

Abstract
Background
The current study investigated the impact of an intervention that included aided augmentative and alternative communication (AAC) technologies on the frequency of symbolic communication turns of school-age children, adolescents, and young adults with severe disability.
Method
Nine students ages 8–20 were engaged in interactive activities using an aided AAC system with visual scene displays (VSDs; concepts embedded within a photograph of a naturally occurring event), and “just-in-time” (JIT) programming (the capability to add new contexts “on the fly”). Effectiveness was evaluated using a single subject multiple probe across participants design.
Results
All participants demonstrated increases in symbolic communication turns upon introduction of the AAC technologies with VSDs using JIT technology.
Conclusions
AAC with VSDs and JIT programming may be effective in increasing symbolic communication for students with severe developmental disability. The fast and easy creation of VSDs and hotspots to provide communication may be a valuable tool for interventionists.
Keywords: augmentative and alternative communication, school-age, adolescents, severe disability, technology
Augmentative and alternative communication (AAC) offers the potential means for increasing social interaction and developing receptive and expressive communications skills by providing a means to increase opportunities for communication (Johnston, Reichle, & Evans, 2004). It can provide a means to meet daily communication needs, interact with others, demonstrate control over one’s environment, and express a wide range of concepts.
Youth and adolescence into young adulthood is a continuing time of development that may bring many changes in both scope and complexity for individuals that require AAC (Smith, 2014). However, although an individual with developmental disability may be chronologically older than the infant and toddler stage, he/she may function at the stage of beginning communication well beyond the language learning years of typically developing children. Although there are several ways to define and describe individuals who are at these early stages of communication, Romski, Sevcik, Hyatt, and Cheslock (2002) describe beginning communicators as individuals who have a vocabulary fewer than 50 words. Beginning communicators may be of any chronological age, and vary in their level and type of disability (Romski et al., 2002).
Caregivers may sometimes assume that because the beginning communicator has a limited expressive vocabulary, he/she is functioning at a very young developmental level, with limited capabilities. This assumption will affect the range and type of interventions chosen, as well as the materials used. It is often difficult to ensure that interventions are both age- and developmentally-appropriate (Calculator, 1988), with methods and materials related to not only the person’s abilities and communication experiences but also his/her age. This can be particularly difficult once the beginning communicator reaches school age and/or adolescence.
AAC System Design
Many AAC technologies impose significant learning demands on beginning communicators, at any age (Light & Drager, 2002). Many AAC technologies, whether realized on a dedicated device or a mobile device such as a tablet or smart phone, use grid-based display systems where language concepts are presented individually, in rows and columns. These systems may impose some meta-linguistic demands on beginning communicators, as the words and concepts are placed out of context (Light et al., 2004). In contrast, visual scene displays (VSDs) have been discussed as an alternative display for beginning communicators and individuals with cognitive and linguistic limitations (Blackstone, Light, Beukelman, & Shane, 2004). VSDs present language concepts embedded within a photograph or image of a naturally occurring event (Wilkinson & Light, 2011), providing increased contextual support and facilitating early language learning. For example, a photograph of a student and teacher engaging in a high-five routine while playing a game could be used as a VSD, with hotspots within the scene (See Figure 1 for an example). Touching the location on the VSD of the student’s face might result in speech output with his name, while touching the location around the hands might result in speech output such as “high five!” or “way to go!”. In this way, the language for the activity is presented within a meaningful context, providing support for understanding and learning, while providing a motivating and interesting context. VSDs also preserve the relationships between concepts as they occur in real life.
Figure 1.

Example of a VSD for a high-five routine during game play (Note: picture is in color on the system)
Much of the research on the use of VSDs with beginning communicators has focused on infants, toddlers, and preschoolers, both typically developing children (Drager, Light, Curran Speltz, Fallon, & Jeffries, 2003; Drager, et al., 2004; Light, et al., 2004; Olin, Reichle, Johnson, & Monn, 2010) and children with developmental disability (Light & Drager, 2009). Light and Drager (2009) have described a successful evidence-based AAC intervention including VSDs for young children with developmental disability. Their intervention departed from traditional AAC interventions in that it focused on sustained social interaction, rather than just wants and needs, and encouraged language learning and interaction through the medium of the aided AAC system itself. This intervention approach may be effective with school-age children and adolescents who are chronologically older but with similar levels of beginning communication skills, provided that the materials and activities are meaningful, motivating, and age appropriate.
Despite the potential for the use of VSDs with beginning communicators of a variety of ages, an additional problem exists with current technology: it is time consuming to program new VSD and new vocabulary. In addition, partners cannot dynamically capture new experiences and add them to the AAC technologies during interactions. As a result, caregivers and professionals are required to spend significant time programming pages and vocabulary “offline”. This is a problem for several reasons. First, the time commitment involved may result in new programming not taking place, leaving students without access to critical vocabulary required for full participation. Second, it is difficult, often impossible, to respond to the interests of the student in the moment and provide critical vocabulary. Parental responsivity, including responding contingently to a child’s cues and following a child’s lead (Spiker, Boyce, & Boyce, 2002), has been shown to play an important role in child development (see Warren & Brady, 2007 for a review). When caregivers have limited means to be responsive, children and adolescents are placed at a disadvantage and relegated to being a passive participant. Third, an inability to capture the interest of the beginning communicator dynamically in the moment means that caregivers are always trying to “catch up” with these interests, which may change by the time the programming can be completed.
One potential solution to these challenges is the use of “just-in-time” (JIT) technology. Technology that allows for fast and easy import of photos as VSDs and easy programming of vocabulary as hotspots within the VSDs would allow partners to respond to the beginning communicator’s interests by adding new communicative contexts and vocabulary “on the fly” dynamically. JIT technology that takes advantage of teachable moments can support dynamic learning and language growth (Schlosser et al., 2015).
A pilot study by Light, et al. (2012) investigated the use of an app with JIT programming relative to a traditional AAC app that did not offer JIT programming. Evaluated using a single subject alternating treatment design, three preschool participants (3–5 years old) who had developmental disability took more communicative turns with the app with JIT programming than the one without. These are promising preliminary results, however it is necessary to further investigate the potential of JIT technologies, and to extend the findings to a wider population of beginning communicators.
The current study sought to answer the following research questions: 1) What is the impact of AAC technologies that support VSD and JIT programming on the frequency of symbolic communication turns produced by school age, adolescent, and young adult students with severe developmental disability during shared context activities? 2) What is the impact of AAC technologies that support VSD and JIT programming on the communication modes used by school age, adolescent, and young adult students with developmental disability during shared context activities?
Method
Experimental design
Three single subject multiple probe designs across participants were used to evaluate the effects of the intervention. Each multiple probe design consisted of three participants, who each participated in two conditions: baseline and intervention. Baseline continued until a stable and consistent pattern with no upward trend was apparent (a minimum of 5 sessions), followed by intervention for a minimum of 5 sessions. Once at least 3 sessions showed a non-decreasing trend with a relative level change from baseline, the next participant in each multiple probe design began the intervention phase.
Participants
Participants were recruited through local school districts, after obtaining permission from school personnel. Letters and emails of introduction were sent to special education teachers and speech-language pathologists to help to identify potential participants. Information was then sent home with potential participants. Consent forms were returned to the research team. The first nine students who met inclusionary criteria participated in the study.
The participants met the following criteria for inclusion, based on parent or teacher report: 1) were between the ages of 8–21 years (i.e., beyond the early primary school years), 2) were in school, 3) demonstrated a significant communication impairment that restricted participation in education, social interaction, or communication activities, 4) used fewer than 50 words functionally through any means (Romski, et al., 2002), 5) reported by parent or teacher to recognize photographs of familiar people, objects, or events, 6) were able to use hands to directly select on a computer screen, and 7) had signed consent from a parent or guardian. For descriptive purposes, each participant was given the Communication Matrix, an assessment tool designed to document the expressive communication skills of children who have severe or multiple disability (Rowland, 2004). The participants ranged in age from 8–20 years (M = 14 years), and had a range of diagnoses. Information about each participant is shown in Table 1 (all names have been changed).
Table 1.
Participant Characteristics
| Participant | Age | Diagnosis | Vision/Hearing | Motor skills | Means of Communication; Communication Matrix# (Rowland, 2004) | School information |
|---|---|---|---|---|---|---|
| Kenneth | 20 | Autism Spectrum Disorder | No identified issues | Independently ambulatory; able to point and isolate finger to direct select | GoTalk 9+ (Mayer Johnson) programmed with 45 picture symbols, primarily snack items, natural gestures, sign approximation for MORE Communication Matrix level IV |
Grade 12; LifeSkills classroom |
| Owen | 16 | Autism Spectrum Disorder | Glasses to correct vision | Independently ambulatory; able to point and isolate finger to direct select | Pointing to white board with “yes” and “no”, natural gestures, vocalizations Communication Matrix level III |
Grade 11; LifeSkills classroom; included during lunch |
| Carl | 17 | Intellectual Disability / Seizure Disorder | No identified issues | Uses a wheelchair, independently navigates; able to point and isolate finger to direct select | Communication book with approx. 40 picture communication symbols used to select leisure activities and snack items, making choices among a field of 3 items Communication Matrix level III |
Grade 12; LifeSkills classroom |
| Amina | 11 | Cerebral Palsy / Seizure Disorder | Glasses to correct vision | Uses a wheelchair, no independent navigation; able to isolate 2 fingers or use whole hand to direct select | Real objects to make a choice between two toys, waves to greet Communication Matrix level III |
Grade 6; LifeSkills classroom; included during homeroom, lunch, art, music |
| Ivan | 16 | Lennox-Gastaut Syndrome / Seizure Disorder | No identified issues | Independently ambulatory; able to point and isolate finger to direct select | Sign approximations, Vocalizations Communication Matrix level III |
Grade 11; LifeSkills classroom; included during lunch |
| Nadia | 13 | Cerebral Palsy / Developmental Delay | No identified issues | Walks with assistance/walker; able to point and isolate finger to direct select | Sign approximations (MORE), digital photographs to choose activities, expresses dislikes by pinching Communication Matrix level III |
Grade 6; LifeSkills classroom |
| Tomieka | 17 | Fetal Alcohol Syndrome (Left hemiplegia, Developmental Delay, Seizure Disorder) | Wears glasses to correct vision | Uses a wheelchair or walk with a walker; able to point and isolate finger to direct select | Digital photographs to choose activities, often indicates choices between activities through eye gaze, shakes head Communication Matrix level III |
Grade 12; LifeSkills classroom |
| Lucille | 8 | Cerebral Vascular Accident at age 3 | No identified issues | Uses a wheelchair or walk with a walker; able to point and isolate finger to direct select | Sign approximations (e.g., PLEASE), vocalizations for “hi” and “bye”, Communication Matrix level IV |
Grade 3; LifeSkills classroom; included at story time, recess, lunch, art, PE, and music |
| Henry | 8 | Autism Spectrum Disorders | No identified issues | Independently ambulatory; able to point and isolate finger to direct select | Sign approximations (MORE, CANDY), approximately 10 picture sign cards to select activities Communication Matrix level III |
Grade 4; specialized school setting |
Communication Matrix Level III: Primarily uses unconventional communication using pre-symbolic behaviors (e.g., body movements, actions on people and objects, vocalizations)
Communication Matrix Level IV: Primarily uses conventional communication using pre-symbolic behaviors (e.g., conventional gestures and vocalizations)
Materials
An Asus Eee Slate EP 121 tablet computer, operated on Window 7, was used to present the AAC software. The tablet computer had a 12.1 capacitive touch screen with a resolution of 1280 × 800. A Samsung Galaxy MP3 player with Bluetooth connectivity, operated on the Android 2.3.6 Gingerbread mobile operating system, with a 5” thin film transistor (TFT) liquid crystal display (LCD) screen and 800 × 480 resolution was used as a music player and as a 3.2 megapixel camera.
Activities were selected including songs, constructed “books”, and game activities (e.g., bean bag toss, table bowling, playing musical instruments, iPad apps). Songs were selected based on participants’ interests, gender, and age group, and included songs from a variety of genres (e.g., popular songs, such as “Starship”, movie songs, such as “I Like to Move It”, or classic songs, such as “Celebration”). Short portions (verses or snippets) of the songs were played at a time. Each song snippet was paired with a sign or gesture that was used consistently and only with that song section (e.g., clapping, signing LOVE). Constructed books were created displaying images from the internet on a variety of topics (e.g., sports, animals, funny pictures, baby faces), along with simple text (e.g., “A cat naps in the box.”, “She has a big red hat.”). The images were printed on white 8” by 11” paper and placed into no gloss plastic cover sheets. These “books” were developed prior to the beginning of data collection and were available during all sessions (baseline and intervention). They were used in place of books that were available in each classroom, which were often children’s books that were not age appropriate.
An AAC application with JIT programming was used throughout this study (under development by InVoTek; www.invotek.org.). The app allowed for the creation of VSDs and hotspots using JIT technology. Capabilities of the application included importing pictures as VSDs via Bluetooth, creating, saving, and deleting hotspots, and recording voice output for a hotspot. The steps for completing the JIT programming were as follows:
Take a photo to serve as a VSD. For the purposes of the present study, the MP3 player was used as a camera. Photos were taken of the participant, interventionist, and/or teacher/aid engaged in each activity, song images, or pages of each “book”. Photographs could also be taken with a cell phone or a digital camera.
Import the photo to the app Photo images were transferred from the MP3 player to the tablet computer using Bluetooth connectivity. Once transferred to the app, each image was automatically displayed on the screen. Two menus on the left of the display contained small VSDs that represented activities (songs, books, games), as well as small VSDs within each activity (song verses, book pages, game components). The interventionist could choose where to place the imported image. See Figure 2 for an example of a first page of a song and a later “verse” within the song. The menus on the left are marked in a red circle (not present on the actual app) to indicate where each VSD could be selected.
Add hotspot(s). Once the VSD was imported, the interventionist would select a function key (labeled B1 in Figure 2) by double tapping with a finger or stylus, and then select an area on the VSD to contain the hotspot.
Record speech output. Selecting another function button allowed for speech output to be recorded. For the songs, the MP3 player was used to store, select, and play the songs, via a small Bluetooth speaker. Speech output for books and activities was recorded via voice.
Figure 2.

Examples of the JIT app. The top panel shows an example of the first “verse” of a song. The circle (not visible in the app) marks the location on the top menu for choosing this activity. The bottom panel shows an example of the second menu for choosing a component of an activity, again with a red circle marking the location (in this case, a later verse of the song, demonstrating the sign or action corresponding to the verse) (Note: pictures are in color on the system)
Each session was videotaped using the Sony Handycam HDR-CX130. The digital recordings were uploaded via iMovie 11 on an Apple Mac Pro running Mac OS X Lion 10.7.4 software.
Procedures
The participants completed a minimum of five baseline sessions and five intervention sessions. Before baseline, a non-standard preference assessment, involving interviewing teachers and/or caregivers, was completed to determine the types of songs, books, and games most likely to be motivating for each participant. A minimum of 10 activities (songs, books, and games) were pre-identified and available during all baseline and intervention sessions. Activities were chosen that were motivating based on participant reaction, provided multiple opportunities for communication, and were both age and developmentally appropriate.
Sessions took place 1–2 times per week, for 15 min. All sessions took place in the participants’ classroom or a nearby room (e.g., school library room) with a teacher or aide present. During both baseline and intervention, one of the authors served as the interventionist and implemented the following steps: 1) provide a communication opportunity (asking a question, making a comment, or providing a choice directed toward the participant), 2) respond to any communicative attempt (fulfill intent, expand on communication with speech and unaided or aided AAC, and 3) provide the next opportunity. Any communicative attempt at any point (i.e., a communicative behavior directed toward the partner) was followed by a response that fulfilled the intent (e.g., playing the next song verse or the next step in an activity). Figure 3 presents a flow chart of the procedures. A minimum of 10 opportunities were provided during each session.
Figure 3.

Flow chart of procedures including prompting hierarchy
No JIT programming took place during the baseline sessions. Participants used any currently available means to communicate (speech, vocalizations, signs, gestures, or current AAC systems). Baseline sessions involved engaging the participant in at least two activities per session, and following the procedures described above. One activity would be introduced, and the interventionist would 1) provide a communication opportunity, 2) respond to any communicative attempt, and 3) provide the next opportunity. The activity and the interventionist were positioned within view of the participant. A least-to-most prompting hierarchy was used after a communication opportunity was provided, consisting of a) an expectant delay of 5 sec, b) a gestural prompt toward the activity, and c) a model prompt using speech.. When the activity either reached a natural end (e.g., the end of a song) or the participant indicated an interest in a different activity (e.g., reaching for different materials), a second activity was introduced, and the same procedures were followed. There was no limit on the number of activities that occurred within a session, which typically ranged from 2–4 activities.
The independent variable was the use of the tablet with the AAC app utilizing JIT programming, and thus, the intervention sessions were identical to the baseline sessions except for the introduction of the technology. Any currently available means to communicate (speech, vocalizations, signs, gestures, or current AAC systems) remained available. As in baseline, each intervention session also involved at least two activities. As before, one activity would be introduced, and the interventionist would continue to 1) provide a communication opportunity, 2) respond to any communicative attempt, and 3) provide the next opportunity. The procedures, and the least-to-most prompting hierarchy, were identical to baseline, with the exception of incorporation of the tablet technology with VSDs (i.e., in addition to the activity and the interventionist, the tablet was positioned within view of the participant, the gestural prompt included a gesture toward the VSD, and the model prompt included using speech and simultaneously selecting a hotspot on the VSD). Intervention also involved the creation of JIT VSDs. For example, the interventionist might say, “You’re reaching for the bowling materials. Let’s take a picture of you bowling.” Once created, the VSDs often served as the opportunity for communication (step 1).
VSDs were created by taking photographs of the participants and/or activities using the MP3 player, and transferring these photographs to the tablet via Bluetooth, a process that took 5–15 sec. Either the interventionist or the classroom teacher took the photos, depending on the content. Once loaded, hotspots were drawn using a finger or stylus, and speech output was recorded. These VSDs and hotspots were then available for immediate use for communication purposes, and for all sessions after.
All VSDs were created during the sessions using the JIT technology; none were preprogrammed. A minimum of 3 JIT elements were programmed during each session (a JIT element was defined as a new VSD or a new hotspot). VSDs were photographs imported via the JIT technology. VSDs of activities (e.g., playing bean bag toss, high five routine) were photographs of the student and/or the interventionist engaged in the activity. With the songs, VSDs were photographs of the interventionist performing the action for each song snippet. VSDs for the constructed books were photographs of the book pages.
Data collection, measures, and analysis
Each session was videotaped. After each session was completed, the video session was loaded onto the Mac Pro computer. If the session exceeded 15 min, a randomly-selected 15 min section of interaction during baseline and intervention was identified. These sections were analyzed by a trained coder, who marked the occurrence of the dependent variable.
The first dependent variable was the number of intentional and intelligible symbolic communicative turns expressed by the participant. A communicative turn was an observed behavior that was intentional, communicative, and bore a symbolic message. An intentional communicative turn was defined as a behavior generated for or with a partner that communicated an identifiable message, or concept beyond a state of being (Carter, 2003). A communicative turn was considered symbolic when the participant’s turn carried associated meaning to stand for something else in a clear consistent manner (e.g., standardized gesture or sign, picture symbol, VSD hotspot, or speech). Communicative turns were coded if they occurred during any point in all sessions (baseline or intervention), whether prompted or unprompted.
The data on the frequency of the students’ turns were graphed separately for each participant, and level, trend, and slope of the data in the intervention phases were visually compared to the data in the baseline phases. Percent nonoverlapping data (PND) was also calculated (Scruggs, Mastropieri, & Casto, 1987) by determining the percent of data points in intervention that exceeded the highest baseline point for each participant.
The second dependent variable was the communication modes for each turn. Turns were counted as one of the following: a) speech or speech approximations, b) signs, idiosyncratic signs/gestures, or sign approximations, or c) speech generating device (use of the tablet or a participant’s existing AAC device). The frequency of communication modes for each session were graphed separately for each participant.
Reliability
Procedural reliability was assessed for number of opportunities presented to the participant in each session and the use of the prompting hierarchy. The video recordings for a random two out of every three sessions were checked by a second coder to ensure that a minimum of 10 opportunities were presented to the participant in each session. Sixty-seven of the 98 sessions were checked, and in each case greater than 10 opportunities were provided. A second coder also watched 5 min of each video recorded session (i.e., 30% of each session) and recorded whether each step in the prompting hierarchy was followed (expectant delay, wait 5 sec, gestural prompt, wait 5 sec, model prompt, fulfill intent). Procedural reliability for the prompting hierarchy was 99% (range 84–100%) using the formula (# completed) / (# completed + # missed) x 100. All of the intervention sessions were checked to determine that at least three JIT elements (VSDs or hotspots) were added each session. The number of vocabulary available (only hotspots) was calculated at the end of each session, by counting the number of hotspots added in each session, and calculating a cumulative total over the course of the study for each participant. Each hotspot was counted as one “vocabulary” item, whether it was recorded as a single word or an entire song verse.
A second coder independently recorded the calculation of turns in 5 min (30%) of each session. Interobserver agreement was calculated on a point-by-point basis using the formula (# agreements) / (# agreements + # disagreements) x 100. Agreements were scored when the first coder and the second coder recorded the same response. Interobserver agreement was 97% (range 80–100%).
Results
Impact of VSD and JIT Technology on Frequency of Turns
Figures 4–6 present the data on the number of communicative turns each participant took during 15 min sessions during baseline and intervention in the three multiple probe designs. Each of the participants demonstrated an increase in communication turns upon introduction of the AAC technologies with VSDs and JIT programming. This increase in turns only occurred once the intervention phase was initiated for each participant. During baseline, the nine participants took an average of 4 turns per 15 min session (range 0–33). During intervention, with the introduction of the AAC app, participants took an average of 30 turns per 15 min session (range 12–78). The percent of nonoverlapping data was 100% in all cases, indicating that the number of communication turns for all participants surpassed the maximum number of turns taken during baseline. PND scores higher than 90% indicate a treatment is “highly effective” (Scruggs, Mastropieri, Cooks, & Escobar, 1986).
Figure 4.

Number of turns per 15-min sessions for Kenneth, Owen, and Carl
Figure 6.

Number of turns per 15-min sessions for Tomieka, Lucille, and Henry
Kenneth (Figure 4) was most motivated by activities surrounding rock music and sports teams. He had a higher number of turns during both baseline and intervention than the other participants. He demonstrated an average of 25 turns (range 21–33) during baseline, and more than doubled his average number of turns during intervention to 59 (range 39–78). Upon his first introduction to the technology and the JIT system his increase in turns was modest, only 6 turns above the highest baseline session. However, this level quickly jumped to 56 turns by the second intervention session. Owen took between 0–2 turns during baseline. The 2 turns, which occurred during one baseline session, consisted of pointing to the word “yes” on a white board. During the intervention sessions Owen took 18–36 turns within the 15 min sessions. He was most interested in songs with a strong beat and books and magazines that contained nature and wildlife pictures. Similarly, Carl took an average of 1 turn per baseline session. The majority of the baseline sessions were 0 turns, while in the first session he signed MUSIC 5 times and MORE once. During the intervention sessions, Carl took between 12–26 turns, selecting vocabulary programmed JIT about songs and table top games (e.g., ring toss).
Amina (Figure 5) was very interested in music-based activities, such as listening to songs or playing music with instruments. She also participated in a bowling activity. She did not take any turns during baseline. During intervention, she increased her turns to 26–34 turns, with an immediate effect upon the introduction of the system. Similarly, Ivan also took no turns during baseline. He did not show any interest to any table activities during the sessions and preferred to wander freely. He was interested, however, in choosing and listening to music, specifically songs from the 1970s. Upon introduction to the system during intervention, his turns increased to 14–28 across the sessions. In contrast, Nadia was interested in the table activities, such as pom poms, beanbag basketball, and musical instruments. She took between 1–10 turns during baseline, almost exclusively consisting of the sign approximation for MORE. She gradually decreased the number of times she used this sign across baseline sessions. During intervention she took 16–30 turns, using the system to comment on the activity and request alternate activities.
Figure 5.

Number of turns per 15-min sessions for Amina, Ivan, and Nadia
The last set of participants showed a similar pattern. Tomieka (Figure 6) took 2 turns during the first baseline session (YES), but did not take any further turns during baseline sessions until intervention when she took 14–33 turns. She was interested in creating craft materials, reading constructed books about animals, and participating in social routines. Lucille expressed one concept during baseline, an idiosyncratic sign indicating pain, taking 0–2 turns during the five sessions. She also demonstrated interest in the constructed books and social routines, as well as some songs. She took 25–30 during intervention. Lastly, Henry took 1–3 turn during baseline. He used sign approximations for BIRD and MORE, and a speech approximation for yeah. During intervention, Henry’s turns increased to 13–56. He liked engaging in and commenting on a beanbag basketball activity and songs.
The number of concepts cumulatively available to each participant during the intervention sessions are shown in Figure 7. An average of 4 vocabulary concepts (hotspots) was added during each intervention session using JIT technology (range 2–14). By the final intervention session (typically 5–7 sessions), an average of 22 vocabulary concepts were available to each participant (range 11–50). After 75 min of intervention for each participant (after the 5th intervention session for each), an average of 21 vocabulary concepts was available to participants (range 11–42) using only the JIT programming (i.e., vocabulary were not pre-programmed).
Figure 7.

Cumulative totals of vocabulary concepts available for intervention sessions
Impact of VSD and JIT Technology on Communication Modes
The number and type of communication modes used by each participant are shown graphically in Figure 8. As is apparent in the figure, the majority of turns taken by the participants after the technology was introduced was using the VSDs on the AAC technology. Participants who used signs, idiosyncratic signs/gestures, and sign approximations continued to use this mode of communication after the AAC technologies were introduced, to varying degrees.
Figure 8.

Modes of communication turns for each session
Number and Type of Opportunities
In an effort to determine if the communication turns increased during the intervention phases because of another element introduced during intervention, a post hoc analysis was performed. While a minimum number of opportunities was specified for each participant in each session, it may be the case that the interventionist unintentionally provided more opportunities during intervention. If so, the increase of communication turns during intervention may be attributable to an increase in opportunities provided, and not to the intervention with AAC technologies. Figure 9 presents graphs for each participant with the number of communication opportunities provided during each session. The number of communication turns taken are also provided in the graphs for comparison purposes. A communication opportunity was defined as a comment, question, or choice directed by the partner to the participant followed by a wait time of at least 5 s or followed by a response from the participant before 5 s elapsed (adapted from Light et al., 1985). As can be seen in the figure, the number of opportunities may have differed from baseline to intervention for some participants, but not for others. In particular, there appears to be an increase in the number of opportunities presented to Tomieka during intervention relative to baseline, and potentially with Kenneth, Carl and Lucille, although to different degrees. An increase is not visually evident for the remaining five participants. There is no clear and apparent pattern overall. Therefore, it may be reasonable to conclude that a difference in the number of opportunities may have influenced performance in intervention relative to baseline for some participants, but this alone does not fully explain the increase in communication turns.
Figure 9.

Communication opportunities and communication turns during all sessions (*Note: unable to code communication opportunities due to corruption of the video files)
Another possibility is that it is not the number of opportunities that is most important, but the type of opportunities. To address this, each opportunity identified was coded as an opportunity following a choice, a question, or a comment. These results are shown in Figure 10, which presents the relative percentages of each of these opportunity types. Again, some differential patterns may be apparent. For example, Carl, Tomieka, and Lucille were presented with more choices during baseline than intervention, while the opportunities presented to Amina and Ivan show an opposite pattern. No consistent pattern is apparent overall. As with number of opportunities, the opportunity types may have influenced the outcomes to some degree, but do not appear to explain the differences seen in communication turns.
Figure 10.
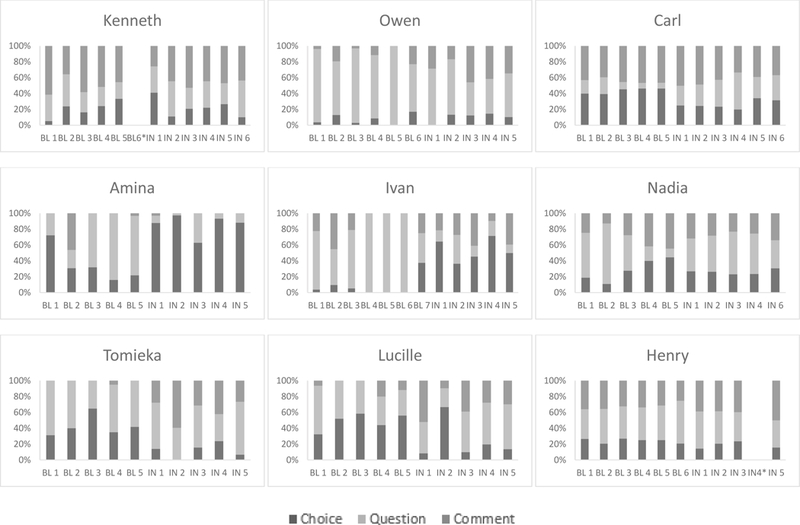
Relative percentages of all communication opportunities during all sessions (*Note: unable to code communication opportunities due to corruption of the video files)
Discussion
The current intervention resulted in increased symbolic communication skills for school age children, adolescents, and young adults with the introduction of AAC technologies. This adds to the literature base on the support for systematic intervention with individuals with severe disability (Snell, et al., 2010). The availability and use of an AAC app that included VSDs and JIT programming was effective in increasing the number of communicative turns for all nine participants. Additionally, the participants who did use signs and idiosyncratic signs/gestures during baseline did not, for the most part, decrease their use of these upon introduction of AAC technologies. The current study highlights the results that can be obtained with appropriate interventions for older youth and young adults with severe disability. When interventions are appropriately designed and supports are appropriately provided, there is potential for significant improvement in communication skills for students at any age. The current intervention was chronologically age-appropriate, occurred within the natural environment, provided access to preferred activities and a means to participation, and involved reciprocal turn-taking by both partners in the interaction. These characteristics are among those suggested by Light, Parsons, and Drager (2002) as appropriate for beginning communicators who are presymbolic; these characteristics may be adapted to the needs of beginning communicators of any age.
The effectiveness of aided AAC intervention relies in large part on the design of the AAC system (Light, Drager, & Wilkinson, 2010). Systems must meet the individual’s cognitive, linguistic, and motoric needs. VSDs provide access to concepts and vocabulary available within a familiar environment (Wilkinson & Light, 2011), providing contextual support and facilitating language learning. JIT programming makes these VSDs immediately available and accessible.
Potential Effects of JIT Programming
Although it is impossible to separate out the effects of JIT programming from the other features of the AAC application, it is possible that the positive effects were due in part to the JIT characteristics. The ease of use of the AAC system allowed partners to easily program new activities and vocabulary that was motivating and interesting for the students. In addition, the JIT system allowed partners to respond contingently to the students’ interests and build on their current focus, without requiring programming of the system that was removed from the activity. As a result, the school-age children and adolescents were able to be more actively engaged in the shared activities. It allowed the interventionist to take advantage of events that happened spontaneously or events that may not have been anticipated before the start of the interaction.
The JIT programming was integrated into the ongoing shared context activities and did not require programming time separate from the interaction. Although parts of the sessions were used for this programming, it did not detract from the overall number of communication turns or participant engagement, as the new vocabulary was immediately available and functional for use. New VSDs and vocabulary relevant to the ongoing activity was often available in less than a minute from the time a decision was made to create a new VSD, allowing the participants to remain engaged in the activities.
Limitations of the Study and Future Research
Despite the positive outcomes, there are several limitations that must be considered. Most of the participants had some symbolic communication (although limited, as is consistent with the inclusionary criterion of being a beginning communicator). Therefore, the study was designed to investigate the effectiveness of the intervention to increase these skills. However, data were not collected on intentional but non-symbolic communication, which may have been a valid representation of the effects of the intervention.
Although each of the participants had access to an increasingly larger number of vocabulary items during intervention, data were not collected on whether the participants acquired the vocabulary and were able to use it appropriately in natural settings. Certainly the increase in communication turns indicates an increase in using the available vocabulary, but use was not documented outside of the sessions.
The small number of participants with a limited range of disabilities limits generalization. Future research should investigate these approaches to AAC intervention and AAC system design with a larger number and broader range of participants. Additionally, the ages of the participants spanned a range of 12 years. There are clearly different considerations necessary for an 8-year old child compared to a 20-year old emerging adult. Although the results were consistent for all the current participants, future research should seek to clarify these differences, and investigate maximizing outcomes for all adolescents and young adults. Also, some of the participants made greater gains than did others; future research should clarify the participant characteristics that may help to explain these results. Future research is also required to investigate the applicability of these findings to an even older population, that is, adults with developmental disability who have exited the school system, yet are still beginning communicators.
It is not possible to evaluate whether participants either generalized the communication skills to new environments or with new partners, as there was no generalization phase included. Similarly, it is not possible to determine whether the participants were able to maintain the levels of communication turns after intervention ended.
The single case multiple probe designs met all recommended evidence standards (Kratochwill, et al., 2002). However, due to recruitment and scheduling issues, the third participant in all three groups of students began baseline at a later point in time than the previous two participants. Thus, while baseline data are low and non-increasing for all of these participants, and presumably would have been consistent with this pattern had their baseline sessions started at the same time as the other students’ baseline sessions, it is impossible to know this with certainty. Additionally, the interventionists, as the researchers, were privy to the hypotheses of the study, which could have potentially influenced the results, although all data were coded from video by a separate coder. Future research should evaluate the intervention using interventionists and coders blind to the study. Future research should also involve parents, caregivers, and teachers to a greater extent, and consider multiple environments, including more inclusive environments that involve peers. In the current study a teacher or aide was present throughout the sessions, which all took place in the school setting, but they did not implement the intervention.
Lastly, it is impossible to disentangle the effects of the JIT programming specifically from the other features of the AAC app. It is possible that the increase in turns was due more to relevant vocabulary being provided in the moment than the use of VSDs, for example. In addition, the study used only a single application. New technologies continue to be developed and marketed; some of which have the capability of the elements described herein (VSDs, JIT, speech output). Future research is required to determine characteristics and features of these apps that are most appropriate for beginning communicators. The effects of JIT specifically could be evaluated by comparing this type of application to another AAC app with VSD capability but without JIT capability.
Conclusion
AAC technologies can provide the power of communication and social connection for individuals with disabilities; however, it is essential that the technologies be appropriately designed for each individual. VSDs can be used with beginning communicators at any age, and the addition of JIT technologies makes these displays more accessible. The fast and easy import of photographs for VSDs, as well as easy identification and creation of hotspots can provide critical vocabulary and communication options that may otherwise be unavailable to individuals with developmental disability within everyday contexts.
Acknowledgements
Portions of this project were presented at the biennial conference of the International Society for Augmentative and Alternative Communication, July 2014, Lisbon, Portugal.
This research was supported by an SBIR Phase 1 grant #1R43HD059231‐01A1 from the National Institutes of Health and by grant # H133E080011 from the National Institute on Disability and Rehabilitation Research of the U.S. Department of Education.
With appreciation to Abby Correia and Nicole Duffy for assistance with coding.
References
- Blackstone S, Light J, Beukelman D, & Shane H (2004). Visual scene displays. Augmentative Communication News, 16, 1–5. [Google Scholar]
- Calculator SN (1988). Promoting the acquisition and generalization of conversational skills by individuals with severe disabilities. Augmentative and Alternative Communication, 4, 94–103. [Google Scholar]
- Carter M (2003). Communicative spontaneity of children with high support needs who use augmentative and alternative communication systems I: Classroom spontaneity, mode, and function. Augmentative and Alternative Communication, 19, 141–154. [Google Scholar]
- Drager K, Light J, Carlson R, D’Silva K, Larsson B, Pitkin L, & Stopper G (2004). Learning of dynamic display AAC technologies by typically developing 3-year-olds: Effect of different layouts and menu approaches. Journal of Speech Language Hearing Research, 47, 1133–1148. [DOI] [PubMed] [Google Scholar]
- Drager KDR, Light JC, Curran Speltz J, Fallon KA, & Jeffries LZ (2003). The performance of typically developing 2 ½-year-olds on dynamic display AAC technologies with different system layouts and language organizations. Journal of Speech Language Hearing Research, 46, 298–312. [DOI] [PubMed] [Google Scholar]
- Johnston S, Reichle J, & Evans J (2004). Supporting augmentative and alternative communication use by beginning communicators with severe disabilities. American Journal of Speech-Language Pathology, 13, 20–30. [DOI] [PubMed] [Google Scholar]
- Kratochwill TR, Hitchcock J, Horner RH, Levin JR, Odom SL, Rindskopf DM & Shadish WR (2010). Single-case designs technical documentation. Retrieved from What Works Clearinghouse website: http://ies.ed.gov/ncee/wwc/pdf/wwc_scd.pdf.
- Light J, Collier B, & Parnes P (1985). Communication interaction between young nonspeaking physically disabled children and their primary caregivers: Part I – discourse patterns. Augmentative and Alternative Communication, 1, 74–83. [Google Scholar]
- Light J & Drager K (2002). Improving the design of augmentative and alternative communication technologies for young children. Assistive Technology, 14, 17–32. [DOI] [PubMed] [Google Scholar]
- Light J, & Drager K (2009). Early intervention for young children with autism, cerebral palsy, Down syndrome, and other disabilities. Retrieved September 26, 2014 from http://aackids.psu.edu/index.php/page/show/id/1
- Light J, Drager K, & Wilkinson K (2012, July). Designing Effective Visual Scene Displays for Young Children with Complex Communication Needs. Paper presented at the biennial conference of the International Society for Augmentative and Alternative Communication, Pittsburgh, PA. [Google Scholar]
- Light J, Jakobs T, Drager K, Chew K, Guthrie S, Mellman L, & Riley K (2012, August). Effects of AAC Systems with “Just in Time” Programming for Children with Complex Communication Needs. Poster presented at the biennial conference of the International Society for Augmentative and Alternative Communication, Pittsburgh, PA. [Google Scholar]
- Light J, Drager K, McCarthy J, Mellott S, Millar D, Parrish C, Parsons A, Rhoads S, Ward M, & Welliver M (2004). Performance of typically developing four- and five-year-old children with AAC systems using different language organization techniques. Augmentative and Alternative Communication, 20, 63–88. [Google Scholar]
- Light JC, Parsons AR, & Drager KDR (2002). “There’s more to life than cookies”: Developing interactions for social closeness with beginning communicators who require augmentative and alternative communication In Reichle J, Beukelman D, & Light J (Eds.) Exemplary practices for beginning communicators: Implications for AAC (pp. 187–218). Baltimore, MD: Paul H. Brookes Publishing Co., Inc. [Google Scholar]
- Olin AR, Reichle J, Johnson L, & Monn E (2010). Examining dynamic visual scene displays: Implications for arranging and teaching symbol selection. American Journal of Speech-Language Pathology, 19, 284–297. [DOI] [PubMed] [Google Scholar]
- Romski MA, Sevcik RA, Hyatt AM, & Cheslock M (2002). A continuum of language intervention strategies for beginning communicators In Reichle J, Beukelman D, & Light J (Eds), Exemplary practices for beginning communicators: Implications for AAC (pp. 1–23). Baltimore, MD: Paul H. Brookes. [Google Scholar]
- Rowland C (1996). Communication matrix. Portland, OR: Design to Learn. [Google Scholar]
- Schlosser RW, Shane HC, Allen AA, Abramson J, Laubscher E, & Dimery K (2015). Just-in-time supports in augmentative and alternative communication. Journal of Developmental and Physical Disabilities, Advance online publication. doi: 10.1007/s10882-015-9452-2 [DOI] [Google Scholar]
- Scruggs TE, Mastropieri MA, & Casto G (1987). The quantitative synthesis of single-subject research: Methodology and validation. Remedial and Special Education, 8, 24–33. [Google Scholar]
- Scruggs TE, Mastropieri MA, Cook S , & Escobar C (1986). Early intervention for children with conduct disorders: A quantitative synthesis of single-subject research. Behavioral Disorders, 11, 260–271. [Google Scholar]
- Smith MM (2014). Adolescence and AAC: Intervention challenges and possible solutions. Communication Disorders Quarterly. Advanced online publication. doi: 10.1177/1525740114539001. [DOI] [Google Scholar]
- Snell ME, Brady N, McLean L, Ogletree BT, Siegel E, Sylvester L, Mineo B, Paul D, Romski MA, & Sevcik R (2010). Twenty years of communication intervention research with individuals who have severe intellectual and developmental disabilities. American Journal on Intellectual and Developmental Disabilities, 115, 364–380. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spiker D, Boyce G, & Boyce L. (2002). Parent-child interactions when young children have disabilities. International Review of Research in Mental Retardation, 25, 35–70. [Google Scholar]
- Warren SF, & Brady NC (2007). The role of maternal responsivity in the development of children with intellectual disabilities. Mental Retardation and Developmental Disabilities Research Reviews, 13, 330–338. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wilkinson K, & Light J (2011). Preliminary investigation of visual attention to human figures in photographs: Potential considerations for the design of aided AAC visual scene displays. Journal of Speech, Language & Hearing Research, 54, 1644–1657. [DOI] [PMC free article] [PubMed] [Google Scholar]