

Abstract
Background:
Anterior cruciate ligament (ACL) tear is a common injury in sports and often occurs during landing from a jump.
Purpose:
To synthesize the evidence on the effects of injury prevention programs (IPPs) on landing biomechanics as they relate to the ligament, quadriceps, trunk, and leg dominance theories associated with ACL injury risk.
Study Design:
Meta-analysis.
Methods:
Six electronic databases were searched for studies that investigated the effect of IPPs on landing task biomechanics. Prospective studies that reported landing biomechanics at baseline and post-IPP were included. Results from trunk, hip, and knee kinematics and kinetics related to the ACL injury theories were extracted, and meta-analyses were performed when possible.
Results:
The criteria were met by 28 studies with a total of 466 participants. Most studies evaluated young females, bilateral landing tasks, and recreational athletes, while most variables were related to the ligament and quadriceps dominance theories. An important predictor of ACL injury, peak knee abduction moment, decreased (P = .01) after the IPPs while other variables related to the ligament dominance theory did not change. Regarding the quadriceps dominance theory, after the IPPs, angles of hip flexion at initial contact (P = .009), peak hip flexion (P = .002), and peak knee flexion (P = .007) increased, while knee flexion at initial contact did not change (P = .18). Moreover, peak knee flexion moment decreased (P = .005) and peak vertical ground-reaction force did not change (P = .10).
Conclusion:
The exercises used in IPPs might have the potential to improve landing task biomechanics related to the quadriceps dominance theory, especially increasing peak knee and hip flexion angles. Importantly, peak knee abduction moment decreased, which indicates that IPPs influence a desired movement strategy to help athletes overcome dangerous ligament dominance loads arising from lack of frontal plane control during dynamic tasks. The lack of findings for some biomechanical variables suggests that future IPPs may be enhanced by targeting participants’ baseline profile deficits, highlighting the need to deliver an individualized and task-specific IPP.
Keywords: kinematics, kinetics, sports injury, neuromuscular training
Anterior cruciate ligament (ACL) tear is one of the most common knee injuries in sports, especially in those involving landing49 and cutting tasks40 such as soccer, volleyball, and American football.20 A study that analyzed mechanisms of ACL injuries in elite women’s netball reported that more than 80% of ACL tears occurred during landing tasks.49
Moreover, due to higher participation rates in sports activities among adolescents and young adults compared with other age groups, ACL injuries are more common among these young people, with an annual incidence reaching almost 69 per 100,000 person-years.20,45 The consequences of ACL injury can be severe; even after successful ACL reconstruction, only 55% of athletes return to competitive sport levels within the first year.2 More important, an ACL tear frequently leads to early posttraumatic knee osteoarthritis regardless of treatment.37
In-depth biomechanical understanding of noncontact ACL injury and associated risk factors is required for the development of effective injury prevention programs (IPPs).26 Four theories13 have been proposed to characterize ACL injury risk in athletes; these theories suggest that participants at high risk of injury land from a jump (1) with their knee in a valgus position and their femur in adduction and internal rotation, thus loading the knee ligaments excessively (ligament dominance theory); (2) with the knee in an extended position and with excessive quadriceps activation relative to the hamstrings, thus generating an anterior shear stress to the tibia (quadriceps dominance theory); (3) with deficits in trunk control (trunk dominance theory); and (4) with large leg-to-leg asymmetries (leg dominance theory). Video analyses of ACL injuries support the 4 theories, as these analyses identified excessive knee valgus (ligament dominance), decreased knee flexion angle (quadriceps dominance), excessive lateral trunk displacement (trunk dominance), and asymmetrical body weight distribution between the 2 legs (leg dominance) during the occurrence of ACL tears.16,22,49
Prevention of ACL injury should target modifiable biomechanical and neuromuscular risk factors. IPPs reduce ACL injuries, although we do not know the exact mechanisms behind this outcome.14,44,50 Several studies have investigated the effectiveness of IPPs designed to improve the biomechanics of landing associated with ACL injury∥∥; however, a comprehensive evaluation of the literature has not been conducted.
Thus, the purpose of this systematic review is to synthesize the evidence on the effect of IPPs on landing biomechanics as they relate to the ligament, quadriceps, trunk, and leg dominance theories of ACL injury.
METHODS
Protocol and Registration
A review protocol was registered in the International Prospective Register of Systematic Reviews (CRD42015020312).
Data Sources
Six electronic databases (MEDLINE, Web of Science, EMBASE, SCOPUS, SportDiscus, and CINAHL) were searched from the earliest records to June 2015 by use of relevant terms. Appendix A, available in the online version of this article, describes the search strategy and results.
Study Selection
Two investigators (T.J.A.L. and E.P.) independently screened titles and abstracts. Full texts were obtained if at least 1 investigator indicated that the study could not be excluded by the title and abstract.
Studies were included if they investigated landing tasks (unilateral or bilateral) by using a 3-dimensional (3D) motion analysis system or by measuring kinetics via a force plate. The studies that fit the aforementioned criteria also had to report data on at least 1 variable associated with at least 1 of the 4 dominance theories. We included any type of prospective study written in English, whereas abstracts or presentations were excluded. Data were extracted from the baseline and post-IPP results. We used the results from the intervention group only, except for studies in which the IPP of the control group met the inclusion criteria, in which case the results from the control group were also included.
Inclusion criteria for the IPPs consisted of training that focused primarily on injury prevention instead of performance enhancement and that occurred for a minimum of 2 days. When different components of the IPPs were presented, all of them were selected for our comparisons if they met the inclusion criteria. In the presence of multiple post-IPP evaluation time points, the assessment immediately after conclusion of the IPP was used.
Participants were included if they were injury-free and over the age of 10. No limits were placed on athletic level and sex; however, to allow for subgroup analysis based on sex, only studies that reported males and females separately were accepted. Last, when data were presented for both limbs (right and left) and for both single-and double-leg landing tasks, the right limb and double-leg landing task were chosen as they were the most commonly reported.
Methodological Assessment
The methodological quality of the studies was evaluated independently by 2 investigators (T.J.A.L. and M.S.). A 15-item, custom-designed, methodological quality assessment scale adapted from Downs and Black10 (questions 1, 6, 9, 11, 12, and 15) and Brown et al5 (questions 2–5, 7, 8, 10, 13, and 14) was used for evaluation purposes. An adapted quality index tool was applied for our review purposes, as the Downs and Black tool was designed mainly for randomized clinical trial studies, rendering some items nonapplicable for the assessment of cross-sectional studies, and the Brown et al tool was designed specifically to assess biomechanical studies. Choosing relevant items from both questionnaires allowed for a more comprehensive assessment of the quality of the studies. Items were scored as 0 = “clearly no,” 1 = “maybe or inadequate information,” and 2 = “clearly yes,” comprising a 30-point scoring system (Appendix B). Any disagreements, which represented 16% of total quality analysis assessment (68 disagreements in 420 items), were resolved by consensus.
Data Extraction
The main outcome variables data we planned to extract regarding the ligament dominance theory13 included hip and knee adduction-abduction at initial contact (IC), peak hip and knee adduction-abduction angles and external moment, and peak hip internal rotation kinematics. Outcome variables data related to the quadriceps dominance theory13 consisted of hip and knee flexion at IC, peak hip and knee flexion angles and external moment, and peak vertical ground-reaction force (vGRF). Planned data extraction for the trunk dominance theory consisted of trunk lateral flexion and trunk rotation,13 and for the leg dominance theory we planned to extract data from variables that examined side-to-side differences.
Due to the different conventions reported by the studies concerning adduction-abduction signs, we adopted the following biomechanical convention: hip adduction (+)/abduction (–) and knee adduction (+)/abduction (–) angles and external moments.
Apart from the biomechanical variables, data were extracted regarding sample size; type, intensity, and duration of IPP; and participants’ age and sex. One investigator (T.J.A.L.) independently extracted data from the selected full-text articles, while a second investigator (E.P.) double checked that all data were correct.
Data Analysis
Review Manager (RevMan 5.3.5; Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014) was used for the meta-analysis by entering means, standard deviations (SDs), and sample sizes before and after the IPPs on all relevant outcome variables that were reported by 2 or more studies. After testing for heterogeneity with the I2 statistic (a priori defined cutoff at I2 ≤ 75%), an inverse variance with random effects approach was used with mean difference effect measures when the scale between the studies was the same and with standardized mean difference when the scales were different.17 Forest plots and 95% confidence intervals (CIs) were produced as per the Cochrane Handbook.17
RESULTS
Study Characteristics
A total of 28 studies¶¶ met the inclusion criteria; however, studies38,42,52 were excluded from the quantitative analysis because they did not provide descriptive data (Figure 1). The authors of those studies were contacted via email, but the requested data could not be obtained.
Figure 1.
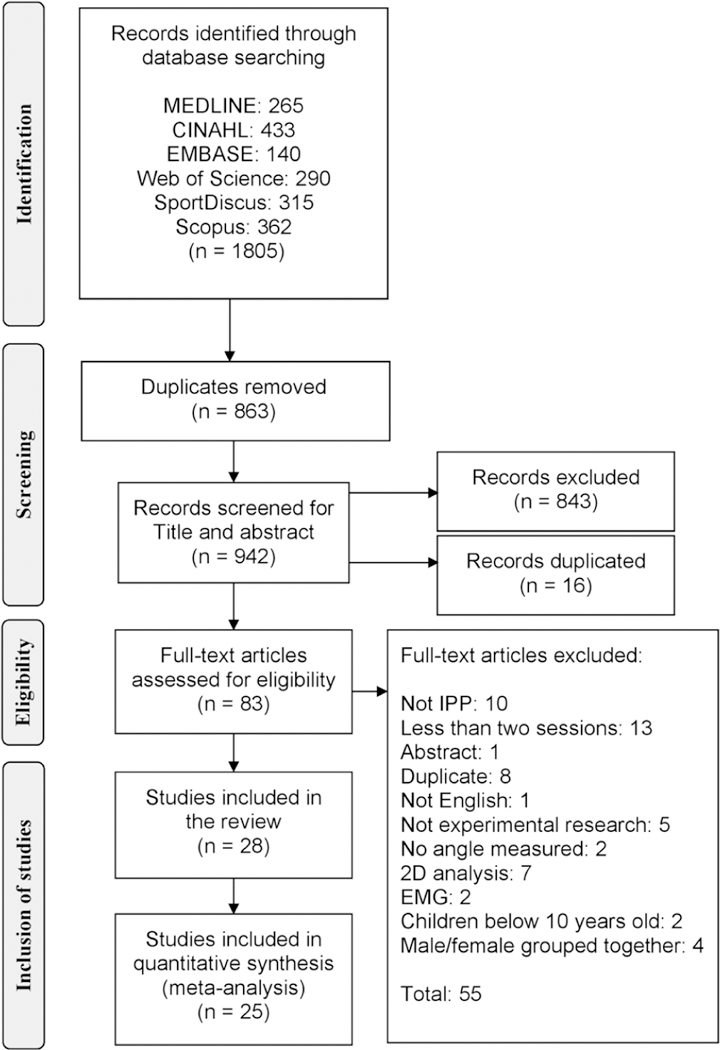
Preferred reporting items for systematic reviews and meta-analyses (PRISMA) flow diagram of search results. EMG, electromyography; IPP, injury prevention program.
Across all studies, a total of 466 participants received an IPP. Twenty-four of the 28 studies included only female participants, while 22 studies used a bilateral leg landing task. In general, participants were athletes or recreational athletes with mean age ranging from 14 to 27 years old.
The IPPs varied from multiple interventions that mixed balance, plyometric, and neuromuscular training to single interventions such as strength or jump-landing training. These programs generally lasted from 4 to 10 weeks of training. A summary of each study, including participant characteristics, sample size, landing task, and IPP intervention, is provided in Appendix C.
Quality Assessment
The methodological quality scores ranged from 17 to 26 of a possible 30 points (Appendix B). Almost all studies met the criteria for 8 questions: clearly define the aim/hypothesis (question 1), clearly define participants’ demographics (question 3) and characteristics (question 4), clearly describe interventions (question 6), describe methods in detail (question 8), clearly define outcome variables (question 13), conduct appropriate statistical analysis (question 14) and provide estimates of random variability (question 15) A large number of studies did not meet the criteria for 6 questions: perform sample size power analysis (question 2), clearly state inclusion and exclusion criteria (question 5), allow participants proper training practice before the test (question 7), attempt to blind the assessors (question 9), report the measurement’s test-retest reliability (question 10), and monitor participants’ compliance with the intervention (question 12).
Heterogeneity Assessment
Differences in landing biomechanics have been reported to exist between males and females21 as well as between unilateral and bilateral landing tasks.39 Because some of the studies reviewed (9/28) reported results regarding male subjects or unilateral tasks, we decided to keep these studies and run a sensitivity analysis to check for differences in the overall results and increased I2. Despite finding no difference or high I2, we retained these studies in the quantitative analysis.
Furthermore, we retained in the quantitative analysis 2 studies1,19 that increased the I2 for peak vGRF, because after sensitivity analysis no change was found in the final result. One study27 increased the I2 in 2 different outcomes; peak knee flexion angle and peak vGRF. Thus, to avoid a study selection bias, we excluded this particular study from the meta-analysis.
Ligament Dominance Theory
Results of all meta-analyses related to the ligament and quadriceps dominance theories are presented in Table 1. The quantitative analysis revealed that peak knee abduction moment decreased after the IPPs (P = .01; Figure 2). In contrast, hip adduction at IC (P = .90), peak hip adduction (P = .48), knee abduction at IC (P = .55), and peak knee abduction (P = .45) angles as well as peak hip adduction moment (P = .63) did not change after the IPPs.
TABLE 1.
Summary of Meta-analysis Evaluating the Effect of IPPs on Primary Biomechanical Variables Related to the Quadriceps and Ligament Dominance Theoriesa
| Kinematic Variables | No. of Studies |
Reference No. | n | Heterogeneity | Test for Overall Effect |
Mean Difference |
95% CI | Result After IPP |
||
|---|---|---|---|---|---|---|---|---|---|---|
| P | I2 | Z | P | |||||||
| Hip flexion at IC | 4 | 8, 11, 18, 23 | 79 | .22 | 30% | 2.60 | .009 | 4.21 | 1.04 to 7.38 | Increased |
| Peak hip flexion | 8 | 6, 8, 11, 12, 18, 23, 30, 48 | 173 | .60 | 0% | 3.14 | .002 | 3.70 | 1.39 to 6.01 | Increased |
| Hip adduction at IC | 3 | 8, 23, 33 | 75 | .19 | 37% | 0.12 | .90 | –0.15 | –2.60 to 2.30 | No effect |
| Peak hip adduction | 5 | 6, 8, 23, 33, 43 | 123 | .15 | 35% | 0.70 | .48 | –0.60 | –2.27 to 1.07 | No effect |
| Knee flexion at IC | 6 | 8, 9, 11, 18, 23, 35 | 104 | .08 | 47% | 1.33 | .18 | 1.83 | –0.87 to 4.52 | No effect |
| Peak knee flexion | 13 | 6–9, 11, 12, 15, 18, 23, 25, 30, 43, 48 | 237 | .15 | 28% | 2.69 | .007 | 2.86 | 0.78 to 4.95 | Increased |
| Knee abduction at IC | 5 | 3, 8, 11, 23, 33 | 108 | .45 | 0% | 0.60 | .55 | –0.25 | –1.05 to 0.56 | No effect |
| Peak knee abduction | 11 | 3, 6, 8, 11, 12, 23, 30, 33, 43, 48, 51 | 239 | .94 | 0% | 0.75 | .45 | –0.29 | –1.05 to 0.47 | No effect |
| Kinematic Variables | No. of Studies |
Reference No. | n | Heterogeneity | Test for Overall Effect |
Standard Mean Difference |
95% CI | Result After IPP |
||
| P | I2 | Z | P | |||||||
| Peak hip flexion moment | 5 | 6, 8, 11, 18, 23 | 109 | .31 | 15% | 1.42 | .16 | –0.22 | –0.51 to 0.08 | No effect |
| Peak hip adduction moment | 4 | 6, 8, 12, 23 | 126 | .72 | 0% | 0.48 | .63 | 0.06 | –0.19 to 0.31 | No effect |
| Peak knee flexion moment | 7 | 6, 8, 9, 11, 18, 23, 51 | 139 | .76 | 0% | 2.81 | .005 | –0.34 | –0.58 to –0.10 | Decreased |
| Peak knee abduction moment | 12 | 3, 6–9, 11, 12, 23, 25, 32, 34, 51 | 260 | .10 | 33% | 2.44 | .01 | –0.28 | –0.50 to –0.05 | Decreased |
| Peak vGRF | 10 | 1, 3, 8, 12, 15, 19, 23, 28, 31, 51 | 214 | .02 | 49% | 1.63 | .10 | –0.23 | –0.51 to 0.05 | No effect |
Most forest plots are in Appendix D. IC, initial contact; IPP, injury prevention program; vGRF, vertical ground-reaction force.
Figure 2.
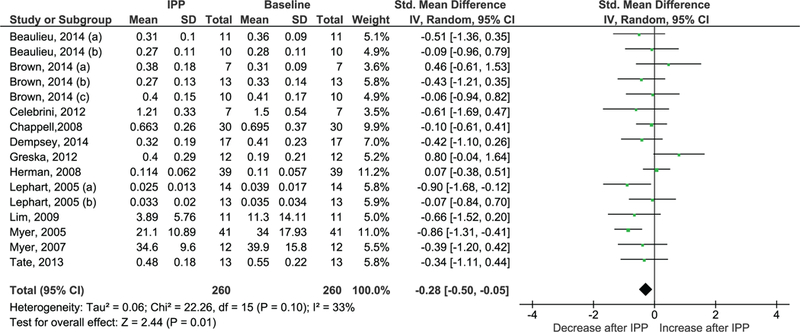
Peak knee abduction moment (Nm or N m/BM or N m/BW*H). BM, body mass; BW, body weight; H, height; IPP, injury prevention program.
A study that did not provide descriptive data for a metaanalysis found a decreased peak knee abduction moment in 9 females after a 4-week plyometric-based IPP,42 while another study did not find any effect of the IPP on 14 females for peak knee abduction angle.38 Only 1 study reported data regarding peak hip internal rotation, which decreased after a soccer season’s preventive program that consisted of stretching, strengthening, plyometric, and agility execises.43
Quadriceps Dominance Theory
Meta-analysis revealed that hip flexion at IC (P = .009), peak hip flexion (P = .002), and peak knee flexion (P = .007) angles increased after the IPPs, while peak knee flexion moment decreased (P = .005). However, peak hip flexion moment (P = .16), knee flexion angle at IC (P = .18), and peak vGRF post-IPP (P = .10) (Figure 3) did not change.
Figure 3.
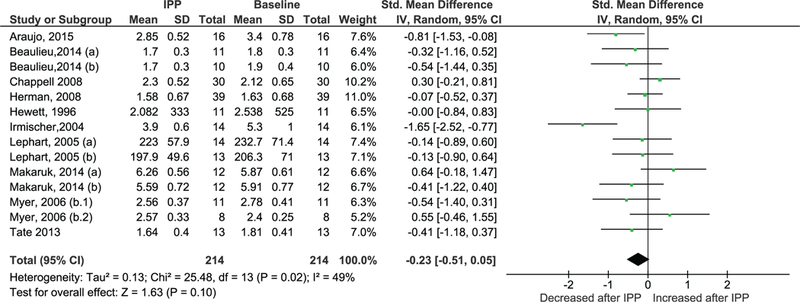
Peak vertical ground-reaction force (BW or %BW). BW, body weight; IPP, injury prevention program.
Among studies that did not provide descriptive data for a meta-analysis, one particular study found decreased peak knee flexion angle and moment in females, from 13% to 25% of the landing phase, after a 4-week plyometric-based IPP.42 Another study found no effect on peak knee flexion angle in female soccer players after 6 weeks of an IPP that consisted of flexibility, functional strength, and jumping-based training.38 A third study, which conducted a neuromuscular exercise program among adolescent basketball players, found increased peak knee flexion angle and decreased peak vGRF.27 A study52 that did not provide descriptive data for a meta-analysis also found no change in peak vGRF after a 6-week plyometric-based IPP in females, while Louw et al27 reported decreased peak vGRF after an IPP that consisted of multiple neuromuscular exercise programs.
Trunk and Leg Dominance Theories
Only 1 study9 investigated, in males, the effect of an IPP on variables related to the trunk dominance theory at IC. No statistical difference was found for trunk lateral flexion (pre-IPP, 8.2 ± 6.3; post-IPP, 5.4 ± 7.6; P = .263) and trunk rotation (pre-IPP, 43.7 ± 23.1; post-IPP, 36 ± 20.4; P = .213). None of the studies included any variable associated with the leg dominance theory.
DISCUSSION
The purpose of this systematic review was to synthesize the evidence regarding the effect of IPPs on landing biomechanics as they relate to the ligament, quadriceps, trunk, and leg dominance theories of ACL injury. A number of important findings emerged: (1) After the IPPs, participants landed with decreased peak knee abduction moment, potentially decreasing their risk factors for ACL injury; (2) after the IPPs, participants landed with increased hip and knee flexion, thus potentially decreasing risk factors associated with the quadriceps dominance theory; (3) IPPs do not appear to result in “softer” landings as measured by peak vGRF; and (4) a dearth of studies are available on the effects of IPPs on variables related to the trunk and leg dominance theories as well as on males in general.
Importantly, the IPPs led to a reduced peak knee abduction moment, which can be helpful from a clinical point of view because this parameter demonstrates 78% sensitivity and 73% specificity as a predictor of ACL injury.14 Promising yet mixed results regarding the ligament dominance theory were found: Peak knee abduction moment was decreased but the other variables associated with this theory, for instance, hip adduction at IC, peak hip adduction, peak hip adduction moment, knee abduction at IC, and peak knee abduction angle, did not reach the same statistically significant findings. We expected that IPPs would positively affect all other variables related to the ligament dominance theory; however, this did not occur. A number of reasons may account for these findings. For instance, from all studies6,8,23,33,43 that assessed hip adduction at IC and peak hip adduction, only one group of participants presented at baseline the risk factor for ACL injury, while most of them landed with the hip abducted pre-IPP.
Furthermore, evidence indicates that an individualized IPP, targeted to the person’s specific risk factors, may be more beneficial than a generic program.32 One study used a prescreening method to identify “high-risk” athletes, defined as those having a high knee abduction moment, and then delivered the IPP to all athletes; only the high-risk athletes had a reduced peak knee abduction moment after the intervention.32 Moreover, a recent study demonstrated that only 36% of female athletes exhibited signs of a ligament dominance deficit.41 Consequently, when provided to all participants, IPPs likely do not make much difference for the majority of participants because they do not have the deficit present.
Regarding the quadriceps dominance theory, IPPs produce changes that are considered protective of ACL injury, such as increased hip and knee flexion during landing. The majority of studies6,8,9,18,23,25,48 that reported increased peak hip and knee flexion angles included activities that prioritized soft landings by increasing knee flexion during IPPs that implemented plyometrics and jump-landing tasks. A potential mechanism by which these changes can protect from ACL tear is that greater hip and knee flexion places the hamstrings in an advantageous position for contraction46 and possibly allows them to act as ACL synergists by pulling the tibia posteriorly, decreasing the anterior tibial force29 and enhancing energy absorption during landing.36 Additionally, greater knee flexion angle at the beginning of landing decreases the forces within the ACL.4 Thus, to improve variables related to the quadriceps dominance theory during a landing task, an IPP consisting of plyometrics and jump-landing exercises that facilitates greater flexion in the knee and hip might be helpful.
Regarding the peak vGRF, it is unclear why the IPPs had no effect for either females or males. Ample evidence shows that landing with greater lower-limb flexion can decrease vGRF47,53; however, even though we found a statistically significant increase in peak hip and knee flexion after IPPs, these changes did not produce lower peak vGRF. Interestingly, of all studies1,3,15,19,28,31,51 that individually reported a statistically significant decrease in peak vGRF, only 1 study1 did not entail a jump-landing training program as the main IPP. Thus, although overall the IPPs had no effect on peak vGRF, it appears that in those individual studies where the IPP consisted mainly of improving landing mechanics, the peak vGRF decreased; however, it is unknown whether focusing on landing mechanics alone to decrease peak vGRF will be sufficient to decrease injury rate.50
Some limitations emerged from this review, as the lack of uniform reporting of biomechanical variables could have decreased the power of the statistical analysis. Furthermore, only a small number of studies included male participants, which limited the power of the subgroup analysis between sexes. Only 1 study9 presented data regarding the trunk dominance theory, and no study was found related to the leg dominance theory. The methodological quality rating revealed that some important methodological features could have influenced the overall results: Only 2 studies blinded testers during assessment; 8 studies reported test-retest reliability of 3D measurement between pre- and posttest assessment; and 13 studies satisfactorily controlled the participants’ compliance (Appendix B). Last, some of the IPPs varied greatly among studies in terms of duration, intensity, and type, raising the possibility that the findings of a meta-analysis may be different as a larger number of studies with more homogeneous programs are published.
In conclusion, regarding the ligament dominance theory, one important variable linked to ACL injury, peak knee abduction moment, significantly decreased after the IPPs. However, some of the other variables related to this theory were not as sensitive to changes from IPPs. Due to differences in the methodological aspects of the studies, it is not clear whether the lack of effect related to the ligament dominance theory is due to participants’ baseline biomechanical profiles or due to the content of IPPs, which should prioritize individualized, task-specific exercises related to the athlete’s risk profile and should provide the necessary control of compliance, duration, and progression of training programs. IPPs in general appear to be effective at reducing some biomechanical risk factors related to the quadriceps dominance theory, especially IPPs that consist of activities to increase hip and knee flexion angles, such as plyometrics and jump-landing tasks. While improvements were found in hip and knee flexion angles, no change was found for peak vGRF.
Supplementary Material
Acknowledgments
source of funding: T.J.A.L. is supported by the National Council for Scientific and Technological Development (CNPq) program “Science without Borders,” Brazil; and by the University of Sydney International Scholarship (USydlS). G.D.M. acknowledges funding support from National Institutes of Health (NIH)/National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS) grants R21AR065068–01A1 and U01AR067997. T.E.H. acknowledges funding support from NIH/NIAMS grants R01AR55563 and R01AR056259. E.P., K.R.F., G.D.M., and T.E.H. acknowledge funding support for this project from NIH grants 5SC3 GM102053. K.R.F. acknowledges funding support from NIH/NIAMS grant R21AR069873.
Footnotes
References 1, 3, 6–9, 11, 12, 15, 18, 19, 23–25, 27, 28, 30–35, 38, 42, 43, 48, 51, 52.
References 1, 3, 6–9, 11, 12, 15, 18, 19, 23–25, 27, 28, 30–35, 38, 42, 43, 48, 51, 52.
One or more of the authors has declared the following potential conflict of interest
REFERENCES
- 1.Araujo S, Cohen D, Hayes L. Six weeks of core stability training improves landing kinetics among female capoeira athletes: a pilot study. J Human Kinetics. 2015;45:27–37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Ardern CL, Taylor NF, Feller JA, Webster KE. Fifty-five per cent return to competitive sport following anterior cruciate ligament reconstruction surgery: an updated systematic review and meta-analysis including aspects of physical functioning and contextual factors. Br J Sports Med. 2014;48(21):1543–1552. [DOI] [PubMed] [Google Scholar]
- 3.Beaulieu ML, Palmieri-Smith RM. Real-time feedback on knee abduction moment does not improve frontal-plane knee mechanics during jump landings. Scand J Med Sci Sports. 2014;24(4):692–699. [DOI] [PubMed] [Google Scholar]
- 4.Beynnon BD, Fleming BC. Anterior cruciate ligament strain in-vivo: a review of previous work. J Biomech. 1998;31(6):519–525. [DOI] [PubMed] [Google Scholar]
- 5.Brown SR, Brughelli M, Hume PA. Knee mechanics during planned and unplanned sidestepping: a systematic review and meta-analysis. Sports Med. 2014;44(11):1573–1588. [DOI] [PubMed] [Google Scholar]
- 6.Brown TN, Palmieri-Smith RM, McLean SG. Comparative adaptations of lower limb biomechanics during unilateral and bilateral landings after different neuromuscular-based ACL injury prevention protocols. J Strength Cond Res. 2014;28(10):2859–2871. [DOI] [PubMed] [Google Scholar]
- 7.Celebrini RG, Eng JJ, Miller WC, Ekegren CL, Johnston JD, MacIntyre DL. The effect of a novel movement strategy in decreasing ACL risk factors in female adolescent soccer players. J Strength Cond Res. 2012;26(12):3406–3417. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Chappell JD, Limpisvasti O. Effect of a neuromuscular training program on the kinetics and kinematics of jumping tasks. Am J Sports Med. 2008;36(6):1081–1086. [DOI] [PubMed] [Google Scholar]
- 9.Dempsey AR, Elliott BC, Munro BJ, Steele JR, Lloyd DG. Can technique modification training reduce knee moments in a landing task? J Appl Biomech. 2014;30(2):231–236. [DOI] [PubMed] [Google Scholar]
- 10.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377–384. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Greska EK, Cortes N, Van Lunen BL, Onate JA. A feedback inclusive neuromuscular training program alters frontal plane kinematics. J Strength Cond Res. 2012;26(6):1609–1619. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Herman DC, Weinhold PS, Guskiewicz KM, Garrett WE, Yu B, Padua DA. The effects of strength training on the lower extremity biomechanics of female recreational athletes during a stop-jump task. Am J Sports Med. 2008;36(4):733–740. [DOI] [PubMed] [Google Scholar]
- 13.Hewett TE, Ford KR, Hoogenboom BJ, Myer GD. Understanding and preventing ACL injuries: current biomechanical and epidemiologic considerations—update 2010. N Am J Sports Phys Ther. 2010;5(4): 234–251. [PMC free article] [PubMed] [Google Scholar]
- 14.Hewett TE, Myer GD, Ford KR, et al. Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: a prospective study. Am J Sports Med. 2005;33(4):492–501. [DOI] [PubMed] [Google Scholar]
- 15.Hewett TE, Stroupe AL, Nance TA, Noyes FR. Plyometric training in female athletes: decreased impact forces and increased hamstring torques. Am J Sports Med. 1996;24(6):765–773. [DOI] [PubMed] [Google Scholar]
- 16.Hewett TE, Torg JS, Boden BP. Video analysis of trunk and knee motion during non-contact anterior cruciate ligament injury in female athletes: lateral trunk and knee abduction motion are combined components of the injury mechanism. Br J Sports Med. 2009;43(6):417–422. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Higgins JPT, Green S. Cochrane Handbook for Systematic Reviews of Interventions The Cochrane Collaboration, 2014. Chichester, England: John Wiley & Sons. [Google Scholar]
- 18.lida Y, Kanehisa H, Inaba Y, Nakazawa K. Short-term landing training attenuates landing impact and improves jump height in landing-to-jump movement. J Strength Cond Res. 2013;27(6):1560–1567. [DOI] [PubMed] [Google Scholar]
- 19.Irmischer BS, Harris C, Pfeiffer RP, DeBeliso MA, Adams KJ, Shea KG. Effects of a knee ligament injury prevention exercise program on impact forces in women. J Strength Cond Res. 2004;18(4): 703–707. [DOI] [PubMed] [Google Scholar]
- 20.Joseph AM, Collins CL, Henke NM, Yard EE, Fields SK, Comstock RD. A multisport epidemiologic comparison of anterior cruciate ligament injuries in high school athletics. J Athl Train. 2013;48(6): 810–817. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Kernozek TW, Torry MR, Van Hoof H, Cowley H, Tanner S. Gender differences in frontal and sagittal plane biomechanics during drop landings. Med Sci Sports Exerc. 2005;37(6):1003–1012. [PubMed] [Google Scholar]
- 22.Krosshaug T, Nakamae A, Boden BP, et al. Mechanisms of anterior cruciate ligament injury in basketball: video analysis of 39 cases. Am J Sports Med. 2007;35(3):359–367. [DOI] [PubMed] [Google Scholar]
- 23.Lephart SM, Abt JP, Ferris CM, et al. Neuromuscular and biomechanical characteristic changes in high school athletes: a plyometric versus basic resistance program. Br J Sports Med. 2005;39(12):932–938. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Letafatkar A, Rajabi R, Tekamejani EE, Minoonejad H. Effects of perturbation training on knee flexion angle and quadriceps to hamstring cocontraction of female athletes with quadriceps dominance deficit: pre-post intervention study. Knee. 2015;22(3):230–236. [DOI] [PubMed] [Google Scholar]
- 25.Lim BO, Lee YS, Kim JG, An KO, Yoo J, Kwon YH. Effects of sports injury prevention training on the biomechanical risk factors of anterior cruciate ligament injury in high school female basketball players [published correction appears in Am J Sports Med. 2011;39(3): NP1]. Am J Sports Med. 2009;37(9):1728–1734. [DOI] [PubMed] [Google Scholar]
- 26.Lin C-F, Liu H, Gros MT, Weinhold P, Garrett WE, Yu B. Biomechanical risk factors of non-contact ACL injuries: a stochastic biomechanical modeling study. J Sport Health Sci. 2012;1(1):36–42. [Google Scholar]
- 27.Louw Q, Grimmer K, Vaughan CL. Biomechanical outcomes of a knee neuromuscular exercise programme among adolescent basketball players: a pilot study. Phys Ther Sport. 2006;7(2):65–73. [Google Scholar]
- 28.Makaruk H, Czaplicki A, Sacewicz T, Sadowski J. The effects of single versus repeated plyometrics on landing biomechanics and jumping performance in men. Biol Sport. 2014;31(1):9–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Markolf KL, Burchfield DM, Shapiro MM, Shepard MF, Finerman GA, Slauterbeck JL. Combined knee loading states that generate high anterior cruciate ligament forces. J Orthop Res. 1995;13(6):930–935. [DOI] [PubMed] [Google Scholar]
- 30.McCurdy K, Walker J, Saxe J, Woods J. The effect of short-term resistance training on hip and knee kinematics during vertical drop jumps. J Strength Cond Res. 2012;26(5):1257–1264. [DOI] [PubMed] [Google Scholar]
- 31.Myer GD, Ford KR, Brent JL, Hewett TE. The effects of plyometric vs. dynamic stabilization and balance training on power, balance, and landing force in female athletes. J Strength Cond Res. 2006;20(2):345–353. [DOI] [PubMed] [Google Scholar]
- 32.Myer GD, Ford KR, Brent JL, Hewett TE. Differential neuromuscular training effects on ACL injury risk factors in “high-risk” versus “low-risk” athletes. BMC Musculoskelet Disord. 2007;8:39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Myer GD, Ford KR, McLean SG, Hewett TE. The effects of plyometric versus dynamic stabilization and balance training on lower extremity biomechanics. Am J Sports Med. 2006;34(3):445–455. [DOI] [PubMed] [Google Scholar]
- 34.Myer GD, Ford KR, Palumbo JP, Hewett TE. Neuromuscular training improves performance and lower-extremity biomechanics in female athletes. J Strength Cond Res. 2005;19(1):51–60. [DOI] [PubMed] [Google Scholar]
- 35.Nagano Y, Ida H, Akai M, Fukubayashi T. Effects of jump and balance training on knee kinematics and electromyography of female basket-ball athletes during a single limb drop landing: pre-post intervention study. Sports Med Arthrosc Rehabil Ther Technol. 2011;3(1):14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Norcross MF, Blackburn JT, Goerger BM, Padua DA. The association between lower extremity energy absorption and biomechanical factors related to anterior cruciate ligament injury. Clin Biomech (Bristol, Avon). 2010;25(10):1031–1036. [DOI] [PubMed] [Google Scholar]
- 37.Oiestad BE, Holm I, Aune AK, et al. Knee function and prevalence of knee osteoarthritis after anterior cruciate ligament reconstruction: a prospective study with 10 to 15 years of follow-up. Am J Sports Med. 2010;38(11):2201–2210. [DOI] [PubMed] [Google Scholar]
- 38.Ortiz A, Trudelle-Jackson E, McConnell K, Wylie S. Effectiveness of a 6-week injury prevention program on kinematics and kinetic variables in adolescent female soccer players: a pilot study. P R Health SciJ. 2010;29(1):40–48. [PubMed] [Google Scholar]
- 39.Pappas E, Hagins M, Sheikhzadeh A, Nordin M, Rose D. Biomechanical differences between unilateral and bilateral landings from a jump: gender differences. Clin J Sport Med. 2007;17(4):263–268. [DOI] [PubMed] [Google Scholar]
- 40.Pappas E, Nightingale EJ, Simic M, Ford KR, Hewett TE, Myer GD. Do exercises used in injury prevention programmes modify cutting task biomechanics? A systematic review with meta-analysis. Br J Sports Med. 2015;49(10):673–680. [DOI] [PubMed] [Google Scholar]
- 41.Pappas E, Shiyko MP, Ford KR, Myer GD, Hewett TE. Biomechanical deficit profiles associated with ACL injury risk in female athletes. Med Sci Sports Exerc. 2016;48(1):107–113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Pfile KR, Hart JM, Herman DC, Hertel J, Kerrigan DC, Ingersoll CD. Different exercise training interventions and drop-landing biomechanics in high school female athletes. J Athl Train. 2013;48(4): 450–462. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Pollard CD, Sigward SM, Ota S, Langford K, Powers CM. The influence of in-season injury prevention training on lower-extremity kinematics during landing in female soccer players. Clin J Sport Med. 2006;16(3):223–227. [DOI] [PubMed] [Google Scholar]
- 44.Pollard CD, Sigward SM, Powers CM. Limited hip and knee flexion during landing is associated with increased frontal plane knee motion and moments. Clin Biomech (Bristol, Avon). 2010;25(2): 142–146. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Sanders TL, Maradit Kremers H, Bryan AJ, et al. Incidence of anterior cruciate ligament tears and reconstruction: a 21-year population-based study. Am J Sports Med. 2016;44(6):1558–1564. [DOI] [PubMed] [Google Scholar]
- 46.Shultz SJ, Beynnon BD, Schmitz RJ. Sex differences in coupled knee motions during the transition from non-weight bearing to weight bearing. J Orthop Res. 2009;27(6):717–723. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Slater A, Campbell A, Smith A, Straker L. Greater lower limb flexion in gymnastic landings is associated with reduced landing force: a repeated measures study. Sports Biomech. 2015;14(1):45–56. [DOI] [PubMed] [Google Scholar]
- 48.Stearns KM, Powers CM. Improvements in hip muscle performance result in increased use of the hip extensors and abductors during a landing task. Am J Sports Med. 2014;42(3):602–609. [DOI] [PubMed] [Google Scholar]
- 49.Stuelcken MC, Mellifont DB, Gorman AD, Sayers MG. Mechanisms of anterior cruciate ligament injuries in elite women’s netball: a systematic video analysis. J Sports Sci. 2016;34(16):1516–1522. [DOI] [PubMed] [Google Scholar]
- 50.Sugimoto D, Myer GD, Foss KD, Hewett TE. Specific exercise effects of preventive neuromuscular training intervention on anterior cruciate ligament injury risk reduction in young females: meta-analysis and subgroup analysis. Br J Sports Med. 2015;49(5):282–289. [DOI] [PubMed] [Google Scholar]
- 51.Tate JJ, Milner CE, Fairbrother JT, Songning Z. The effects of a home-based instructional program aimed at improving frontal plane knee biomechanics during a jump-landing task. J Orthop Sports Phys Ther. 2013;43(7):486–494. [DOI] [PubMed] [Google Scholar]
- 52.Vescovi JD, Canavan PK, Hasson S. Effects of a plyometric program on vertical landing force and jumping performance in college women. Phys Ther Sport. 2008;9(4):185–192. [DOI] [PubMed] [Google Scholar]
- 53.Wernli K, Ng L, Phan X, Davey P, Grisbrook T. The relationship between landing sound, vertical ground reaction force, and kinematics of the lower limb during drop landings in healthy men. J Orthop Sports Phys Ther. 2016;46(3):194–199. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.