychres.2018.05.001 [DOI] [PubMed] [Google Scholar]
- 66.West S, King V, Carey TS, Lohr KN, McKoy N, Sutton SF, et al. Systems to rate the strength of scientific evidence. Rockville, MD; 2002. [PMC free article] [PubMed]
- 67.Penn D, Roberts DL, Munt ED, Silverstein E, Jones N, Sheitman B. A pilot study of social cognition and interaction training (SCIT) for schizophrenia. Schizophr Res. 2005. December 15;80(2–3):357–9. 10.1016/j.schres.2005.07.011 [DOI] [PubMed] [Google Scholar]
- 68.Frommann N, Streit M, Wölwer W. Remediation of facial affect recognition impairments in patients with schizophrenia: a new training program. Psychiatry Res. 2003. March;117(3):281–4. [DOI] [PubMed] [Google Scholar]
- 69.Lecce S, Bianco F, Demicheli P, Cavallini E. Training preschoolers on first-order false belief understanding: Transfer on advanced ToM skills and metamemory. Child Dev. 2014. July;n/a-n/a. [DOI] [PubMed] [Google Scholar]
- 70.Baron-Cohen S, Golan O, Wheelwright S, Hill JJ. Mind Reading: The Interactive Guide to Emotions. London: Jessica Kingsley Limited; 2004. [Google Scholar]
- 71.Lopata C, Thomeer ML, Volker MA, Nida RE. Effectiveness of a cognitive-behavioral treatment on the social behaviors of children with Asperger’s disorder. Focus Autism Other Dev Disabl. 2006;21:237–244. [Google Scholar]
- 72.Fonagy P, Bateman AW. Mechanisms of change in mentalization-based treatment of BPD. J Clin Psychol. 2006. April;62(4):411–30. 10.1002/jclp.20241 [DOI] [PubMed] [Google Scholar]
- 73.Marsh PJ, Green MJ, Russell TA, McGuire J, Harris A, Coltheart M. Remediation of facial emotion recognition in schizophrenia: Functional predictors, generalizability, and durability. Am J Psychiatr Rehabil. 2010. May 21;13(2):143–70. [Google Scholar]
- 74.Steerneman P, Jackson S, Pelzer H, Muris P. Children with social handicaps: An intervention programme using a theory of mind approach. Clin Child Psychol Psychiatry. 1996. April 26;1(2):251–63. [Google Scholar]
- 75.Hogarty GE, Flesher S. Practice principles of cognitive enhancement therapy for schizophrenia. Schizophr Bull. 1999. January 1;25(4):693–708. 10.1093/oxfordjournals.schbul.a033411 [DOI] [PubMed] [Google Scholar]
- 76.Roder V, Studer K, Brenner H. Experiences with an integrated psychological therapy program for training communication and cognitive abilities in the rehabilitation of severely ill chronic schizophrenic patients. Schweiz Arch Neurol Psychiatr. 1987;138(1):31–44. [PubMed] [Google Scholar]
- 77.Fisher M, Holland C, Merzenich MM, Vinogradov S. Using neuroplasticity-based auditory training to improve verbal memory in schizophrenia. Am J Psychiatry. 2009. Jul;166(7):805–11. 10.1176/appi.ajp.2009.08050757 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Gabbatore I, Sacco K, Angeleri R, Zettin M, Bara BG, Bosco FM. Cognitive pragmatic treatment: A rehabilitative program for traumatic brain injury individuals. J Head Trauma Rehabil. 2015;30(5):E14–28. 10.1097/HTR.0000000000000087 [DOI] [PubMed] [Google Scholar]
- 79.Ojeda N, Peña J, Bengoetxea E, Garcia A, Sanchez P, Elizagarate E, et al. REHACOP: a cognitive rehabilitation programme in psychosis. Rev Neurol. 2012;54(10):640. [PubMed] [Google Scholar]
- 80.Adams MP. Explaining the theory of mind deficit in autism spectrum disorder. Philos Stud. 2013. March 11;163(1):233–49. [Google Scholar]
- 81.Hong Y-Y, Benet-Martinez V, Chiu C-Y, Morris MW. Boundaries of cultural influence: Construct activation as a mechanism for cultural differences in social perception. J Cross Cult Psychol. 2003. July 26;34(4):453–64. [Google Scholar]
- 82.Lewandowski KE, Eack SM, Hogarty SS, Greenwald DP, Keshavan MS. Is cognitive enhancement therapy equally effective for patients with schizophrenia and schizoaffective disorder? Schizophr Res. 2011. February;125(2–3):291–4. 10.1016/j.schres.2010.11.017 [DOI] [PubMed] [Google Scholar]
- 83.Higgins JP, Altman DG. Assessing risk of bias in included studies In: Cochrane Handbook for Systematic Reviews of Interventions. Chichester, UK: John Wiley & Sons, Ltd; p. 187–241. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
(PDF)
(PDF)
(PDF)
(PDF)
Data Availability Statement
All relevant data are within the manuscript and its Supporting Information files.