

Dear Editor,
A 40-year-old female modern dancer presented with pain and tenderness at the lateral aspect of the left hip for 6 months. The pain was initially noticed during her performance and then aggravated, making her difficult to perform certain dancing postures. During the physical examination, a specific tender point was palpated on the left lateral iliac crest (IC) [Figure 1a]. The ultrasound (US) examination revealed focal swelling and hypoechoic at the proximal gluteus medius (GMed) attachment on the IC [Figure 1b and c]. Proximal GMed tendinopathy was impressed. US-guided percutaneous needle tenotomy (PNT) and injection with hypertonic dextrose (prolotherapy) were performed on the lesion for two times with a 1-month interval, and the patient reported limited improvement. One month after the second treatment, another US-guided PNT and injection of platelet-rich plasma (PRP) were performed [Figure 1d], and she finally had significant symptom relief.
Figure 1.
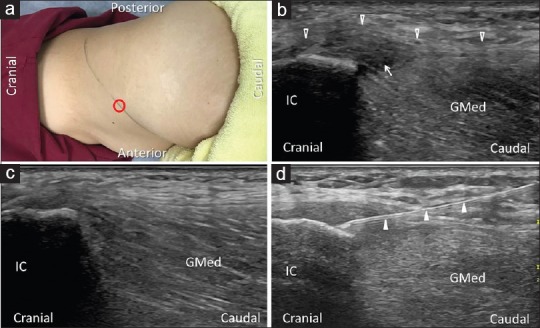
(a) The tender point (red circle) on the patient's left iliac crest (dark line). (b) Longitudinal ultrasound image of the abnormal side of proximal gluteus medius tendon (arrow) at the attachment on the iliac crest, with the comparison of the normal side (c). (d) Percutaneous needle tenotomy of proximal gluteus medius tendinopathy. Void arrowhead: gluteal aponeurotic fascia; white arrowhead: needle shaft
While disorders of the GMed tendon more commonly occur at the distal insertion on the greater trochanter, especially the anterior band inserting on the lateral facet,[1] our case presented with an uncommon GMed tendinopathy involving the proximal attachment on the IC. Through literature review, we only found one study reporting the diagnosis of proximal GMed tendinopathy.[2] Several studies had reported similar pathologies and image findings on the outer lip of IC, including the diagnosis of proximal iliotibial band (ITB) enthesopathy,[3] proximal tensor fascia lata tendinopathy,[4] and gluteal aponeurotic fascia injury.[5] The tensor fascia lata originates from the anterior superior iliac spine and the anterior outer lip of the IC, and the gluteal aponeurotic fascia originates from the posterior outer lip of the IC. The tensor fascia lata contributes fibrous components to the ITB together with the gluteus maximus muscle. The gluteal aponeurotic fascia covers the GMed muscle, partially serving as the flat tendon of the origin of GMed muscle.[5] Diseases of these closely related structures, although not prevalent, are usually overlooked and misdiagnosed with more common lateral hip pathologies, such as hip arthritis and tendon/bursa problems around the greater trochanter.[5]
Tenotomy is an effective way to treat recalcitrant tendinopathy, which involves multiple needle passages into the diseased tendon, causing local trauma and stimulating the degenerative tendon to regenerate.[4] The augmentation with prolotherapy and PRP are both aimed to hasten the natural healing process. PRP provided faster improvement in our case. Unlike the biologic effect induced by the injection of hypertonic dextrose, the therapeutic effect of PRP is more likely to be mediated by delivering high concentration of growth factors to the lesion.[2] Further studies are needed to compare the therapeutic effect of PNT alone and the combination of various injection therapies.
In conclusion, the proximal GMed tendinopathy should be considered in the differential diagnosis in patients with lateral hip pain, and US-guided tenotomy with PRP can be an effective treatment for recalcitrant cases.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Hoffman DF, Smith J. Sonoanatomy and pathology of the posterior band of the gluteus medius tendon. J Ultrasound Med. 2017;36:389–99. doi: 10.7863/ultra.16.03073. [DOI] [PubMed] [Google Scholar]
- 2.Housner JA, Jacobson JA, Misko R. Sonographically guided percutaneous needle tenotomy for the treatment of chronic tendinosis. J Ultrasound Med. 2009;28:1187–92. doi: 10.7863/jum.2009.28.9.1187. [DOI] [PubMed] [Google Scholar]
- 3.Posadzy-Dziedzic M, Vanhoenacker FM. Proximal iliotibial band enthesopathy. JBR-BTR. 2012;95:369. doi: 10.5334/jbr-btr.728. [DOI] [PubMed] [Google Scholar]
- 4.Bradberry DM, Sussman WI, Mautner KR. Ultrasound-guided percutaneous needle tenotomy for chronic tensor fascia lata tendinopathy: A Case series and description of sonographic findings. PM R. 2018 doi: 10.1016/j.pmrj.2018.01.009. pii: S1934-1482(17)30534-8. [DOI] [PubMed] [Google Scholar]
- 5.Huang BK, Campos JC, Michael Peschka PG, Pretterklieber ML, Skaf AY, Chung CB, et al. Injury of the gluteal aponeurotic fascia and proximal iliotibial band: Anatomy, pathologic conditions, and MR imaging. Radiographics. 2013;33:1437–52. doi: 10.1148/rg.335125171. [DOI] [PubMed] [Google Scholar]