

ABSTRACT
The objective of this systematic review was to survey the current scientific knowledge regarding the state of somatic health among the Indigenous Sami people in Norway, Finland, Sweden and the Kola Peninsula in Russia; and assess the quality of the identified studies. A systematic search in the databases Pubmed, EBSCOhost (AMED, Medline, Cinahl) and Svemed was conducted from January 2000, through December 2017. This systematic search identified 399 articles. After screening abstracts, 93 articles were reviewed in full text, 32 of which met the inclusion criteria. The scientific quality of the evidence was rated according to the Newcastle–Ottawa scale. Based on the studies with moderate to high scientific quality, there is evidence for stating that the majority of the Sami included in this review experience good health. Mortality and life expectancy are similar, with only minor differences, to those of a non-Sami population. The cancer risk rate among Sami was lower than that of the general population of Norway, Sweden and Finland. Self-reported myocardial infarction prevalence was similar between Sami and non-Sami, but Angina pectoris was more prevalent among Sami. In Sweden, cardiovascular disease rates were similar between Sami and non-Sami. Musculoskeletal pain symptoms are common among the Sami population, as are obesity and overweight. To conclude, there are knowledge gaps in regard to the somatic health situation of the Indigenous Sami in the circumpolar area, especially in Russia, Finland and Sweden; as current knowledge is mainly based on publications from the SAMINOR study in Norway. No study obtained the highest quality score, suggesting a need to implement longitudinal prospective studies.
KEYWORDS: Indigenous, Sami, health, systematic review, Newcastle-Ottawa scale
Introduction
A review of Sami health research from 2011 stated that “in comparison with other Indigenous People in the circumpolar region, the health and living conditions are exceptionally good” [1]. Nevertheless, over recent years it has become clear that there are pronounced challenges and threats to Sami people and their health. These threats have been hypothesized as connected to the cumulative effects of resource exploitation, climate change and ongoing conflicts with the majority society. These threats can be found among most Indigenous Peoples [2,3]. The first global overview of Indigenous Peoples’ health and wellbeing concluded that Indigenous peoples’ health and social outcomes were poorer than those of the majority populations living in the same countries [4].
For the Indigenous Sami people, living in northern Norway, Sweden, Finland and Russia, there are difficulties in obtaining a coherent overview of their health situation. These countries lack official statistics that include ethnicity. One of the recurring themes in the literature pertaining to Sami health is the uncertainty in reliable, official health statistics. This uncertainty has been addressed by several reports and studies [5,6]. However, a population-based study of health and living conditions in northern Norway [7,8], building on self-determination of ethnic origins, has increased the knowledge regarding the Sami people´s health situation in Norway. Comprehensive scientific knowledge on the Sami people’s somatic health situation in the other countries they inhabit is fractional and partially outdated. Mental health issues, on the other hand, have been explored and subjected to literature reviews to a greater extent [2,3].
This is the first systematic review of somatic health among the Indigenous Sami. Systematic reviews are placed on the second highest level of the evidence hierarchy in science (after meta-analyses), and we aim to establish what can be authoritatively stated in regard to the current status of Sami somatic health, in addition to assessing the quality and strength of peer-reviewed articles, published during the 21st century, that focus on somatic health among the Sami People. The Newcastle–Ottawa Scale (NOS) is employed for generating quality assessments [9].
Materials and methods
The review followed the process in accordance with the Preferred Reporting Items for Systematic research and Meta-Analyses (PRISMA) Statement [10].
Search strategy
Three electronic databases were used: EBSCOhost; where the databases AMED, Medline and Cinahl were selected; Pubmed; and Svemed. The search encompassed all articles published in English or Swedish/Norwegian between the dates 2000–01-01 to 2017–12-31. The search term used was “Sami” (or spellings Sámi or Saami), with the specification that Sami should be mentioned in the abstracts. Other inclusion criteria were that the publications had been peer-reviewed, and that the reported results should concern the 21st century.
Publications focusing on mental health, genetics and issues regarding the health-care system/utilisation were excluded, as well as studies not relevant to the aim of this study. Studies and review articles with no clearly defined Sami population, or no outcome measures on wellbeing from a somatic point of view, were also excluded.
Quality assessment
The quality of the included studies was assessed with the Newcastle–Ottawa Scale (NOS) [9], as modified by the authors to suite this review. The studies were each awarded stars, up to a maximum of 8 for cohort studies and case-control studies, respectively. Up to 4 stars could be assigned for selection, 1 star for comparability and up to 3 stars for exposure/outcome. Cross-sectional studies could receive 6 stars at most; up to 3 stars for selection, 1 star for comparability and up to 2 stars for outcome. The quality scores are presented as numbers of the total attainable score for each study. A study receiving a quality score above 50% of the highest possible score was assessed as a study of moderate quality. Only studies receiving the maximum score of eight can be assessed as high-quality.
Study selection and data collection
One of the authors began with an initial screening of titles and abstracts, aiming to exclude studies obviously unrelated to the Sami people. Studies where the word “Sami” was not about the Sami people, instead referred to short names of diseases/studies (acronyms), names of hospitals, first or last names of authors, measurements methods/equipment and analysis methods were thus excluded. After the initial screening, the two authors independently read all the abstracts to identify potentially eligible articles for inclusion in the review. All article abstracts identified by one of the authors were discussed in concert beforehand until consensus and agreement were reached, and the article was retrieved for full-text reading. Full articles were then read independently by the 2 authors. Articles that met the inclusion criteria were included in the review. The authors independently evaluated the quality. Any disagreements between the authors were resolved during discussions that lasted until consensus was reached.
Results
The systematic search of the databases identified 684 potentially eligible articles, of which 52 were identified through Svemed, 311 through Ebsco and 321 through Pubmed, respectively. Three articles were immediately excluded due to their having been published before 2000. After duplicate removals, 399 articles remained. The initial screening excluded 115 articles, leaving 284 abstracts to be screened (Figure 1), during which process a further 191 articles were excluded. 93 articles were then retrieved and reviewed in full-text. Of these, a total of 61 were excluded. These are provided as supplemental material. The main reasons for article exclusions were; data not including twenty-first century, unclear Sami population, no outcome measures (mainly qualitative studies), or study focusing on substance abuse, diet or mental health. The publication countries of the excluded articles are presented in a circle chart, with the majority coming from Norway, following by Sweden, Finland and others. The others include 3 articles each from Russia, Italy and Canada, respectively (Figure 2). Finally, a total of 32 articles met the inclusion criteria and were analysed (Table 1). 16 articles were from Norway, 14 from Sweden and 2 from Finland. The included articles may have also dealt with other issues, but we have selected outcomes that are relevant to our aim. Around half of the included studies were assessed as being of moderate to high quality. None of the reviewed articles obtained the highest score, that is, 8 stars based on the NOS. The quality scores for the included studies range from 0 to 7.
Figure 1.
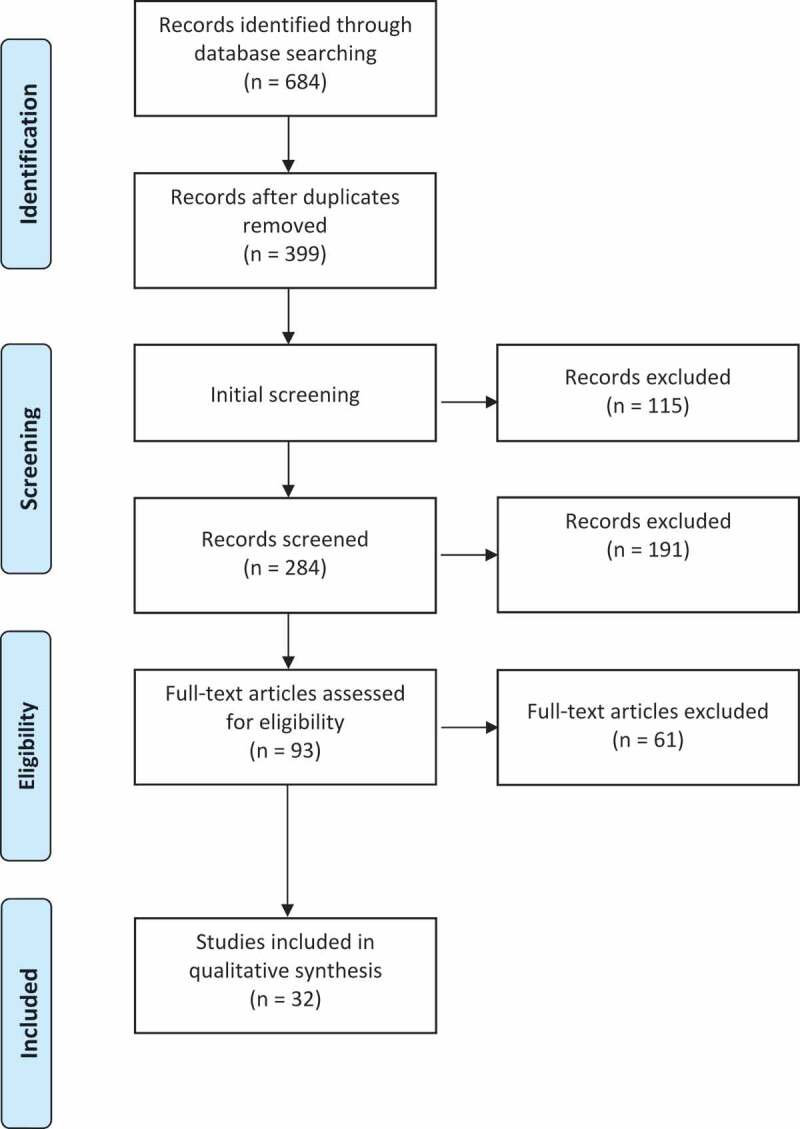
PRISMA flow chart showing numbers of included and excluded studies
Figure 2.
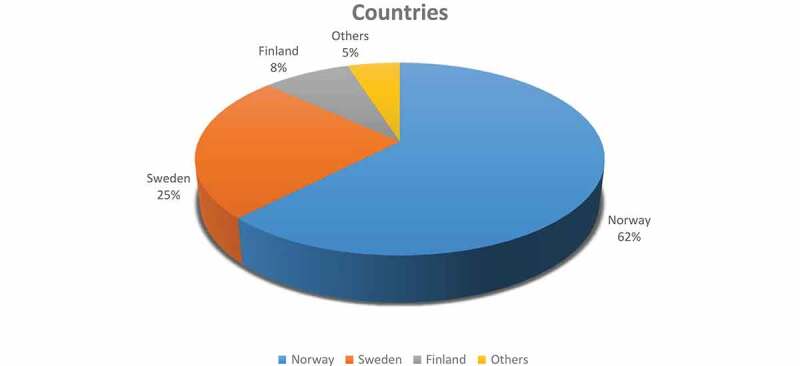
Circle chart of excluded articles, categorised by country
Table 1.
Summary of studies concerning the somatic health of the Sami people included in the review
| Author publication year |
Country/ setting |
Study design | Study population/ response rate |
Subjects(n)/ age |
Outcome measures | Findings | Quality score |
Author conclusions |
Comment |
|---|---|---|---|---|---|---|---|---|---|
| Abrahamsson A et al., 2013 |
Sweden/ Counties of Norrbotten, Jämtland or Stockholm |
Cross-sectional Questionnaire | Sami pop/ 53,4% Non-Sami pop/ 57,7% Reindeer herders/ non- reindeer herders |
n = 613/ mean age 49,9 n = 525/ mean age 48,0 n = 116/ mean age 52,1 n = 493/ mean age 49,3 |
Self-reported health (SRH) Sence of coherence (SOC) |
Reindeer-herding Sami, lower SOC than non-herding Sami. ”Healthy” 68,4% non-herders 62.4% herders 75.9% non-Sami 67.3% Sami Not statistically significant. |
3(6) | Age, health and predictors of SOC are related to the reindeer husbandry life and belonging to their community | Electoral register of the Sami Parliament |
| Ahlm K et al., 2010 |
Sweden | Cohort Register-based |
Members of reindeer-herding Sami families n = 7482 |
n = 158/ mean age 47 |
Unnatural deaths | 37% vehicle accidents whereof 50% were alcohol affected. 23% suicides |
4(8) | Improve safety of transportation and change alcohol behaviour can prevent accidents. | Reindeer-herders/owners from occupational register of Statistics Sweden and national register of reindeer herding enterprises. Spouses and children from the kinship register of Statistics Sweden |
| Bakken K et al., 2006 |
Norway The Saminor 1 study (2003–2004) |
Cross-sectional Questionnaire |
Sami and non-Sami/ 60% |
n = 12 378 36–79 years |
Insomnia | Lower prevalence of insomnia compared to non-Sami | 3(6) | The results may be due to differences in attitudes to sleep as a phenomena among the Sami | Sami language criteria and self-identification |
| Broderstad AR et al., 2011 |
Norway The Saminor 1 study (2003–2004) |
Cross-sectional Questionnaire |
Sami and non-Sami/ 61% |
n = 16 323 36–79 years |
Iron status; serum-ferritin transferrin saturation obesity |
Reindeer pattern; Higher Mean transferrin saturation & s-ferritin More individuals with overweight and obesity. | 4(6) | High levels of s-ferritin may be due to high intake of reindeer meat. Overweight and obesity is associated with s-ferritin levels. |
Sami language criteria and self-identification Article focus on iron stores in relation to dietary patterns; 5 dietary patterns whereof 1 “reindeer pattern” |
| Broderstad AR et al., 2007 |
Norway The Saminor 1 study (2003–2004) |
Cross-sectional Questionnaire |
Sami and non-Sami/ 54,8 % Inland vs coastal |
n = 14 873 36–79 years |
Iron status; serum-ferritin transferrin saturation |
Higher mean s-ferritin and transferrin saturation in inland Sami compared to coastal Sami/non-Sami | 4(6) | Differences in iron levels might be due to nutritional habits. Probably no differences in iron metabolism between Sami and non-Sami. |
Sami language criteria and self-identification |
| Broderstad AR & Melhus M, 2016 | Norway The Saminor 1 study (2003–2004) |
Cross-sectional Questionnaire Non-fasting blood samples Physical tests |
Sami and non-Sami/ 61% |
n = 15 112 36–79 years |
Metabolic syndrome(MetS) Diabetes Mellitus BMI |
High Mets prevalence in both groups. No ethnic differences in diabetes prevalence but in received treatment. Higher mean BMI among Sami. |
4(6) | Culture and linguistic specific preventive actions in the healthcare systems is important to improve health status in the whole population. | Sami language criteria and self-identification Sami affiliation 34% |
| Brustad M et al., 2008 |
Norway The Saminor 1 study (2003–2004) |
Cross-sectional Questionnaire | 24 municipalities in Norway divided into coastal and inland residences 5–10% reported to be Sami in the 1970 Census 61% response rate |
n = 12,811 36–79 years mean age 54.6 |
Self-perceived health BMI |
54.4–56.5% reported good health According to BMI more than 70% was classified as overweight |
4(6) | 5 dietary pattern were identified and characterised by additional life-style factors. | Sami language criteria and self-identification Ethnicity divided into 4 groups. Sami affiliation 33% Article focus on dietary patterns and its association to self- perceived health, ethnicity, life-style and demographic factors |
| Brustad M et al., 2009 |
Norway | Register-based retrospective cohort 1991–2006 |
Inside/outside SUF area Coastal/inland residence |
Calculated per 1000 subjects per 5 years | Mortality | Mortality rates were similar between geographical areas with low and high density of Sami | 7(8) | The risk of mortality has a homogenous pattern across ethnic groups but there are indications of differences in infant mortality. | SUF = Sami Development Fund |
| Daerga L et al., 2004 |
Sweden | Prospective cohort Questionnaire Clinical examinations Interviews |
Reindeer herding Sami/ 60% |
n = 51 26 men/ mean age 50.2 25 women/ mean age 49.6 |
Work-related musculoskeletal pain (MSP) | MSP were prevalent. High exposure of vehicle the main cause among men and psycho-social risk factors among women | 0(8) | Implementing of an intervention programme may reduce the severity of MSP symptoms among reindeer herders. | 2-year intervention prevention programme |
| Daerga L et al., 2008 |
Sweden | Questionnaire Cross-sectional |
Reindeer herding (RH) family members/Swedish reference population Response rate 67.3% |
n = 99 56 men 43 women Adults over 18 years |
Physical function General health |
RH scored higher on physical function than the reference population, but lower on general health scales. | 4(6) | The health-related quality of life was similar compared to a Swedish reference population. | Data from 7 reindeer-herding communities Article focus on quality of life related to physical, psychosocial and socioeconomic conditions. |
| Eckhoff C et al., 2014 |
Norway | Cross-sectional Questionnaire 2003–2005 |
4881 Sami youths /non Sami youths 10% indigenous Sami Response rate 83% |
n = 4881/ 15–16 years |
Musculoskeletal pain (MSP) | High prevalence of MSP, higher among females. 22,4% reported 3–4 pain sites |
3(6) | No difference in MSP between Sami and non-Sami | The Norwegian Arctic Adolescent Health Study (NAAHS) |
| Edin-Liljegren A et al., 2004 |
Sweden | Retrospective cohort | Sami Reindeer-herding Sami (RH) Non-Reindeer herding Sami Controls |
n = 611 n = 170 n = 441 n = 1222 30,40,50, 60 years of age |
Cardiovascular disease (CVD) | Similar risk factor patterns between Sami and non-Sami in developing CVD. RH men had lower blood pressure, higher job demands, and were more physically active. | 5(8) | Different exposure to psychosocial- and behaviour risk factors partly explained the differences, which suggests are related to working conditions and lifestyle factors. | Cohort constructed from national population registers. Data from CVD preventive programme 1990–2001. Article focus on risk factors. |
| Eliassen BM et al., 2013 |
Norway The Saminor 1 study (2003–2004) |
Cross-sectional Questionnaire | Sami | N = 4027 36–79 years |
CVD | Marginalised Sami living in Norwegian dominated areas were more likely to report cardiovascular diseases than non-marginalised Sami living in Sami majority areas. | 4(6) | The exposure to chronic stress following marginalisation were suggested as a plausible explanation. | Sami language criteria and self-identification |
| Eliassen BM et al., 2014 |
Norway The Saminor 1 study (2003–2004) |
Cross-sectional Questionnaire Clinical examinations |
Sami non-Sami/ 60.9% |
N = 15,206 36–79 years |
Angina pectoris symptoms (APS) Self-reported Angina (SRA) |
APS and SRA more prevalent in Sami compared to non-Sami. | 4(6) | In women, less moderate alcohol consumption and leisure time physical activity in Sami may explain the ethnic difference. | Sami language criteria and self-identification |
| Eliassen BM et al, 2015 |
Norway The Saminor 1 study (2003–2004) |
Cross-sectional Questionnaire | Sami non-Sami/ 60.9% |
N = 15,206 36–79 years |
Myocardial infarction(SMI) | No ethnic differences in SMI | 4(6) | Similar living conditions and close interactions between ethnics groups may explain the findings. | Sami language criteria and self-identification |
| Eriksen AMA et al., 2016 |
Norway The Saminor 2 study |
Cross-sectional Questionnaire |
Sami non-Sami/ 27% |
N = 11,130 2167 Sami 8963 non-Sami 18–69 years |
Chronic pain(ChP) | Chronic pain; Sami men 48.5% Sami women 52.8% |
3(6) | Childhood violence was associated with adult ChP & increased number of pain sites. | Sami language criteria and self-identification 19.5% Sami residents Article focus on association between childhood violence and chronic pain. |
| Hansen KL et al., 2010 |
Norway The Saminor 1 study (2003–2004) |
Cross-sectional Questionnaire | Sami non-Sami Sami 33.1% Kven 7.8% Norwegian 59.1% |
n = 12 265 36–79 years |
Self-reported health | Poor health; Sami men 28.8–31.4% Sami women 32.9–35.4% Sami reports poorer health than the Norwegian population. Women reports poorer health than men. |
3(6) | Self-reported ethnic discrimination and low socio-economic status contributes to the inequalities. | Sami were grouped according to their Sami affiliation. Article focus on discrimination and ethnicity. |
| Harbo HF et al., 2007 |
Norway | Clinical examinations Blood samples | Sami Sami controls non-Sami controls |
n = 12 n = 200 n = 312 |
Multiple sclerosis (MS) |
Lower prevalence of MS among Sami | 4(8) | Low frequency of MS-associated haplotype together with genetic and environmental factors may contribute to the findings. | Sami language criteria and identified in clinical settings or in questionnaire. |
| Hassler S et al., 2005 |
Sweden | Register-based Cohort |
Constructed Sami cohort, non-Sami reference population |
N = 41,721 7482 reindeer-herding Sami/34,239 non-herding Sami non-Sami ref pop 4 times larger |
Standard mortality ratio (SMR) Life expectancy Death causes |
Lower SMR for cancer and a higher SMR for injuries with external causes in Sami men Higher SMRs for diseases of the circulatory and respiratory systems in Sami women, compared to ref pop. | 7(8) | Similarities in mortality patterns due to close interactions between ethnic groups. Differences may be explained by lifestyle, psychosocial and/or genetic factors. | National kinship register. Occupational register of Statistics Sweden 1960–1990. National register of Reindeer enterprises. Electoral register of the Sami Parliament 1993 and 1997. |
| Hassler S et al., 2008 |
Sweden | Register-based Cohort |
Constructed Sami cohort, non-Sami reference population |
N = 41,721 7482 reindeer-herding Sami/34,239 non-herding Sami non-Sami ref pop 4 times larger |
Cancer | Sami women; higher risk for stomach- and ovaries cancer. Lower risk for bladder cancer. Sami men; higher risk for stomach cancer lower risks for colon-, prostate cancer, malignant melanoma and non-Hodgkins lymphoma. |
7(8) | The differences are suggested to be related to traditional Sami lifestyle factors, for example diet and physical activity, as protective factors from developing cancer. | National kinship register. Occupational register of Statistics Sweden 1960–1990. National register of Reindeer enterprises. Electoral register of the Sami Parliament 1993 and 1997. |
| Naseribafrouei A et al., 2016 |
Norway The Saminor 1 study (2003–2004) |
Cross- sectional Questionnaire Non-fasting blood samples |
Sami non-Sami/ 60,9% |
N = 15,208 36–79 years |
Pre-diabetes(PD) Diabetes mellitus (DM) |
PD Sami; men 3.4% women 2,7% DM Sami; men 5,5% women 4,8% |
4(6) | Heterogeneity in the prevalence of PD and DM in different geographical regions and between different ethnic groups | Sami; language criteria and self-identification |
| Nystad T et al., 2010 |
Norway The Saminor 1 study (2003–2004) |
Questionnaire Clinical examination | Sami non-Sami/ 57.3% |
n = 15 546 36–79 years |
Obesity BMI |
High prevalence of obesity. Sami women more obese than Norwegian women. Sami men less obese than Norwegian men. | 5(6) | More studies are needed to examine if the ethnic differences are due to dietary habits and/or physical activities. | Sami language criteria and self-identification |
| Omma L et al., 2012 |
Sweden | Cross-sectional Questionnaire | Sami youths 59% |
n = 516 18–28 years |
Self-reported health Headache |
95.3% felt healthy 72,3% men 63,3% women Often headaches men 4,6% women 13,2% |
3(6) | Young Sami had good health. Physical health in young Sami may be better than in young Swedes. | Sami Educational Centre Jokkmokk, Sami parliament electoral register, Reindeer-owner register, the Sami youth organisation, 24 Sami organisations. Article focus mental health. |
| Omma L et al, 2015 |
Sweden | Cross-sectional Questionnaire |
Sami children 12–18 years 70% |
n = 121 12–18 years |
Health-related quality of life (HRQOL) Physical wellbeing |
30–40% reported low-functioning and well-being. High physical wellbeing was reported by 27%. |
5(6) | Those with an explicit Sami identity reported low HRQOL in some aspects. Ethnicity-relative negative treatments partly explain the lower HRQOL. | Sami school programmes |
| Ross AB et al., 2009 |
Sweden | Cross-sectional Questionnaire Clinical measurements |
Reindeer-herding Sami (RS) Non-reindeer herding Sami (NRS) non-Sami controls (NS) |
n = 145 n = 450 n = 1000 Mean age 42–47.4 years |
Blood glucose Blood pressure Physical activity BMI |
RS women lower plasma glucose. RS men lower diastolic blood pressure. RS higher physical activity to NRS. BMI 25,2–26,2 |
3(6) | No significant difference of BMI among the groups. Traditional lifestyle defined by occupation is reflected in food and nutrient intake. |
The Västerbotten Cardiovascular Intervention Programme (1990–2001) Article focus on food and nutrient intake. |
| Sjölander P et al., 2008 |
Sweden (1985–2002) |
Register-based Cohort |
Sami cohort Reindeer herding(RH) non-herding Sami (NH) non-Sami controls, 4 times larger |
n = 15,914 n = 4465 n = 11,449 .n = 71,550 |
Incidence & mortality from Stroke, Subarachnoid haemorrhage (SAH) Acute myocardial infarct (AMI) |
No elevated risk of developing AMI among the Sami. Higher incidences of stroke and SAH for both Sami men and women. | 6(8) | Differences in incidence of stroke are caused by behavioural and psychosocial risk factors. | RH: National Occupational registers & Registers of Reindeer Breeding Enterprisers NH: Electoral registers of the Sami parliament and National Kinship registers |
| Sjölander P et al., 2008 |
Sweden | Cross-sectional Questionnaire |
Reindeer herders (RH) 68% Controls; women, reindeer herding families Men, blue-collar workers |
n = 74 men ≥18 years Controls; n = 53 women n = 194 |
Musculoskeletal symptoms | RH men symptoms in any region previous 7 days 78% 12 months 92% |
5(6) | Musculoskeletal symptoms constitute a health problem in reindeer husbandry which calls for preventive actions. | Reindeer-herding communities 1 Jämtland 3 Västerbotten 4 Norrbotten |
| Soininen L et al., 2008 |
Finland Municipalities of Inari and Utsjoki (1979–2005) |
Retrospective cohort |
Sami* non-Sami ”mixed” Sami *Sami classified as a person with at least 75% of any ethnic group of Sami |
n = 2091 n = 4161 |
Mortality | Cancer mortality is low. Accidents and suicides are common. | 6(8) | The total mortality rates of the Sami do not differ from that of the general population. The Sami men had a lower disease mortality compared with the Finnish population | National population register; Sami classification by interview Sami persons to identify language and from studying genealogical sources. |
| Soininen L et al., 2012 |
Finland Municipalities of Inari and Utsjoki (1979–2009) |
Retrospective cohort |
Cancer patients; Sami non-Sami “mixed” Controls; Finnish patients outside the cohort |
n = 2091 n = 4161 n = 20 181 |
Cancer patients survival in rural areas compared to average Finnish cancer patients | Sami; 204 cancer cases non-Sami;391 cancer cases |
6(8) | No difference between the cancer survival in the different groups. Long distances to medical care or Sami ethnicity have no influence of the cancer survival | Sami identified by material of the Finnish International Biological programme which were based on interview and by genealogical sources |
| Spein AR et al., 2013 |
Norway The Norwegian Arctic Adolescent Health study (2003–2005) |
Cross-sectional Questionnaire |
Sami youths 10th-11th graders |
n = 350 | Self-reported health (SRH) | 89% of the Sami youth reported good or very good health | 3(6) | Physical activity was protective for good SRH. Suicidal thoughts were risk factors associated with poor SRH. | Sami; Objective questions of ethnicity and language and subjective questions of self-identification |
| Storm C et al., 2006 |
Sweden The municipalities of Gällivare and Kiruna |
Cross-sectional Questionnaire |
Sami women 21–70 years 65% |
N = 487 | Neck-shoulder pain (NSP) Temporomandibular disorders (TMD) Headache Self-reported health |
Prevalence: NSP 56%, TMD 32%, Headache 61% Good health 86% |
4 (6) | Musculoskeletal symptoms are common among an adult sample of Sami women. Comorbidity between symptoms was found. |
Electoral register of the Sami parliament or registered as reindeer herders/owners in the Swedish Board of Agriculture. |
| Storm C et al., 2007 |
Sweden The municipalities of Gällivare and Kiruna |
2-year follow up Questionnaire Clinical case-control study |
Sami women | n = 68 mean age 48.7 |
Neck-shoulder pain (NSP) Temporomandibular disorders (TMD) Headache BMI |
Annual incidence rate TMD 6.5% Cases has higher BMI (28.2) than controls (25.4) |
7(8) | Severe TMD symptoms remained unchanged over the 2-year follow-up and was related to impaired general health and awareness of oral para-functions. | Electoral register of the Sami parliament or registered as reindeer herders/owners in the Swedish Board of Agriculture. |
General health and health-related quality of life
Based on data from the SAMINOR study in Norway, a population-based study of health and living conditions, Sami people reported poorer health than the general Norwegian population. The prevalence of good/very good health was reported as 64.6–67.1% among Sami women, and 68.6–71.2% among Sami men, depending on different categorisations of Sami. A gender difference was observed, with women reporting poorer health than men. Sami ethnicity was associated with poorer self-reported health when compared to the Norwegian majority population. Discrimination was suggested as being partly to blame for the health inequalities [11]. The general health state was reported as good by 86% of a sample of Sami women in Arctic Sweden. 24% had a disease which was under medical care, and 29% took prescription medications [12]. Among Sami youths in Sweden, 95% felt healthy and 91% slept well. Men reported good health more often than women [13]. In Norway as well, a majority (88.5%) of Sami and non-Sami adolescents reported good or very good health [14]. This was also true for participants aged 36–79 in the SAMINOR study [15], and for Sami adolescents, with 89% reporting good or very good health [16]. According to the SAMINOR study data, self-reported insomnia and use of hypnotics were less common in the Sami population than among the majority. The prevalence of hypnotic use was 7.1%. Between 66.9% and 71.0% of the Sami reported no problem with insomnia, compared to 64.4% among the non-Sami population [17]. Sense of coherence (SOC) is hypothesized as being closely related to health. In a Swedish sample, no significant differences between Sami and non-Sami were found. Reindeer-herding Sami, on the other hand, have lower SOC than non-herding Sami. 68.4% of the non-herders declare themselves healthy, compared to 62.4% of the herders. 75.9% of the non-Sami, compared to 67.3% of the Sami, declare themselves healthy. Neither of these differences were statistically significant [18]. In a sample of 99 adult men and women in reindeer-herding families, the health-related quality of life was similar when compared to a Swedish reference population. On the SF-36 questionnaire used to assess the health-related quality of life, both men and women scored higher on physical function than the reference population, but lower on the included general health scales [19]. Among Sami schoolchildren in Sweden, the health-related quality of life was lower than for Swedish schoolchildren in general [20].
Mortality and causes of death
The included studies indicate more similarities than differences in mortality rates among the Sami and non-Sami populations in their traditional geographical area, Sápmi. In Arctic Norway, mortality rates did not differ among different geographic regions with higher or lower proportions of Sami. There was a difference in infant mortality rate between what was defined as coastal non-Sami areas (1.8/1000) and Sami inland area (6.2/1000) [21]. In Sweden, also, the differences in mortality rates and life expectancy at birth (LEB) between the Sami and the reference population (RP) were small (LEB 74.9 years for Sami men compared to 74.6 years for men in the RP and 80.3 years for women in RP compared to 80.0 for Sami women) based on a cohort between 1961 and 2000. Sami men were found to have a lower Standardised Mortality Ratio (SMR) for cancer, and a higher SMR for injuries with external causes, compared to the reference population. Among Sami women, higher SMRs for diseases of the circulatory and respiratory systems were found when compared to the reference population. An increased risk of dying of subarachnoid haemorrhage was also reported among both Sami men and women. Life expectancy at birth was 74.9 years for Sámi men, and 80.0 years for Sami women, with no statistically significant difference compared to the reference population. The most common causes of death were diseases of the circulatory system, followed by cancer and injuries with external causes [22]. Among reindeer-herding Sami families in Sweden, accidents related to transport vehicles were the causes of 158 unnatural deaths between 1961 and 2000. Road traffic accidents contributed to 16% of deaths, and snowmobile fatalities accounted for 11%. Half of the victims were alcohol affected. Suicides accounted for 23% of deaths [23]. Deaths caused by vehicle accidents were also common in Finland, based on a cohort between 1979 and 2005. Suicide mortality among Sami men was elevated compared to non-Sami men. However, a lower disease-related mortality among Sami men was observed, compared to the general population, attributable to the low mortality from cancer, but possibly also related to diet, physical activity and genetics. Also among Sami men, SMRs for dementia and Alzheimer´s disease were higher, while SMRs for circulatory diseases were similar between the populations [24].
Cardiovascular and cerebrovascular diseases
In Sweden, similar patterns for Sami and non-Sami people in regard to the risk of developing cardiovascular diseases were reported. Varying exposures to psychosocial- and behaviour risk factors partly explained the differences, which were suggested as being related to working conditions and lifestyle factors. Reindeer-herding men had lower blood pressure, higher job demands, and were more physically active [25]. In Norway, marginalised Sami living in Norwegian-dominated areas were more likely to report cardiovascular diseases than non-marginalised Sami living in Sami majority areas. The authors suggest exposure to chronic stress as a result of marginalisation as a plausible explanation. No gender differences were found [26]. The prevalence of self-reported myocardial infarction was similar for Sami and non-Sami people in rural areas of Norway, based on a health survey in 2003–2004. Similar living conditions and close interactions between ethnic groups were considered as a plausible explanation for the similarities. Self-reported angina pectoris, on the other hand, was found to be more prevalent in Sami compared to non-Sami. In Sweden, no elevated risk for acute myocardial infarction were found in a Sami cohort compared to a demographically matched non-Sami population, between 1985 and 2002. Higher incidence rates of stroke and subarachnoid haemorrhage for Sami men and women, compared to a non-Sami control population, were observed [27–29].
Cancer
The cancer incidence rate among the Sami was lower than that of the general population of Sweden. Sami also had a lower cancer incidence rate than that of the non-Sami living in the same geographical area. In Finland, a lower incidence rate of cancer among the Sami, compared to the general population, has also been found. In Sweden, Sami women had higher risks for stomach cancer and ovarian cancer, but lower risk for bladder cancer, compared to a demographically matched reference population. Sami men had also a higher risk for stomach cancer, but lower risks were reported for colon cancer, prostate cancer, malignant melanoma and for non-Hodgkins lymphoma when compared to the non-Sami reference population. Reindeer-herding Sami showed a lower relative cancer risk compared to the non-reindeer herding Sami. The differences are hypothesized as relating to traditional Sami lifestyle practices, for example, diet and physical activity, which are suggested to be protective factors. In Finland, no differences in cancer survival rates were observed between Sami cancer patients and non-Sami patients living in the same rural area or when compared to the general population. The authors concluded that neither living a long distance away from accessible medical care, nor Sami ethnicity, influenced the cancer survival rate in northern Finland [30,31].
Metabolic syndrome and diabetes mellitus
A high prevalence of metabolic syndrome (MetS) in both Sami and non-Sami populations was observed, based on the SAMINOR study conducted in 2003–2004. Central obesity, elevated systolic blood pressure and high triglyceride levels were the most prevalent risk markers. Using the European waist circumference cut-off as the definition for MetS, a prevalence of between 22.3% and 38.7% was reported in the Sami population [32]. In Norway, a diabetes prevalence of 5.2% in Sami men, and 5.0% in Sami women, was reported by the SAMINOR study. The study did not differentiate between type 1 or type 2 Diabetes Mellitus. No ethnic differences were found; however, ethnicity affected the treatment. A combined treatment involving insulin and tablets was used more frequently among Sami men than among non-Sami men, and treatment with tablets was more commonly used among Sami women than among non-Sami women. The age-standardised prevalence of pre-diabetes was reported as 2.7–3.4%, and the prevalence of Diabetes Mellitus as 4.6–4.8% among the Sami population. The prevalence of both Diabetes and pre-diabetes increased with age, and no ethnic differences were found [32,33].
Musculoskeletal pain disorders and other pain symptoms
Among adolescents between 15 and 16 years old in Norway, a high prevalence of musculoskeletal pain was observed. There were gender differences, with higher pain prevalence in females. No differences between Sami and non-Sami youths were found. Headaches were reported by 66% of Sami females, compared to 43% of Sami men. Neck/shoulder pain was reported by 46% of Sami females, and 29% of Sami men. Back pain, and pain in the arms, knees or legs was reported by approximately 30%, of men and women, respectively. A strong association was found between musculoskeletal pain sites and psychosocial problems, with a linkage between childhood violence and chronic pain in adulthood also being reported, but the Sami youths did not suffer symptoms at a greater rate than the non-Sami youths [14]. Between 48% and 55.1% reported chronic pain, according to the SAMINOR study, with no ethnic differences. However, chest and stomach pain were more frequently reported by Sami men than non-Sami men. Sami women reported stomach and pelvic pain more frequently than non-Sami women [34]. In Sweden, frequent headaches were reported by 9.5% of a sample of young Sami, aged 18–28 [13], and in an adult Sami female population, 61% reported headaches. In the same sample of adults, the prevalence of pain and/or dysfunction in the jaw-face region was 32%, and pain in the neck/shoulder region was reported by 56% [12]. Severe symptoms were usually related to impaired general health [35]. A high prevalence of musculoskeletal symptoms was also reported in a group of 51 Sami individuals in Sweden involved in reindeer herding. High exposure to the use of motor vehicles was the main cause of musculoskeletal pain among men, while psychosocial risk factors were suggested as the main cause in women. Musculoskeletal symptoms were more common among women [36]. The prevalence of self-reported musculoskeletal symptoms was also high in a sample of 74 male reindeer herders followed over a 12-month period; headaches were reported by 39% of them, neck pain by 57% and lower back pain by 73% [37].
Other diseases/disorders/deficiencies/loads
In Norway, a low prevalence of multiple sclerosis in a Sami population was reported, compared to the non-Sami. The author suggested that a low frequency of an MS-associated haplotype was related to the low prevalence among Sami, together with other reduced genetic and environmental risk factors associated with the disease. There are no data on MS prevalence among Sami in Finland, Sweden or Russia [38].
The first study to evaluate the iron status of a multi-ethnic population in different geographic regions, including self-perceived Sami, was the SAMINOR study (2003–2004) in Norway. Geographic differences in iron levels were reported and hypothesized as being related to nutritional habits. The authors concluded that iron metabolism probably does not differ between the Sami people at a group level compared to a non-Sami population. Sami men and women living in inland areas had higher s-ferritin than either non-Sami in the same area or coastal Sami. Inland residents have also higher transferrin saturation than coastal residents. Higher levels of s-ferritin and mean transferrin saturation were found in participants with higher intake of reindeer meat, in addition to obesity and overweight. Obesity was associated with s-ferritin in both genders. Over 70% were classified as having overweight, with individuals having overweight being the most frequent consumers of reindeer meat, and having a low level of physical activity. The mean BMI among all ethnic groups was above the WHO classification of overweight. Results from a Swedish study showed a mean BMI between 25.2 and 26.2 among a Sami population, with no differences between genders, or non-reindeer herders vs reindeer herders or when compared with a control group [15,39–41]. In a sample of Sami women in Arctic Sweden, obesity was found to be related to severe TMD (mean BMI 28.2) in comparison with TMD free controls (mean BMI 25.4) [35]. The prevalence of obesity, based on SAMINOR data, was reported to be high, especially in Sami women [42].
Discussion
This systematic review was conducted in order to overview current knowledge regarding the state of somatic health among the Indigenous Sami. As the Sami People’s traditional lands – Sápmi – extend across four countries (Norway, Sweden, Finland and the Kola Peninsula of Russia), presenting a coherent picture of the somatic health situation of the only recognised Indigenous People in the north of Europe is a challenging task. However, what stands out in this review is that Norway has the strongest position in terms of knowledge concerning Sami somatic health. Much of this is due to the publications stemming from the Centre for Sami Health Research at the Arctic University of Norway. Summary results built on robust data from Norway showed only minor differences in health and wellbeing, favouring the non-indigenous in the same geographical region.
A systematic review assessing the quality of studies on the Sami population´s health situation has not been previously conducted. A systematic review compiles results from original studies regarding the subject, and is characterised by its assessment of the quality of the included studies, using a standardised tool. In this review, we used the Newcastle–Ottawa scale, which is a commonly used tool in medicine. Advantages with the NOS tool are that it is validated for case-control – and cohort studies. It is also user-friendly. However, it is not yet validated for cross-sectional studies, which were the majority of studies included in this review. As majority of studies on the health of the indigenous Sami are of cross-sectional design, that is one reason why none of the studies obtain the highest score. Additionally, this leads to a gap in knowledge due to the fact that no conclusions on causality of diseases can be drawn.
Longitudinal prospective studies in the health field concerning the Sami people are missing. It is obvious that such studies are much-needed, to explore risk factors and risk assessments for diseases/disorders affecting the Sami people. A call for improved data is in accordance with the United Nations Sustainable Development Goals (especially no. 17), and was also highlighted by the Lowitja–Lancet Collaboration, in their global review, as something every nation state needed to improve [4]. At the same time, Walker et. al. (2017) underline that this future work needs to be done in close collaboration with indigenous communities [43]. One should also have in mind that the concept of health may vary between Indigenous people and the majority people. Western methods of understanding health, and preventing poor health, tend to be focused on the individual; which is also how nation states’ systems of collecting data and relevant information are built [44,45]. Langås-Larsen et al. (2018) argue that traditional social networks still exist in northern communities, and that they, especially in Sami context, are important when persons become ill. These networks are activated when people fall ill and include the use of traditional healers that point to a broader understanding of disease and illness [46].
Additionally, our review also highlights that definitions of study populations varied widely between the studies, making comparisons and concluding results difficult. Determining Sami identity is a challenging task in itself. A Swedish population-based study used register-based data (1960–2000) without self-identification, while the SAMINOR study is based on self-identification, and then linking the populations to registers. In Sweden, it is obvious that reindeer herding is a recurrent identifier of indigenous identity. This is in accordance with the Swedish state’s system of identifying reindeer herding as an occupation for Sami people only. Hence, focusing on the health of reindeer herders is by definition working in the field of Indigenous Sami health. However, it is important to stress the well-established fact that reindeer herders are a minority within the Indigenous Sami population [47].
International guidelines for health research favour self-identification. However, Pettersen and Brustad (2015) point out that even though their general results were that Sami identification was rather consistent over time; they found an increasing willingness to self-identify as Sami if the individual had commenced higher education. Consequently, researchers must be aware of the historical and social context in which their study is taking place [48].
Different studies use different criteria of Sami ethnicity, and it also seems to be country related. In Norway, the inclusion criteria are mostly based on language criteria and geographical connections. In Sweden, the studies are based on reindeer herders vs non-reindeer herders or on individuals registered in the electoral register of the Sami Parliament.
Despite the uncertainty, there is evidence that the majority of adult Sami experience good health. Sami men are feeling healthier than women. Regarding youth samples, there are different results between different studies [12–16,20]. Mortality and life expectancy were similar between Sami and non-Sami population, with only minor differences. Common death causes were diseases of the circulatory system, cancer and vehicle accidents [21,22,24]. There is also evidence from Norway that self-reported myocardial infarction rates were similar among Sami and non-Sami, but Angina pectoris was more prevalent among Sami. In Sweden, cardiovascular disease rates were similar between Sami and non-Sami [25–29]. As with the general populations of the Nordic countries, the incidence of cancer among the Sami people has increased over recent decades. Cancer is one of the few diseases that has been thoroughly studied in the Sami population. A major reason for that was the increased cancer risk due to nuclear fallout contamination in areas within Sápmi as a result of the Chernobyl nuclear reactor accident in 1986, and also from nuclear weapons testing on the island of Novaya Zemlya in the 1950s and 1960s. To date, no detectable excess of the radiation-sensitive cancers, such as leukaemia and thyroid cancer, has been observed in any of the countries. At present, conclusive results from Norway, Sweden and Finland reveal a generally lower risk of developing and dying of cancer for Sami than for non-Sami people living in the same geographical regions. However, cancers of the stomach in these regions are more prevalent than the national average. In all countries, Sami show a lower risk of prostate cancer. Among Sami men in both Finland and Norway, significantly lower standardised incidence ratios for bladder cancer were observed. Breast cancer was less common in Finland among Sami compared to non-Sami. Suggested explanations for the low cancer risks are connected to the traditional Sami lifestyle, such as dietary components (high intake of antioxidants and unsaturated fatty acids), and high levels of physical activity that may be protective factors against developing cancer. Genetic factors have also been suggested as an explanation for this lower risk of developing cancer [30,31,49]. The prevalence of Diabetes mellitus is around 5%, based on the SAMINOR survey, with no ethnic differences. No data on a Sami sample from the other countries exists [32,33]. There is evidence of a high prevalence of musculoskeletal pain symptoms in youths and adults within the Sami population. Around 20% of the European population suffers from chronic pain [50]. The most common causes of pain in the orofacial region are temporomandibular disorders (TMD), which are regarded as musculoskeletal disorders in the jaw-face region. Comorbidity between TMD, headache, and neck/shoulder pain was observed [12–14,34,35,37]. At the time of this review, no studies on musculoskeletal disorders among Sami existed from either Finland or Russia. There is evidence that obesity and overweight are common among Sami individuals, especially among women. This was associated with higher levels of s-ferritin as a consequence of higher intake of reindeer meat [15,35,39,41,42].
We have assessed a quality score above 50% of the highest possible score as a study of moderate quality. Only studies where the maximum score is 8 can be assessed as a high-quality study. No study within this review reached the highest score, but several studies were nevertheless of high quality.
Although there is reliable evidence in certain areas, there is still a great need for more research within the field of Sami health in several other areas. When planning future epidemiological studies involving the Sami people, longitudinal prospective studies are suggested. This will improve the scientific evidence to a great extent. More studies from Russia, Finland and Sweden are also needed. In comparison with Norway, where the national state provides financial support for Sami health research, the other states also need to take actions for knowledge improvements. Collaborations across the borders, preferably comparative studies covering the traditional land area of the Sami people, across Norway, Sweden, Finland and Russia would also be encouraged. This would offer larger population sizes, similarities in data collection and analysis methods, as well as calibration in examination methods. To enable comparisons between studies, and also between countries, it might also be advantageous to use the same definition of Sami identity in research.
Conclusion
To summarise, this review shows that there are extensive knowledge gaps regarding the state of somatic health among the indigenous Sami population in the circumpolar area, especially in Russia, Finland and Sweden. Current knowledge is somewhat outdated and fragmented, with the one exception of the SAMINOR study in Norway. No studies included in this review managed to obtain the highest quality score according to the assessment tool used, and thus more longitudinal prospective studies are suggested.
Supplementary Material
Acknowledgments
Financial support was provided by the Knut and Alice Wallenberg Foundation through their Wallenberg Academy Fellows programme (2012.0222).
Correction Statement
This article has been republished with minor changes. These changes do not impact the academic content of the article.
Disclosure statement
No potential conflict of interest was reported by the authors.
Supplementary material
Supplemental data for this article can be accessed here.
References
- [1].Sjölander P. What is known about the health and living conditions of the indigenous people of northern Scandinavia, the Sami?. Glob Health Action. 2011;4 PubMed PMID: 22007156; PubMed Central PMCID: PMC3195409. doi: 10.3402/gha.v4i0.8457. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].Stoor JPA. Kunskapssammanställning om samers psykosocial ohälsa. Kiruna: Sametinget. Sverige; 2016. ISBN 978-91-981500-9-4. [Google Scholar]
- [3].Redvers J, Bjerregaard P, Eriksen H, et al. A scoping review of Indigenous suicide prevention in circumpolar regions. Int J Circumpolar Health. 2015;74:27509 PubMed PMID: 25742882; PubMed Central PMCID: PMCPMC4981753. . [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].Anderson I, Bang A, Bjertness E, et al. Indigenous and tribal peoples’ health - authors’ reply. Lancet. 2016. December 10;388(10062):2868 PubMed PMID: 27979402. [DOI] [PubMed] [Google Scholar]
- [5].Axelsson P. Abandoning “the other”: statistical enumeration of Swedish Sami, 1700 to 1945 and beyond. Ber Wiss. 2010;33(3):263–16. PubMed PMID: 21466142. [DOI] [PubMed] [Google Scholar]
- [6].Madden R, Axelsson P, Kukutai T, et al. Statistics on indigenous peoples: international effort needed. Stat J IAOS. 2016;32(1):37–41. [Google Scholar]
- [7].Lund E, Melhus M, Hansen KL, et al. Population based study of health and living conditions in areas with both Sami and Norwegian populations–the SAMINOR study. Int J Circumpolar Health. 2007. April;66(2):113–128. PubMed PMID: 17515251; eng. [DOI] [PubMed] [Google Scholar]
- [8].Brustad M, Hansen KL, Broderstad AR, et al. A population-based study on health and living conditions in areas with mixed Sami and Norwegian settlements - The SAMINOR 2 questionnaire study. Int J Circumpolar Health. 2014;73. doi: 10.3402/ijch.v73.23147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].Wells BS GA, O’Connell D, Peterson J, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. http://wwwohrica/programs/clinical_epidemiology/oxfordasp. 2011.
- [10].Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. J Clin Epidemiol. 2009. October;62(10):1006–1012. PubMed PMID: 19631508. [DOI] [PubMed] [Google Scholar]
- [11].Hansen KL, Melhus M, Lund E. Ethnicity, self-reported health, discrimination and socio-economic status: a study of Sami and non-Sami Norwegian populations. Int J Circumpolar Health. 2010. April;69(2):111–128. PubMed PMID: 20359443; eng. [DOI] [PubMed] [Google Scholar]
- [12].Storm C, Wänman A. Temporomandibular disorders, headaches, and cervical pain among females in a Sami population. Acta Odontol Scand. 2006;64(5):319–325 PubMed PMID: 16945899. [DOI] [PubMed] [Google Scholar]
- [13].Omma L, Jacobsson LH, Petersen S. The health of young Swedish Sami with special reference to mental health. Int J Circumpolar Health. 2012;71:18381 PubMed PMID: 22765937; PubMed Central PMCID: PMCPmc3417696. eng. . [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].Eckhoff C, Kvernmo S. Musculoskeletal pain in Arctic indigenous and non-indigenous adolescents, prevalence and associations with psychosocial factors: A population-based study. BMC Public Health. 2014;14(1). DOI: 10.1186/1471-2458-14-617 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Brustad M, Parr CL, Melhus M, et al. Dietary patterns in the population living in the Sami core areas of Norway–the SAMINOR study. Int J Circumpolar Health. 2008. February;67(1):82–96. PubMed PMID: 18468261; eng. [PubMed] [Google Scholar]
- [16].Spein AR, Pedersen CP, Silviken AC, et al. Self-rated health among Greenlandic Inuit and Norwegian Sami adolescents: associated risk and protective correlates. Int J Circumpolar Health. 2013;72 PubMed PMID: 23396865; PubMed Central PMCID: PMCPmc3567202. eng. doi: 10.3402/ijch.v72i0.19793. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17].Bakken K, Melhus M, Lund E. Use of hypnotics in Sami and non-Sami populations in northern Norway. Int J Circumpolar Health. 2006. June;65(3):261–270. PubMed PMID: 16871832; eng. [DOI] [PubMed] [Google Scholar]
- [18].Abrahamsson A, Lindmark U, Gerdner A. Sense of coherence of reindeer herders and other Samis in comparison to other Swedish citizens. Int J Circumpolar Health. 2013;72:20633 PubMed PMID: 23853763; PubMed Central PMCID: PMC3709198. . [DOI] [PMC free article] [PubMed] [Google Scholar]
- [19].Daerga L, Edin-Liljegren A, Sjolander P. Quality of life in relation to physical, psychosocial and socioeconomic conditions among reindeer-herding Sami. Int J Circumpolar Health. 2008. February;67(1):8–26. PubMed PMID: 18468256; eng. [PubMed] [Google Scholar]
- [20].Omma L, Petersen S. Health-related quality of life in indigenous Sami schoolchildren in Sweden. Acta Paediatrica. 2015;104(1):75–83. (Oslo, Norway: 1992). . [DOI] [PubMed] [Google Scholar]
- [21].Brustad M, Pettersen T, Melhus M, et al. Mortality patterns in geographical areas with a high vs. low Sami population density in Arctic Norway. Scand J Public Health. 2009. July;37(5):475–480. PubMed PMID: 19541760; eng. [DOI] [PubMed] [Google Scholar]
- [22].Hassler S, Johansson R, Sjolander P, et al. Causes of death in the Sami population of Sweden, 1961-2000. Int J Epidemiol. 2005. June;34(3):623–629. PubMed PMID: 15737965; eng. [DOI] [PubMed] [Google Scholar]
- [23].Ahlm K, Hassler S, Sjolander P, et al. Unnatural deaths in reindeer-herding Sami families in Sweden, 1961-2001. Int J Circumpolar Health. 2010. April;69(2):129–137. PubMed PMID: 20356469; eng. [DOI] [PubMed] [Google Scholar]
- [24].Soininen L, Pukkola E. Mortality of the Sami in northern Finland 1979-2005. Int J Circumpolar Health. 2008. February;67(1):43–55. PubMed PMID: 18468258; eng. [PubMed] [Google Scholar]
- [25].Edin-Liljegren A, Hassler S, Sjolander P, et al. Risk factors for cardiovascular diseases among Swedish Sami–a controlled cohort study. Int J Circumpolar Health. 2004;63(Suppl 2):292–297. PubMed PMID: 15736671; eng. [DOI] [PubMed] [Google Scholar]
- [26].Eliassen B-M, Graff-Iversen S, Melhus M, et al. Ethnic difference in the prevalence of angina pectoris in Sami and non-Sami populations: the SAMINOR study. Int J Circumpolar Health. 2014;73 PubMed PMID: 24422205. doi: 10.3402/ijch.v73.21310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [27].Sjölander P, Hassler S, Janlert U. Stroke and acute myocardial infarction in the Swedish Sami population: incidence and mortality in relation to income and level of education [Artikel]. [Stroke and acute myocardial infarction in the Swedish Sami population: incidence and mortality in relation to income and level of education]. Scand J Public Health. 2008;36(1):84–91. PubMed PMID: 08021365. [DOI] [PubMed] [Google Scholar]
- [28].Eliassen BM, Graff-Iversen S, Melhus M, et al. Ethnic difference in the prevalence of angina pectoris in Sami and non-Sami populations: the SAMINOR study. Int J Circumpolar Health. 2014;73 PubMed PMID: 24422205; PubMed Central PMCID: PMC3889176. doi: 10.3402/ijch.v73.21310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [29].Eliassen BM, Graff-Iversen S, Braaten T, et al. Prevalence of self-reported myocardial infarction in sami and non-sami populations: the SAMINOR study. Int J Circumpolar Health. 2015;74. doi: 10.3402/ijch.v74.24424. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [30].Hassler S, Sjölander P, Grönberg H, et al. Cancer in the Sami population of Sweden in relation to lifestyle and genetic factors. Eur J Epidemiol. 2008;23(4):273–280. PubMed PMID: 18322808. . [DOI] [PubMed] [Google Scholar]
- [31].Soininen L, Pokhrel A, Dyba T, et al. Survival of Sami cancer patients. Int J Circumpolar Health. 2012;71:18959 PubMed PMID: 22765936; PubMed Central PMCID: PMCPmc3417662. eng. . [DOI] [PMC free article] [PubMed] [Google Scholar]
- [32].Broderstad AR, Melhus M. Prevalence of metabolic syndrome and diabetes mellitus in Sami and Norwegian populations. The SAMINOR-a cross-sectional study. BMJ Open. 2016. April 22;6(4):e009474 PubMed PMID: 27105711; PubMed Central PMCID: PMCPMC4853968. . [DOI] [PMC free article] [PubMed] [Google Scholar]
- [33].Naseribafrouei A, Eliassen BM, Melhus M, et al. Ethnic difference in the prevalence of pre-diabetes and diabetes mellitus in regions with Sami and non-Sami populations in Norway - the SAMINOR1 study. Int J Circumpolar Health. 2016;75:31697 PubMed PMID: 27507149; PubMed Central PMCID: PMCPMC4978855. . [DOI] [PMC free article] [PubMed] [Google Scholar]
- [34].Eriksen AM, Schei B, Hansen KL, et al. Childhood violence and adult chronic pain among indigenous Sami and non-Sami populations in Norway: a SAMINOR 2 questionnaire study. Int J Circumpolar Health. 2016;75:32798 PubMed PMID: 27802844; PubMed Central PMCID: PMCPMC5090132. . [DOI] [PMC free article] [PubMed] [Google Scholar]
- [35].Storm C, Wänman A. A two-year follow-up study of temporomandibular disorders in a female Sami population: validation of cases and controls as predicted by questionnaire. Acta Odontol Scand. 2007. November;65(6):341–347. PubMed PMID: 18071955; eng. [DOI] [PubMed] [Google Scholar]
- [36].Daerga L, Edin-Liljegren A, Sjolander P. Work-related musculoskeletal pain among reindeer herding Sami in Sweden–a pilot study on causes and prevention. Int J Circumpolar Health. 2004;63(Suppl 2):343–348. PubMed PMID: 15736681; eng. [DOI] [PubMed] [Google Scholar]
- [37].Sjölander P, Daerga L, Edin-Liljegren A, et al. Musculoskeletal symptoms and perceived work strain among reindeer herders in Sweden. Occup Med (Lond). 2008. December;58(8):572–579. PubMed PMID: 19054753. [DOI] [PubMed] [Google Scholar]
- [38].Harbo HF, Utsi E, Lorentzen AR, et al. Low frequency of the disease-associated DRB1*15-DQB1*06 haplotype may contribute to the low prevalence of multiple sclerosis in Sami. Tissue Antigens. 2007. April;69(4):299–304. PubMed PMID: 17389012; eng. [DOI] [PubMed] [Google Scholar]
- [39].Broderstad AR, Melhus M, Lund E. Iron status in a multiethnic population (age 36-80 yr) in northern Norway: the SAMINOR study. Eur J Haematol. 2007. November;79(5):447–454. PubMed PMID: 17924860; eng. . [DOI] [PubMed] [Google Scholar]
- [40].Ross AB, Johansson A, Vavruch-Nilsson V, et al. Adherence to a traditional lifestyle affects food and nutrient intake among modern Swedish Sami. Int J Circumpolar Health. 2009;68(4):372–385. PubMed PMID: 19917189. [DOI] [PubMed] [Google Scholar]
- [41].Broderstad AR, Melhus M, Brustad M, et al. Iron stores in relation to dietary patterns in a multiethnic population: the SAMINOR study. Public Health Nutr. 2011. June;14(6):1039–1046. PubMed PMID: 21208473; eng. [DOI] [PubMed] [Google Scholar]
- [42].Nystad T, Melhus M, Brustad M, et al. Ethnic differences in the prevalence of general and central obesity among the Sami and Norwegian populations: the SAMINOR study [Artikel]. [Ethnic differences in the prevalence of general and central obesity among the Sami and Norwegian populations: the SAMINOR study]. Scand J Public Health. 2010;38(1):17–24. PubMed PMID: 10021364. [DOI] [PubMed] [Google Scholar]
- [43].Walker J, Lovett R, Kukutai T, et al. Indigenous health data and the path to healing. Lancet. 2017. November 4;390(10107):2022–2023. PubMed PMID: 29115232. [DOI] [PubMed] [Google Scholar]
- [44].Kirmayer LJ. The health and well-being of Indigenous youth. Acta Paediatr Int J Paediatr. 2015;104(1):2–4. [DOI] [PubMed] [Google Scholar]
- [45].Axelsson P, Kukutai T, Kippen R. The field of Indigenous health and the role of colonisation and history. J Pop Res. 2016;33(1):1–7. [Google Scholar]
- [46].Langas-Larsen A, Salamonsen A, Kristoffersen AE, et al. “We own the illness”: a qualitative study of networks in two communities with mixed ethnicity in Northern Norway. Int J Circumpolar Health. 2018. December;77(1):1438572 PubMed PMID: 29466927; PubMed Central PMCID: PMCPMC5827718. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [47].Axelsson P, Sköld P. Indigenous populations and vulnerability. characterizing vulnerability in a sami context [Indigenous Populations and Vulnerability. Characterizing Vulnerability in a Sami Context]. Annales De Démographie Historique. 2006;111(1):115–132. Fr. [Google Scholar]
- [48].Pettersen T, Brustad M. Same Sámi? A comparison of self-reported Sámi ethnicity measures in 1970 and 2003 in selected rural areas in northern Norway. Ethnic Racial Stud. 2015;38(12):2071–2089. [Google Scholar]
- [49].Hassler S, Soininen L, Sjolander P, et al. Cancer among the Sami–a review on the Norwegian, Swedish and Finnish Sami populations. Int J Circumpolar Health. 2008. December;67(5):421–432. PubMed PMID: 19186763; eng. [DOI] [PubMed] [Google Scholar]
- [50].Breivik H, Collet B, Ventafridda V, et al. Survey of chronic pain in Europe: prevalence,impact on daily life, and treatment. Eur J Pain. 2006;10:287–333. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.