

Abstract
Background:
Childhood maltreatment is one of the most potent predictors of future psychopathology, including internalizing disorders. It remains unclear whether heightened amygdala reactivity to threat and elevated stress exposure may be implicated in the pathogenesis and maintenance of internalizing disorders among individuals with a history of childhood maltreatment.
Methods:
Using data from a sample of 1144 young adults, we investigated the contribution of baseline threat-related amygdala reactivity and prospective major stressful life events to internalizing symptoms severity one year later (on average) in individuals with a history of maltreatment (n=100) and propensity-score-matched non-maltreated peers (n=96).
Results:
Even after stringently matching for several potentially confounding variables - including baseline internalizing symptoms, socio-economic-status and IQ – childhood maltreatment status predicted increased amygdala reactivity at baseline, elevated post-baseline exposure to major stressful life events and internalizing symptoms at follow-up. We also showed, for the first time, that amygdala reactivity at baseline and also post-baseline exposure to major stressful life events mediated the association between a history of maltreatment and future internalizing symptoms.
Conclusion:
These findings provide support for the view that maltreatment is a potent developmental insult leading to long-lasting neurocognitive recalibrations of the threat processing system. It is possible that such alterations, over time, may impact mental health functioning by compromising the ability to effectively negotiate everyday challenges (‘stress susceptibility’). These alterations were not, however, found to sensitize an individual to the impact of major stressful life events. The results of this study also lend compelling support to the view that increased psychiatric risk, in the context of childhood maltreatment, follows from an increased propensity to experience major stressful life events (‘stress generation’).
Keywords: Maltreatment, Child Abuse, Amygdala, Stress, Internalizing Disorder
Introduction
Epidemiological and neurocognitive evidence suggests that childhood maltreatment is a developmental insult with profound and far-reaching consequences (Green et al., 2010; Kessler et al., 2010). Parental maltreatment is known to account for the emergence of a significant proportion of all psychiatric disorders across the life-span (Green et al., 2010; Kessler et al., 2010). Moreover, psychiatric patients with a history of maltreatment tend to have unfavorable prognoses. For example, in the context of internalizing disorders, (e.g. depression and anxiety) those with a history of maltreatment exhibit earlier onset of symptoms, greater comorbidity, higher relapse risks and poorer responsiveness to evidence-based interventions (Agnew-Blais & Danese, 2016; Hovens et al., 2010; Nanni, Uher, & Danese, 2012; Teicher & Samson, 2013). Despite the well-established link between childhood maltreatment and subsequent disorder, we still lack precision in our understanding of the mechanisms and markers underlying increased psychiatric vulnerability (McCrory, Gerin, & Viding, 2017; McCrory & Viding, 2015). In particular, prospective studies are required to determine whether maltreatment-related neurobiological and cognitive alterations are mechanistically implicated in the emergence of future disorders. The absence of such studies limits the possibility of developing preventative diagnostic tools and clinical interventions to identify and provide support for those maltreated individuals at greatest risk.
It has been proposed that the biological embedding of maltreatment experience is associated with recalibration of several neurocognitive systems (Danese & McEwen, 2012; McCrory, Gerin, et al., 2017; McCrory & Viding, 2015). These adaptations are postulated to provide proximal benefits for a child in an abusive or neglectful home environment but confer risk (‘latent vulnerability’) for psychopathology, since such adaptations are not thought to be optimized for more normative environments (McCrory & Viding, 2015). Candidate neurocognitive systems include threat processing (Hein & Monk, 2016; McCrory, Gerin, et al., 2017; McCrory & Viding, 2015), reward processing (McCrory, Gerin, et al., 2017) and autobiographical memory processing (McCrory, Puetz, et al., 2017). These neurocognitive changes can confer latent vulnerability either directly or indirectly. Direct effects capture how maltreatment-related neurocognitive changes alter the way in which an individual perceives, processes and responds to the social world around them. For example, recalibration of the threat processing system may have a direct effect on psychological functioning by compromising and placing greater pressure on the emotion regulatory system (Tottenham & Gabard-Durnam, 2017). This may increase the degree to which everyday challenges burden and tax an individual and/or increase the deleterious impact of major stressful life events (‘stress susceptibility’) (Admon et al., 2009; McLaughlin et al., 2014; Swartz, Knodt, Radtke, & Hariri, 2015). In other words, negotiating daily stressors and major negative life events may become more difficult. Equally, neurocognitive changes in the threat processing system can alter how an individual influences their own social experience. Direct effects here capture the way in which an individual may act in ways that precipitate the likelihood of stressor events occurring (‘stress generation’), for instance by increasing rejection sensitivity (Puetz et al., 2014, 2016) and conflictual interactions (Hernandez, Trout, & Liu, 2016). Indirect effects (not examined in this study), capture how maltreatment-related neurocognitive changes influence how an individual elicits and sustains a network of social support (McCrory, Gerin, et al., 2017).
Several lines of evidence support the view that altered threat processing is associated with internalizing symptomatology. Among groups of adults (not selected based on maltreatment status), it has been reported that amygdala reactivity on its own (Mattson, Hyde, Shaw, Forbes, & Monk, 2016), and in interaction with stress exposure (Admon et al., 2009; McLaughlin et al., 2014; Swartz et al., 2015), predicts future internalizing symptomatology several years later. Thus, variability in amygdala reactivity on its own may represent a neural biomarker capable of indexing psychiatric risk; moreover, amygdala reactivity may also potentiate the effects of stressor events. While extant studies have documented an association between childhood maltreatment experience and increased amygdala reactivity to threat (Hein & Monk, 2016; McCrory, Gerin, et al., 2017) its prognostic value has not previously been investigated. Here, using a longitudinal design and a propensity score matched control group, we aimed to investigate for the first time the potential contribution of baseline threat-related amygdala reactivity to future internalizing psychopathology among individuals with significant childhood maltreatment experiences. In particular, we investigated whether baseline amygdala reactivity on its own (i.e. independently of subsequent major stressful life events) would mediate the association between maltreatment status and increased future internalizing symptoms. In addition, we explored whether baseline amygdala reactivity in interaction with subsequent major stressful life events was associated with increased future internalizing symptoms.
Extant findings also suggest that a history of childhood maltreatment is associated with a higher incidence of stressful life events (Finkelhor, Ormrod, & Turner, 2007; Hankin, 2005; Hernandez et al., 2016; Liu, Choi, Boland, Mastin, & Alloy, 2013; Uhrlass & Gibb, 2007; Widom, Czaja, & Dutton, 2014, 2008), which in turn potentiate psychiatric risk (Espejo et al., 2007; Harkness, Lumley, & Truss, 2008; Hernandez et al., 2016; Kendler, Kuhn, & Prescott, 2004; McLaughlin, Conron, Koenen, & Gilman, 2010; Uhrlass & Gibb, 2007). However, it remains unclear whether these associations are in fact secondary to baseline levels of symptomatology and other co-occurring risk factors, and whether they apply to individuals who have experienced parental maltreatment above clinical thresholds. Previous studies have not concurrently controlled for the impact of several potentially confounding factors such as, socio-economic-status, IQ, ethnicity, age, gender and, crucially, baseline symptom levels. Another common limitation is that a number of previous studies have conflated the experience of parental childhood maltreatment with other forms of early adversity (e.g. death of parent, severe illness, poverty) and/or have measured maltreatment as a continuous variable, thus including mostly individuals who experienced maltreatment within normative/subclinical ranges. Here, we address these methodological limitations by carefully selecting a group of individuals with significant experiences of self-reported childhood maltreatment and systematically controlling for a set of potentially confounding variables using a propensity score matched control group. This allowed us to test, in the context of stringent controls, whether a history of childhood maltreatment is associated with higher incidence of post-baseline major stressful life events and whether this may explain, in part, the association between childhood maltreatment and future internalizing symptoms. Using the baseline measure of amygdala activation, it was also possible to explore whether amygdala reactivity to threat was associated with increased likelihood of major stressful life events.
To summarize, in the current study we wished to examine the impact of a history of childhood maltreatment on threat processing, stress exposure and internalizing symptoms in a sample of university students who are negotiating the developmental challenge of establishing autonomy and independence as young adults and who we know (from extant research) to be particularly vulnerable to mental health difficulties (Auerbach et al., 2018). It will be important for future studies to examine the impact of childhood maltreatment at other developmental periods in order to inform a life-course perspective.
We had two main hypotheses. First, that individual variability in baseline threat-related amygdala reactivity would capture latent vulnerability to future internalizing symptoms either on its own or in interaction with major stressful life events. That is, we investigated whether, in the context of maltreatment, heightened amygdala reactivity was associated with increased future internalizing symptoms generally, or only in the context of major life stressors. Second, we hypothesized that (even after stringent matching for several potentially confounding variables) maltreatment would be associated with an increased likelihood of major stressful life events occurring, and that these would in turn partly mediate the association between maltreatment and future symptoms. In an exploratory step we investigated whether individual differences in amygdala response to threat could partly account for any increased likelihood of subsequently experiencing major stressful live events.
Method
Participants
Participants were drawn from the Duke Neurogenetics Study (DNS), which consisted of 1144 young adults who completed baseline neuroimaging and questionnaire assessments. Participants with longitudinal data were selected for inclusion in analyses (n=584). In line with studies of childhood maltreatment prevalence (Radford et al., 2011; Stoltenborgh, Bakermans-Kranenburg, Alink, & van IJzendoorn, 2015), a subset of individuals reported experiences of significant childhood abuse and/or neglect (Maltreated Group: MT; n=100). Propensity score matched (PSM) controls (Control Group: CT; n=96) were selected from those individuals who reported no history of childhood abuse or neglect (Non-Maltreated Group: Non-MT; n=127). That is, after PSM, 31 Non-MT individuals were discarded. More information regarding the DNS sample, subdivision into the MT and Non-MT groups and PSM can be found in the Supplementary Materials and Methods section (Appendix S1).
Procedure and measures
Baseline assessment
fMRI paradigm.
The neuroimaging protocol included a face-matching paradigm that has been shown to evoke robust (Prather, Bogdan, & Hariri, 2013) and reliable (Manuck, Brown, Forbes, & Hariri, 2007) threat-related amygdala reactivity across a wide range of populations. This task has been described in detail in previous published research from the Duke Neurogenetics Study (Prather et al., 2013; Swartz et al., 2015) and more information can be found in the Supplementary Materials and Methods section (Appendix S1).
Behavioral measures.
Measures of anxiety and depression were collected using the Mood and Anxiety Symptoms Questionnaire (MASQ) (Watson et al., 1995). In line with previous investigations, scores across all four subscales (depression, anxiety, anxious arousal and anhedonia) were summed together to create a total internalizing symptoms score (Swartz et al., 2015). Experience of childhood abuse and neglect were assessed using the Childhood Trauma Questionnaire (Bernstein et al., 1994). This is a retrospective 28-items screening tool which assess five subtypes of maltreatment: emotional, physical and sexual abuse and physical and emotional neglect. Each of the CTQ’s five subscales has robust internal consistency, test-retest reliability, and convergent validity with a clinician-rated interview of childhood abuse (Bernstein et al., 1994, 2003; Bernstein, Ahluvalia, Pogge, & Handelsman, 1997). This is one of the best validated self-reported/retrospective measure of childhood abuse and also one of the most commonly implemented in studies of childhood maltreatment. Moreover, as part of a large battery of demographic information and questionnaires, participants reported their age, gender, ethnicity and socio-economic status (operationalized using the information related to highest parental education achievement by either parent).
Longitudinal assessment
Behavioral measures.
Every 3 months participants were invited by email to complete the MASQ. They also reported their experience of major stressful life events since their last assessment (e.g. break-up with partner, death of a good friend, major argument with friend or family member, personal injury, etc.) using the Life Events Scale for Students (LESS) (Clements & Turpin, 1996). If multiple longitudinal assessments were available, the last available MASQ score was selected. For the longitudinal major stressful life events (LESS) scores, all available post-baseline assessments were used to create a standardized metric of stressful life events per year, which also included a measure of severity of impact. The time-lapsed between baseline and last post-baseline assessment between the MT group (mean = 11.8 months, s.d. = 7.7, min = 1.2, max = 43.9) and the CT group (mean = 11.4 months, s.d. = 7.9, min = 2.7, max = 45.7) was not significantly different t(197) = - 0.37, p = .71. Moreover, the number of post-baseline assessments was also similar across groups (about half of participants completed two or three post-baseline assessments).
Data analysis
Propensity Score Matching.
The MT Group was propensity score matched (PSM) to the Non-MT sample for the following variables: age, gender, SES, IQ, ethnicity and baseline internalizing symptoms. PSM allowed us to find the best possible match on several categorical and continuous potential confounders, thus minimizing the difference between the MT and CT groups. We did not include levels of major stressful life events at baseline as we were interested in the relationship between childhood maltreatment experience and overall tendency to experience stressful life events in adulthood. The Supplementary Materials and Methods section (Appendix S1) and the Supplementary Results section (Appendix S2) provide further information on the matching procedure, rationale and output.
fMRI analysis.
The general analytic strategy has been reported in previously published research from the Duke Neurogenetics Study (Swartz et al., 2015), and is described in detail in the Supplementary Materials and Methods section (Appendix S1). It was hypothesized that our findings would be specific to threat-related amygdala reactivity, thus the analyses focused on the contrast of angry and fearful faces (vs. neutral faces), because each represents a canonical threat stimuli (Prather et al., 2013; Whalen et al., 2009). Left and right amygdala threat-reactivity for our contrast of interest (i.e. angry and fearful faces > neutral faces) was highly correlated (r = 0.81, p < .001). Thus, in order to reduce the number of comparisons performed, we averaged the parameter estimates across hemispheres to obtain one mean parameter estimate of amygdala reactivity to threat.
Statistical models.
The main goals of the analyses presented in this paper were: i) to assess the impact of a history of childhood maltreatment (independently of concurrent internalizing symptoms and a specific set of relevant person-specific factors) on both amygdala reactivity and major stressful life events; and ii) to investigate if those two variables (in interaction or independently) contributed to increased risk of future psychopathology among maltreated individuals. All analyses were performed with the propensity score matched data, which included a weighting variable. In order to simultaneously assess the relationship between maltreatment status, amygdala reactivity, major stressful life events and future internalizing symptoms, a parallel mediation model (with baseline amygdala and post-baseline exposure to stressful life events as mediators) and a moderated mediation model (with baseline amygdala as the mediator and post-baseline exposure to major stressful life events as the moderator) were performed in the R package Lavaan in combination with Lavaan.Survey.
Results
Propensity Score Matching
Full Matching yielded satisfactory results with a reduction in the overall standardized mean difference across all covariates from 0.42 to 0.09 post-matching (Table 1; see the Supplementary Results section (Appendix S2), the Supplementary Table S1 and Supplementary Table S2 for more details on the PSM output and other groups’ characteristics). Notably, the standardized mean difference of key variables, such as baseline internalizing symptoms, was reduced from 1.02 (before matching) to 0.02 (post matching). All analyses were performed using the MT group (n=100) and the propensity score-matched CT group (n=96) - i.e. the Non-MT group after propensity score matching.
Table 1.
Balance in Covariates Before and After Matching between the Maltreated and Non-Maltreated Group/Controls.
| Mean | Standardized Mean Difference1 |
||||
|---|---|---|---|---|---|
| MT | Non-MT | CT (Non- MT Post Matching) |
Before Matching |
Post Matching |
|
| Distance | 0.6 | 0.3 | 0.6 | 1.16 | −0.00 |
| Age | 19.41 | 19.79 | 19.57 | −0.21 | −0.09 |
| Gender (female) | 63 % | 66 % | 70 % | −0.06 | −0.15 |
| IQ | 119.63 | 123.16 | 120.47 | −0.31 | −0.07 |
| Ethnicity (Caucasian) | 30% | 63% | 35.5% | −0.70 | −0.11 |
| SES | 7.53 | 7.9 | 7.36 | −0.24 | 0.09 |
| Baseline Internalizing symptoms | 127.65 | 100.29 | 127.07 | 1.02 | 0.02 |
| Average Absolute Standardized Mean Difference2 |
− | − | − | 0.42 | 0.09 |
MT = Maltreated group (n=100), Non-MT = Non-Maltreated group (n=127), CT = Control group (i.e. matched Non-Maltreated individuals; N = 96), IQ = intelligence quotient, SES = socio-economic status (i.e. parent with highest education level).
Each standardized mean difference is obtained by subtracting the mean in the MT group minus mean in the CT group, divided by the standard deviation of the MT group.
The average absolute standardized mean difference is the average of the absolute values of standardized mean differences for all covariates.
Maltreatment status and future internalizing symptoms
Maltreatment status significantly predicted future levels of internalizing symptoms reported on average one year later (β = 16.07, βstandardized = 0.60, p < .001). The MT and CT group showed a mean internalizing symptom score at follow-up of 118.78 (s.d. = 31.34) and 102.71 (s.d. = 18.71), respectively.
Mediation analyses
A parallel mediation analysis using structural equation modelling (SEM) was run to explore the role of (i) baseline amygdala reactivity to threat and (ii) post-baseline exposure to major stressful life events on future internalizing symptoms severity. As shown in Figure 1 (path a2), maltreatment status was associated with higher threat-related baseline amygdala reactivity. Higher baseline amygdala reactivity partially mediated the association between maltreatment status and levels of future internalizing symptoms (Figure 1, indirect pathway a2 × b2). In other words, the higher levels of symptoms in the MT group followed from increased baseline amygdala reactivity.
Figure 1.
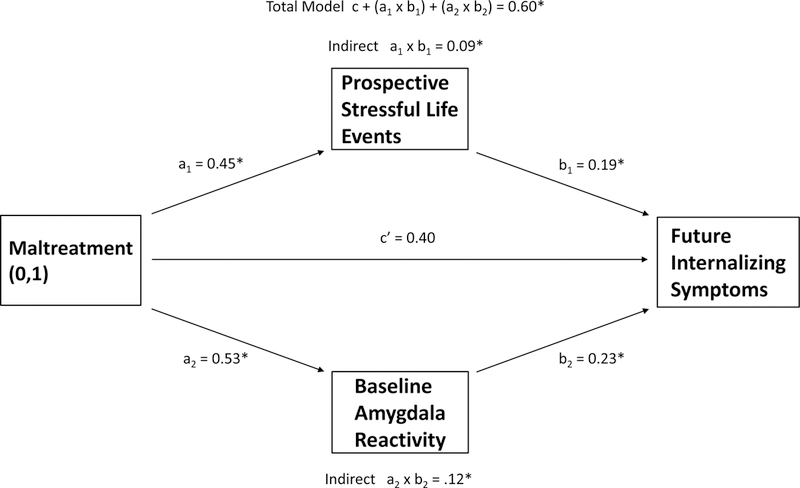
Parallel structural equation mediation model depicting how the association between future internalizing symptoms and maltreatment status is partially mediated by both baseline amygdala reactivity to threat and post-baseline exposure to major stressful life events. Note. Coefficient values are standardized; * indicates statistically significant coefficients; the interaction terms (i.e. indirect effects) significance threshold were measured using Monte Carlo test of mediation (MacKinnon, Lockwood, & Williams, 2004)
We also ran an SEM moderated mediation analysis, based on Preacher, Rucker & Hayes (2007) model 3 (Preacher, Rucker, & Hayes, 2007) (the specific path that is moderated is conceptually represented in Supplementary Figure S1). This model tested whether the mediating effect of baseline amygdala reactivity on the relationship between maltreatment status and future internalizing symptoms was conditional on post-baseline exposure to major stressful life events. This revealed that post-baseline exposure to major stressful life events did not interact with baseline amygdala reactivity in predicting future symptom levels (βstandardized = 0.05, MonteCarlo 95% CIs LL = −0.04 UL= 0.14). Moreover, the index of moderated mediation, which formally tested if the mediating effect of amygdala on the association between maltreatment status and future symptoms is influenced by exposure to major stressful life events, was also non-significant (βstandardized = 0.03, MonteCarlo 95% CIs LL = −0.03 UL= 0.09). That is, in the context of maltreatment, baseline amygdala reactivity was not found to sensitize an individual to the impact of subsequent major stressful life events.
In the parallel mediation model, we also found that maltreatment status predicted higher post-baseline occurrence of major stressful life events (path a1 in Figure 1). The mean occurrence of these (per year) for the MT and CT groups, respectively, was 4.00 (s.d. = 4.54) and 2.25 (s.d. = 3). A t-test revealed that the average rated impact of each stressful event, however, did not differ between the groups t(197) = 0.15, p = .88. In other words, individuals in the MT group experienced significantly more major stressful events, but the reported impact of individual events did not differ between the groups. Furthermore, higher post-baseline exposure to major stressful life events was found to partially mediate the association between maltreatment status and levels of future internalizing symptoms (Figure 1, indirect pathway a1 × b1). In other words, the higher levels of symptoms in the MT group followed from increased occurrence of post-baseline exposure to major stressful life events.
Finally, in the parallel mediation model, the covariation term between baseline amygdala reactivity and post-baseline major stressful life events (not graphically represented in Figure 1) was not statistically significant (βstandardized = −0.09, p =. 35). This suggests that baseline amygdala reactivity was not associated with the occurrence of post-baseline stressful life events.
Discussion
The study had three main findings. First, we found that the association between maltreatment history and future internalizing symptoms severity was partially explained by the contribution of higher baseline amygdala reactivity to threat. Second, even in this propensity score matched sample, where baseline symptoms levels and other potentially contributing factors were comparable between the groups, individuals with a history of childhood maltreatment showed a higher incidence of post-baseline major stressful life events. This, in turn, partially mediated the relationship between maltreatment status and future internalizing symptoms. Third, a history of childhood maltreatment was found to have a prognostic value for internalizing symptoms that goes above and beyond that of other factors, including baseline symptoms severity.
Several independent research groups have postulated that cognitive and neurobiological alterations in salience detection and threat reactivity may serve as mediators between the experience of childhood maltreatment and the later development of internalizing disorders (Hein & Monk, 2016; McCrory, Gerin, et al., 2017; Shackman, Shackman, & Pollak, 2007; Tottenham & Gabard-Durnam, 2017). According to the theory of latent vulnerability, maltreatment can lead to a cascade of neurocognitive recalibrations, including changes in threat processing, which may be adaptive in the context of chaotic, dangerous and species-atypical home environments (McCrory & Viding, 2015). While helpful in the short-term, these adaptations may be poorly optimized for negotiating more normative environments over the longer term. For example, changes in how an individual responds to threat can curtail opportunities and the resources necessary for developing other affective and cognitive functions. Increased amygdala reactivity, in particular, may entail an increased experience of negative emotions, reduced emotion regulation and hypervigilance.
In this study, the implementation of PSM allowed us to demonstrate that maltreatment experience is associated with increased threat-related amygdala reactivity (Hein & Monk, 2016; McCrory, Gerin, et al., 2017; Tottenham & Gabard-Durnam, 2017) even when accounting for other potentially confounding factors including concurrent internalizing symptom severity and socio-economic status, which have been linked extensively with both maltreatment (Green et al., 2010) and amygdala reactivity (Etkin & Wager, 2007; Gianaros et al., 2008; Hamilton et al., 2012). Moreover, we found that higher baseline amygdala reactivity to threat contributed (independently of major stressful life events) to the association between a history of maltreatment and future internalizing symptoms severity reported on average one year later. These findings provide unique support for the notion that the experience of childhood maltreatment may lead to neurocognitive alterations in threat processing that are not simply epiphenomenal, but rather contribute to psychiatric vulnerability later in life (McCrory & Viding, 2015).
In relation to experiential and environmental factors, we found that a higher incidence of major stressful life events partly mediated the association between maltreatment status and future internalizing symptoms severity. Again, using PSM we were able to mitigate the effects of potentially confounding factors commonly associated with childhood maltreatment known to increase the likelihood of stressful life experiences including higher internalizing symptomatology (Liu & Alloy, 2010) and lower IQ (Breslau, Lucia, & Alvarado, 2006). It has been postulated that growing up in an abusive environment can lead to alterations in a number of domains that in the longer term can compromise social and emotional functioning (McCrory, Gerin, et al., 2017). For instance, recent neurocognitive evidence indicate that children exposed to maltreatment show increased susceptibility to psychosocial stressors (Puetz et al., 2014, 2016), reduced affect regulation (McCrory, Gerin, et al., 2017), and increased rejection sensitivity associated with higher likelihood of conflictual interactions (Hernandez et al., 2016). Moreover, overgeneral autobiographical memory, commonly associated with the experience of abuse and neglect (McCrory, Puetz, et al., 2017), is thought to reduce social problem solving ability (Raes et al., 2005). One important implication is that such maladaptive social functioning may not only compromise an individual’s ability to establish and sustain positive relationships that help buffer the impact of future stressors, but also act in ways that might potentiate the generation of stressful life events (e.g. relationship breakdowns, exclusion from school, peer-victimization, and difficulties in the work environment). This concept of ‘stress generation’ has been well documented in the context of adult depression (Liu & Alloy, 2010). It will be of interest to explore in future studies, with an appropriate measure, the degree to which these stressor events are interpersonal in nature - as opposed to events like accidents or deaths among family members that are typically not thought to be related to the agency of the individual.
Our exploratory analyses did not find that individual differences in amygdala reactivity to threat were associated with the occurrence of major stressful life events. It is possible that increased amygdala reactivity may only lead to stress generation for particular forms of stress (e.g. interpersonal conflict, aggression, rejection sensitivity) that were not captured with the life events questionnaire implemented in this study. Thus, a future direction for research would be to examine these more specific occurrences of interpersonal stress to test whether amygdala reactivity is associated with stress generation for specific types of negative life events. Moreover, future neuroimaging studies will be helpful in examining whether maltreatment-related changes in other neurocognitive domains – such as reward processing, affect regulation, and autobiographical memory, etc – are associated with increased liability to stress generation.
Contrary to what has been observed in previous ‘typical’ samples - i.e. selected blind to maltreatment status (Admon et al., 2009; McLaughlin et al., 2014; Swartz et al., 2015) - we did not find that higher baseline amygdala reactivity interacted with exposure to major stressful life events in accounting for future internalizing symptoms. That is, amygdala reactivity was not found to further sensitize individuals with maltreatment histories to the impact of subsequent major stressful life events. Larger sample sizes and greater variation in stress exposure severity are necessary to replicate this finding. However, in accounting for this null finding, it is important to consider the possibility that different factors are likely to underlie the same endophenotype (increased amygdala reactivity) among those with maltreatment and non-maltreatment histories. While heightened amygdala reactivity in those with non-maltreatment histories is likely to primarily reflect an intrinsic neurobiological risk factor (Admon et al., 2009; McLaughlin et al., 2014; Swartz et al., 2015), in individuals with maltreatment histories such heightened reactivity may primarily reflect a neurocognitive response to early stress exposure and adverse experiences (Dannlowski et al., 2012; Hein & Monk, 2016; McCrory, Gerin, et al., 2017; Tottenham et al., 2011). Therefore, the way in which amygdala reactivity is implicated in stress sensitization and in the pathogenesis of psychiatric disorders may differ among individuals with and without a history maltreatment. In other words, the computational significance of the same neural index (here amygdala reactivity) will require investigation in future studies. One possibility is that baseline reactivity simply captures one part of a broader computational system that functions differently in those with maltreatment experience.
Our current analyses feature several strengths including a longitudinal design, a large sample which included a group of individuals with significant experiences of maltreatment and the implementation of PSM for the selection of a tightly matched comparison peer group. However, there are also notable limitations. First, the maltreated and non-maltreated participants consisted of university students; replication would help establish that these findings are evident in other groups within the general population. Nonetheless, the findings reported here are consistent with previous investigations characterized by samples of different educational and socioeconomic backgrounds as well as age. In particular, these prior studies also reported greater symptom severity (Green et al., 2010; Kessler et al., 2010; Nanni et al., 2012), amygdala hyperactivity (Hein & Monk, 2016; McCrory, Gerin, et al., 2017) and increased stress exposure (Finkelhor et al., 2007; Hankin, 2005; Hernandez et al., 2016; Liu et al., 2013; Uhrlass & Gibb, 2007; Widom et al., 2008) in individuals with childhood maltreatment histories. This suggests that the effects of maltreatment on multiple levels of functioning are pervasive and likely to be consistent across different populations. Second, it has been proposed that childhood maltreatment occurring earlier in life may lead to more profound alterations in amygdala functioning due to region-specific neurodevelopmental trajectories (Tottenham & Gabard-Durnam, 2017). However, the retrospective/self-reported assessments of maltreatment used in this study did not provide age of onset information. It will be important in future work to investigate the existence of sensitive periods during which the impact of maltreatment on the brain may be particularly potent. Retrospective/self-reported assessments are also poor at capturing maltreatment during infancy or early childhood and may in addition be compromised by the fact that maltreatment exposure is often associated with dissociative/overgeneral cognitive styles (e.g. McCrory, Puetz, et al., 2017) which may lead to under-reports and limited conscious awareness of the experience of abuse and neglect. Finally, it is important to note that notwithstanding the fact that we have controlled for internalising symptoms and SES within our design, it remains theoretically possible (but in our view unlikely given the variety of life events measured in our study and the propensity score matching) that a third, yet unidentified factor, drives both the occurrence of maltreatment and the increased frequency of major stressful life events. Prospective studies already demonstrate a robust association between maltreatment and future stressful life events (e.g. Finkelhor et al., 2007; Widom et al., 2014, 2008). However, a design that measures both factors contemporaneously over time is required to definitively establish a causal relationship, such that maltreatment experience can be shown to precede any increase in the frequency of major stressful life events.
In conclusion, we found that increased baseline amygdala reactivity to threat partly explains the association between a maltreatment history and future internalizing symptoms. This finding is consistent with the view that recalibration of amygdala reactivity to threat may increase stress susceptibility in the context of how everyday challenges burden and tax an individual. Future work will be necessary to investigate this possibility further. However, the current data indicated that altered amygdala reactivity was not found to increase sensitivity to major life stressors as measured via a well validated screen of stressful life events. We also provide the most definitive evidence to date that maltreatment status predicts a greater number of major stressful life events that in turn are associated with greater internalizing symptoms. These findings powerfully emphasize the way in which latent vulnerability can unfold as a result of stress generation of dependent events, akin to what has been postulated in depression (Liu & Alloy, 2010). Further work is needed to delineate the neurocognitive and social mechanisms that are associated both with increased stress susceptibility and with increased stress generation following maltreatment. Such work is crucial to inform our understanding of the pathogenesis of psychiatric disorder and guide the development of novel preventative strategies that could offset the likelihood of disorders arising in the first place (McCrory, Gerin, et al., 2017; Teicher & Samson, 2013).
Supplementary Material
Key Points.
Individuals with a history of childhood maltreatment, compared to stringently matched non-maltreated peers, showed increased amygdala reactivity to threat at baseline. This, in turn, predicted higher future internalizing symptoms.
These findings are consistent with the view that exposure to childhood maltreatment leads to functional recalibration of neural systems that are associated with poorer mental health later in life.
Individuals with a history of childhood maltreatment compared to their peers also experienced major stressful life events more frequently post baseline. This, in turn, predicted higher future internalizing symptoms.
This highlights the role that ‘stress generation’ (i.e. the increased propensity to experience negative life events) may play in the pathogenesis of psychiatric disorders following maltreatment.
Acknowledgments
The Duke Neurogenetics Study received support from Duke University as well as US-National Institute on Drug Abuse Grant R01DA033369 and R01DA031579. This work was further supported by US-National Institute on Aging Grant R01AG049789. J.B.P is a fellow of MQ: Transforming Mental Health (MQ16IP16); M.I.G. is in receipt of a PhD Impact studentship jointly funded by University College London (UCL) and the Anna Freud National Centre for Children and Families; J.R.S is supported by Prop. 63, the Mental Health Services Act and the Behavioral Health Center of Excellence at UC Davis; E.V. is a Royal Society Wolfson Research Merit Award holder. The authors would like to thank the Duke Neurogenetics Study participants and the staff of the Laboratory of NeuroGenetics. The authors have declared that they have no competing or potential conflicts of interest.
Footnotes
Conflict of interest statement: No conflicts declared.
Supporting information
Additional supporting information may be found online in the Supporting Information section at the end of this article.
References
- Admon R, Lubin G, Stern O, Rosenberg K, Sela L, Ben-Ami H, & Hendler T (2009). Human vulnerability to stress depends on amygdala’s predisposition and hippocampal plasticity. Proceedings of the National Academy of Sciences of the United States of America, 106(33), 14120–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Agnew-Blais J, & Danese A (2016). Childhood maltreatment and unfavourable clinical outcomes in bipolar disorder: a systematic review and meta-analysis. The Lancet Psychiatry, 3(4), 342–349. [DOI] [PubMed] [Google Scholar]
- Auerbach RP, Mortier P, Bruffaerts R, Alonso J, Benjet C, Cuijpers P, Demyttenaere K, et al. (2018). WHO World Mental Health Surveys International College Student Project: Prevalence and Distribution of Mental Disorders. Journal of Abnormal Psychology, ahead of print. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bernstein DP, Ahluvalia T, Pogge D, & Handelsman L (1997). Validity of the childhood trauma questionnaire in an adolescent psychiatric population. Journal of the American Academy of Child and Adolescent Psychiatry, 36(3), 340–348. [DOI] [PubMed] [Google Scholar]
- Bernstein DP, Fink L, Handelsman L, Foote J, Lovejoy M, Wenzel K, Sapareto E, et al. (1994). Initial reliability and validity of a new retrospective measure of child-abuse and neglect. American Journal of Psychiatry, 151(8), 1132–1136. [DOI] [PubMed] [Google Scholar]
- Bernstein DP, Stein JA, Newcomb MD, Walker E, Pogge D, Ahluvalia T, Stokes J, et al. (2003). Development and validation of a brief screening version of the Childhood Trauma Questionnaire. Child Abuse and Neglect, 27(2), 169–190. [DOI] [PubMed] [Google Scholar]
- Breslau N, Lucia VC, & Alvarado GF (2006). Intelligence and other predisposing factors in exposure to trauma and posttraumatic stress disorder. Archives of General Psychiatry, 63(11), 1238. [DOI] [PubMed] [Google Scholar]
- Clements K, & Turpin G (1996). The life events scale for students: Validation for use with British samples. Personality and Individual Differences, 20(6), 747–751. Pergamon. [Google Scholar]
- Danese A, & McEwen BS (2012). Adverse childhood experiences, allostasis, allostatic load, and age-related disease. Physiology and Behavior, 106(1), 29–39. [DOI] [PubMed] [Google Scholar]
- Dannlowski U, Stuhrmann A, Beutelmann V, Zwanzger P, Lenzen T, Grotegerd D, Domschke K, et al. (2012). Limbic scars: Long-term consequences of childhood maltreatment revealed by functional and structural magnetic resonance imaging. Biological Psychiatry, 71(4), 286–293. [DOI] [PubMed] [Google Scholar]
- Espejo EP, Hammen CL, Connolly NP, Brennan PA, Najman JM, & Bor W (2007). Stress sensitization and adolescent depressive severity as a function of childhood adversity: A link to anxiety disorders. Journal of Abnormal Child Psychology, 35(2), 287–299. [DOI] [PubMed] [Google Scholar]
- Etkin A, & Wager TD (2007). Functional neuroimaging of anxiety: A meta-analysis of emotional processing in PTSD, social anxiety disorder, and specific phobia. American Journal of Psychiatry, 164(10), 1476–1488. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Finkelhor D, Ormrod RK, & Turner HA (2007). Re-victimization patterns in a national longitudinal sample of children and youth. Child Abuse and Neglect, 31(5), 479–502. [DOI] [PubMed] [Google Scholar]
- Gianaros PJ, Horenstein JA, Hariri AR, Sheu LK, Manuck SB, Matthews KA, & Cohen S (2008). Potential neural embedding of parental social standing. Social Cognitive and Affective Neuroscience, 3(2), 91–96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Green JG, McLaughlin KA, Berglund PA, Gruber MJ, Sampson NA, Zaslavsky AM, & Kessler RC (2010). Childhood adversities and adult psychiatric disorders in the national comorbidity survey replication I: associations with first onset of DSM-IV disorders. Archives of general psychiatry, 67(2), 113–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hamilton JP, Etkin A, Furman DJ, Lemus MG, Johnson RF, & Gotlib IH (2012). Functional neuroimaging of major depressive disorder: a meta-analysis and new integration of base line activation and neural response data. The American journal of psychiatry, 169(7), 693–703. [DOI] [PubMed] [Google Scholar]
- Hankin BL (2005). Childhood maltreatment and psychopathology: Prospective tests of attachment, cognitive vulnerability, and stress as mediating processes. Cognitive Therapy and Research, 29(6), 645–671. [Google Scholar]
- Harkness KL, Lumley MN, & Truss AE (2008). Stress generation in adolescent depression: The moderating role of child abuse and neglect. Journal of Abnormal Child Psychology, 36(3), 421–432. [DOI] [PubMed] [Google Scholar]
- Hein TC, & Monk CS (2016). Research Review: Neural response to threat in children, adolescents, and adults after child maltreatment - a quantitative meta-analysis. Journal of Child Psychology and Psychiatry, 58(3), 222–230. [DOI] [PubMed] [Google Scholar]
- Hernandez EM, Trout ZM, & Liu RT (2016). Vulnerability-specific stress generation: Childhood emotional abuse and the mediating role of depressogenic interpersonal processes. Child Abuse and Neglect, 62, 132–141. [DOI] [PubMed] [Google Scholar]
- Hovens JGFM, Wiersma JE, Giltay EJ, Van Oppen P, Spinhoven P, Penninx BWJH, & Zitman FG (2010). Childhood life events and childhood trauma in adult patients with depressive, anxiety and comorbid disorders vs. controls. Acta Psychiatrica Scandinavica, 122(1), 66–74. [DOI] [PubMed] [Google Scholar]
- Kendler KS, Kuhn JW, & Prescott CA (2004). Childhood sexual abuse, stressful life events and risk for major depression in women. Psychological Medicine, 34(8), 1475–1482. [DOI] [PubMed] [Google Scholar]
- Kessler RC, McLaughlin KA, Green JG, Gruber MJ, Sampson NA, Zaslavsky AM, Aguilar-Gaxiola S, et al. (2010). Childhood adversities and adult psychopathology in the WHO World Mental Health Surveys. The British Journal of Psychiatry, 197(5), 378–85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liu RT, & Alloy LB (2010). Stress generation in depression: A systematic review of the empirical literature and recommendations for future study. Clinical Psychology Review. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liu RT, Choi JY, Boland EM, Mastin BM, & Alloy LB (2013). Childhood abuse and stress generation: The mediational effect of depressogenic cognitive styles. Psychiatry Research, 206(2–3), 217–222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MacKinnon DP, Lockwood CM, & Williams J (2004). Confidence limits for the indirect effect: distribution of the product and resampling methods. Multivariate Behavioral Research, 39(1), 99–128. NIH Public Access. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Manuck SB, Brown SM, Forbes EE, & Hariri AR (2007). Temporal stability of individual differences in amygdala reactivity. American Journal of Psychiatry, 164(10), 1613–1614. [DOI] [PubMed] [Google Scholar]
- Mattson WI, Hyde LW, Shaw DS, Forbes EE, & Monk CS (2016). Clinical neuroprediction: Amygdala reactivity predicts depressive symptoms 2 years later. Social Cognitive and Affective Neuroscience, 11(6), 892–898. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCrory EJ, Gerin MI, & Viding E (2017). Annual Research Review: Childhood maltreatment, latent vulnerability and the shift to preventative psychiatry – the contribution of functional brain imaging. Journal of Child Psychology and Psychiatry, 58(4), 338–357. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCrory EJ, Puetz VB, Maguire EA, Mechelli A, Palmer A, Gerin MI, Kelly PA, et al. (2017). Autobiographical memory: a candidate latent vulnerability mechanism for psychiatric disorder following childhood maltreatment. The British Journal of Psychiatry, 211(4), 216–222. Royal College of Psychiatrists. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCrory EJ, & Viding E (2015). The theory of latent vulnerability: Reconceptualizing the link between childhood maltreatment and psychiatric disorder. Development and Psychopathology, 27(2), 493–505. [DOI] [PubMed] [Google Scholar]
- McLaughlin KA, Busso DS, Duys A, Green JG, Alves S, Way M, & Sheridan MA (2014). Amygdala response to negative stimuli predicts PTSD symptom onset following a terrorist attack. Depression and Anxiety, 31(10), 834–842. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McLaughlin KA, Conron KJ, Koenen KC, & Gilman SE (2010). Childhood adversity, adult stressful life events, and risk of past-year psychiatric disorder: A test of the stress sensitization hypothesis in a population-based sample of adults. Psychological Medicine, 40(10), 1647–1658. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nanni V, Uher R, & Danese A (2012). Childhood maltreatment predicts unfavorable course of illness and treatment outcomes in depression: A meta-analysis. The American Journal of Psychiatry, 169(2), 141–151. [DOI] [PubMed] [Google Scholar]
- Prather AA, Bogdan R, & Hariri AR (2013). Impact of sleep quality on amygdala reactivity, negative affect, and perceived stress. Psychosomatic Medicine, 75(4), 350–358. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Preacher KJ, Rucker DD, & Hayes AF (2007). Addressing moderated mediation hypotheses: Theory, methods, and prescriptions. Multivariate Behavioral Research, 42(1), 185–227. [DOI] [PubMed] [Google Scholar]
- Puetz VB, Kohn N, Dahmen B, Zvyagintsev M, Schüppen A, Schultz RT, Heim CM, et al. (2014). Neural response to social rejection in children with early separation experiences. Journal of the American Academy of Child and Adolescent Psychiatry, 53(12), 1328–1337.e8. [DOI] [PubMed] [Google Scholar]
- Puetz VB, Viding E, Palmer A, Kelly PA, Lickley R, Koutoufa I, Sebastian CL, et al. (2016). Altered neural response to rejection-related words in children exposed to maltreatment. Journal of Child Psychology and Psychiatry and Allied Disciplines, 57(10), 1165–1173. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Radford L, Corral S, Bradley C, Fisher H, Bassett C, Howat N, & Collishaw S (2011). Child Abuse and Neglect in the UK Today: Research into the prevalence of child maltreatment in the United Kingdom National Society for the Prevention of Cruelty to Children (NSPCC). London. [Google Scholar]
- Raes F, Hermans D, Williams MJ, Demyttenaere K, Sabbe B, Pieters G, & Eelen P (2005). Reduced specificity of autobiographical memory: A mediator between rumination and ineffective social problem-solving in major depression? Journal of Affective Disorders, 87(2–3), 331–335. [DOI] [PubMed] [Google Scholar]
- Shackman JE, Shackman AJ, & Pollak SD (2007). Physical abuse amplifies attention to threat and increases anxiety in children. Emotion, 7(4), 838–852. [DOI] [PubMed] [Google Scholar]
- Stoltenborgh M, Bakermans-Kranenburg MJ, Alink LRA, & van IJzendoorn MH (2015). The prevalence of child maltreatment across the globe: Review of a series of meta-analyses. Child Abuse Review, 24(1), 37–50. [Google Scholar]
- Swartz JR, Knodt AR, Radtke SR, & Hariri AR (2015). A neural biomarker of psychological vulnerability to future life stress. Neuron, 85(3), 505–511. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Teicher MH, & Samson JA (2013). Childhood maltreatment and psychopathology: A case for ecophenotypic variants as clinically and neurobiologically distinct subtypes. The American journal of psychiatry, 170(10), 1114–33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tottenham N, & Gabard-Durnam LJ (2017). The developing amygdala: a student of the world and a teacher of the cortex. Current Opinion in Psychology, 17, 55–60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tottenham N, Hare TA, Millner A, Gilhooly T, Zevin JD, & Casey BJ (2011). Elevated amygdala response to faces following early deprivation. Developmental Science, 14(2), 190–204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Uhrlass DJ, & Gibb BE (2007). Childhood emotional maltreatment and the stress generation model of depression. Journal of Social and Clinical Psychology, 26(1), 119–130. [Google Scholar]
- Watson D, Clark LA, Weber K, Assenheimer JS, Strauss ME, & McCormick RA (1995). Testing a tripartite model: II. Exploring the symptom structure of anxiety and depression in student, adult, and patient samples. Journal of abnormal psychology, 104(1), 3–14. [DOI] [PubMed] [Google Scholar]
- Whalen PJ, Davis CF, Oler JA, Kim H, Kim JM, & Neta M (2009). Human amygdala responses to facial expressions of emotion In Whalen PJ & Phelps EA (Eds.), The human amygdala (p. 265–288.). Guilford Press. [Google Scholar]
- Widom CS, Czaja S, & Dutton MA (2014). Child abuse and neglect and intimate partner violence victimization and perpetration: A prospective investigation. Child abuse & neglect, 38(4), 650–663. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Widom CS, Czaja SJ, & Dutton MA (2008). Childhood victimization and lifetime revictimization. Child Abuse and Neglect, 32(8), 785–796. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.