

Abstract
In spite of the growing literature on prevalence and patterns of health care use in later life globally, studies have generally overlooked subjective standpoints of vulnerable Ghanaian older people obstructing the achievement of the United Nations’ health-related Sustainable Development Goals. We examined the prevalence and patterns of health care use among poor older people in the Atwima Nwabiagya District of Ghana. Cross-sectional data were obtained from an Aging, Health, Lifestyle and Health Services Survey conducted between June 1 and 20, 2018 (N = 200). Chi-square and Fisher’s exact tests were carried out to estimate the differences between gender and health care utilization with significant level of less than or equal to 0.05. Whereas, 85% of the respondents utilized health care, females were higher utilizers (88% vs. 75%) but males significantly incurred higher health care expenditure. The majority utilized health services on monthly basis (38%) and consulted public health care providers (77%). While 68% utilized services from hospitals, most sourced health information from family members (54%) and financed their health care through personal income (45%). The study found that the Livelihood Empowerment Against Poverty grant played a little role in reducing health poverty. Stakeholders should review social programs that target poor older people in order to improve their well-being and utilization of health care.
Keywords: Health care use, Livelihood Empowerment Against Poverty, Poor older people, Health information
Introduction
Statistics available show the increasing nature of the aging population in the world particularly in sub-Saharan Africa (Ghana Statistical Service [GSS], 2013; Kwankye, 2013; Olukoya, 2014; Oyetunde, Ojo, & Ojewale, 2013; United Nations [UN], 2015, 2017; World Health Organization [WHO], 2015a, 2015b). In 2015, there were 901 million people aged 60 years or above globally. By 2050, nearly 2.1 billion people in the world are projected to reach 60 years or above. The population of older people aged 65 years or above in Africa in 2015 was 64.4 million. However, two thirds of the world’s older people live in the developing countries, of which their numbers are rising faster than in the developed countries (UN, 2015). In Ghana, the older population is growing rapidly (GSS, 2013) and this is causing an increase in the dependence level with numerous negative effects on their health and well-being (Van Der Wielen, Channon & Falkingham, 2018).
The rise in the population of older persons worldwide is due to the decline in fertility rates, increasing life expectancy (Balcombe, 2001; GSS, 2013; Kwankye, 2013; UN, 2017), improved medical care (UN, 2015), improvement in nutrition, health care education, and income (Balcombe, 2001). Life expectancies between the periods 1950-1955, 2000-2005 were 46.6 and 66 years, respectively and are predicted to hit 76 years by 2045-2050 (Mba, 2010). However, the increase in the aging population is expected to be accompanied by increasing number of cardio vascular diseases (Agyemang et al., 2012; Weiskopf, Weinberger, & Grubeck-Loebenstein, 2009) because older people have weak immune system which either cannot withstand diseases (Weiskopf et al., 2009) or become more susceptible to diseases and infections (Viña, Borrás, & Miquel, 2007). Older people in Low -and Middle- Income Countries (LMICs) tend to suffer from a wide range of health problems (Gyasi & Phillips, 2018) comprising communicable and noncommunicable diseases (Aboderin & Beard, 2015; Awoke et al., 2017; WHO, 2014), such as high blood pressure (14%), arthritis (14%), and anemia (76%) (WHO, 2015a), diabetes, kidney disease (Robinson, 2007), musculoskeletal conditions, respiratory problems, and oral health (WHO, 2014). Consequently, there is the need to understand their utilization of health care services (Nyamezea, 2017). It is argued that with increasing aging population, the use of health care would also increase (Guo, Du, Hu, & Zheng, 2016), because of the multiple diseases associated with aging (Awoke et al., 2017; Bernstein et al., 2003).
In spite of the growing literature on prevalence and patterns of health care use in later life globally, studies have generally overlooked the subjective standpoints of vulnerable Ghanaian older people obstructing the achievement of the UN Sustainable Development Goal 3; to ensure healthy lives and promote well-being for all at all ages. In addition, there are limited studies on the extent of use of health care, sources of information on health care, and health care expenditure among poor older people in Ghana. A better understanding of the prevalence and patterns of health care use among poor older people has become important following upsurge of communicable and noncommunicable diseases in later life and the need for social policy to improve older people’s health. This study, therefore, examined the prevalence and patterns of health care use among poor older people enrolled in the Livelihood Empowerment Against Poverty (LEAP) program in the Atwima Nwabiagya District of Ghana. The LEAP is a financial transfer policy sponsored by the Government of Ghana (GOG), the World Bank, and the UN International Children’s Emergency Fund to give financial protection to households and people considered as extremely poor (Handa et al., 2013; Ministry of Manpower, Youth and Employment, 2007). It also provides free national health insurance enrollment for poor older people with the aim of improving their health care use (Handa et al., 2013). Beneficiaries of LEAP program include older persons who are 65 years or above, persons with disability, and orphaned and vulnerable children (Handa et al., 2013; Peprah, Kyiyaga, Afful, Abalo, & Agyemang-Duah, 2017). Furthermore, it seeks to improve the livelihood and health care use of the beneficiaries to better socioeconomic development of the country (Ministry of Gender, Children and Social Protection, 2016). The beneficiaries receive a bimonthly minimum and maximum amount of GH¢ 64 and 106 (US$13.42-22.23),1 respectively (Agyemang-Duah, Peprah, & Peprah, 2019b). The individual decides on how to use the money either for health care or other basic needs (Agyemang-Duah et al., 2019b). Poor older people were considered to be persons aged 65 years or above receiving financial support from the LEAP program (Agyemang-Duah, Peprah, & Peprah, 2019a; Agyemang-Duah et al., 2019b).
For this study, the Health Belief Model (HBM) was used as a theoretical framework to explain health behavior and the reason behind the use of health care services (Rosenstock, 1974). From the HBM, it is argued that people have the likelihood of accepting health recommendation such as visiting health facility if they have the motive to do so (Rosenstock, 1974, 1988). Persons who believe to be susceptible to a particular condition are most likely to follow a particular health action (Conner, 2010). However, Henshaw & Freedman-Doan (2009) maintained that HBM provides a structure for developing and evaluating programs designed to increase mental health awareness and appropriate utilization. Leavitt (1979) also argued that the single best predictor of utilization is a person’s belief of his own susceptibility to disease, followed by belief of benefits associated with preventive health behavior. The HBM model employed for the study would help people understand the factors and health conditions that result in utilization of health care and its patterns among poor older people. This study is important in two areas. First, it is critical to health policy design and planning which would help in improving health care services delivery. Second, it will help health decision makers and institutions to increase access to health care that would contribute to the attainment of Sustainable Development Goal 3 that focuses on ensuring healthy lives and promoting well-being for all at all ages by 2030.
Method
Sample and Data
The empirical analysis of the study used data from an Aging, Health, Lifestyle and Health Services (AHLHS) survey. It involved a cross sectional survey conducted between June 1 and 20, 2018. This study was to investigate the prevalence and patterns of health care use among poor older people under the LEAP program in the Atwima Nwabiagya District of Ghana. In this study, health care utilization was operationalized as seeking services offered by medical providers including nurses, and doctors in a form of contact (Exavery, 2010; Saeed, Xicang, Yawson, Nguah, & Nsowah-Nuamha, 2015). Although, many international, regional, and local aging studies have employed 50 or more years benchmark to define older person including the WHO’s survey on Global Ageing and Adult Health (Awoke et al., 2017; Bourne et al., 2010; Dogbey, 2015; Gyasi & Phillips, 2018; Saeed et al., 2015; Saeed et al., 2016; Zotorvie, 2015), this study defined an older person using the chronological age as a person who has attained 65 years or above (Adei, Anning, & Mireku, 2015; Hsu & Hsu, 2016), which was in line with the criteria for enrolling poor older people in the LEAP program in the study area and more broadly Ghana.
The AHLHS survey involved 200 study participants in 16 randomly selected communities in the study district through cluster and simple random sampling techniques. A simple random sampling technique was used to recruit the respondents which helped to ensure fairness and transparent sampling procedure. This ensured that every respondent has an equal chance of taking part in the study (WHO, 2001a). Furthermore, simple random sampling was employed in this study because the list of the subject was available. The applicability of the simple random sampling is that it is mostly employed in medical research (Elfil & Negida, 2017). The actual sampling and selection procedure followed eight main stages. First, the list of all beneficiaries of the LEAP program from the Department of Social Welfare, Atwima Nwabiagya District Assembly was obtained. Second, a total number of 401 poor older people aged 65 years or above was extracted. Third, a required sample size (N = 200) was estimated based on Miller & Brewer’s (2003) formula for sample size estimation. This method of determining sample size is representative, generalizable, and has been applied in various aging studies in Ghana (Adei et al., 2015; Anning, 2012). Fourth, a blindfolded person was made to select the required sample size allotted for each study community without replacement until the assigned sample for each community was obtained. Fifth, the sample was distributed among the randomly selected communities based on proportion. Sixth, the selected sample was taken to the various chosen communities for the data collection exercise to start. In this case, the selection procedures were thoroughly explained to each of the recruited respondents. Seventh, the randomly selected respondents were invited to take part in the study. Lastly, provision was made such that if any of the randomly selected respondents was not available or declined to participate in the study, the selection process was repeated to get a replacement. However, there was no such case in this study.
To ensure the vast heterogeneous population and socioeconomic background of poor older people under the LEAP program, all geographical areas were fully represented for true and representative findings. Thus far, the study district was clustered into three geographical areas; North (Abira, Boahenkwaa, Adagya, and Wurapong), Central (Kontomire, Hiawu-Besease, Kyereyease, and Apuyem), and South (Amanchia, Koben, Seidi, Fankamawe, Nkorang, and Nkaakom) where an estimate of 32, 67, and 101 of the total sample size was, respectively, allocated based on proportion. The selection of the study participants followed exclusion and inclusion of criteria paradigm. Whereas all poor older people aged 65 or older who agreed to participate in the study and were enrolled in the LEAP program were included in the study, those who were sick as at the time of the survey were excluded from the study.
Outcome Measures and Data Collection Processes
This paper was extracted from a wider AHLHS survey which focused on prevalence and patterns of health care use among poor older people under the LEAP program in the Atwima Nwabiagya District of Ghana. Health care use was the outcome variable operationalized as dummy variable indicating utilization or non-utilization of health care within a 12-month period preceding the survey. This 12 months estimate rate of health care use outcome is found to be consistent with previous studies (Amente & Kebede, 2016; Brinda, Attermann, Gerdtham, & Enemark, 2016; Suominen-Taipale, Martelin, Koskinen, Holmen, & Johnsen, 2006). The baseline characteristics were collected in relation to gender, age, marital status, ethnicity, religion, education, income, family support, and health insurance. Also, data on the health conditions of the respondents and their perceived health status were collected. It further considered pertinent variables on patterns and health care use such as whether respondents have sought health care for health problems in the last 1 year, number of times a respondent has used health care in the last 1 year, frequency of health care, sources of information on health care, health care expenditure, type of health care provider, kind of health care facility, number of times a respondent seeks health care after detecting a symptom, those that decide the type of health care for respondents, number of kilometers a respondent travels to access health care, means of getting to the hospital, health items a respondent spend their income on, and sources of income to pay for medical bills.
Data were collected through face-to-face interviewer administered questionnaire to elicit data from qualified study participants. The survey questionnaire was written in English language. Due to the low educational level of the respondents, the interviews were conducted in Twi but the responses were written in English Language. Three graduate students with background in Medical Geography, and Health and Development from the Department of Geography and Rural Development, Kwame Nkrumah University of Science and Technology, Ghana, were recruited and trained to assist in the data collection process. The research assistants were given training for 2 days. With this, the first author explained the purpose of the study to them and monitored the data collection process. In all, each administered questionnaire lasted between 30 and 40 min.
Ethics and Consent to Participate
All ethical considerations with regard to the Declaration of Helsinki were considered (World Medical Association, 2001). This study was approved by the Committee on Human Research Publication and Ethics (CHRPE), Kwame Nkrumah University of Science and Technology School of Medical Sciences, and Komfo Anokye Teaching Hospital, Kumasi, Ghana (CHRPE/AP/311/18). Study respondents were fully briefed on the study purpose and the procedure of the data collection process. Both written and verbal informed consents were obtained from the study participants. Also, the study participants were further assured of the strict confidentiality of the information they provided.
Analytical Techniques
Data were verified, carefully checked for inconsistencies and cross-reference was made to the original questionnaires to inform modifications and corrections. The primary data were entered into database and analyzed statistically using SPSS software (Version 16.0). Descriptive statistics were performed to describe the background characteristics of the study sample. A non-parametric Pearson’s chi-square (χ²) and Fisher’s exact tests were performed to compare prevalence and patterns of health care use with gender. The interpretation of test results took into consideration probability value of less than or equal to 0.05 as significant. Data were organized and presented by frequency tables and proportionate counts.
Results
Sample Characteristics of the Study Participants
Table 1 presents data on the sociodemographic characteristics of the respondents in the study area. Majority of the respondents were females (78%), aged 65 to 69 (29%), single (74%), had no formal education (63%), belonged to the Akan ethnic group (84%), and professed Christian faiths (83%). The trend that majority of the respondents were females is not surprising because about 75% of the beneficiaries enrolled in the LEAP program in Ghana and in particular the study area are females. Due to the gendered dimension of poverty in Ghana, the LEAP program seeks to empower vulnerable people especially, women to escape from poverty. Most (38%) of the respondents received earned monthly income of less than GH¢100% ($20.96) and 96% had enrolled in the NHIS . Only a few (38%, n = 76) respondents received family support.
Table 1.
Sociodemographic Characteristics of the Study Sample.
| Variable | Category | n = 200 | % |
|---|---|---|---|
| Gender | Male | 44 | 22.0 |
| Female | 156 | 78.0 | |
| Age | 65-69 | 58 | 29.0 |
| 70-74 | 40 | 20.0 | |
| 75-79 | 23 | 11.5 | |
| 80-84 | 29 | 14.5 | |
| 85-89 | 14 | 7.0 | |
| 90 and above | 36 | 18.0 | |
| Ethnic Group | Akan | 168 | 84.0 |
| Northerner | 32 | 16.0 | |
| Religion | Christianity | 165 | 82.5 |
| Islam | 29 | 14.5 | |
| African Traditional Religion | 6 | 3.0 | |
| Marital Status | Single | 148 | 74.0 |
| Married | 52 | 26.0 | |
| Education | No formal education | 125 | 62.5 |
| Basic school education | 54 | 27.0 | |
| High school education | 21 | 10.5 | |
| Monthly income (GH¢) | 100.00 or less ($20.96) | 76 | 38.0 |
| 101.00-200.00 ($21.17-41.93) | 75 | 37.5 | |
| 201.00-300.00 ($42.14-62.89) | 35 | 17.5 | |
| Above 300 ($62.89) | 14 | 7.0 | |
| Ever registered for health insurance | Yes | 192 | 96.0 |
| No | 8 | 4.0 | |
| Received family support | Yes | 76 | 38 |
| No | 124 | 62 |
Note. NHIS = National Health Insurance Scheme.
Prevalence and Patterns of Health care Use
The study found a higher utilization of health care (85%) among poor older people for the past 1 year preceding the survey (Table 2). Females (88% vs. 75%) were higher utilizers of health care services compared to the males (p = .035). In terms of frequency of health care utilization in the last year preceding the survey, 11% had used health care services at least once. While most (49%) had utilized health care services for 5 times or more, 18% had used it twice. About 38% reported that they utilized health care services on a monthly basis, 4% and 24.7% used it every week and 2 weeks, respectively. Whereas more females (24.8%) than males (24.2%) utilized health care services every week, more males (39.4%) than females (37.2%) utilized health care services every month but it was not statistically significant (p = .999). More respondents consulted public health care providers (77%) than the private health care providers (23%). Also, more males (79%) than females (77%) consulted public health care providers. On the contrary, more females (23%) consulted private health care providers than the males (21%). There was no statistically significant association between gender and the kind of provider or the facility a respondent seeks health treatment from (p = .792) (Table 2).
Table 2.
Prevalence and Patterns of Health care Use by Gender.
| Variable | Category | Male (n = 44) |
Female (n = 156) |
Total = 200 |
p value |
|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | |||
| Have you ever sought formal health care for your health problems in the last 1 year | Yes | 33 (75) | 137 (87.8) | 170 (85) | .035 |
| No | 11 (25) | 19 (12.2) | 30 (15) | ||
| How many times have you sought formal health care in the last 1 year? | 1 | 4 (12.1) | 14 (10.2) | 18 (10.6) | .976 |
| 2 | 5 (15.2) | 26 (19) | 31 (18.2) | ||
| 3 | 3 (9.1) | 12 (8.8) | 15 (8.8) | ||
| 4 | 5 (15.2) | 17 (12.4) | 22 (12.9) | ||
| 5 or more | 16 (48.5) | 68 (49.6) | 84 (49.4) | ||
| How often did you seek formal health care? | Every week | 1 (3) | 5 (3.6) | 6 (3.5) | .999 |
| Every 2 weeks | 8 (24.2) | 34 (24.8) | 42 (24.7) | ||
| Every month | 13 (39.4) | 51 (37.2) | 64 (37.6) | ||
| Every 3 months | 5 (15.2) | 22 (16.1) | 27 (15.9) | ||
| More than 3 months | 6 (18.2) | 25 (18) | 31 (18.2) | ||
| What type of health provider or facility did you consult most? | Public health facility | 26 (78.8) | 105 (76.6) | 131 (77.1) | .792 |
| Private health facility | 7 (21.2) | 32 (23.4) | 39 (22.9) | ||
| What kind of health facility (either public or private) do you normally use? | Hospital | 24 (72.7) | 92 (67.2) | 116 (68.2) | .819 |
| Clinic | 7 (21.2) | 34 (24.8) | 41 (24.1) | ||
| Health center | 2 (6.1) | 11 (8) | 13 (7.6) | ||
| Community-Based Health Planning and Services (CHPS) compound | 0 (0) | 0 (0) | 0 (0) | ||
| How early did you seek health care for your health problems after detecting the symptoms? | Immediately/in a day | 3 (9.1) | 16 (11.7) | 19 (11.2) | .860 |
| 3 days | 13 (39.4) | 57 (41.6) | 70 (41.2) | ||
| 4-6 days | 8 (24.2) | 22 (16.1) | 30 (17.6) | ||
| Between a week and a month | 8 (24.2) | 37 (27) | 45 (26.5) | ||
| More than a month | 1 (3) | 5 (3.6) | 6 (3.5) | ||
| Who mostly decide the type of health care for you? | Based on their own decision | 16 (48.5) | 77 (56.2) | 93 (54.7) | .587 |
| Family members | 15 (45.4) | 46 (33.6) | 61 (35.9) | ||
| Friends | 2 (6.1) | 13 (9.5) | 15 (8.8) | ||
| Health care providers | 0 (0) | 1 (0.7) | 1 (0.6) |
p < .05.
Concerning the kind of health care facility respondents normally use, the responses were hospital (68%), clinic (24%), and health center (8%), respectively. Majority of the male participants (73%) utilized more hospitals than females (67%) but this was statistically insignificant (p = .819). About 41% declared that they sought health care every 3 days after detecting the symptoms, with 11% seeking health care immediately or in a day after detecting the symptoms. Just 4% sought health care beyond a month after detecting the symptoms (Table 2). More females (42%) than males (39%) sought health care to solve their health problems 3 days after detecting the symptoms. The respondents (N = 170) utilized health care to prevent diseases and poor health (49%), to improve their general health (35%), and for early detection of disease (16%) (Figure 1).
Figure 1.
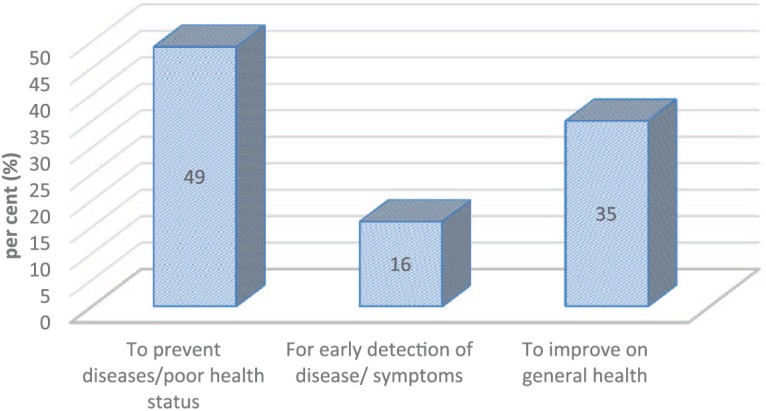
Reasons for using health care.
Perceived Health Status and Chronic Non-Communicable Diseases (NCDs) Among the Respondents
In Figure 2, 42% of the respondents rated their health as poor with 20% describing their health as good. With regard to the incidence of NCDs, hypertension (high blood pressure; 51.7%) was the most prevalent disease suffered by the respondents followed by diabetes (28.3%), eye problem (12%), stroke (4.5%), bones and joint disorder (3%), and ear problem (2.5%)*. Other diseases included asthma (1%), arthritis (1%), chronic kidney disease (1%), depression (1%), insomnia (1%), cancer (0.5%), and respiratory diseases (0.5%) (Figure 3).
Figure 2.

Perceived health status of the respondents.
Figure 3.

Chronic non-communicable diseases among the respondents.
Note. Sum of percentages is more than 100 as multiple responses were possible.
Sources of Health care Information and Decision
More than half (55%) of the respondents made their own decision regarding where to seek health care. About 36% and 9% of the respondents consulted family members and friends, respectively, concerning health care utilization. Regarding the sources of information on health care utilization, multiple sources were reported comprising family members (54%), friends (21%), health care professionals (14%), media (11%), and literature (1%). However, there was no statistically significant difference between gender and sources of information on health care utilization (p = .269).
Health care Accessibility Information
In terms of kilometers covered to access or use health care, 13% reported that they traveled 1 km. While majority (33%) traveled 2 km to access health care, 31.2% traveled 5 or more km to access health care. More males (49%) than females (29%) traveled 2 km to access health care services in the study area (Table 2). Regarding the means of transport used to access health care facilities, majority (82%, n = 139) of the respondents mentioned that they used commercial vehicles. More females (83%) than males (79%) relied on commercial vehicle such as minicabs (“trotro”) and taxis to access health care in the study area (Table 3). In addition, more male health care users (12%) than females (8%) used motor bikes to access health care services. In relation to waiting time, 61% of the respondents spent between 20 to 40 min before seeing a health care provider (Table 3). In general, females (26%) waited for a longer time at the health care facility than males (24%) as they spent more than 40 min at the health care facility before seeing a doctor (p = .030).
Table 3.
Prevalence and Patterns of Health care Use by Gender (Continued).
| Variable | Category | Male (n = 44) |
Female (n = 156) |
Total = 200 |
p value |
|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | |||
| Where do you normally seek health care information from? | Health professionals | 4 (12.1) | 20 (14.6) | 24 (14.1) | .269 |
| Family | 19 (57.6) | 72 (52.6) | 91 (53.5) | ||
| Friends | 5 (15.2) | 31 (22.6) | 36 (21.2) | ||
| Media | 4 (12.1) | 14 (10.2) | 18 (10.6) | ||
| Drug stores | 0 (0) | 0 (0) | 0 (0) | ||
| Literature | 1 (3) | 0 (0) | 1 (0.6) | ||
| How many kilometers do you cover to access/use health care? | Less or equal to 1 km | 1 (3) | 21 (15.3) | 22 (12.9) | .057 |
| 2 km | 16 (48.5) | 40 (29.2) | 56 (32.9) | ||
| 3 km | 2 (6.1) | 26 (19) | 28 (16.5) | ||
| 4 km | 2 (6.1) | 9 (6.6) | 11 (6.5) | ||
| 5 or more | 12 (36.4) | 41 (29.9) | 53 (31.2) | ||
| How do you get to the health facility? | Walking | 1 (3) | 9 (6.6) | 10 (5.9) | .407 |
| Motor bike | 4 (12.1) | 11 (8) | 15 (8.8) | ||
| Bicycle | 2 (6.1) | 2 (1.5) | 4 (2.4) | ||
| Commercial vehicle | 26 (78.8) | 113 (82.5) | 139 (81.8) | ||
| Private vehicle | 0 (0) | 2 (1.5) | 2 (1.2) | ||
| Tricycle/Aboboyaa | 0 (0) | 0 (00) | 0 (0) | ||
| How long do you wait at the health facility before you see a doctor? | Less than 20min | 0 (0) | 23 (16.8) | 23 (13.5) | .030 |
| 20-40 min | 25 (75.8) | 79 (57.7) | 104 (61.2) | ||
| More than 40 min | 8 (24.2) | 35 (25.5) | 43 (25.3) | ||
| How much do you spend when you visit health care? | Less than GH ¢50 ($10.48) | 4 (12.1) | 39 (28.5) | 43 (25.3) | .004 |
| GH¢ 50-100 ($10.48-20.96) | 15 (45.5) | 75 (54.7) | 90 (52.9) | ||
| More than GH¢100 ($20.96) | 14 (42.4) | 23 (16.8) | 37 (21.8) | ||
| Which of the following best describes your regular source of funds to pay for your health care cost? | Personal income | 13 (39.4) | 64 (46.7) | 77 (45.3) | .716 |
| NHIS subscription | 10 (30.3) | 29 (21.2) | 39 (22.9) | ||
| Social support network | 0 (0) | 3 (2.2) | 3 (1.8) | ||
| Family members | 8 (24.2) | 32 (23.4) | 40 (23.5) | ||
| Friends | 0 (0) | 3 (2.2) | 3 (1.8) | ||
| LEAP grant | 2 (6.1) | 6 (4.4) | 8 (4.7) | ||
| Which health care item do you mostly spend your income on? | Health aide | 2 (6.1) | 1 (0.7) | 3 (1.8) | .180 |
| Long-term care | 3 (9.1) | 12 (8.8) | 15 (8.8) | ||
| Ambulance | 0 (0) | 4 (2.9) | 4 (2.4) | ||
| In-patient | 4 (12.1) | 7 (5.1) | 11 (6.5) | ||
| Out-patient | 7 (21.2) | 32 (23.4) | 39 (22.9) | ||
| Drugs | 17 (51.5) | 81 (59.1) | 98 (57.6) | ||
| In general, are you satisfied with health care use? | Yes | 26 (78.8) | 95 (69.3) | 121 (71.2) | .282 |
| No | 7 (21.2) | 42 (30.7) | 49 (28.8) |
Note. NHIS = National Health Insurance Scheme; LEAP = Livelihood Empowerment Against Poverty.
p < .05.
Health care Expenditure and Satisfaction
More than half (53%) of the respondents spent GH¢50 to GH¢100 ($10.48-20.96) anytime they access health care. However, majority of the males (42%) spent more than GH¢100 ($20.96) on health care compared with their female colleagues (p = .004). Sources of funds for health care among the respondents included personal income (45%), National Health Insurance Scheme (NHIS) subscription (23%), social support network (2%), family members (24%), and LEAP subvention (5%) (Table 3). More females (47%) than males (39%) relied on personal income to pay for their medical expenses. In addition, greater fraction of the respondents spent their income on drugs (58%) followed by out-patient (23%), in-patient (7%), ambulance (2%), long-term care (9%), and health aide (2%). The results showed statistically insignificant difference between male and female in relation to the kind of health care items respondents spend their income on (p = .180). In total, 71% (n = 121) of the respondents reported that they were satisfied with health care use but the males were more satisfied than the females (79% vs. 69%) (Table 3).
Discussion
Despite the effort of the GOG through the LEAP program to reduce poverty among poor older people, there is no information on the contribution of the LEAP to health care services utilization by poor older people in Ghana. In relation to this, the study examined the prevalence and patterns of health care utilization among poor older people under the LEAP program. Overall, our study found a higher prevalence (85%) of health care utilization among poor older people in the Atwima Nwabiagya District of Ghana. Yet, it cannot largely be attributed to the enrollment of poor older people under the LEAP scheme. As the findings revealed, the LEAP grant provided a small portion (5%) of the health expenditure of poor older people investigated by this study in the Atwima Nwabiagya District. The findings revealed that majority of the poor older people enrolled in the LEAP program spent between GH¢ 50 ($10.48) and GH¢100 ($20.96) on health care anytime they visit health facility. Comparing these amounts spent on health care and the LEAP grant received by the poor older people bimonthly (between GH¢ 64 and GH¢106 [$13.42-22.23]), it could be argued that the grant is not sufficient to cater their health care needs and other basic needs such as food and clothing. Those whose health care expenditure exceeded the LEAP grant received bimonthly sought support from other health financing sources. However, the LEAP program is still important because it provides poor older people with a source of income to reduce their poverty conditions. Thus, there should be an upward adjustment of the LEAP grant by the GOG.
Our study found that health care services utilized by poor older people were financed mostly through personal income regardless of the introduction of NHIS. In spite of the fact that NHIS increases the use of health care services (Ansah et al., 2009; Gyasi, Phillips, & Buor, 2018; Hanvoravongchai & Hsiao, 2007; Kim & Lee, 2016; Schneider & Hanson, 2006), some poor older individuals were skeptical about the services provided by physicians and nurses, hence they paid for their treatment instead of the NHIS privileges. Gyasi et al. (2018) argued that the use of health care services among older people irrespective of their economic status is chiefly a function of health status and perceived personal health beliefs rather than just a NHIS enrollment. The NHIS subscription serving as a source of funds for health care for poor older people agreed with earlier studies conducted in Ghana. For instance, the NHIS as a pro-poor policy helped the poor and vulnerable populations such as the older people access health care services and reduce their health care costs (Agyepong & Adjei, 2008; Gyasi et al., 2018). In Ghana, health insurance was introduced to get rid of the financial barrier to health care and user fees at the point of use (Saeed et al., 2015). Also, social support networks provided an avenue for few poor older people to get funds to access health care services when their health insurance do not cover treatment or they do not have money to pay for their health treatment. From the HBM perspective, poor older people who believed that services provided for NHIS enrollees were not good would resort to different medical treatment that demands payment. However, poor older people who paid for their medical bills with their personal income instead of using NHIS subvention might be as a result of their perceived health beliefs and philosophies. Unsurprisingly, the study found that support from family members constituted an important source of funds for health care for poor older people. This is consistent with previous studies that reported similar findings (Agyemang-Duah et al., 2019b; Gyasi et al., 2018). For example, Gyasi et al. (2018) found that social support obtained from friends, relatives, and community members provided avenues for health information delivery and other assistance in the form of funds for traveling and payment of health care use. We found insignificant difference between gender and sources of funds for health care.
Although it can be argued that the study focused on poor older people, it is consistent with previous studies that found a higher prevalence (90%) of health care services utilization of older people in Germany (Hajek, Bock, & König, 2017). As argued by Awoke et al. (2017), biological process of aging and multiple chronic conditions cause older people to utilize more of health care services. Gyasi et al. (2018) also assert that presence of chronic health conditions, self-rated health, and functional impairment are the variables that strongly relate to health care use in later life. Besides, poor older persons often bear higher portion of disease and require regular health care (Gyasi et al., 2018), which in turn lead to frequent use of health facilities. However, other studies in Ethiopia and rural South Africa reported a lower prevalence rate of 49.6% and 45%, respectively (Amente & Kebede, 2016; Gómez-Olivé, Thorogood, Clark, Kahn, & Tollman, 2013). These results could be due to differences in sociocultural factors, methodology, and study settings. The study discovered that poor older females were significantly higher utilizers of health care services compared with their male counterparts. In congruent to this study, a large body of scholarships had reported a correlation between gender and the use of health care services (Galdas, Cheater, & Marshall, 2005; Gerritsen & Devillé, 2009; Mackenzie, Gekoski, & Knox, 2006).
From the HBM perspective, individuals are most likely to follow a particular health action if they believe themselves to be vulnerable to a particular condition (Conner, 2010). In line with this, several scholars argue that women use more health care services because of their higher burden of diseases and disability in later life (Rieker & Bird, 2005), and they are more proactive in medical seeking than men (Bertakis, Azari, Helms, Callahan, & Robbins, 2000; Dhingra, Zack, Strine, Pearson, & Balluz, 2010; Institute of Public Health, 2011; Krishnaswamy et al., 2009; Liu, 2014). Contrary to this argument, our study discovered that more poor older men consulted public health care providers than the females. And this is inconsistent with previous studies that show that women consult or visit public health care providers or centers more frequently than men (Carretero, Calderón-Larrañaga, Poblador-Plou, & Prados-Torres, 2014; Tenenbaum, Nordeman, Sunnerhagen, & Gunnarsson, 2017). In general, the study found that most poor older people consulted public health care providers than private health care providers due to their economic and financial conditions. More poor older females were found to consult private health care providers. This might arise from the situation where some older women have special health cases. Also, poor older people seek care at private health facility to avoid long waiting time at public health center or obtain special/recommended treatment. For public health care system in Ghana, it aims to ensure/improve equity in access to health care and provide health care for all Ghanaians at all ages. Most of the poor older people interviewed sought formal health care for 5 times or more in the last year prior to the survey. Yet, there should be health promotion and disease prevention education programs for older people so that those who do not utilize health services frequently would be encouraged to do so.
Our study found that drugs, out-patient, long-term care, in-patient, and health aide were the items poor older people interviewed spent their income on anytime they visit health care facility for treatment. Drugs constituted the major health care item the poor older people spent their income on. Because many poor older people suffered from NCDs such as hypertension and diabetes and, therefore, needed to take drugs daily, drugs purchase took greater proportion of their income, especially those drugs which were not covered under the NHIS (Agyemang-Duah et al., 2019b). The findings revealed that the respondents utilized health care services to prevent diseases and poor health, to improve their general health and for early detection of disease. Evidently, the study showed that majority of poor older people used various modalities of health care resources for prevention of disease and poor health. It is therefore not surprising that majority of the respondents described their health as poor since they are often afflicted with diseases and face greater health challenges. Herein, the HBM helps to explain how poor older people perceive their health status impacts utilization of health care and influence the kind of health care facility they should consult. However, poor older people who perceived their health as poor would be more likely to consult health care providers and follow certain health care utilization pattern.
Our study discovered that most poor older people sought health care for their health problems after detecting the symptoms in 3 days. This may suggest that poor older people have a good health care seeking behavior in terms of seeking early treatment to avoid further health complications. The study participants suffered from various NCDs including hypertension, diabetes, eye problem, stroke, bones and joint disorder, ear problem, asthma, arthritis, chronic kidney disease, depression, insomnia, cancer, and respiratory diseases. Hypertension and diabetes were therefore found to be the top two NCDs afflicting most poor older people in this study. This is consistent with previous research output that shows similar findings (Bao et al., 2015; Tyagi, 2014). It is also in agreement with the finding of WHO (2001b, 2003) that between 60% and 75% of older people suffer from hypertension. In Ethiopia, Amente and Kebede (2016) reported that hypertension (14%) and diabetes (5.2%) were among the predominant NCDs that older people suffer from. Poor eating habits, consumption of sugar beverages, and physical inactivity among older people are contributing factors of NCDs such as diabetes and hypertension (Nugent, 2008; Ofori-Asenso & Garcia, 2016). However, change of dietary behavior and lifestyle through regular exercise and intake of fruits and vegetables has potential to reduce the incidence of hypertension among poor older people. Hence, health promotion and disease prevention education and outreach programs by health institutions and stakeholders are required to enhance the health of the poor older people.
Interestingly, family members were found as the major source of health care information among the poor older people. This finding presents useful information for health policy makers and health institutions to educate older people on the negative implication of seeking health care from family members without consulting health professionals such as doctors. However, one key finding of the study was that most of the poor older people interviewed traveled 2 km or more to access health care for their various health problems and waited for 20 to 40 min at the health facility before seeing a doctor. Waiting for a long time at health facility before taken care of by health practitioners, particularly doctors may deter older people from utilizing health care regularly. This however calls for health institutions to strengthen their effort to solve long-waiting time at the health facilities in Ghana and other LMICs. As the poor older people often find it difficult to access health facilities due to inadequacy of funds, the study found that most poor older people used a commercial vehicle as a means of transport to access health care facility when it is deemed necessary. For policy implications, this study helps in informing pro-poor policies geared toward improving older people’s access to health care. It also provides information for reassessing poverty reduction programs that focus on poor older people by not only giving grants but also increasing poor older people’s enrollment in the NHIS.
The study therefore has both strengths and limitations. One of the strengths of the study is that it is one of the first studies to focus on utilization of health care services among poor older people in Ghana and other developing countries as many studies have largely concentrated on older people in general. Secondly, the use of LEAP as a poverty reduction program to identify poor older people helps in finding the patterns of health care services use for health care policy evaluation and social policy analysis. Furthermore, it helps to evaluate the effectiveness of poverty reduction programs and its role of reducing health poverty in Ghana. Since the study was cross-sectional, data collection design might have had impact on the results and limited our capacity to draw generalizations. Self-reported responses could expose our results to subjective biases which in a way could affect the correctness of the responses through faulty recall, overestimation, or underestimation. Efforts were made to deal with these limitations by minimizing the potential measurement errors in the assessment of outcome and cleaning up the data for consistency in the responses. The study did not examine the association between sociodemographic factors and self-rated heath status among poor older people so we recommend that future studies evaluate it. We also suggest that future research should use a larger sample size and replicate the study in different districts or regions of Ghana to inform health policy toward improving [poor] older people’s access to health care. Other LMICs that have similar social programs should investigate its role in health care utilization among beneficiaries.
Conclusion
The study found a higher prevalence of health care utilization among poor older people under LEAP program in the Atwima Nwabiagya District of Ghana. Yet, we found that the LEAP grant played a little role in reducing health poverty among the poor older people. Social capital through family relations, friendship, and social organizations was found to provide great support for the poor older people to finance their health care. The study found a statistically significant association between gender and health care use. Whereas more poor older females were found to consult private health care providers, most poor older males consulted public health care providers than the females. Hypertension and diabetes were the top two NCDs the respondents were afflicted with. Therefore, any social programs that seek to improve social well-being of the poor older people should take health poverty into account. We argue that the LEAP program alone cannot reduce health poverty of the poor older people and therefore, support in terms of funds from family members, friends, and social support networks should be strengthened to increase their access to health care.
Exchange rate as at June 2018 (GH¢ 4.77 = US$1.00)
Declaration of Conflicting Interests: The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The authors received no financial support for the research, authorship, and/or publication of this article.
ORCID iD: Williams Agyemang-Duah  https://orcid.org/0000-0001-8658-004X
https://orcid.org/0000-0001-8658-004X
References
- Aboderin A. G., Beard J. (2015). Older people’s health in sub-Saharan Africa. The Lancet, 385, e9-e11. [DOI] [PubMed] [Google Scholar]
- Adei D., Anning A., Mireku S. I. (2015). Basic needs for the aged in selected districts in Ashanti region of Ghana. Research on Humanities and Social Sciences, 5, 92-108. [Google Scholar]
- Agyemang C. G., Attah-Adjepong E., Owusu-Dabo A., De-Graft Aikins J., Addo A. K., Edusei B. C., . . . Ogedegbe G. (2012). Stroke in Ashanti region of Ghana. Ghana Medical Journal, 46(2), 12-17. [PMC free article] [PubMed] [Google Scholar]
- Agyemang-Duah W., Peprah C., Peprah P. (2019. a). Factors influencing the use of public and private health care facilities among poor older people in rural Ghana. Journal of Public Health. Advance online publication. doi: 10.1007/s10389-018-01010-y [DOI] [Google Scholar]
- Agyemang-Duah W., Peprah C., Peprah P. (2019. b). “Let’s talk about money”: How do poor older people finance their healthcare in rural Ghana? A qualitative study. International Journal for Equity in Health, 18(1), 1-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Agyepong I. A., Adjei S. (2008). Public social policy development and implementation: A case study of the Ghana National Health Insurance scheme. Health Policy and Planning, 23, 150-160. doi: 10.1093/heapol/czn002 [DOI] [PubMed] [Google Scholar]
- Amente T., Kebede B. (2016). Determinants of health service utilization among older adults in Bedele Town, illubabor zone, Ethiopia. Journal of Diabetes & Metabolism, 7(11), 713. [Google Scholar]
- Anning A. (2012). The emerging problems of the aged in Ghana: Issues of housing and basic care a case study of some selected districts in Ashanti region (Master’s thesis, School of Graduate Studies, Kwame Nkrumah University of Science and Technology, Kumasi, Ghana). Retrieved from http://ir.knust.edu.gh/bitstream/123456789/7603/1/ALEX%2BANNING.pdf
- Ansah E. K., Narh-Bana S., Asiamah S., Dzordzordzi V., Biantey K., Dickson K., . . . Whitty C. J. (2009). Effect of removing direct payment for health care on utilisation and health outcomes in Ghanaian children: A randomised controlled trial. PLoS Medicine, 6(1), e1000007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Awoke A. M., Negin J., Moller J., Farell P., Yawson E. A., Biritwum B., Kowal P. (2017). Predictors of public and private healthcare utilization and associated health system responsiveness among older adults in Ghana. Global Health Action, 10(1), 1301723. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Balcombe R. N. (2001). Ageing: Definitions, mechanisms and the magnitude of the problem. Best Practice & Research: Clinical Gastroenterology, 15, 836-849. [DOI] [PubMed] [Google Scholar]
- Bao C., Mayila M., Ye Z., Wang J., Jin M., He W., Chen K. (2015). Forecasting and analyzing the disease burden of aged population in China, based on the 2010 global burden of disease study. International Journal of Environmental Research and Public Health, 12, 7172-7184. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bernstein A. B., Hing E., Moss A. J., Allen K. F., Siller A. B., Tiggle R. B. (2003). Health care in America: Trends in utilization. Hyattsville, MD: National Center for Health Statistics; Retrieved from https://www.cdc.gov/nchs/data/misc/healthcare.pdf [Google Scholar]
- Bertakis K. D., Azari R., Helms L. J., Callahan E. J., Robbins J. A. (2000). Gender differences in the utilization of health care services. The Journal of Family Practice, 49, 147-152. [PubMed] [Google Scholar]
- Bourne P. A., Morris C., Charles C. A. D., Eldemire-Shearer D., Kerr-Campbell M. D., Crawford T. V. (2010). Health literacy and health seeking behavior among older men in a middle-income nation. Patient Related Outcome Measures, 1, 39-49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brinda E. M., Attermann J., Gerdtham U. G., Enemark U. (2016). Socio-economic inequalities in health and health service use among older adults in India: Results from the WHO Study on global ageing and adult health survey. Public Health, 141, 32-41. [DOI] [PubMed] [Google Scholar]
- Carretero M. T., Calderón-Larrañaga A., Poblador-Plou B., Prados-Torres A. (2014). Primary health care use from the perspective of gender and morbidity burden. BMC Women’s Health, 14(1), Article 145. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Conner M. (2010). Chapter 2: Cognitive determinants of health behavior. In Handbook of behavioral medicine (pp. 19-30). doi: 10.1007/978-0-387-09488-5_2 [DOI] [Google Scholar]
- Dhingra S. S., Zack M., Strine T., Pearson W. S., Balluz L. (2010). Determining prevalence and correlates of psychiatric treatment with Andersen’s behavioral model of health services use. Psychiatric Services, 61, 524-528. [DOI] [PubMed] [Google Scholar]
- Dogbey L. S. (2015). Health-related lifestyles and health conditions among the elderly in Ghana (Master’s thesis). University of Ghana, Accra. [Google Scholar]
- Elfil M., Negida A. (2017). Sampling methods in clinical research; an educational review. Emergency, 5(1), e52. [PMC free article] [PubMed] [Google Scholar]
- Exavery A. (2010). Determinants of health care utilisation among the elderly population in rural Ghana (Master’s thesis, University of the Witwatersrand, Johannesburg, South Africa). Retrieved from http://wiredspace.wits.ac.za/bitstream/handle/10539/9106/ResearchReport382128.pdf?sequence=1
- Galdas P. M., Cheater F., Marshall P. (2005). Men and health help-seeking behaviour: Literature review. Journal of Advanced Nursing, 49, 616-623. [DOI] [PubMed] [Google Scholar]
- Gerritsen A. A., Devillé W. L. (2009). Gender differences in health and health care utilisation in various ethnic groups in the Netherlands: A cross-sectional study. BMC Public Health, 9(1), Article 109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ghana Statistical Service. (2013). The elderly in Ghana 2010 population & housing census report. Accra, Ghana: Author; Retrieved from http://www.statsghana.gov.gh/gssmain/fileUpload/pressrelease/2010_PHC_National_Analytical_Report.pdf [Google Scholar]
- Gómez-Olivé F. X., Thorogood M., Clark B., Kahn K., Tollman S. (2013). Self-reported health and health care use in an ageing population in the Agincourt sub-district of rural South Africa. Global Health Action, 6, 19305. doi: 10.3402/gha.v6i0.19305 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Guo C., Du W., Hu C., Zheng X. (2016). Prevalence and factors associated with healthcare service use among Chinese elderly with disabilities. Journal of Public Health, 38, e345-e351. [DOI] [PubMed] [Google Scholar]
- Gyasi R. M., Phillips D. R., Buor D. (2018). The role of a health protection scheme in health services utilisation among community-dwelling older persons in Ghana. The Journals of Gerontology, Series B: Psychological Sciences & Social Sciences. Series B, XX (XX), 1-13. doi: 10.1093/geronb/gby082 [DOI] [PubMed] [Google Scholar]
- Gyasi R. M., Phillips R. D. (2018). Gender, self-rated health and functional decline among community-dwelling older adults. Archives of Gerontology and Geriatrics, 77, 174-183. [DOI] [PubMed] [Google Scholar]
- Hajek A., Bock J.-O., König H.-H. (2017). Which factors affect health care use among older Germans? Results of the German ageing survey. BMC Health Services Research, 17, Article 30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Handa S., Park M. J., Darko R. O., Osei-Akoto I., Davis B., Daidone S. (2013). Livelihood empowerment against poverty program impact evaluation report. Chapel Hill: Carolina Population Center, The University of North Carolina at Chapel Hill. [Google Scholar]
- Hanvoravongchai P., Hsiao W. C. (2007). Thailand: Achieving universal coverage with social health insurance. In Hsiao W. C., Shaw P. (Eds.), Social health insurance for developing nations (pp. 133-154). Washington, DC: World Bank. [Google Scholar]
- Henshaw E. J., Freedman-Doan C. R. (2009). Conceptualizing mental health care utilization using the health belief model. Clinical Psychology: Science and Practice, 16, 420-439. [Google Scholar]
- Hsu W.-C., Hsu Y.-P. (2016). Patterns of outpatient care utilization by seniors under the National Health Insurance in Taiwan. Journal of the Formosan Medical Association, 115, 325-334. [DOI] [PubMed] [Google Scholar]
- Institute of Public Health. (2011). National Health and Morbidity Survey 2011 (NHMS 2011): Healthcare demand and out-of-pocket health expenditure (Vol. III). Retrieved from http://iku.moh.gov.my/images/IKU/Document/REPORT/NHMS2011-VolumeIII.pdf [Google Scholar]
- Kim H.-K., Lee M. (2016). Factors associated with health services utilization between the years 2010 and 2012 in Korea: Using Andersen’s behavioral model. Osong Public Health and Research Perspectives, 7, 18-25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Krishnaswamy S., Subramaniam K., Low W. Y., Aziz J. A., Indran T., Ramachandran P., . . . Patel V. (2009). Factors contributing to utilization of health care services in Malaysia: A population-based study. Asia Pacific Journal of Public Health, 21, 442-450. [DOI] [PubMed] [Google Scholar]
- Kwankye S. O. (2013). Growing old in Ghana: Health and economic implications. Postgraduate Medical Journal of Ghana, 2, 88-97. [Google Scholar]
- Leavitt F. (1979). The health belief model and utilization of ambulatory care services. Social Science & Medicine. Part A: Medical Psychology & Medical Sociology, 13, 105-112. [DOI] [PubMed] [Google Scholar]
- Liu L. F. (2014). The health heterogeneity of and health care utilization by the elderly in Taiwan. International Journal of Environmental Research and Public Health, 11, 1384-1397. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mackenzie C. S., Gekoski W. L., Knox V. J. (2006). Age, gender, and the underutilization of mental health services: The influence of help-seeking attitudes. Aging & Mental Health, 10, 574-582. [DOI] [PubMed] [Google Scholar]
- Mba J. C. (2010). Population ageing in Ghana: Research gaps and the way forward. Journal of Aging Research, 2010, 672157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller R. L., Brewer J. D. (2003). A-Z of social research. London, England: SAGE. [Google Scholar]
- Ministry of Gender, Children and Social Protection. (2016). The state of the livelihood empowerment against poverty programme. Accra: Government of Ghana. [Google Scholar]
- Ministry of Manpower, Youth and Employment. (2007). The National Social Protection Strategy (NSPS): Investing in people. Accra: Government of Ghana. [Google Scholar]
- Nugent R. (2008). Chronic diseases in developing countries: Health and economic burdens. Annals of the New York Academy of Sciences, 1136, 70-79. doi: 10.1196/annals.1425.027 [DOI] [PubMed] [Google Scholar]
- Nyamezea Y. (2017). Older adults Ghanaians and health care access. Innovation in Aging, 1(1), 1232. [Google Scholar]
- Ofori-Asenso R., Garcia D. (2016). Cardiovascular diseases in Ghana within the context of globalization. Cardiovascular Diagnosis and Therapy, 6, 67-77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Olukoya P. (2014). Ghana country assessment report on ageing and health. Geneva, Switzerland: World Health Organization; Retrieved from http://apps.who.int/iris/bitstream/10665/126341/1/9789241507332_eng.pdf [Google Scholar]
- Oyetunde M. O., Ojo O. O., Ojewale L. Y. (2013). Nurses’ attitude towards the care of the elderly: Implications for gerontological nursing training. Journal of Nursing Education and Practice, 3(7), 1-9. [Google Scholar]
- Peprah P., Kyiyaga E. M., Afful H., Abalo E. M., Agyemang-Duah W. (2017). Does the Ghanaian livelihood empowerment against poverty programme lead to an increase in household productive livelihood assets? Analysing the Ashanti scenario. Cogent Social Sciences, 3(1),1298174. [Google Scholar]
- Rieker P. P., Bird C. E. (2005). Rethinking gender differences in health: Why we need to integrate social and biological perspectives. The Journals of Gerontology, Series B: Psychological Sciences & Social Sciences, 60, 40-47. [DOI] [PubMed] [Google Scholar]
- Robinson K. (2007). Trends in health status and health care use among older women. Retrieved from https://www.cdc.gov/nchs/data/ahcd/agingtrends/07olderwomen.pdf [PubMed]
- Rosenstock I. M. (1974). Historical origins of the health belief model. Health Education Monographs Winter, 2, 328-335. [Google Scholar]
- Rosenstock I. M. (1988). Enhancing patient compliance with health recommendations. Journal of Pediatric Health Care, 2, 67-72. [DOI] [PubMed] [Google Scholar]
- Saeed B. I. I., Xicang Z., Yawson A. E., Nguah S. B., Nsowah-Nuamha N. N. (2015). Impact of socioeconomic status and medical conditions on health and healthcare utilization among aging Ghanaians. BMC Public Health, 15, Article 276. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Saeed B. I. I., Yawson A. E., Nguah S., Agyei-Baffour P., Emmanuel N., Ayesu E. (2016). Effect of socio-economic factors in utilization of different healthcare services among older adult men and women in Ghana. BMC Health Services Research, 16, Article 390. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schneider P., Hanson K. (2006). Horizontal equity in utilisation of care and fairness of health financing: A comparison of micro-health insurance and user fees in Rwanda. Health Economics, 15, 19-31. [DOI] [PubMed] [Google Scholar]
- Suominen-Taipale A. L., Martelin T., Koskinen S., Holmen J., Johnsen R. (2006). Gender differences in health care use among the elderly population in areas of Norway and Finland. A cross-sectional analysis based on the HUNT study and the FINRISK Senior Survey. BMC Health Services Research, 6(1), Article 110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tenenbaum A., Nordeman L., Sunnerhagen K. S., Gunnarsson R. (2017). Gender differences in care-seeking behavior and healthcare consumption immediately after whiplash trauma. PLoS ONE, 12(4), e0176328. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tyagi P. (2014). Double burden of disease: Double burden of communicable and non-communicable diseases in old age in South Asia. Retrieved from https://www.helpage.org/silo/files/double-burden-of-disease-report.pdf
- United Nations. (2015). World population ageing 2015 (ST/ESA/SER.A/390). Department of Economic and Social Affairs, Population Division; Retrieved from http://www.un.org/en/development/desa/population/publications/pdf/ageing/WPA2015_Report.pdf [Google Scholar]
- United Nations. (2017). World population ageing 2017—Highlights (ST/ESA/SER.A/397). Department of Economic and Social Affairs, Population Division. [Google Scholar]
- Van Der Wielen N., Channon A. A., Falkingham J. (2018). Does insurance enrolment increase healthcare utilisation among rural-dwelling older adults? Evidence from the national health insurance scheme in Ghana. BMJ Global Health, 3(e000590), 1-9. doi:10.1136/bmjgh-2017-000590 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Viña J., Borrás C., Miquel J. (2007). Theories of ageing: Critical review. IUBMB Life, 59, 249-254. [DOI] [PubMed] [Google Scholar]
- Weiskopf D., Weinberger B., Grubeck-Loebenstein B. (2009). The aging of the immune system. European Society for Organ Transplantation, 22, 1041-1050. [DOI] [PubMed] [Google Scholar]
- World Health Organization. (2001. a). Health research methodology: A guide for training in research methods (2nd ed.). Retrieved from https://apps.who.int/iris/handle/10665/206929
- World Health Organization. (2001. b). Men, ageing and health: Achieving health across the life span. Retrieved from https://www.who.int/ageing/publications/men/en/
- World Health Organization. (2003). Ageing and health: A health promotion approach for developing countries. Manila, Philippines: Regional Office for the Western Pacific, World Health Organization. [Google Scholar]
- World Health Organization. (2014). Ghana country assessment report on ageing and health. Geneva, Switzerland. Retrieved from http://apps.who.int/iris/bitstream/10665/126341/1/9789241507332_eng.pdf
- World Health Organization. (2015. a). WHO country office for Ghana annual report 2014. Retrieved from https://www.afro.who.int/sites/default/files/2017-05/ghana-annual-report-2014-final.pdf
- World Health Organization. (2015. b). World report on ageing and health. Geneva, Switzerland. Retrieved from http://apps.who.int/iris/bitstream/10665/186463/1/9789240694811_eng.pdf
- World Medical Association. (2001). World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. Bulletin of the World Health Organization, 79, 373-374. [PMC free article] [PubMed] [Google Scholar]
- Zotorvie O. H. (2015). Assessing health care utilisation among the elderly with chronic conditions in Ghana (Master’s thesis). University of Ghana, Accra. [Google Scholar]