

Abstract
Background:
Unlike the literature on anterior cruciate ligament reconstruction, studies on medial patellofemoral ligament (MPFL) reconstruction lack evidence-based guidelines regarding postoperative rehabilitation. An effective postoperative protocol may contribute greatly to a successful outcome following MPFL reconstruction, yet the quality and variability of these published protocols remain unknown.
Purpose:
To assess the quality and variability of MPFL rehabilitation protocols publicly available on the internet and associated with US academic orthopaedic programs.
Study Design:
Systematic review.
Methods:
All available isolated MPFL reconstruction rehabilitation protocols from US academic orthopaedic programs participating in the Electronic Residency Application Service were collected and included in this review. These protocols were evaluated for inclusion of various rehabilitation components, the timing of suggested initiation of these activities, and whether the protocol used evaluation-based guidelines.
Results:
A total of 27 protocols were included. Of these, 25 (93%) recommended immediate postoperative bracing. Time to initiation of full weightbearing ranged from 2 to 8 weeks. The most common strengthening exercises endorsed were quadriceps sets (89%), straight-legged raise (85%), and leg press (81%). The most common proprioception exercises endorsed were balance board (41%), single-legged balance (41%), and TheraBand control (33%). The median time suggested to return to play was 17 weeks. No functional test appeared in the majority of the protocols. Of the 27 protocols, 20 (74%) used evaluation-based guidelines.
Conclusion:
There is substantial variability in content and timing across rehabilitation protocols following MPFL reconstruction. This lack of clear guidelines can cause confusion among patients, therapists, and surgeons, leading to suboptimal patient outcomes and making it difficult to compare outcomes across the literature.
Keywords: knee, ligaments, physical therapy, rehabilitation
The goal of medial patellofemoral ligament (MPFL) reconstruction is to stabilize the patella to enable patients to return to their baseline level of function, including the ability to return to preinjury activity level. Successful attainment of this goal not only requires technically successful surgery but is also presumably predicated on adherence to a comprehensive postoperative rehabilitation protocol.31 The MPFL literature is relatively lacking in evidence-based guidelines regarding postoperative rehabilitation, with many components of the protocol having been adapted from the anterior cruciate ligament (ACL) reconstruction rehabilitation literature, which is considerably more robust.3,8,11–15,17,20,21
Outcome data on patients completing specific rehabilitation programs following MPFL reconstruction are scarce. One study by Ahmad et al1 noted improvements in International Knee Documentation Committee, Kujala, Lysholm, and Tegner scores after a specified program detailing timing of range of motion (ROM) and strengthening exercises (quadriceps, hamstrings, and hip muscles) as well as running and agility training. A study by Steiner et al29 reported high patient satisfaction and Kujala and Lysholm scores after a specific protocol of weightbearing and active exercises, although it did not specify the timing of these activities. Without data or standardized protocols, generating evidence-based guidelines is an impossible task. One review published by the Musculoskeletal Institute at the Johns Hopkins Hospital makes recommendations on the timing of brace wear, weightbearing, ROM, activities, sport-specific training, and return to sport following MPFL reconstruction,21 yet other studies have similarly reviewed the literature to devise a standardized protocol and have drawn different conclusions, including that about the timing of these activities.19,31
In our increasingly cost-conscious environment and with emerging evidence that unsupervised home therapy may be as effective as supervised rehabilitation,6,9,10,15,16,25,30 patients are likely to play an increasingly proactive and independent role in their recovery from surgery. As such, it is vital that patients be given clear and appropriate direction regarding the components and timing of their rehabilitation. Ideally, these recommendations would be evidence based and standardized across different centers, as variability in protocols can lead to confusion on the part of both therapists and patients. Indeed, a prior study of ACL rehabilitation protocols found that there was high variability in the composition and timing of rehabilitation components and that many protocols recommended modalities that were not evidence based.18 Furthermore, many rehabilitation protocols are not based on evaluation-based guidelines, which may be more appropriate than strict time-based regimens.19,21
The purpose of this study was to assess the quality and variability of MPFL rehabilitation protocols publicly available on the internet and associated with academic orthopaedic programs in the United States. To our knowledge, this is the first study to review publicly available MPFL protocols, relevant at a time when most patients are technologically literate and may seek out this information on their own. We hypothesized that there is wide variability in the content and timing of specific modalities that are recommended, which may affect our ability to draw comparisons across the literature and lead to suboptimal patient outcomes.
Methods
Rehabilitation protocols from US academic orthopaedic programs for MPFL reconstruction were reviewed. To eliminate search bias, a list of academic programs that participate in the Residency Match was obtained from the Electronic Residency Application Service (ERAS). Two study authors (A.C.L., M.E.S.) conducted searches to obtain publicly available MPFL reconstruction rehabilitation protocols from each of these programs. The search was threefold: first, the program’s website was identified and searched; second, a web-based search was performed to identify MPFL rehabilitation protocols affiliated with any of these programs; third, the name of each orthopaedic surgeon affiliated with an institution plus the phrase “MPFL reconstruction rehabilitation protocol” was searched. Adult MPFL reconstruction protocols were included from ERAS orthopaedic academic centers with a residency program, as were pediatric MPFL reconstruction protocols from ERAS orthopaedic centers with a pediatric orthopaedic fellowship program. Protocols from non-ERAS programs, those lacking phases of rehabilitation, and protocols for MPFL reconstruction with concomitant tibial tubercle osteotomy were excluded.
Protocols that met inclusion criteria were reviewed by the same 2 study authors. Any differences in analysis were discussed and jointly adjudicated on. All rehabilitation components in each protocol were recorded and grouped into the categories found in Table 1: prehabilitation, postoperative adjunct therapy, early motion and weightbearing, strengthening, proprioception, functional testing, and return to activity or sport. The primary outcome was inclusion of these identified components in the published rehabilitation protocol. The secondary outcome was the initiation of a specific modality at a specified time point. For each rehabilitation activity, the proportion of protocols that included the component was calculated. Additionally, the time of initiation (median and range) for each component was determined across the included protocols. All activities endorsed by more than 1 protocol were included in the analysis.
Table 1.
Rehabilitation Protocol Components
| Protocol Structure | Phases, Phase Goals, and Precautions |
|---|---|
| Prehabilitation | Range of motion, quadriceps strengthening |
| Postoperative adjunct therapy | Continuous passive motion, brace use, neuromuscular electric stimulation, ice, patellar glide |
| Early motion and weightbearing | Flexion/extension goals, weightbearing parameters, hamstrings stretch, calf stretch, quadriceps stretch |
| Strengthening | Straight-legged raise, resisted straight-legged raise, quadriceps sets/isometrics, ankle pumps, toe raise, minisquats, squats, hamstring curls, resisted hamstring curls, leg press, step-up/down, wall sits, single-legged squats, resisted knee extension, walking lunges, lunges, heel slides, bridging with ball squeeze |
| Proprioception | Weight shifting, 1-legged balance, balance board, ball toss, perturbation, TheraBand control, mini-trampoline balance, cone touch |
| Functional testing | Single-hop test, 3-hop test, isokinetic quadriceps strength, isokinetic hamstring strength, quadriceps/hamstring strength ratio, or nonspecific functional test |
| Return to activity/sport | Treadmill, stationary bike, normal gait, elliptical, stair climber, swimming, backward running, straight-line running/jogging, jumping/plyometrics, cutting/ pivoting, agility (carioca, side shuffle), sport-specific drills, return to practice/sport |
Results
The search process is demonstrated in Figure 1. A total of 155 programs were in the ERAS database and were searched. Thirty programs were found to have protocols for MPFL reconstruction; of these, 4 protocols were excluded for lacking recommendations regarding the timing of initiation of certain components, and 2 programs were excluded because they were targeted toward patients undergoing concomitant tibial tubercle osteotomy procedures. Two programs had more than 1 protocol available online. A total of 27 protocols were therefore assessed.
Figure 1.

Flowchart demonstrating search process. ERAS, Electronic Residency Application Service; MPFL, medial patellofemoral ligament.
Prehabilitation
None of the 27 protocols offered preoperative instructions, including preparation guidelines, strength exercises, proprioception exercises, or ROM activities.
Postoperative Adjunct Therapy
Six types of postoperative adjunct therapies were evaluated and are demonstrated in Figure 2. These included immediate postoperative knee bracing, neuromuscular electrical stimulation, patellar glide/mobilization, ice and compression, routine postrecovery functional bracing, and continuous passive motion. The majority of protocols (25 of 27; 93%) recommended immediate postoperative knee bracing. Of these, 50% discontinued bracing at 6 weeks (range, 2-9 weeks). Fourteen protocols (52%) endorsed neuromuscular electrical stimulation; 9 (33%), ice as needed; 7 (26%), routine postrecovery patellar stabilization bracing; and 4 (15%), continuous passive motion.
Figure 2.

Postoperative adjunct therapy—the majority of protocols recommended immediate postoperative knee bracing. CPM, continuous passive motion; NMES, neuromuscular electrical stimulation; postop, postoperative.
ROM and Weightbearing
Out of 27 protocols, 26 (96%) offered knee flexion and extension ROM guidelines, which are shown in Figure 3. Only 11 of the 27 protocols (41%) recommended that the knee remain locked in full extension at any point after surgery. Fifty percent of protocols recommended that 90° of flexion be attempted by 2 weeks (range, 0-6 weeks). Fifty percent of protocols recommended that 110° to 120° of flexion be attempted by 3 weeks (range, 2-10 weeks). Fifty percent of protocols recommended that full flexion be attempted by 6 weeks (range, 4-12 weeks).
Figure 3.

Range of motion—a minority of protocols recommended that the knee remain locked in full extension at any point after surgery. There was significant variability in target achievement dates for 90°, 110°/120°, and full flexion. Medians are shown as vertical black lines, while ranges are shown as gray bars.
Weightbearing recommendations are demonstrated in Figure 4. Overall, 24 protocols (89%) made timing recommendations about postoperative weightbearing. Of these, 19 mentioned goals specific to partial weightbearing, with a majority allowing partial weightbearing immediately postoperatively (range, 0-1 week). Of the 27 protocols, 18 (67%) mentioned goals specific to full weightbearing, with 50% recommending that full weightbearing be attempted by 4 weeks postoperatively (range, 0-8 weeks). Five protocols that advised on partial weightbearing did not make any recommendation for the timing of initiation of full weightbearing, while 1 protocol advocated immediate full weightbearing without a partial weightbearing period.
Figure 4.
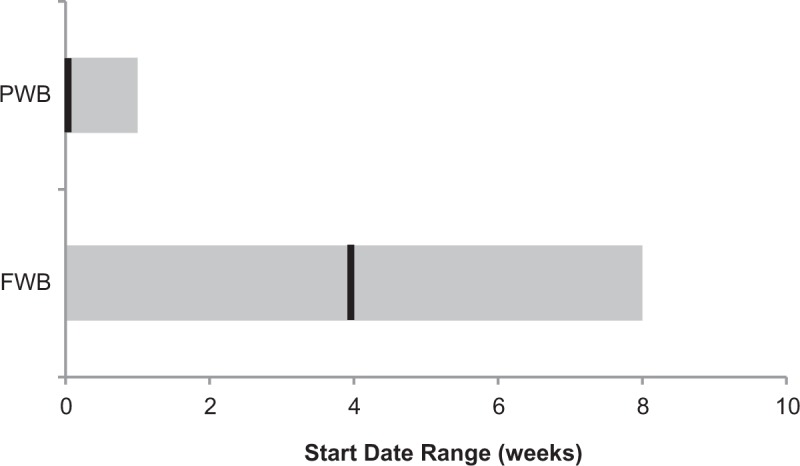
Weightbearing—no protocol suggested a period of nonweightbearing postoperatively. There was significant variability in target achievement dates for full weightbearing activity; black lines indicate medians, with ranges shown in gray. FWB, full weightbearing; PWB, partial weightbearing.
Strengthening
Seventeen strengthening exercises were assessed across all protocols and are shown in Figure 5. Each protocol included a mean of 8.0 (range, 2-14) of the assessed strengthening exercises. The most common strengthening exercises endorsed were quadriceps sets (89%), straight-legged raise (85%), and leg press (81%). Out of the 17 exercises, 11 were endorsed by <50% of protocols.
Figure 5.

Strengthening—quadriceps sets/isometrics, single-legged raise, leg press, and step-up/step-downs were the most common strengthening exercises prescribed. There were wide ranges in recommended initiation time points of the most commonly prescribed strength exercises; black lines indicate medians, with ranges shown in gray. quad, quadriceps; SLR, straight-legged raise.
Regarding timing to initiation, the earliest exercises that were recommended were heel slides (median, 0 weeks; range, 0-1 weeks), quadriceps sets/isometrics (median, 0 weeks; range, 0-2 weeks), ankle pumps (median, 0 weeks; range, 0-2 weeks), and straight-legged raise (median, 0 weeks; range, 0-6 weeks). Several exercises were recommended to be reserved for later in the postoperative course. These include hamstrings curls (median, 8 weeks; range, 2-11 weeks), lunges (median, 6 weeks; range, 4-12 weeks), and walking lunges (median, 6 weeks; range, 6-6 weeks). The exercises with the greatest variation in recommended time to initiation were single-legged squats (median, 6 weeks; range, 4-19 weeks) and leg press (median, 6 weeks; range, 2-16 weeks).
Proprioception
Seven proprioception exercises were assessed across all protocols and are demonstrated in Figure 6. Each protocol included a mean of 1.6 of the assessed proprioception exercises (range, 0-4). None of the exercises were recommended by >50% of the protocols, with the most common proprioception exercises endorsed being balance board (41%), single-legged balance (41%), and TheraBand control (33%). Three of the 7 exercises were recommended in <20% of the protocols (weight shifting, mini-trampoline balance, and perturbation).
Figure 6.

Proprioception: balance board was the sole proprioception exercise recommended by >40% of protocols. There was wide variability in the recommended time to initiate various proprioception activities; black lines indicate medians, with ranges shown in gray.
In terms of timing to initiation, the earliest exercises that were recommended were TheraBand control (median, 1 week; range, 0-6 weeks), mini-trampoline balance (median, 4 weeks; no variation among protocols), and weight shifting (median, 4 weeks; range, 0-4 weeks). Exercises that were recommended later in the postoperative course included 1-legged balance (median, 6 weeks; range, 2-9 weeks), ball toss (median, 6 weeks; range, 4-6 weeks), and perturbation (12 weeks, recommended by 1 protocol).
Functional Testing
Five functional tests were identified across the protocols (Figure 7). None of these components were included in >35% of the protocols. Two functional tests were recommended at a median 12 weeks postoperatively, including isokinetic quadriceps strength (range, 12-19 weeks) and hamstring strength (range, 12-17 weeks). Three protocols recommended evaluation of quadriceps: hamstrings isokinetic strength ratio at a median 13 weeks (range, 12-16 weeks), the single hop test at a median 14 weeks (range, 12-19 weeks), and the 3 hop test at a median 16 weeks (range, 16-17 weeks).
Figure 7.

Functional testing: the single-hop test was the most commonly prescribed functional test. There was wide variability in target achievement dates for all activities surveyed; black lines indicate medians, with ranges shown in gray. Quad, quadriceps.
Return to Activity/Sport
Of the 27 studied protocols, 23 (85%) mentioned return to sport or play as a goal of MPFL reconstruction rehabilitation (Figure 8). Fifty percent of protocols recommended that patients return to sport or play by 17 weeks, with substantial variability across protocols (range, 12-26 weeks).
Figure 8.

Return to activity/sport: there was a wide range of activities recommended across protocols; stationary bike the most commonly suggested. There was significant variability in target achievement dates for all activities surveyed; black lines indicate medians, with ranges shown in gray.
Other than return to sport, 11 other rehabilitation activities were analyzed. Of these activities, the 3 most commonly reported were stationary bike (85%), straight-line running or jogging (74%), and agility exercises (63%). The activities recommended early in the recovery course included stationary bike (median, 4 weeks; range, 0-12 weeks), elliptical (median, 6 weeks; range, 6-13 weeks), stair climber (median, 8 weeks; range, 2-13 weeks), and treadmill (median, 7 weeks; range, 2-16 weeks). Those activities recommended later in the recovery course included agility exercises (median, 12.5 weeks; range, 10-19 weeks), jumping/plyometrics (median, 13 weeks; range, 6-17 weeks), sport-specific drills (median, 13 weeks; range, 10-19 weeks), and cutting/pivoting (median, 16 weeks; range, 12-19 weeks).
Discussion
Overall, there is a dearth of publicly available information on rehabilitation following MPFL reconstruction, with only 24 of 155 (17%) of ERAS programs providing recommendations on specific modalities and timing in adults undergoing this procedure. Among the programs that provide recommendations, there exists wide variation with respect to postoperative adjunct therapy, ROM and weightbearing, strengthening, proprioception, functional testing, and return to sport guidelines and time points. All protocols lacked specific instructions for each exercise or activity that they recommended.
Wide variability was found in both weightbearing and ROM recommendations, 2 of the most basic elements of postoperative protocol. Eighteen protocols made recommendations for full weightbearing at a median 4 weeks, ranging from 0 to 8 weeks postoperatively. Of 27 protocols, 9 did not mention the use of assistive devices such as crutches in the rehabilitation plan. Regarding ROM, more conservative protocols recommended that patients maintain the knee locked in full extension for a period of time postoperatively and progress to full flexion at up to 12 weeks, while other protocols made more aggressive recommendations, with immediate 90° of knee flexion and full flexion at just 4 weeks postoperatively.
In addition, our study demonstrated substantial variability in recommendations regarding return to play. Of the 27 protocols, 23 (85%) noted return to sport/activity at a median 17 weeks, with wide variation (range, 12-26 weeks) across studies. A recent systematic review by Zaman et al32 analyzed return to play after MPFL reconstruction, reporting that while the majority (96.2%) of studies included criteria to determine return to play, 34% provided no specific timeline to determine the appropriate initiation of sport. Similarly, while the majority of protocols in our study listed return to sport as a major goal of rehabilitation postoperatively, relatively few included functional testing as a part of the protocol. In the ACL rehabilitation literature, functional tests—especially the single- and 3-hop tests—are often used to determine readiness to return to play.2,22,23 This lack of guidance and specific criteria for determining the timing of return to activity could lead to inappropriate return to sport, thus increasing the chance for reinjury or suboptimal outcomes.
Compared with a study by Makhni et al18 analyzing rehabilitation protocols after ACL reconstruction, in which 42 of the ERAS programs were found to provide rehabilitation protocols, there were fewer ERAS programs providing MPFL rehabilitation protocols. This difference is likely due to the lower prevalence and more recent emergence of MPFL reconstruction as compared with ACL reconstruction.6 One discrepancy in these studies is that Makhni et al18 reported that 31% of the ACL reconstruction rehabilitation protocols included a prehabilitation component, while no MPFL protocols in our study recommended a prehabilitation period. While the ACL literature is replete with evidence, including a randomized controlled trial demonstrating improved outcomes associated with prehabilitation,28 the MPFL literature lacks high-quality data on the subject. Perhaps the lack of prehabilitation recommendations in MPFL reconstruction is due to patients with patellofemoral instability not tolerating a presurgical program to the same degree as patients undergoing ACL reconstruction.
The variations in protocol recommendations in the MPFL literature likely stem from our poor understanding of best practices after MPFL reconstruction, with many components of MPFL rehabilitation being adapted from practices in the ACL reconstruction literature. Indeed, outcome data after MPFL reconstruction with specific rehabilitation protocols are scarce.
In a case series of 20 patients undergoing MPFL reconstruction, Ahmad et al1 instructed patients to begin passive and active ROM exercises 2 weeks postoperatively, progressing to quadriceps, hamstrings, and hip muscle strengthening exercises at 6 weeks, with running and agility training at 12 weeks. These authors found that International Knee Documentation Committee, Kujala, Lysholm, and Tegner scores improved significantly after surgery. Similarly, in a case series of 34 patients undergoing MPFL reconstruction, Steiner et al29 instructed patients to use a continuous passive motion machine and allowed full weightbearing and active exercises, although the specific timing for these activities postoperatively was not specified. At follow-up, 97% of patients were satisfied with their outcome; 85% had a good or excellent Kujala score; and 91% had a good or excellent Lysholm score. While there is little guidance, several groups have attempted to provide recommendations on MPFL-specific activities postoperatively. One such review by the Musculoskeletal Institute at the Johns Hopkins Hospital advocated the use of a locked brace for the first 2 weeks, with progression to full weightbearing by the end of 2 weeks, normal gait between 2 and 6 weeks, full ROM with sport-specific training between 6 and 12 weeks, and return to sport at 12 or more weeks after passing a hop test.21 Others have drawn different conclusions. Manske and Prohaska,19 for example, suggested a full return to sport between 17 and 21 weeks, while Vitale et al31 recommended 19 to 36 weeks depending on the patient’s recovery.
At our institution, we have a formalized 5-phase MPFL rehabilitation protocol that is provided to our patients and therapists. Each phase contains phase-specific goals, precautions, treatment recommendations, and minimum criteria for advancement to the subsequent phase. These include specific prescriptions about ROM, weightbearing, strengthening, adjunct treatments, and functional activities. Overall, the phases progress as follows:
from a protection phase, with ambulation in an extension brace, preventing quadriceps inhibition and maintaining ROM;
to a gait phase, with normal gait, postural stability/alignment, neuromuscular control, and achievement of full ROM;
to a strengthening phase, identifying and rectifying muscle/soft tissue imbalances and focusing on functional progression;
to an advanced strengthening and function phase, with a focus on core stability, cross-training, and plyometric exercises; and
to a return-to-play phase, with recommendations on advanced plyometrics, cutting/deceleration training, and cardiovascular fitness.
Given the trend toward independent rehabilitation, a goal in each phase is the ability for patients to perform these activities as part of a home exercise program. Regarding the time to return, in our experience patients at 17 weeks postoperatively do not have the quadriceps strength to do plyometrics, and return to early activities tends to require at least 6 months of rehabilitation. Additionally, the lack of representation of functional tests in the protocols included in this study reflects a general reliance on time-based over evaluation-based guidelines; of the 27 protocols reviewed, 20 (74%) used evaluation-based guidelines. While general timelines can be helpful to provide a sense of overall progression, rehabilitation cannot apply a one-size-fits-all model, as age, baseline health, occupation, and level of sport may all influence a patient’s rehabilitation.
Finally, in addition to the wide variability observed across the studied protocols, all guidelines lacked specific instructions on how to perform each exercise or recommended activity, and many protocols used nonstandard abbreviations to refer to specific exercises, without defining these abbreviations. Patients often do not possess the requisite medical literacy to understand or comply with the recommendations, which can cause confusion. In a study of taped clinical encounters, Castro et al7 demonstrated that medical jargon was used 37% of the time, and they found low rates of patient comprehension. Furthermore, poor comprehension of a rehabilitation protocol may lead to poor outcomes. In their study of ACL reconstruction, Treacy et al30 found that patients who were noncompliant with their rehabilitation regimen had worse outcomes as measured by Lysholm score, patient satisfaction, and return to preoperative activity, when compared with compliant patients. It is likely that the protocols lacked patient-friendly instructions because they are intended for physical therapists or other professionals. However, in this era of increasing cost-consciousness in health care4,5,26 and mounting published literature on the efficacy of home-based regimens in many orthopaedic injuries,6,7,10,18,24,25,27 we are likely to witness a trend away from professional physical therapy sessions and toward more independent rehabilitation. Perhaps most relevant for patients undergoing MPFL reconstruction are the several studies indicating no clear benefit of supervised versus home-based therapy after ACL reconstruction.15,16,25,30
Acknowledging these realities, the protocol provided by our institution focuses on the teaching of home exercise programs to empower patients to be active participants in their recovery. While patients are able to perform many of these activities on their own, several advanced exercises (eg, plyometrics, isokinetic testing, cross-training) require the assistance of a professional. Further research is needed to determine which of these more resource-intensive exercises is most beneficial to the patient recovering from MPFL reconstruction.
There are several limitations to our study. First, our search was confined to the publicly available MPFL reconstruction rehabilitation protocols from ERAS institutions. As a result, this review likely represents a minority of the MPFL rehabilitation protocols available, as non-ERAS protocols and protocols not freely available on the internet were not searched. However, this methodology was selected as a way to focus on the highest-quality protocols and minimize selection bias. Additionally, without outcome data available to correspond with each analyzed protocol, this study is limited in its ability to appraise the effectiveness of each regimen. Finally, as some of the protocols identified were more than 5 years old, certain protocols may have been updated since that time, but these updates may not be publicly available.
Conclusion
There are relatively few publicly available MPFL reconstruction rehabilitation protocols from US academic institutions. Despite recent efforts to analyze rehabilitation strategies after MPFL reconstruction, there is little consensus, with substantial variability among current protocols regarding types of activities and timing of initiation in the postoperative period. Recommendations for return to sport ranged from 12 to 26 weeks, with a median of 17 weeks. This variability can lead to suboptimal patient outcomes and make it difficult to compare across interventions and studies. Further research needs to be performed to identify the most beneficial rehabilitation activities and standardize postoperative protocols.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: S.M.S. has received consulting fees from Medical Device Business Services and Pfizer and has received hospitality payments from Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
- 1. Ahmad CS, Brown GD, Shubin Stein BE. The docking technique for medial patellofemoral ligament reconstruction: surgical technique and clinical outcome. Am J Sports Med. 2009;37(10):2021–2027. [DOI] [PubMed] [Google Scholar]
- 2. Ardern CL, Webster KE, Taylor NF, Feller JA. Return to sport following anterior cruciate ligament reconstruction surgery: a systematic review and meta-analysis of the state of play. Br J Sports Med. 2011;45(7):596–606. [DOI] [PubMed] [Google Scholar]
- 3. Baltaci G, Harput G, Haksever B, Ulusoy B, Ozer H. Comparison between Nintendo Wii Fit and conventional rehabilitation on functional performance outcomes after hamstring anterior cruciate ligament reconstruction: prospective, randomized, controlled, double-blind clinical trial. Knee Surg Sports Traumatol Arthrosc. 2013;21(4):880–887. [DOI] [PubMed] [Google Scholar]
- 4. Bozic KJ. Improving value in healthcare. Clin Orthop Relat Res. 2013;471(2):368–370. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Bozic KJ. Value-based healthcare and orthopaedic surgery. Clin Orthop Relat Res. 2012;470(4):1004–1005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Büker N, Akkaya S, Akkaya N, et al. Comparison of effects of supervised physiotherapy and a standardized home program on functional status in patients with total knee arthroplasty: a prospective study. J Phys Ther Sci. 2014;26(10):1531–1536. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Castro CM, Wilson C, Wang F, Schillinger D. Babel babble: physicians’ use of unclarified medical jargon with patients. Am J Health Behav. 2007;31(suppl 1):S85–S95. [DOI] [PubMed] [Google Scholar]
- 8. Christanell F, Hoser C, Huber R, Fink C, Luomajoki H. The influence of electromyographic biofeedback therapy on knee extension following anterior cruciate ligament reconstruction: a randomized controlled trial. Sports Med Arthrosc Rehabil Ther Technol. 2012;4(1):41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Coppola SM, Collins SM. Is physical therapy more beneficial than unsupervised home exercise in treatment of post surgical knee disorders? A systematic review. Knee. 2009;16(3):171–175. [DOI] [PubMed] [Google Scholar]
- 10. Coulter C, Perriman DM, Neeman TM, Smith PN, Scarvell JM. Supervised or unsupervised rehabilitation after total hip replacement provides similar improvements for patients: a randomized controlled trial. Arch Phys Med Rehabil. 2017;98(11):2253–2264. [DOI] [PubMed] [Google Scholar]
- 11. De Carlo MS, Sell KE. The effects of the number and frequency of physical therapy treatments on selected outcomes of treatment in patients with anterior cruciate ligament reconstruction. J Orthop Sports Phys Ther. 1997;26(6):332–339. [DOI] [PubMed] [Google Scholar]
- 12. Feller JA, Webster KE, Taylor NF, Payne R, Pizzari T. Effect of physiotherapy attendance on outcome after anterior cruciate ligament reconstruction: a pilot study. Br J Sports Med. 2004;38(1):74–77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Fu CLA, Yung SHP, Law KYB, et al. The effect of early whole-body vibration therapy on neuromuscular control after anterior cruciate ligament reconstruction: a randomized controlled trial. Am J Sports Med. 2013;41(4):804–814. [DOI] [PubMed] [Google Scholar]
- 14. Fukuda TY, Fingerhut D, Moreira VC, et al. Open kinetic chain exercises in a restricted range of motion after anterior cruciate ligament reconstruction: a randomized controlled clinical trial. Am J Sports Med. 2013;41(4):788–794. [DOI] [PubMed] [Google Scholar]
- 15. Grant JA, Mohtadi NG, Maitland ME. Comparison of home versus physical therapy-supervised rehabilitation programs after anterior cruciate ligament reconstruction: a randomized clinical trial. J Orthop Sports Phys Ther. 2006;36(4):251. [DOI] [PubMed] [Google Scholar]
- 16. Grant JA, Mohtadi NGH. Two- to 4-year follow-up to a comparison of home versus physical therapy-supervised rehabilitation programs after anterior cruciate ligament reconstruction. Am J Sports Med. 2010;38(7):1389–1394. [DOI] [PubMed] [Google Scholar]
- 17. Hohmann E, Tetsworth K, Bryant A. Physiotherapy-guided versus home-based, unsupervised rehabilitation in isolated anterior cruciate injuries following surgical reconstruction. Knee Surg Sports Traumatol Arthrosc. 2011;19(7):1158–1167. [DOI] [PubMed] [Google Scholar]
- 18. Makhni EC, Crump EK, Steinhaus ME, et al. Quality and variability of online available physical therapy protocols from academic orthopaedic surgery programs for anterior cruciate ligament reconstruction. Arthroscopy. 2016;32(8):1612–1621. [DOI] [PubMed] [Google Scholar]
- 19. Manske RC, Prohaska D. Rehabilitation following medial patellofemoral ligament reconstruction for patellar instability. Int J Sports Phys Ther. 2017;12(3):494–511. [PMC free article] [PubMed] [Google Scholar]
- 20. Mayr HO, Stüeken P, Münch E-O, et al. Brace or no-brace after ACL graft? Four-year results of a prospective clinical trial. Knee Surg Sports Traumatol Arthrosc. 2014;22(5):1156–1162. [DOI] [PubMed] [Google Scholar]
- 21. McGee TG, Cosgarea AJ, McLaughlin K, Tanaka M, Johnson K. Rehabilitation after medial patellofemoral ligament reconstruction. Sports Med Arthrosc. 2017;25(2):105–113. [DOI] [PubMed] [Google Scholar]
- 22. Myer GD, Paterno MV, Ford KR, Quatman CE, Hewett TE. Rehabilitation after anterior cruciate ligament reconstruction: criteria-based progression through the return-to-sport phase. J Orthop Sports Phys Ther. 2006;36(6):385–402. [DOI] [PubMed] [Google Scholar]
- 23. Nwachukwu BU, Schairer WW, Bernstein JL, Dodwell ER, Marx RG, Allen AA. Cost-effectiveness analyses in orthopaedic sports medicine: a systematic review. Am J Sports Med. 2015;43(6):1530–1537. [DOI] [PubMed] [Google Scholar]
- 24. Ohinmaa A, Vuolio S, Haukipuro K, Winblad I. A cost-minimization analysis of orthopaedic consultations using videoconferencing in comparison with conventional consulting. J Telemed Telecare. 2002;8(5):283–289. [DOI] [PubMed] [Google Scholar]
- 25. Papalia R, Vasta S, Tecame A, D’Adamio S, Maffulli N, Denaro V. Home-based vs supervised rehabilitation programs following knee surgery: a systematic review. Br Med Bull. 2013;108:55–72. [DOI] [PubMed] [Google Scholar]
- 26. Porter ME. A strategy for health care reform—toward a value-based system. N Engl J Med. 2009;361(2):109–112. [DOI] [PubMed] [Google Scholar]
- 27. Porter ME. What is value in health care? N Engl J Med. 2010;363(26):2477–2481. [DOI] [PubMed] [Google Scholar]
- 28. Shaarani SR, O’Hare C, Quinn A, Moyna N, Moran R, O’Byrne JM. Effect of prehabilitation on the outcome of anterior cruciate ligament reconstruction. Am J Sports Med. 2013;41(9):2117–2127. [DOI] [PubMed] [Google Scholar]
- 29. Steiner TM, Torga-Spak R, Teitge RA. Medial patellofemoral ligament reconstruction in patients with lateral patellar instability and trochlear dysplasia. Am J Sports Med. 2006;34(8):1254–1261. [DOI] [PubMed] [Google Scholar]
- 30. Treacy SH, Barron OA, Brunet ME, Barrack RL. Assessing the need for extensive supervised rehabilitation following arthroscopic ACL reconstruction. Am J Orthop. 1997;26(1):25–29. [PubMed] [Google Scholar]
- 31. Vitale TE, Mooney B, Vitale A, Apergis D, Wirth S, Grossman MG. Physical therapy intervention for medial patellofemoral ligament reconstruction after repeated lateral patellar subluxation/dislocation. Int J Sports Phys Ther. 2016;11(3):423–435. [PMC free article] [PubMed] [Google Scholar]
- 32. Zaman S, White A, Shi WJ, Freedman KB, Dodson CC. Return-to-play guidelines after medial patellofemoral ligament surgery for recurrent patellar instability: a systematic review. Am J Sports Med. 2018;46(10):2530–2539. [DOI] [PubMed] [Google Scholar]