

Abstract
Background
The use of surgical drains has been considered mandatory after pancreatic surgery. The role of prophylactic abdominal drainage to reduce postoperative complications after pancreatic surgery is controversial.
Objectives
To assess the benefits and harms of routine abdominal drainage after pancreatic surgery, compare the effects of different types of surgical drains, and evaluate the optimal time for drain removal.
Search methods
For the initial version of this review, we searched the Cochrane Library (2015, Issue 3), MEDLINE (1946 to 9 April 2015), Embase (1980 to 9 April 2015), Science Citation Index Expanded (1900 to 9 April 2015), and Chinese Biomedical Literature Database (CBM) (1978 to 9 April 2015). For this updated review, we searched the Cochrane Library, MEDLINE, Embase, Science Citation Index Expanded, and CBM from 2015 to 28 August 2016.
Selection criteria
We included all randomized controlled trials that compared abdominal drainage versus no drainage in people undergoing pancreatic surgery. We also included randomized controlled trials that compared different types of drains and different schedules for drain removal in people undergoing pancreatic surgery.
Data collection and analysis
We identified five trials (of 985 participants) which met our inclusion criteria. Two review authors independently identified the trials for inclusion, collected the data, and assessed the risk of bias. We performed the meta‐analyses using Review Manager 5. We calculated the risk ratio (RR) for dichotomous outcomes and the mean difference (MD) for continuous outcomes with 95% confidence intervals (CI). For all analyses, we employed the random‐effects model.
Main results
Drain use versus no drain use
We included three trials involving 711 participants who were randomized to the drainage group (N = 358) and the no drainage group (N = 353) after pancreatic surgery. There was inadequate evidence to establish the effect of drains on mortality at 30 days (2.2% with drains versus 3.4% no drains; RR 0.78, 95% CI 0.31 to 1.99; three studies; low‐quality evidence), mortality at 90 days (2.9% versus 11.6%; RR 0.24, 95% CI 0.05 to 1.10; one study; low‐quality evidence), intra‐abdominal infection (7.3% versus 8.5%; RR 0.89, 95% CI 0.36 to 2.20; three studies; very low‐quality evidence), wound infection (12.3% versus 13.3%; RR 0.92, 95% CI 0.63 to 1.36; three studies; low‐quality evidence), morbidity (64.8% versus 62.0%; RR 1.04, 95% CI 0.93 to 1.16; three studies; moderate‐quality evidence), length of hospital stay (MD ‐0.66 days, 95% CI ‐1.60 to 0.29; three studies; moderate‐quality evidence), or additional open procedures for postoperative complications (11.5% versus 9.1%; RR 1.18, 95% CI 0.55 to 2.52; three studies). There was one drain‐related complication in the drainage group (0.6%).
Type of drain
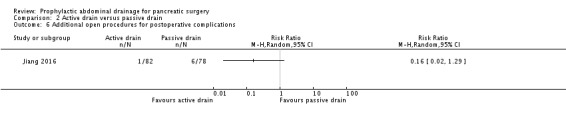
We included one trial involving 160 participants who were randomized to the active drain group (N = 82) and the passive drain group (N = 78) after pancreatic surgery. There was no evidence of differences between the two groups in mortality at 30 days (1.2% with active drain versus 0% with passive drain), intra‐abdominal infection (0% versus 2.6%), wound infection (6.1% versus 9.0%; RR 0.68, 95% CI 0.23 to 2.05), morbidity (22.0% versus 32.1%; RR 0.68, 95% CI 0.41 to 1.15), or additional open procedures for postoperative complications (1.2% versus 7.7%; RR 0.16, 95% CI 0.02 to 1.29). The active drain group was associated with shorter length of hospital stay (MD ‐1.90 days, 95% CI ‐3.67 to ‐0.13; 14.1% decrease of an 'average' length of hospital stay) than in the passive drain group. The quality of evidence was low, or very low.
Early versus late drain removal
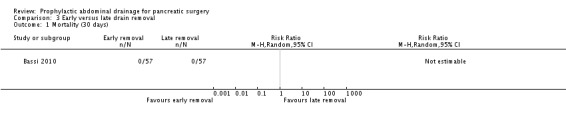
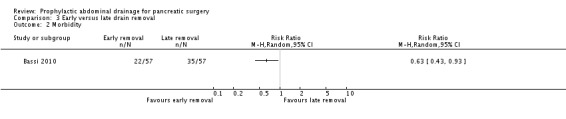
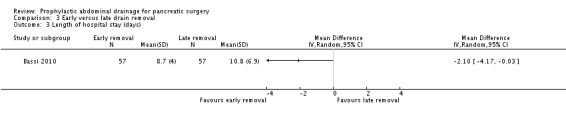
We included one trial involving 114 participants with a low risk of postoperative pancreatic fistula who were randomized to the early drain removal group (N = 57) and the late drain removal group (N = 57) after pancreatic surgery. There was no evidence of differences between the two groups in mortality at 30 days (0% for both groups) or additional open procedures for postoperative complications (0% with early drain removal versus 1.8% with late drain removal; RR 0.33, 95% CI 0.01 to 8.01). The early drain removal group was associated with lower rates of postoperative complications (38.5% versus 61.4%; RR 0.63, 95% CI 0.43 to 0.93), shorter length of hospital stay (MD ‐2.10 days, 95% CI ‐4.17 to ‐0.03; 21.5% decrease of an 'average' length of hospital stay), and hospital costs (17.0% decrease of 'average' hospital costs) than in the late drain removal group. The quality of evidence for each of the outcomes was low.
Authors' conclusions
It is unclear whether routine abdominal drainage has any effect on the reduction of mortality and postoperative complications after pancreatic surgery. In case of drain insertion, low‐quality evidence suggests that active drainage may reduce hospital stay after pancreatic surgery, and early removal may be superior to late removal for people with low risk of postoperative pancreatic fistula.
Keywords: Humans, Abdomen, Device Removal, Device Removal/adverse effects, Device Removal/mortality, Drainage, Drainage/methods, Length of Stay, Pancreas, Pancreas/surgery, Postoperative Complications, Postoperative Complications/mortality, Postoperative Complications/prevention & control, Randomized Controlled Trials as Topic, Time Factors
Drain use after pancreatic surgery
Review question
Is drain use able to reduce postoperative complications after pancreatic surgery?
Background
The use of surgical drains has been considered mandatory after pancreatic surgery. The role of drain use to reduce complications after pancreatic surgery (called postoperative complications) is controversial.
Study characteristics
We searched for all relevant, well‐conducted studies up to August 2016. We included five randomized controlled trials (an experiment in which participants are randomly allocated to two or more interventions, possibly including a control intervention or no intervention, and the results are compared). The five studies included 985 participants. Three of the five trials randomized 711 participants to drain use (number of participants (N) = 358) or no drain use (N = 353). One trial randomized 170 participants to active drain (suction drains under low or high pressure, N = 82) and passive drain (drains without suction, N = 78). One trial randomized 114 participants with low risk of postoperative pancreatic fistula (a complication during which the pancreas is disconnected from the nearby gut, and then reconnected to allow pancreatic juice containing digestive enzymes to enter the digestive system) to early drain removal (N = 57) and late drain removal (N = 57).
Key results
There was insufficient evidence to determine the effect on death (2.2% with drain use versus 3.4% with no drain use), infections in the abdomen (7.3% versus 8.5%), wound infections (12.3% versus 13.3%), overall complications (64.8% versus 62.0%), duration of hospital stay (14.3 days versus 13.8 days), or additional open procedures for postoperative complications (11.5% versus 9.1%) between drain use and no drain use. There was one drain‐related complication (the drainage tube was broken) in the drain use group (0.6%).
There was insufficient evidence to determine the effect on death (1.2% with active drain versus 0% with passive drain), infections in the abdomen (0% versus 2.6%), wound infections (6.1% versus 9.0%), overall complications (22.0% versus 32.1%), or additional open procedures for postoperative complications (1.2% versus 7.7%) between active drain and passive drain. Active drain was associated with shorter length of hospital stay (14.1% decrease of an 'average' duration of hospitalization) than passive drain.
Information on deaths following early or late removal of drains was available from one small study in which there were no deaths in either group. Rates of additional open procedures for postoperative complications were low (0% with early removal versus 1.8% with late removal). Early drain removal was associated with a lower complication rate (38.5% versus 61.4%), shorter duration of hospitalization (21.5% decrease of an 'average' duration of hospitalization), and lower hospital costs (17.0% decrease of 'average' hospital costs) than in the late drain removal.
It is not clear whether routine drain use has any effect on the reduction of death and postoperative complications after pancreatic surgery. In case of drain insertion, active drain appears to be associated with earlier discharge from hospital than passive drain after pancreatic surgery, and early removal appears to be better than late removal for people with a low risk of postoperative pancreatic fistula.
Quality of the evidence
All trials were at high risk of bias (suggesting the possibility of overestimating the benefits or underestimating the harms). Overall, the quality of the evidence varied from very low to moderate.
Summary of findings
Summary of findings for the main comparison.
Drain use versus no drain use for pancreatic surgery
| Drain use versus no drain use for pancreatic surgery | ||||||
| Patient or population: people undergoing elective open pancreatic resections Intervention: drain use versus no drain use | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| No drain use | Drain use | |||||
| Mortality (30 days) | Study population | RR 0.78 (0.31 to 1.99) | 711 (3 studies) | ⊕⊕⊝⊝ low1,2,3 | ‐ | |
| 34 per 1000 | 27 per 1000 (11 to 68) | |||||
| Moderate | ||||||
| 31 per 1000 | 24 per 1000 (10 to 62) | |||||
| Mortality (90 days) | Study population | RR 0.24 (0.05 to 1.1) | 134 (1 study) | ⊕⊕⊝⊝ low1,3,4 | ‐ | |
| 121 per 1000 | 29 per 1000 (6 to 133) | |||||
| Moderate | ||||||
| 121 per 1000 | 29 per 1000 (6 to 133) | |||||
| Intra‐abdominal infection | Study population | RR 0.89 (0.36 to 2.2) | 711 (3 studies) | ⊕⊝⊝⊝ very low1,2,3,5 | ‐ | |
| 85 per 1000 | 76 per 1000 (31 to 187) | |||||
| Moderate | ||||||
| 66 per 1000 | 59 per 1000 (24 to 145) | |||||
| Drain‐related complications | See comment | See comment | Not estimable | 179 (1 study) | ⊕⊕⊝⊝ low1,3,4 | There was 1 drain‐related complication in the drainage group. The drainage tube was broken. |
| Morbidity | Study population | RR 1.04 (0.93 to 1.16) | 711 (3 studies) | ⊕⊕⊕⊝ moderate1,3 | ‐ | |
| 620 per 1000 | 645 per 1000 (577 to 720) | |||||
| Moderate | ||||||
| 596 per 1000 | 620 per 1000 (554 to 691) | |||||
| Length of hospital stay | The mean length of hospital stay in the no drain group was 13.8 days | The mean length of hospital stay in the drain groups was 0.66 days lower (1.6 lower to 0.29 higher) | MD ‐0.66 (‐1.60 to 0.29) | 711 (3 studies) | ⊕⊕⊕⊝ moderate1,3 | ‐ |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; MD: mean difference; RR: risk ratio. | ||||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
1 Downgraded one level for serious risk of bias. 2 Downgraded one level for serious imprecision (the confidence interval of risk ratio overlapped 0.75 and 1.25, very few events). 3 Publication bias could not be assessed because of the few trials. 4 Downgraded one level for serious imprecision (small sample sizes, very few events). 5 Downgraded one level for serious heterogeneity.
Summary of findings 2.
Active drain versus passive drain for pancreatic surgery
| Active drain versus passive drain for pancreatic surgery | ||||||
| Patient or population: people undergoing elective open pancreatic resections Intervention: active drain versus passive drain | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Passive drain | Active drain | |||||
| Mortality (30 days) | Study population | RR 2.86 (0.12 to 69.06) | 160 (1 study) | ⊕⊝⊝⊝ very low1,2,3 | ‐ | |
| 0 per 1000 | 0 per 1000 (0 to 0) | |||||
| Moderate | ||||||
| 0 per 1000 | 0 per 1000 (0 to 0) | |||||
| Intra‐abdominal infection | Study population | RR 0.19 (0.01 to 3.9) | 160 (1 study) | ⊕⊝⊝⊝ very low1,2,3 | ‐ | |
| 26 per 1000 | 5 per 1000 (0 to 100) | |||||
| Moderate | ||||||
| 26 per 1000 | 5 per 1000 (0 to 101) | |||||
| Morbidity | Study population | RR 0.68 (0.41 to 1.15) | 160 (1 study) | ⊕⊕⊝⊝ low1,3,4 | ‐ | |
| 321 per 1000 | 218 per 1000 (131 to 369) | |||||
| Moderate | ||||||
| 321 per 1000 | 218 per 1000 (132 to 369) | |||||
| Length of hospital stay | The mean length of hospital stay in the passive drain was 14.5 days | The mean length of hospital stay in the active drain was 1.9 days lower (3.67 to 0.13 lower) | MD ‐1.90 (‐3.67 to ‐0.13) | 160 (1 study) | ⊕⊕⊝⊝ low1,3,5 | ‐ |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; MD: mean difference; RR: risk ratio. | ||||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
1 Downgraded one level for serious risk of bias. 2 Downgraded two levels for very serious imprecision (small sample sizes, very few events, confidence intervals of risk ratios overlapped 0.75 and 1.25). 3 Publication bias could not be assessed because of the few trials. 4 Downgraded one level for serious imprecision (small sample sizes, very few events). 5 Downgraded one level due to serious imprecision (total population size was less than 400).
Summary of findings 3.
Early versus late drain removal for pancreatic surgery
| Early versus late drain removal for pancreatic surgery | ||||||
| Patient or population: people undergoing elective open pancreatic resections Intervention: early versus late drain removal | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Late drain removal | Early drain removal | |||||
| Mortality (30 days) | See comment | See comment | Not estimable | 114 (1 study) | ⊕⊕⊝⊝ low1,2,3 | There was no mortality in either group. |
| Morbidity | Study population | RR 0.63 (0.43 to 0.93) | 114 (1 study) | ⊕⊕⊝⊝ low1,2,3 | ‐ | |
| 614 per 1000 | 387 per 1000 (264 to 571) | |||||
| Moderate | ||||||
| 614 per 1000 | 387 per 1000 (264 to 571) | |||||
| Length of hospital stay (days) | The mean length of hospital stay in the late removal group was 10.8 days | The mean length of hospital stay in the early removal group was 2.1 days lower (4.17 to 0.03 lower) | MD ‐2.10 (‐4.17 to ‐0.03) | 114 (1 study) | ⊕⊕⊝⊝ low1,2,4 | ‐ |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; MD: mean difference; RR: risk ratio. | ||||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
1 Downgraded one level due to serious risk of bias. 2 Publication bias could not be assessed because of the few trials. 3 Downgraded one level for serious imprecision (small sample sizes, very few events). 4 Downgraded one level due to serious imprecision (total population size was fewer than 400).
Background
Description of the condition
See 'Glossary' for an explanation of terms (Appendix 1).
Pancreatic cancer ranks 13th in terms of the most common cancers and eighth as the cause of cancer death from a global viewpoint (Anderson 2006; Lowenfels 2006). Regional differences exist in the incidence, and the number of new cases diagnosed per year (Anderson 2006). The overall incidence of pancreatic cancer is approximately 4 to 10 cases per 100,000 people per year (Dragovich 2011). The most common cause of pancreatic cancer is heavy tobacco usage (Lowenfels 2006).
Although the exact incidence of chronic pancreatitis worldwide is unknown, the estimated incidence of chronic pancreatitis is 6 cases per 100,000 people per year in Europe and probably all western countries (Spanier 2008). The prevalence of chronic pancreatitis in the UK, France, Japan, and south India is 3 cases, 26 cases, 4 cases, and 114 to 200 cases per 100,000 people, respectively (Bornman 2001; Braganza 2011; Garg 2004; Lévy 2006). The most common cause of chronic pancreatitis is alcohol abuse (Braganza 2011; Spanier 2008).
Pancreatic surgery is performed to treat various pancreatic and extra‐pancreatic diseases, including pancreatic cancers, chronic pancreatitis, biliary and duodenal malignancy, etc. (Cheng 2013a; Cheng 2014; Cheng 2016; Connor 2005; Gurusamy 2013). Although mortality of pancreatic surgery has been reduced to less than 5% currently, overall morbidity is still high, ranging from 30% to 60% (Bassi 2005; Connor 2005; Giovinazzo 2011; Gurusamy 2013; Wente 2007a; Wente 2007b). The most common complications after pancreatic surgery include delayed gastric emptying (19% to 23%) (Wente 2007a; Wente 2007b), pancreatic fistula (2% to 30%; Bassi 2005; Cheng 2016; Hackert 2011; Wente 2007a; Wente 2007b), intra‐abdominal abscess (9% to 10%; Wente 2007a; Wente 2007b), wound infection (5% to 15%; Andrén‐Sandberg 2011; Halloran 2002), and postoperative bleeding (1% to 8%; Wente 2007a; Wente 2007b).
Description of the intervention
As a measure to reduce postoperative complications, prophylactic drains are traditionally placed in the subhepatic space near both the biliary and pancreatic anastomoses after pancreatic resections (Conlon 2001; Fisher 2011). Abdominal drainage has been in use for over 1000 years (Memon 2001).
Surgical drains are artificial tubes used to remove blood, pus, or other body fluids from wounds (Durai 2009). There are two main types of surgical drains: open and closed (Cheng 2015; Durai 2009; Gurusamy 2007a; Wang 2011). An open drain communicates with the atmosphere (e.g. corrugated drain, Penrose drain, sump drain; Durai 2009; Gurusamy 2007a; Wang 2011). A closed drain consists of a tube that drains into a collection bag or bottle where the contents are not exposed to the atmosphere (Durai 2009; Gurusamy 2007a; Wang 2011). Closed drains may be either active (suction drains under low or high pressure; e.g. Jackson‐Pratt drain, Redivac) or passive (drains without suction; e.g. Robinson drain, Pigtail drain; Durai 2009; Gurusamy 2007a; Wang 2011).
How the intervention might work
Surgeons have routinely used drains after pancreatic surgery because of the possible collection of bile, pancreatic juice, or blood, which may require additional procedures (Adham 2013; Bassi 2010; Conlon 2001; Correa‐Gallego 2013; Fisher 2011; Giovinazzo 2011; Heslin 1998; Jeekel 1992; Kawai 2006; Lim 2013; Mehta 2013; Paulus 2012; Van Buren 2014). The primary reasons for placing abdominal drains after pancreatic resections are: 1. drainage of established intra‐abdominal collections (e.g. bile, pancreatic juice, pus); 2. prevention of further fluid accumulation; and 3. identification and monitoring of any fistula or bleeding (Adham 2013; Bassi 2010; Conlon 2001; Correa‐Gallego 2013; Fisher 2011; Giovinazzo 2011; Heslin 1998; Jeekel 1992; Kawai 2006; Lim 2013; Mehta 2013; Paulus 2012; Van Buren 2014). Theoretically, abdominal drainage has the potential to prevent or control postoperative complications (e.g. intra‐abdominal abscess, pancreatic or biliary fistula, bleeding; Adham 2013; Bassi 2010; Conlon 2001; Correa‐Gallego 2013; Fisher 2011; Giovinazzo 2011; Heslin 1998; Jeekel 1992; Kawai 2006; Lim 2013; Mehta 2013; Paulus 2012; Van Buren 2014). The use of surgical drains has been considered mandatory after pancreatic surgery since the mid‐1930s (Allen 2011).
However, some surgeons have argued that abdominal drainage may fail to reduce postoperative complications because a drain may become sealed off and ineffective within a few days after pancreatic surgery (Heslin 1998; Paulus 2012). The drain itself appears to act as a foreign body and may interfere with wound healing (Correa‐Gallego 2013; Fisher 2011; Paulus 2012). The drainage tube creates a pathway for contamination and may increase the risk of postoperative infectious complications (Inoue 2011; Jeekel 1992). In addition, the use of a drain may be associated with an increased length of hospital stay (Fisher 2011; Mehta 2013; Paulus 2012). Moreover, abdominal drainage may be associated with some rare adverse events such as bowel perforation, hernia, and bleeding (Cameron‐Strange 1985; Henkus 1999; Makama 2010; Nomura 1998; Reed 1992; Sahu 2008; Srivastava 2007; Van Hee 1983). Studies have suggested that routine placement of prophylactic abdominal drains may be unnecessary and may be associated with an increased complication rate (Adham 2013; Correa‐Gallego 2013; Fisher 2011; Giovinazzo 2011; Heslin 1998; Jeekel 1992; Lim 2013; Mehta 2013; Paulus 2012).
Why it is important to do this review
Routine use of prophylactic abdominal drainage in people undergoing pancreatic surgery is controversial. This is an update of a previous Cochrane Review assessing the role of prophylactic abdominal drainage for pancreatic surgery.
Objectives
To assess the benefits and harms of routine abdominal drainage after pancreatic surgery, compare the effects of different types of surgical drains, and evaluate the optimal time for drain removal.
Methods
Criteria for considering studies for this review
Types of studies
We included all randomized controlled trials (RCTs), regardless of sample size, language, or publication status, that compared 1. drain use versus no drain use, 2. different types of drains, or 3. different schedules for drain removal in people undergoing pancreatic surgery. We excluded quasi‐randomized trials, in which the allocation was performed on the basis of a pseudo‐random sequence (e.g. odd/even hospital number or date of birth, alternation, and non‐randomized studies) because of the potential for bias (Reeves 2011).
Types of participants
We included people, regardless of age, sex, or race, who underwent elective pancreatic resections (open or laparoscopic) for any pancreatic or extra‐pancreatic disease.
Types of interventions
Drain use versus no drain use.
One type of drain versus another.
Early versus late drain removal (no more than four days versus more than four days).
Types of outcome measures
Primary outcomes
-
Mortality:
30‐day mortality;
90‐day mortality.
-
Infectious complications:
intra‐abdominal infection;
wound infection.
Drain‐related complications.
Secondary outcomes
Morbidity as defined by study authors. We classified morbidity by the Clavien‐Dindo classification of surgical complications (Clavien 2009).
Length of hospital stay.
Hospital costs.
-
Additional procedures for postoperative complications:
open procedures;
radiological interventions (radiological drainage requiring insertion of drain or percutaneous aspiration).
Pain, quality of life.
The main reason to justify abdominal drainage was the assumption that it would reduce the infectious complication rate and subsequent mortality and morbidity rates. Other clinical outcomes were chosen to assess whether abdominal drainage results in earlier discharge from hospital, fewer reoperations, and improvement in health‐related quality of life and cost effectiveness.
Reporting of the outcomes listed here was not an inclusion criterion for the review.
Search methods for identification of studies
We designed the search strategies with the help of a Cochrane Upper Gastrointestinal and Pancreatic Diseases (UGPD) Information Specialist before searching. We placed no restrictions on the language of publication when searching the electronic databases or reviewing reference lists in identified studies.
Electronic searches
For the initial version of this review, we searched the Cochrane Library (2015, Issue 3), MEDLINE (1946 to 9 April 2015), Embase (1980 to 9 April 2015), Science Citation Index Expanded (1900 to 9 April 2015), and Chinese Biomedical Literature Database (CBM) (1978 to 9 April 2015) (Peng 2015). For this updated review, we searched the following electronic databases from 2015 to 28 August 2016 with no language or date of publication restrictions:
the Cochrane Library (2016, Issue 8) (Appendix 2);
MEDLINE (Ovid) (2015 to 28 August 2016) (Appendix 3);
Embase (Ovid) (2015 to 28 August 2016) (Appendix 4);
Science Citation Index Expanded (Web of Science) (2015 to 28 August 2016) (Appendix 5); and
Chinese Biomedical Literature Database (CBM) (2015 to 28 August 2016) (Appendix 6).
Searching other resources
We checked reference lists of all primary studies and review articles for additional references. We contacted authors of identified trials and ask them to identify other published and unpublished studies.
We searched PubMed for errata or retractions from eligible trials and reported the date this was done within the review (www.ncbi.nlm.nih.gov/pubmed). We also searched the meeting abstracts via the Society of American Gastrointestinal and Endoscopic Surgeons (SAGES; www.sages.org/; accessed 30 August 2016) and Conference Proceedings Citation Index to explore further relevant clinical trials.
Clinical trials registers/trial result registers
We searched the following databases to identify ongoing trials (accessed 30 August 2016):
World Health Organization International Clinical Trials Registry Platform search portal (apps.who.int/trialsearch/);
ClinicalTrials.gov (www.clinicaltrials.gov/);
Current Controlled Trials (www.controlled‐trials.com/);
European (EU) Clinical Trials Register (www.clinicaltrialsregister.eu/);
Chinese Clinical Trial Register (www.chictr.org/).
Data collection and analysis
We conducted this systematic review according to the Cochrane Handbook for Systematic Reviews of Intervention (Higgins 2011) and the Cochrane UGPD Group Module (Forman 2011).
Selection of studies
Two review authors (ML, JX) independently screened titles and abstracts for inclusion all the studies we identified as a result of the search and coded them as 'retrieve' (eligible or potentially eligible/unclear) or 'do not retrieve'. We retrieved the full‐text study reports/publications and two review authors (ML, JX) independently screened the full text and identified studies for inclusion, and identified and recorded reasons for exclusion of the ineligible studies. We resolved any disagreements through discussion or, if required, we consulted a third review author (YC). We identified and excluded duplicates and collated multiple reports of the same study, so that each study rather than each report was the unit of interest in the review. We recorded the selection process in sufficient detail to complete a PRISMA flow diagram and a Characteristics of excluded studies table (Moher 2009).
Data extraction and management
We used a standard data collection form for study characteristics and outcome data, which had been piloted on at least one study in the review. Two review authors (ML, JX) extracted the following study characteristics from included studies:
methods: study design, total duration study and run in, number of study centres and location, study setting, withdrawals, and date of study;
participants: number (N), mean age, age range, gender, severity of condition, diagnostic criteria, inclusion criteria, and exclusion criteria;
interventions: intervention, comparison;
outcomes: primary and secondary outcomes specified and collected, time points reported;
notes: funding for trial, notable conflicts of interest of trial authors.
Two review authors (ML, JX) independently extracted outcome data from included studies. We noted in the Characteristics of included studies table if outcome data were not reported in a usable way. We resolved disagreements by consensus or by involving a third review author (YC). One review author (SH) copied across the data from the data collection form into Review Manager 5. We double checked that the data were entered correctly by comparing the study reports with how the data were presented in the systematic review. A second review author spot‐checked study characteristics for accuracy against the trial report.
Assessment of risk of bias in included studies
Two review authors (NC, SH) independently assessed risk of bias for each study using the criteria outlined in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). We resolved any disagreements by discussion or by involving a third review author (YC). We assessed the risk of bias according to the following domains:
random sequence generation;
allocation concealment;
blinding of outcome assessment;
incomplete outcome data;
selective outcome reporting;
other bias.
We graded each potential source of bias as high, low, or unclear risk, and provided a quote from the study report together with a justification for our judgement in the 'Risk of bias' table. We summarized the 'Risk of bias' judgements across different studies for each of the domains listed. We considered blinding separately for different key outcomes where necessary (e.g. for unblinded outcome assessment, risk of bias for all‐cause mortality may be very different than for a participant‐reported pain scale). Where information on risk of bias related to unpublished data or correspondence with a trialist, we noted this in the 'Risk of bias' table.
When considering treatment effects, we took into account the risk of bias for the studies that contributed to that outcome.
Assessment of bias in conducting the systematic review
We conducted the review according to the published protocol (Cheng 2013b), and reported any deviations from it in the 'Differences between protocol and review' section of the systematic review.
Measures of treatment effect
We analysed dichotomous data as risk ratio (RR) and continuous data as mean difference (MD) or standardized mean difference (SMD) with 95% confidence intervals (CI). We ensured that higher scores for continuous outcomes had the same meaning for the particular outcome, explained the direction to the reader and reported where the directions were reversed if this was necessary.
We undertook meta‐analyses only where this was meaningful, that is, if the treatments, participants, and underlying clinical question were similar enough for pooling to make sense.
A common way that trialists indicated when they had skewed data was by reporting medians and interquartile ranges. When we encountered this, we noted that the data were skewed and considered the implication of this.
Where multiple trial arms were reported in a single trial, we included only the relevant arms. If two comparisons (e.g. drug A versus placebo and drug B versus placebo) were entered into the same meta‐analysis, we halved the control group to avoid double counting.
Unit of analysis issues
The unit of analysis was the individual participant. We did not find any cross‐over or cluster‐randomized trials.
Dealing with missing data
We contacted investigators or study sponsors in order to verify key study characteristics and obtained missing numerical outcome data where possible (e.g. when a study was identified as abstract only). However, there was no reply. Thus, we used only the available data in the analyses.
Assessment of heterogeneity
We used the I2 statistic to measure heterogeneity among the trials in each analysis (Higgins 2003). When we identified substantial heterogeneity (greater than 50%), we explored it by prespecified subgroup analysis, and we interpreted summary effect measures with caution.
Assessment of reporting biases
We did not perform funnel plots to assess reporting biases because the number of trials included was fewer than 10 (Sterne 2011).
Data synthesis
We performed the meta‐analyses using Review Manager 5 software (RevMan 2014). Two review authors (NC, SH) independently checked and entered all of the data into Review Manager 5. We resolved any discrepancy between the two review authors by discussion. For all analyses, we employed a random‐effects model.
'Summary of findings' table
We created 'Summary of findings' tables using the following outcomes: mortality, intra‐abdominal infection, drain‐related complications, morbidity, and length of hospital stay. We used the five GRADE considerations (study limitations, consistency of effect, imprecision, indirectness, and publication bias) to assess the quality of a body of evidence as it related to the studies which contributed data to the meta‐analyses for the prespecified outcomes. We used the methods and recommendations described in Section 8.5 and Chapter 12 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011), and used GRADEpro software (GRADEpro 2015). We justified all decisions to downgrade or upgrade the quality of studies using footnotes, and made comments to aid the reader's understanding of the review where necessary. We considered whether there was any additional outcome information that we were unable to incorporate into meta‐analyses and noted this in the comments, and stated if it supported or contradicted the information from the meta‐analyses.
Subgroup analysis and investigation of heterogeneity
We had intended to perform the following subgroup analyses, but were unable to because of limited data:
RCTs with low risk of bias versus RCTs with high risk of bias;
different aetiologies (pancreatic cancer, chronic pancreatitis, and others);
type of operation (proximal, distal, and central pancreatectomy).
Sensitivity analysis
We intended to perform sensitivity analyses defined a priori to assess the robustness of our conclusions. This involved:
changing between a fixed‐effect model and a random‐effects model;
changing between RR, risk differences (RD), and odds ratios (OR) for dichotomous outcomes;
changing between MD and SMD for continuous outcomes;
changing between worst‐case scenario analysis and best‐case scenario analysis for missing data.
If the results did not change, they were considered to have low sensitivity. If the results changed, they were considered to have high sensitivity.
Reaching conclusions
We based our conclusions only on findings from the quantitative or narrative synthesis of included studies for this review. We avoided making recommendations for practice and our implications for research could give the reader a clear sense of where the focus of any future research in the area should be and what the remaining uncertainties were.
Results
Description of studies
See: Characteristics of included studies; Characteristics of excluded studies tables.
Results of the search
In this updated review, we identified 276 records through the electronic searches of the Cochrane Library (16 records), MEDLINE (Ovid) (47 records), Embase (Ovid) (135 records), Science Citation Index Expanded (Web of Science) (71 records), and Chinese Biomedical Literature Database (CBM) (7 records). We did not identify any records through scanning reference lists of the identified RCTs. We excluded 39 duplicates and 234 clearly irrelevant records through reading titles and abstracts. The remaining three records were retrieved for further assessment. We excluded one study for the reasons listed in the Characteristics of excluded studies table. In total, two RCTs fulfilled the inclusion criteria for this update. The study flow diagram is shown in Figure 1.
Figure 1.
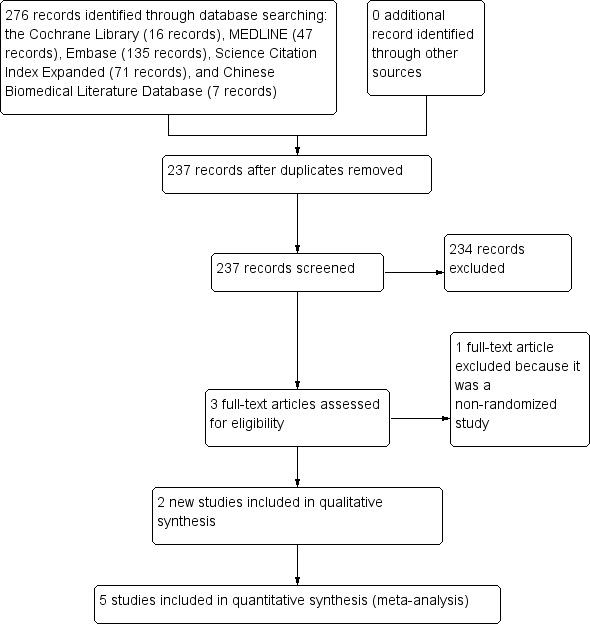
Study flow diagram.
Included studies
The first published version of this review from 2015 included three trials published between 2001 and 2014 (Bassi 2010; Conlon 2001; Van Buren 2014). We added two recent studies published in 2016 into this updated review (Jiang 2016; Witzigmann 2016). Therefore, we included five trials and all of these provided data for the analyses. Details of the trials are shown in the Characteristics of included studies table.
Drain use versus no drain use
Three studies randomized 711 participants who underwent elective pancreatic resections (604 pancreaticoduodenectomy, 40 distal pancreatectomy, and 67 other pancreatic surgery) to those who had drainage tubes inserted postoperatively (N = 358) and those who did not (N = 353). Two of these studies were conducted in the USA (Conlon 2001; Van Buren 2014), and one in Germany (Witzigmann 2016). The mean age was 63.9 years. One or two drainage tubes were placed near both the biliary and pancreatic anastomoses. These trials measured mortality, morbidity, wound infection, intra‐abdominal infection, various postoperative complications, reoperation, additional radiological intervention, and length of hospital stay (Conlon 2001; Van Buren 2014; Witzigmann 2016).
One type of drain versus another
One study randomized 160 participants undergoing elective pancreaticoduodenectomy to the active drain group or the passive drain group (Jiang 2016). This trial was conducted in China. One drainage tube was placed near both the biliary and pancreatic anastomoses. The mean age was 59.6 years. The outcomes reported were mortality, morbidity, wound infection, intra‐abdominal infection, various postoperative complications, reoperation, operation time, and length of hospital stay.
Early versus late drain removal
One study randomized 114 participants with low risk of postoperative pancreatic fistula undergoing elective pancreatic resections (75 pancreaticoduodenectomy and 39 distal pancreatectomy) to the early drain removal group or the late drain removal group (Bassi 2010). This trial was conducted in Italy. Two drainage tubes were placed near both the biliary and pancreatic anastomoses. One drainage tube was placed near the pancreatic stump after distal pancreatectomy. The mean age was 56.6 years. The outcomes reported were pancreatic fistula, abdominal complications, pulmonary complications, reoperation, length of hospital stay, hospital readmission, postoperative mortality, morbidity, and hospital costs.
Excluded studies
We excluded 11 studies. Details are listed in the Characteristics of excluded studies table. One trial was excluded because it focused on pancreatic duct drainage (Lee 2009); the rest were not RCTs.
Ongoing studies
We found one ongoing study (Čečka 2015). Two hundred and twenty‐three participants undergoing pancreatic resection will be randomized to closed suction drain or closed gravity drain. This trial is currently recruiting participants, being performed in Czech Republic, and was initiated in October 2013. The primary outcome is the rate of rate of postoperative pancreatic fistula. The secondary outcomes are postoperative morbidity, including wound infection, intra‐abdominal collections, delayed gastric emptying, postoperative haemorrhage, pneumonia, abdominal rupture, cardiac events, and neurological complications.
Risk of bias in included studies
Figure 2 and Figure 3 show the risk of bias of the included studies. All five trials were at high risk of bias (Bassi 2010; Conlon 2001; Jiang 2016; Van Buren 2014; Witzigmann 2016).
Figure 2.
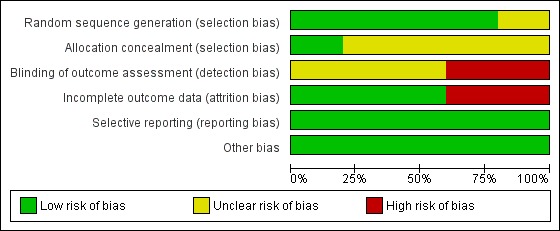
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
Figure 3.
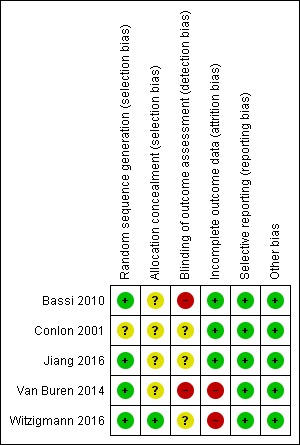
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Allocation
Random sequence generation was at low risk of bias in four trials (Bassi 2010; Jiang 2016; Van Buren 2014; Witzigmann 2016). Allocation concealment was at low risk of bias in one trial (Witzigmann 2016).
Blinding
Blinding of outcome assessment was at high risk of bias in two trials (Bassi 2010; Van Buren 2014).
Incomplete outcome data
There were no postrandomization dropouts in three trials (Bassi 2010; Conlon 2001; Jiang 2016). There were some dropouts in two trials, but the data were not analyzed on an intention‐to‐treat basis (Van Buren 2014; Witzigmann 2016). Thus both trials were at high risk of bias regarding incomplete outcome data (Van Buren 2014; Witzigmann 2016).
Selective reporting
The trial protocol was available for three trials (Bassi 2010; Van Buren 2014; Witzigmann 2016). All of the studies' prespecified outcomes were reported. Thus, these three trials were considered to be free of selective reporting. The other two trials reported all of the primary outcomes of this review (Conlon 2001; Jiang 2016). There was some selective outcome reporting in the secondary outcomes, but the review authors considered the trial to be free of selective reporting for the primary outcomes.
Other potential sources of bias
Baseline imbalance was at low risk of bias in all five trials.
Effects of interventions
See: Table 1; Table 2; Table 3
See: Table 1; Table 2; Table 3.
Drain use versus no drain use
Three trials (711 participants) compared drain use with no drain use (Conlon 2001; Van Buren 2014; Witzigmann 2016). Three hundred and fifty‐eight participants were randomized to the drainage group and 358 participants to the no drainage group. See: Table 1.
Mortality (30 days)
Three trials (711 participants) reported this outcome. The mean 30‐day mortality was 2.8% (2.2% with drain use versus 3.4% with no drain use). There was no significant difference in 30‐day mortality between groups (RR 0.78, 95% CI 0.31 to 1.99; P = 0.60; I2 = 2%; P = 0.36) (Analysis 1.1).
Analysis 1.1.
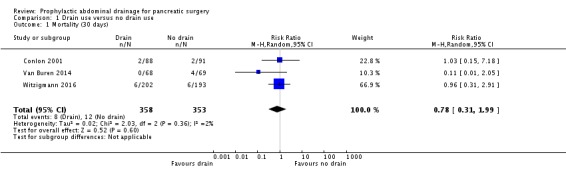
Comparison 1 Drain use versus no drain use, Outcome 1 Mortality (30 days).
Mortality (90 days)
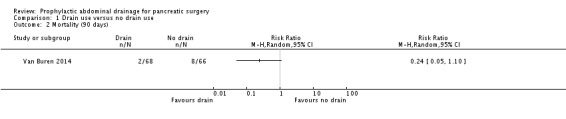
One trial (137 participants) reported this outcome. The mean 90‐day mortality was 7.3% (2.9% with drain use versus 11.6% with no drain use). There was no significant difference in 90‐day mortality between groups (RR 0.24, 95% CI 0.05 to 1.10; P = 0.07) (Analysis 1.2).
Analysis 1.2.
Comparison 1 Drain use versus no drain use, Outcome 2 Mortality (90 days).
Intra‐abdominal infection
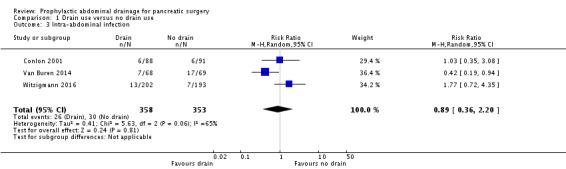
Three trials (711 participants) reported this outcome. The mean intra‐abdominal infection rate was 7.9% (7.3% with drain use versus 8.5% with no drain use). There was no significant difference in intra‐abdominal infection rate between groups (RR 0.89, 95% CI 0.36 to 2.20; P = 0.81; I2 = 65%; P = 0.06) (Analysis 1.3).
Analysis 1.3.
Comparison 1 Drain use versus no drain use, Outcome 3 Intra‐abdominal infection.
Wound infection
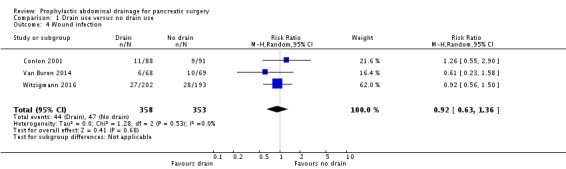
Three trials (711 participants) reported this outcome. The mean wound infection rate was 12.8% (12.3% with drain use versus 13.3% with no drain use). There was no significant difference in wound infection rate between groups (RR 0.92, 95% CI 0.63 to 1.36; P = 0.68; I2 = 0%; P = 0.53) (Analysis 1.4).
Analysis 1.4.
Comparison 1 Drain use versus no drain use, Outcome 4 Wound infection.
Drain‐related complications
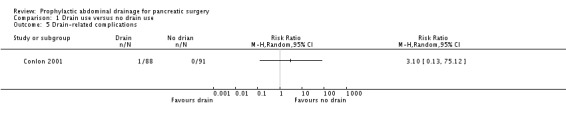
One trial (179 participants) reported this outcome. There was one drain‐related complication (broken drain) in the drainage group (Conlon 2001) (Analysis 1.5).
Analysis 1.5.
Comparison 1 Drain use versus no drain use, Outcome 5 Drain‐related complications.
Morbidity
Three trials (711 participants) reported this outcome. The mean morbidity was 63.4% (64.8% with drain use versus 62.0% with no drain use). There was no significant difference in morbidity between groups (RR 1.04, 95% CI 0.93 to 1.16; P = 0.51; I2 = 0%; P = 0.73) (Analysis 1.6).
Analysis 1.6.
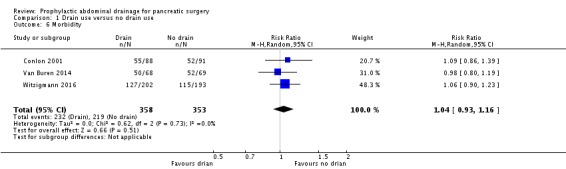
Comparison 1 Drain use versus no drain use, Outcome 6 Morbidity.
Length of hospital stay
Three trials (711 participants) reported this outcome. The mean hospital stay was 14.0 days (14.3 days with drain use versus 13.8 days with no drain use). There was no significant difference in length of hospital stay between groups (MD ‐0.66 days, 95% CI ‐1.60 to 0.29; P = 0.17; I2 = 22%; P = 0.28) (Analysis 1.7).
Analysis 1.7.
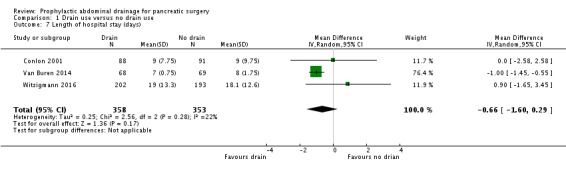
Comparison 1 Drain use versus no drain use, Outcome 7 Length of hospital stay (days).
Hospital costs
None of the trials reported this outcome.
Additional open procedures for postoperative complications
Three trials (711 participants) reported this outcome. A total of 73 participants needed additional open procedures for postoperative complications (41 with drain use versus 32 with no drain use). There was no significant difference in need for additional open procedures between groups (RR 1.18, 95% CI 0.55 to 2.52; P = 0.67; I2 = 43%; P = 0.18) (Analysis 1.8).
Analysis 1.8.

Comparison 1 Drain use versus no drain use, Outcome 8 Additional open procedures for postoperative complications.
Additional radiological interventions for postoperative complications
Two trials (316 participants) reported this outcome. A total of 40 participants need additional radiological interventions for postoperative complications (17 with drain use versus 23 with no drain use). There was no significant difference in need for additional radiological interventions between groups (RR 0.78, 95% CI 0.19 to 3.25; P = 0.74; I2 = 80%; P = 0.02) (Analysis 1.9).
Analysis 1.9.
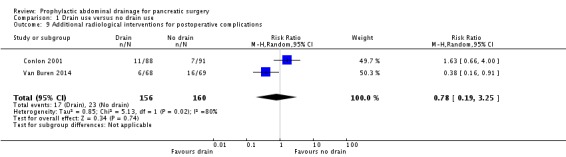
Comparison 1 Drain use versus no drain use, Outcome 9 Additional radiological interventions for postoperative complications.
Pain/quality of life
None of the trials reported this outcome.
Active drain versus passive drain
One trial (160 participants) compared active drain versus passive drain (Jiang 2016). Eighty‐two participants were randomized to the active drain group and 78 participants to the passive drain group. See: Table 2.
Mortality (30 days)
The mean mortality was 0.6% (1.2% with active drain versus 0% with passive drain). There was no significant difference in 30‐day mortality between groups (RR 2.86, 95% CI 0.12 to 69.06; P = 0.52) (Analysis 2.1).
Analysis 2.1.
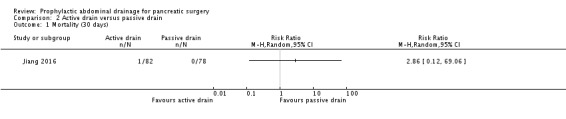
Comparison 2 Active drain versus passive drain, Outcome 1 Mortality (30 days).
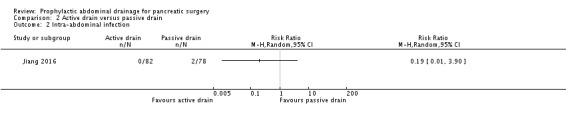
Intra‐abdominal infection
The mean intra‐abdominal infection rate was 1.3% (0% with active drain versus 2.6% with passive drain). There was no significant difference in intra‐abdominal infection rate between groups (RR 0.19, 95% CI 0.01 to 3.90; P = 0.28) (Analysis 2.2).
Analysis 2.2.
Comparison 2 Active drain versus passive drain, Outcome 2 Intra‐abdominal infection.
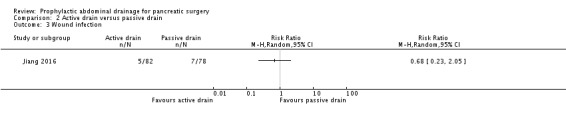
Wound infection
The mean wound infection rate was 7.5% (6.1% with active drain versus 9.0% with passive drain). There was no significant difference in wound infection rate between groups (RR 0.68, 95% CI 0.23 to 2.05; P = 0.49) (Analysis 2.3).
Analysis 2.3.
Comparison 2 Active drain versus passive drain, Outcome 3 Wound infection.
Drain‐related complications
The trial did not report this outcome.
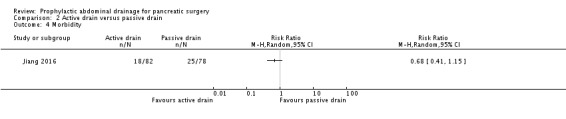
Morbidity
The mean morbidity was 26.9% (22.0% with active drain versus 32.1% with passive drain). There was no significant difference in morbidity between groups (RR 0.68, 95% CI 0.41 to 1.15; P = 0.51) (Analysis 2.4).
Analysis 2.4.
Comparison 2 Active drain versus passive drain, Outcome 4 Morbidity.
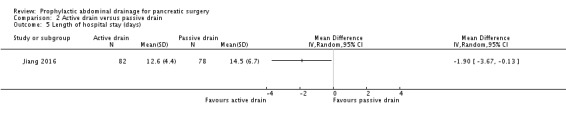
Length of hospital stay
The mean hospital stay was 13.5 days. The length of hospital stay was shorter in the active drain group (12.6 days) than in the passive drain group (14.5 days) (MD ‐1.90 days, 95% CI ‐3.67 to ‐0.13; P = 0.03) (Analysis 2.5).
Analysis 2.5.
Comparison 2 Active drain versus passive drain, Outcome 5 Length of hospital stay (days).
Hospital costs
The trial did not report this outcome.
Additional open procedures for postoperative complications
Seven participants needed additional open procedures for postoperative complications (1 with active drain versus 6 with passive drain). There was no significant difference in need for additional open procedures between groups (RR 0.16, 95% CI 0.02 to 1.29; P = 0.08) (Analysis 2.6).
Analysis 2.6.
Comparison 2 Active drain versus passive drain, Outcome 6 Additional open procedures for postoperative complications.
Additional radiological interventions for postoperative complications
The trial did not report this outcome.
Pain/quality of life
The trial did not report these outcomes.
Early versus late drain removal
One trial (114 participants with low risk of postoperative pancreatic fistula) compared early versus late drain removal (Bassi 2010). Fifty‐seven participants were randomized to the early drain removal group and 57 participants to the late drain removal group. See: Table 3.
Mortality (30 days)
There was no mortality in either group (Analysis 3.1).
Analysis 3.1.
Comparison 3 Early versus late drain removal, Outcome 1 Mortality (30 days).
Intra‐abdominal infection
The trial did not report this outcome
Wound infection
The trial did not report this outcome
Drain‐related complications
The trial did not report this outcome.
Morbidity
The mean morbidity was 50% (38.5% with early drain removal versus 61.4% with late drain removal). The morbidity was lower in the early drain removal group than in the late drain removal group (RR 0.63, 95% CI 0.43 to 0.93; P = 0.02) (Analysis 3.2).
Analysis 3.2.
Comparison 3 Early versus late drain removal, Outcome 2 Morbidity.
Length of hospital stay
The mean hospital stay was 9.8 days. The length of hospital stay was shorter in the early drain removal group (8.7 days) than in the late drain removal group (10.8 days) (MD ‐2.10 days, 95% CI ‐4.17 to ‐0.03; P = 0.05) (Analysis 3.3).
Analysis 3.3.
Comparison 3 Early versus late drain removal, Outcome 3 Length of hospital stay (days).
Hospital costs
The total hospital costs were lower in the early drain removal group (10,071 Euros) than in the late drain removal group (EUR 12,140) (MD ‐EUR 2069.00, 95% CI ‐3872.26 to ‐265.74; P = 0.02) (Analysis 3.4).
Analysis 3.4.
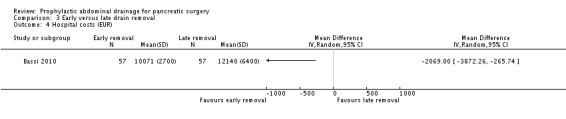
Comparison 3 Early versus late drain removal, Outcome 4 Hospital costs (EUR).
Additional open procedures for postoperative complications
One participant needed an additional open procedure for postoperative complications (0 with early drain removal versus 1 with late drain removal). There was no significant difference in need for additional open procedures between groups (RR 0.33, 95% CI 0.01 to 8.01; P = 0.50) (Analysis 3.5).
Analysis 3.5.
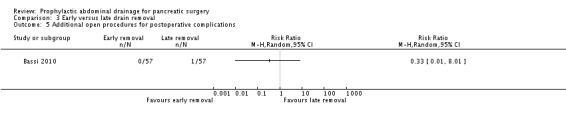
Comparison 3 Early versus late drain removal, Outcome 5 Additional open procedures for postoperative complications.
Additional radiological interventions for postoperative complications
The trial did not report this outcome.
Pain/quality of life
The trial did not report these outcomes.
Subgroup analysis
We did not perform any of the planned subgroup analyses because this review included only five trials.
Sensitivity analysis
We performed the following planned sensitivity analyses:
changing between a fixed‐effect model and a random‐effects model;
changing statistics among RR, RD, and OR for dichotomous outcomes;
changing statistics between MD and SMD for continuous outcomes;
changing between worst‐case scenario analysis and best‐case scenario analysis for missing data.
We observed no change in the results by changing between a fixed‐effect and a random‐effects model, calculating the RD and OR for dichotomous outcomes, or calculating the SMD for continuous outcomes. There were 46 postrandomization dropouts in two trials. We observed no change in the results by changing between worst‐case scenario analysis and best‐case scenario analysis for missing data except for the outcome 'mortality (90 days)' (Analysis 4.1; Analysis 4.2).
Analysis 4.1.
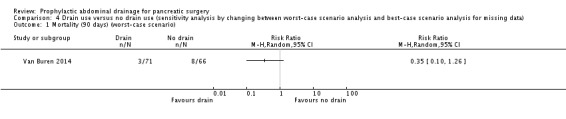
Comparison 4 Drain use versus no drain use (sensitivity analysis by changing between worst‐case scenario analysis and best‐case scenario analysis for missing data), Outcome 1 Mortality (90 days) (worst‐case scenario).
Analysis 4.2.
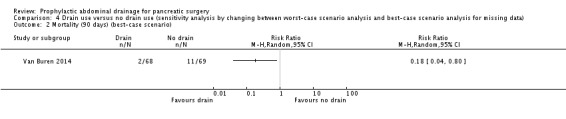
Comparison 4 Drain use versus no drain use (sensitivity analysis by changing between worst‐case scenario analysis and best‐case scenario analysis for missing data), Outcome 2 Mortality (90 days) (best‐case scenario).
Discussion
Summary of main results
For the comparison of drain use with no drain use, we found that there were no clear differences in any of the primary outcomes measured. Drains may lead to drain‐related complications. For the comparison of active drain with passive drain, we found that active drain was associated with earlier discharge from hospital than passive drain. Data comparing early versus late drain removal were available from only one trial. We found that they favoured early drain removal for people with low risk of postoperative pancreatic fistula.
The routine use of drains has been considered surgical dogma after a pancreatic resection. Jeekel and coworkers first challenged the dogma in the 1990s (Jeekel 1992). They reported a cohort in which 22 people underwent pancreaticoduodenectomy without undue complications after abandoning abdominal drainage. They concluded that abdominal drainage after pancreaticoduodenectomy may be omitted. Since then, several non‐randomized studies (Adham 2013; Correa‐Gallego 2013; Fisher 2011; Giovinazzo 2011; Heslin 1998; Kawai 2006; Lim 2013; Mehta 2013; Paulus 2012) and one RCT (Conlon 2001) have tested drain use versus no drain use after pancreatic resections. All of the trials found a similar or higher complication rate in the drainage group over the no drainage group. In addition, the routine use of surgical drains was associated with an increased length of hospital stay (Fisher 2011; Mehta 2013; Paulus 2012). Some authors suggested that routine prophylactic drainage after pancreatic resections could be safely abandoned (Adham 2013; Correa‐Gallego 2013; Mehta 2013). Twenty‐two years after the first reports of a 'no drain' policy and 13 years after the first RCT (Conlon 2001), Van Buren and coworkers conducted an RCT which compared drain use versus no drain use after pancreatic resections (Van Buren 2014). They found that pancreaticoduodenectomy without drain use was associated with an increased rate and severity of complications. They questioned the safety of not routinely placing drains in all participants after pancreaticoduodenectomy. In contrast, Witzigmann and colleagues performed another RCT on this topic (Witzigmann 2016). They found that pancreatic resection without drain use was superior to drain use in terms of clinically relevant pancreatic fistula and fistula‐associated complications. They suggested that there was no need for routine prophylactic drainage after pancreatic resection.
The 30‐day mortality in this review was approximately 2.8% and the 90‐day mortality was approximately 7.3%. There was no significant difference in either 30‐day or 90‐day mortality between the drainage group and the no drainage group. However, this review involved only 711 participants and therefore, was underpowered to detect a significant difference in this outcome.
Surgical morbidity was used to assess the efficacy of prophylactic abdominal drainage to reduce postoperative complications. The routine use of abdominal drainage after pancreatic surgery did not significantly reduce the incidence of postoperative complications in this review (64.8% with drain use versus 62.0% with no drain use). There are several possible reasons that may help to explain this. First, surgical drains may reduce some postoperative complications, but they may also be associated with drain‐related postoperative complications (e.g. broken drain). Second, this review only included two trials with 711 participants that compared drain use with no drain use. These studies may not have had the statistical power to detect the efficacy of abdominal drainage to reduce postoperative complications. Interestingly, surgical morbidity was lower in the early drain removal group (38.5%) than in the late drain removal group (61.4%) for people with low risk of postoperative pancreatic fistula. Thus, surgical drains may not benefit people with a low risk of postoperative pancreatic fistula. Surgical drains are more likely to increase the incidence of some postoperative complications if the duration of abdominal drainage is prolonged. Many factors have been considered to influence the development of postoperative pancreatic fistula (e.g. age, obesity, cardiovascular diseases, diabetes mellitus, pancreatic texture, and pancreatic duct size; Ramacciato 2011). It seems that older (e.g. over 60 years of age), overweight people with cardiovascular diseases, diabetes mellitus, soft pancreatic texture, and a small pancreatic duct diameter (e.g. less than 3 mm) are more likely to have postoperative pancreatic fistula (Ramacciato 2011; Riall 2008). One RCT demonstrated that the use of a somatostatin analogue reduced the risk of postoperative pancreatic fistula (Allen 2014). The use of drains may be more relevant in people with a higher risk of postoperative pancreatic fistula, which requires further investigation.
Length of hospital stay and hospital costs are important outcomes from the patient and healthcare funder perspectives. Active drain was associated with a shorter length of hospital stay (1.90 days) in cases where the surgeon considered abdominal drainage was necessary. In the case of drain insertion, early drain removal was associated with a shorter length of hospital stay (2.10 days) and lower hospital costs (EUR 2069) than a later drain removal.
Overall completeness and applicability of evidence
All of the trials included people undergoing elective pancreaticoduodenectomy (N = 839, 85.2%), distal pancreatectomy (N = 79, 8.0%), and other pancreatic surgery (N = 67, 6.8%) for various pancreatic and extra‐pancreatic diseases, including pancreatic cancers, ampullary cancers, chronic pancreatitis, biliary and duodenal malignancy, etc. The majority (58.6%) of the participants had pancreatic cancers (48.4%) or ampullary cancers (10.2%). Because only one trial included 11 participants (1.1%) undergoing laparoscopic pancreatic resections, the results of this review are not applicable to people undergoing laparoscopic pancreatic resections. The role of abdominal drainage after laparoscopic pancreatic resections therefore requires further assessment. Thus, the results of this review are only applicable to people undergoing elective open pancreaticoduodenectomy, distal pancreatectomy, and other pancreatic surgery for various pancreatic and extra‐pancreatic diseases, especially for pancreatic cancers or ampullary cancers.
Quality of the evidence
None of the trials were at low risk of bias. The trials included under each comparison were too few to assess inconsistency and publication bias. There was no indirectness of evidence because the trials did not perform the indirect comparison of one type of drain versus another. The CIs of the majority of outcomes were wide, indicating that the estimates of effect obtained were imprecise. Overall, the quality of the evidence was considered to be very low to moderate (Table 1; Table 2; Table 3).
Potential biases in the review process
The review included only five trials with 985 participants; thus, there are a lack of data on this topic to date. Additionally, we did not perform funnel plots to assess the publication bias due to the small number of included trials.
Agreements and disagreements with other studies or reviews
There is increasing evidence in Cochrane Reviews that routine abdominal drainage after various abdominal operations is not mandatory (Cheng 2015; de Jesus 2004; Gurusamy 2007a; Gurusamy 2007b; Gurusamy 2007c; Wang 2011). The routine use of surgical drains has also been questioned in other areas, including thyroid, gynaecological, and orthopaedic surgeries (Charoenkwan 2010; Gates 2005; Parker 2007; Samraj 2007).
One systematic review that compared drain use with no drain use in people undergoing pancreatic resections included three trials that we had considered for this review (Conlon 2001; Fisher 2011; Heslin 1998). Two of these trials were non‐randomized, so were not included in this review. They concluded that the routine use of abdominal drains after pancreatic resection may result in a higher risk for major complications (Van der Wilt 2013). This review does not make any specific recommendation because the number of participants included in this review did not have the statistical power to detect the benefit of abdominal drainage. A sample size of 870 (435 in each group) would be required to detect an absolute reduction in the intra‐abdominal infection rate of 5% (from 10% to 5%) at 80% power and an alpha‐error set at 0.05 (Conlon 2001).
Another systematic review compared early drain removal with late drain removal in people undergoing pancreatic resection (Diener 2011), and included two trials that we had considered for this review (Bassi 2010; Kawai 2006). One of the trials was not randomized, so we did not include it (Kawai 2006). The authors of the systematic review concluded that early drain removal seemed to be superior to late drain removal (Diener 2011). Our results concluded that early drain removal seemed to be superior to late drain removal for people with low risk of postoperative pancreatic fistula.
Authors' conclusions
There is no clear evidence to support routine prophylactic abdominal drainage after pancreatic surgery. In the case of drain insertion, low‐quality evidence suggests that active drain may reduce hospital stay after pancreatic surgery, and early removal may be superior to late removal for people with low risk of postoperative pancreatic fistula.
More trials with low risks of bias and sufficient sample size are necessary to assess the benefits and harms of abdominal drainage for various pancreatic resections (e.g. proximal, distal, and central pancreatectomy).
Future trials should report the rate and grade of the postoperative complication according to the Clavien‐Dindo Classification (Clavien 2009; Dindo 2004).
Future randomized trials should use adequate methods of randomization and allocation concealment. Future trials need to employ blinding of outcome assessors.
Future trials should analyze the data on an intention‐to‐treat basis in case of postrandomization dropouts.
Acknowledgements
We acknowledge the contribution of authors of previous version of this review: Su Peng, Chen Yang, Jiong Lu, Sijia Wu, and Rongxing Zhou.
We acknowledge the help and support of the Cochrane Upper Gastrointestinal and Pancreatic Diseases Review Group. The authors would also like to thank the following editors and peer referees who provided comments to improve the review: Sarah Rhodes (Editor), Adam Berger, Alfretta Vanderheyden, and Paul Moayyedi (Editor), and to Megan Prictor for copy editing the review.
The methods section of this review is based on a standard template used by Cochrane Upper Gastrointestinal and Pancreatic Diseases Review Group.
Appendices
Appendix 1. Glossary of terms
Abscess: a collection of pus that has built up within the tissue of the body.
Active drain: suction drains under low or high pressure.
Adverse events: side effects.
Anastomosis: connection between two organs (e.g. stomach and small intestine) created by surgery.
Biliary: related to the bile duct.
Chronic pancreatitis: long‐standing inflammation of the pancreas.
Delayed gastric emptying: a medical condition consisting of a paresis (partial paralysis) of the stomach, resulting in food remaining in the stomach for an abnormally long time.
Duodenal: related to the first section of the small intestine.
Drainage: the process or system by which water or waste liquid flows away.
Incidence: the rate at which something happens.
Morbidity: the proportion of people with any postoperative complications.
Mortality: the proportion of deaths after surgery.
Pancreas: the organ in the body that produces insulin and a liquid that helps your body to use the food that you eat.
Pancreatic: relating to the pancreas.
Pancreatic anastomoses: the surgical connection of the bile‐pancreatic duct and gut to form a continuous channel.
Pancreatic fistula: a complication whereby the pancreas is disconnected from the nearby gut, and then reconnected to allow pancreatic juice containing digestive enzymes to enter the digestive system.
Pancreaticoduodenectomy: a major surgical operation involving the pancreas, duodenum, and other organs.
Passive drain: drains without suction.
Postoperative: relating to the time after someone has had a medical operation.
Prevalence: the total number of people with an illness at a designated time.
Prophylactic: protective or preventive.
Randomized controlled trials: an experiment in which participants are randomly allocated to two or more interventions, possibly including a control intervention or no intervention, and the results are compared.
Subhepatic: under the liver.
Appendix 2. EBM Reviews (via Ovid) ‐ Cochrane Central Register of Controlled Trials (2015 to Issue 8, 2016)
exp Pancreas/
common bile duct/ or "ampulla of vater"/ or "sphincter of oddi"/ or exp Duodenum/
pancrea*.ab,ti.
or/1‐3
carcinoma/ or adenocarcinoma/ or exp Neoplasms/
(carcino* or cancer$ or neoplasm* or tumour$ or tumor$ or cyst$ or growth$ or adenocarcinoma* or malign*).tw.
5 or 6
4 and 7
pancreatic neoplasms/ or exp carcinoma, islet cell/ or carcinoma, pancreatic ductal/ or Duodenal Neoplasms/ or Common Bile Duct Neoplasms/ or exp Pancreatitis/
8 or 9
General Surgery/
(surger* or operatio* or operative therap* or resection*).tw.
11 or 12
10 and 13
pancreatectomy/ or pancreaticoduodenectomy/ or pancreaticojejunostomy/
(pancreatectom* or pancreaticojejunostom* or pancreaticoduodenectom* or pancreaticogastrostom* or duodenopancreatectom*).ab,ti.
or/14‐16
drainage/ or negative‐pressure wound therapy/ or suction/
(drain* or suction*).ab,ti.
18 or 19
17 and 20
Appendix 3. MEDLINE (via Ovid) search strategy (2015 to 28 August 2016)
randomized controlled trial.pt.
controlled clinical trial.pt.
randomized.ab.
placebo.ab.
drug therapy.fs.
randomly.ab.
trial.ab.
groups.ab.
or/1‐8
exp animals/ not humans.sh.
9 not 10
exp Pancreas/
common bile duct/ or "ampulla of vater"/ or "sphincter of oddi"/ or exp Duodenum/
pancrea*.ab,ti.
or/12‐14
carcinoma/ or adenocarcinoma/ or exp Neoplasms/
(carcino* or cancer$ or neoplasm* or tumour$ or tumor$ or cyst$ or growth$ or adenocarcinoma* or malign*).tw.
16 or 17
15 and 18
pancreatic neoplasms/ or exp carcinoma, islet cell/ or carcinoma, pancreatic ductal/ or Duodenal Neoplasms/ or Common Bile Duct Neoplasms/ or exp Pancreatitis/
19 or 20
General Surgery/
(surger* or operatio* or operative therap* or resection*).tw.
22 or 23
21 and 24
pancreatectomy/ or pancreaticoduodenectomy/ or pancreaticojejunostomy/
(pancreatectom* or pancreaticojejunostom* or pancreaticoduodenectom* or pancreaticogastrostom* or duodenopancreatectom*).ab,ti.
or/25‐27
drainage/ or negative‐pressure wound therapy/ or suction/
(drain* or suction*).ab,ti.
29 or 30
11 and 28 and 31
Appendix 4. Embase (via Ovid) search strategy (2015 to 28 August 2016)
random:.tw. or placebo:.mp. or double‐blind:.tw.
pancreas/ or "islets of langerhans"/ or pancreas, exocrine/ or pancreatic ducts/
exp common bile duct/ or exp Vater papilla/ or exp duodenum/
pancrea*.ab,ti.
2 or 3 or 4
carcinoma/ or adenocarcinoma/ or exp neoplasm/
(carcino* or cancer$ or neoplasm* or tumour$ or tumor$ or cyst$ or growth$ or adenocarcinoma* or malign*).tw.
6 or 7
5 and 8
pancreas islet cell tumor/ or exp pancreas cancer/ or exp duodenum cancer/ or exp duodenum carcinoma/ or exp Vater papilla tumor/ or exp Vater papilla carcinoma/ or exp bile duct cancer/ or exp pancreatitis/
9 or 10
surgery/
(surger* or operatio* or operative therap* or resection*).tw.
12 or 13
11 and 14
exp pancreas resection/ or exp pancreaticojejunostomy/ or exp pancreaticoduodenectomy/
(pancreatectom* or pancreaticojejunostom* or pancreaticoduodenectom* or pancreaticogastrostom* or duodenopancreatectom*).ab,ti.
or/15‐17
exp drain/ or exp suction/ or exp abscess drainage/ or exp abdominal drainage/ or exp wound drainage/ or exp surgical drainage/ or exp vacuum assisted closure/ or exp negative pressure wound therapy/
(drain* or suction*).ab,ti.
19 or 20
1 and 18 and 21
Appendix 5. Science Citation Index Expanded search strategy (2015 to 28 August 2016)
Topic=(pancrea* or (common bile duct*) or (ampulla of vater) or (sphincter of oddi) or duodenum) AND Topic=(carcino* or cancer* or neoplasm* or tumour* or tumor* or cyst* or growth* or adenocarcinoma* or malign*)
Topic=((surger* or operatio* or operative therap* or resection*)) OR Topic=((pancreatectom* or pancreaticojejunostom* or pancreaticoduodenectom* or pancreaticogastrostom* or duodenopancreatectom*))
Topic=(drain* or suction*) OR Topic=(negative‐pressure wound therap*) OR Topic=(vacuum assisted closure*)
#3 AND #2 AND #1
Topic=(single blind* or double blind* or clinical trial* or placebo* or random* or controlled clinical trial* or research design or comparative stud* or controlled trial* or (follow up stud*) or prospective stud*)
#5 AND #4
Appendix 6. Chinese Biomedical Literature Database (CBM) search strategy (2015 to 28 August 2016)
主题词:随机对照试验/全部树/全部副主题词
主题词:临床对照试验/全部树/全部副主题词
主题词:临床试验/全部树/全部副主题词
主题词:病例对照研究/全部树/全部副主题词
主题词:随机分配/全部树/全部副主题词
主题词:对比研究/全部树/全部副主题词
主题词:前瞻性研究/全部树/全部副主题词
主题词:安慰剂/全部树/全部副主题词
全部字段:随机
全部字段:单盲
全部字段:双盲
全部字段:盲法
(#1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12)
主题词:胰腺肿瘤/全部树/全部副主题词
主题词:胰腺疾病/全部树/全部副主题词
全部字段:胰腺占位
全部字段:胰腺癌
全部字段:胰头癌
主题词:胆总管肿瘤/全部树/全部副主题词
全部字段:胆总管下端占位
全部字段:胆总管下端肿瘤
全部字段:胆总管下端癌
主题词:肝胰管壶腹/全部树/全部副主题词
全部字段:壶腹部占位
全部字段:壶腹部肿瘤
全部字段:壶腹癌
全部字段:vater壶腹癌
主题词:十二指肠肿瘤/全部树/全部副主题词
主题词:十二指肠疾病/全部树/全部副主题词
全部字段:十二指肠占位
全部字段:十二指肠乳头腺癌
主题词:胰腺炎/全部树/全部副主题词
主题词:胰腺炎,慢性/全部树/全部副主题词
(#14 OR #15 OR #16 OR #17 OR #18 OR #19 OR #20 OR #21 OR #22 #23 OR #24 OR #25 OR #26 OR #27 OR #28 OR #29 OR #30 OR #31 OR #32 OR #33)
主题词:外科手术/全部树/全部副主题词
主题词:吻合术, 外科/全部树/全部副主题词
全部字段:手术治疗
全部字段:手术
全部字段:切除术
(#35 OR #36 OR #37 OR #38 OR #39)
(#34 AND #40)
主题词:胰腺/全部树/SU
主题词:胰腺切除术/全部树/全部副主题词
主题词:胰十二指肠切除术/全部树/全部副主题词
全部字段:胰体尾切除术
全部字段:胰腺部分切除
全部字段:胰十二指肠吻合术
全部字段:胰头十二指肠吻合术
全部字段:Whipple术式
全部字段:Child术式
(#41 OR #42 OR #43 OR #44 OR #45 OR #46 OR#47 OR #48 OR #49 OR #50)
主题词:引流/全部树/全部副主题词
主题词:抽吸/全部树/全部副主题词
主题词:负压伤口治疗/全部树/全部副主题词
全部字段:腹腔引流
全部字段:引流管
全部字段:手术引流
全部字段:伤口引流
全部字段:负压引流
(#52 OR #53 OR #54 OR #55 OR #56 OR #57 OR# 58 OR #59)
(#13 AND #51 AND #60)
Data and analyses
Comparison 1.
Drain use versus no drain use
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Mortality (30 days) | 3 | 711 | Risk Ratio (M‐H, Random, 95% CI) | 0.78 [0.31, 1.99] |
| 2 Mortality (90 days) | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 3 Intra‐abdominal infection | 3 | 711 | Risk Ratio (M‐H, Random, 95% CI) | 0.89 [0.36, 2.20] |
| 4 Wound infection | 3 | 711 | Risk Ratio (M‐H, Random, 95% CI) | 0.92 [0.63, 1.36] |
| 5 Drain‐related complications | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 6 Morbidity | 3 | 711 | Risk Ratio (M‐H, Random, 95% CI) | 1.04 [0.93, 1.16] |
| 7 Length of hospital stay (days) | 3 | 711 | Mean Difference (IV, Random, 95% CI) | ‐0.66 [‐1.60, 0.29] |
| 8 Additional open procedures for postoperative complications | 3 | 711 | Risk Ratio (M‐H, Random, 95% CI) | 1.18 [0.55, 2.52] |
| 9 Additional radiological interventions for postoperative complications | 2 | 316 | Risk Ratio (M‐H, Random, 95% CI) | 0.78 [0.19, 3.25] |
Comparison 2.
Active drain versus passive drain
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Mortality (30 days) | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 2 Intra‐abdominal infection | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 3 Wound infection | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 4 Morbidity | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 5 Length of hospital stay (days) | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 6 Additional open procedures for postoperative complications | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected |
Comparison 3.
Early versus late drain removal
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Mortality (30 days) | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 2 Morbidity | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 3 Length of hospital stay (days) | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 4 Hospital costs (EUR) | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 5 Additional open procedures for postoperative complications | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected |
Comparison 4.
Drain use versus no drain use (sensitivity analysis by changing between worst‐case scenario analysis and best‐case scenario analysis for missing data)
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Mortality (90 days) (worst‐case scenario) | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 2 Mortality (90 days) (best‐case scenario) | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected |
What's new
Last assessed as up‐to‐date: 28 August 2016.
| Date | Event | Description |
|---|---|---|
| 28 August 2016 | New citation required but conclusions have not changed | Searches rerun, two additional trials found |
| 28 August 2016 | New search has been performed | Searches rerun and new evidence incorporated |
Differences between protocol and review
Because overall infectious complications were not reported, we chose a type of infectious complication (intra‐abdominal infection) for the 'Summary of findings' table.
Characteristics of studies
Characteristics of included studies [ordered by study ID]
| Methods | Randomized controlled trial. | |
| Participants | Country: Italy. Number randomized: 114. Postrandomization dropout: 0 (0%). Mean age: 56.6 years. Females: 55 (48.2%). Pancreatic cancer: 56 (49.1%). Biliary cancer: 2 (1.8%). Ampullary cancer: 7 (6.1%). Chronic pancreatitis: 3 (2.6%). Other: 46 (40.4%). Pancreaticoduodenectomy: 75 (65.8%). Distal pancreatectomy: 39 (34.2%). Other pancreatic surgery: 0 (0%). Inclusion criteria:
Exclusion criteria:
|
|
| Interventions | Participants (N = 114) were randomly assigned to 1 of 2 groups. Group 1: early drain removal (postoperative day 3) (N = 57). Group 2: late drain removal (postoperative day 5 or later) (N = 57). |
|
| Outcomes | Pancreatic fistula, abdominal complications, pulmonary complications, reoperation, length of hospital stay, hospital readmission, postoperative mortality, morbidity, and hospital costs. | |
| Notes | 2 drainage tubes (Penrose drains) were placed in relation to the pancreatic and biliary anastomoses through separate skin incisions after pancreaticoduodenectomy. 1 drainage tube was placed in relation to the pancreatic stump through separate skin incisions after distal pancreatectomy. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "eligible patients were randomized by a computer‐generated allocation schedule". |
| Allocation concealment (selection bias) | Unclear risk | Comment: no information provided. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Quote: "Masking: Open Label" in the protocol. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: there were no postrandomization dropouts. |
| Selective reporting (reporting bias) | Low risk | Comment: the study protocol was available. All of the study's prespecified outcomes were reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other sources of bias. |
| Methods | Randomized controlled trial. | |
| Participants | Country: USA. Number randomized: 179. Postrandomization dropout: 0 (0%). Mean age: 65.4 years. Females: 90 (50.3%). Pancreatic cancer: 142 (79.3%). Biliary cancer: 3 (1.7%). Duodenal cancer: 10 (5.6%). Ampullary cancer: 24 (13.4%). Chronic pancreatitis: 0 (0%). Pancreaticoduodenectomy: 139 (77.7%). Distal pancreatectomy: 40 (22.3%). Other pancreatic surgery: 0 (0%). Inclusion criteria:
Exclusion criteria:
|
|
| Interventions | Participants (N = 86) were randomly assigned to 1 of 2 groups. Group 1: drainage (N = 91). Group 2: no drainage (N = 88). |
|
| Outcomes | Mortality, morbidity, wound infection, intra‐abdominal infection, various postoperative complications, reoperation, additional radiological intervention, and length of hospital stay. | |
| Notes | 2 drainage tubes (Jackson‐Pratt closed suction drains) were placed in relation to the pancreatic and biliary anastomoses through separate skin incisions after pancreaticoduodenectomy. 1 drainage tube was placed in relation to the pancreatic stump through separate skin incisions after distal pancreatectomy. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Comment: no information provided. |
| Allocation concealment (selection bias) | Unclear risk | Quote: "patients were randomized during surgery by the envelope method". Comment: no information was provided whether the envelope was opaque or not. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Comment: no information provided. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: there were no postrandomization dropouts. |
| Selective reporting (reporting bias) | Low risk | Comment: all the primary outcomes were reported. There was some selective outcome reporting in the secondary outcomes, but the review authors considered this trial to be free of selective reporting for the primary outcomes. |
| Other bias | Low risk | Comment: the study appeared to be free of other sources of bias. |
| Methods | Randomized controlled trial. | |
| Participants | Country: China. Number randomized: 160. Postrandomization dropout: 0 (0%). Mean age: 59.6 years. Females: 42 (26.3%). Pancreatic cancer: 53 (33.1%). Biliary cancer: 36 (22.5%). Duodenal cancer: 28 (17.5%). Ampullary cancer: 33 (20.6%). Chronic pancreatitis: 5 (3.1%). Pancreaticoduodenectomy: 160 (100%). Distal pancreatectomy: 0 (0%). Other pancreatic surgery: 0 (0%). Inclusion criteria:
Exclusion criteria:
|
|
| Interventions | Participants (N = 160) were randomly assigned to 1 of 2 groups. Group 1: active drain (N = 82). Group 2: passive drain (N = 78). |
|
| Outcomes | Mortality, morbidity, wound infection, intra‐abdominal infection, various postoperative complications, reoperation, readmission, additional radiological intervention, and length of hospital stay. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "we randomized our patients using a computer‐generated random number". |
| Allocation concealment (selection bias) | Unclear risk | Comment: no information provided. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote: "Patients were prospectively assigned a code and data were recorded in a database by two nurses". Comment: no information provided whether the 2 nurses were blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: there were no postrandomization dropouts. |
| Selective reporting (reporting bias) | Low risk | Comment: all the primary outcomes were reported. There was some selective outcome reporting in the secondary outcomes, but the review authors considered this trial to be free of selective reporting for the primary outcomes. |
| Other bias | Low risk | Comment: the study appeared to be free of other sources of bias. |
| Methods | Randomized controlled trial. | |
| Participants | Country: USA. Number randomized: 137. Postrandomization dropout: 3 (2.2%). Mean age: 63.2 years. Females: 62 (45.3%). Pancreatic cancer: 67 (48.9%). Biliary cancer: not mentioned. Duodenal cancer: not mentioned. Ampullary cancer: 17 (12.4%). Chronic pancreatitis: 15 (10.9%). Pancreaticoduodenectomy: 137 (100%). Distal pancreatectomy: 0 (0%). Other pancreatic surgery: 0 (0%). Inclusion criteria:
Exclusion criteria:
|
|
| Interventions | Participants (N = 137) were randomly assigned to 1 of 2 groups. Group 1: drainage (N = 68). Group 2: no drainage (N = 69). |
|
| Outcomes | Mortality, morbidity, wound infection, intra‐abdominal infection, various postoperative complications, reoperation, readmission, additional radiologic intervention, and length of hospital stay. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Randomization was performed using a computerized randomization system at the coordinating center". |
| Allocation concealment (selection bias) | Unclear risk | Comment: no information provided. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Quote: "Masking: open label". |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Quote: "There were 3 cases for which the randomization group assignment was inadvertently not followed". |
| Selective reporting (reporting bias) | Low risk | Comment: the study protocol was available. All of the study's prespecified outcomes were reported. |
| Other bias | Low risk | Comment: the study appears to be free of other sources of bias. |
| Methods | Randomized controlled trial. | |
| Participants | Country: Germany. Number randomized: 438. Postrandomization dropout: 43 (2.2%). Mean age: 63.4 years. Females: 139 (35.2%). Pancreatic cancer: 159 (40.3%). Biliary cancer: 23 (5.8%). Duodenal cancer: 5 (1.3%). Ampullary cancer: 19 (4.8%). Chronic pancreatitis: 101 (25.6%). Pancreaticoduodenectomy: 328 (83.0%). Distal pancreatectomy: 0 (0%). Other pancreatic surgery: 67 (17.0%). Inclusion criteria:
Exclusion criteria:
|
|
| Interventions | Participants (N = 395) were randomly assigned to 1 of 2 groups. Group 1: drainage (N = 202). Group 2: no drainage (N = 193). |
|
| Outcomes | Mortality, morbidity, wound infection, intra‐abdominal infection, various postoperative complications, reoperation, operation time, and length of hospital stay. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "A random list was created by GWT‐TUD Ltd". |
| Allocation concealment (selection bias) | Low risk | Quote: "The random allocation sequence was implemented by the use of sequentially numbered opaque envelopes". |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Comment: no information provided. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Quote: "A total of 438 patients were randomized. Forty‐three patients (9.8%) were excluded because no pancreatic resection with consecutive pancreaticojejunal anastomosis was performed. Thus, the intention‐to‐treat population consisted of 395 patients". Comment: there are 43 postrandomization dropouts. The study did not perform an intention‐to‐treat analysis which included the 43 dropouts. |
| Selective reporting (reporting bias) | Low risk | Comment: the study protocol was available. All of the study's prespecified outcomes were reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other sources of bias. |
IU: international unit; N: number of participants.
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Adham 2013 | A non‐randomized study. |
| Behrman 2015 | A non‐randomized study. |
| Correa‐Gallego 2013 | A non‐randomized study. |
| Fisher 2011 | A non‐randomized study. |
| Giovinazzo 2011 | A non‐randomized study. |
| Heslin 1998 | A non‐randomized study. |
| Jeekel 1992 | Case series. |
| Kawai 2006 | A non‐randomized study. |
| Lee 2009 | Randomized controlled trial about pancreatic duct drainage. |
| Lim 2013 | A non‐randomized study. |
| Mehta 2013 | A non‐randomized study. |
| Paulus 2012 | A non‐randomized study. |
Characteristics of ongoing studies [ordered by study ID]
| Trial name or title | DRAPA Trial ‐ Closed‐Suction Drains Versus Closed Gravity Drains in Pancreatic Surgery: Study Protocol for a Randomized Controlled Trial. |
| Methods | Randomized controlled trial. |
| Participants | Country: Czech Republic. Number of enrolment: 223. Inclusion criteria:
Exclusion criteria:
|
| Interventions | Participants are randomly assigned to 1 or 2 groups. Group 1: closed suction drain (active drain). Group 2: closed gravity drain (passive drain). |
| Outcomes | Primary outcome: rate of postoperative pancreatic fistula. Secondary outcomes: postoperative morbidity, including wound infection, intra‐abdominal collections, delayed gastric emptying, postoperative haemorrhage, pneumonia, abdominal rupture, cardiac events, and neurological complications. |
| Starting date | October 2013. |
| Contact information | Principal investigator: Filip Cecka, Department of Surgery, University Hospital Hradec Kralove, Hradec Kralove, Czech Republic, 50005. Tel: +42049583 ext 4272. Email: filip.cecka@seznam.cz. |
| Notes |
Contributions of authors
Conceiving the review: YC.
Designing the review: NC.
Co‐ordinating the review: SH.
Designing search strategies: YC, NC.
Study selection: ML, JX.
Data extraction: ML, JX.
Writing the review: YC, SH.
Providing general advice on the review: NC.
Securing funding for the review: SH.
Performing previous work that was the foundation of the current study: YC.
Sources of support
Internal sources
-
Chongqing Medical University, China.
Provided funding for the review.
External sources
No sources of support supplied
Declarations of interest
YC: none known.
JX: none known.
ML: none known.
NC: none known.
SH: none known.
New search for studies and content updated (no change to conclusions)
References
References to studies included in this review
- Bassi C, Molinari E, Malleo G, Crippa S, Butturini G, Salvia R, et al. Early versus late drain removal after standard pancreatic resections: results of a prospective randomized trial. Annals of Surgery 2010;252(2):207‐14. [] [DOI] [PubMed] [Google Scholar]; 2864182
- Conlon KC, Labow D, Leung D, Smith A, Jarnagin W, Coit DG, et al. Prospective randomized clinical trial of the value of intraperitoneal drainage after pancreatic resection. Annals of Surgery 2001;234(4):487‐93. [] [DOI] [PMC free article] [PubMed] [Google Scholar]; 2864184
- Jiang H, Liu N, Zhang M, Lu L, Dou R, Qu L. A randomized trial on the efficacy of prophylactic active drainage in prevention of complications after pancreaticoduodenectomy. Scandinavian Journal of Surgery 2016;1(1):1457496916665543. [] [DOI] [PubMed] [Google Scholar]; 4439016
- McMillan MT, Fisher WE, Buren G, McElhany A, Bloomston M, Hughes SJ, et al. The value of drains as a fistula mitigation strategy for pancreatoduodenectomy: something for everyone? Results of a randomized prospective multi‐institutional study. Journal of Gastrointestinal Surgery 2015;19(1):21‐30. [] [DOI] [PubMed] [Google Scholar]; McMillan MT, Malleo G, Bassi C, Butturini G, Salvia R, Roses RE, et al. Drain management after pancreatoduodenectomy: reappraisal of a prospective randomized trial using risk stratification. Journal of the American College of Surgeons 2015;221(4):798‐809. [] [DOI] [PubMed] [Google Scholar]; Buren G, Bloomston M, Hughes SJ, Winter J, Behrman SW, Zyromski NJ, et al. A randomized prospective multicenter trial of pancreaticoduodenectomy with and without routine intraperitoneal drainage. Annals of Surgery 2014;259(4):605‐12. [] [DOI] [PubMed] [Google Scholar]; 2864186
- Witzigmann H, Diener M K, Kienkötter S, Rossion I, Bruckner T, Werner B, et al. No need for routine drainage after pancreatic head resection: the dual‐center, randomized, controlled PANDRA trial (ISRCTN04937707). Annals of Surgery 2016;264(3):528‐37. [] [DOI] [PubMed] [Google Scholar]; 4439020
References to studies excluded from this review
- Adham M, Chopin‐Laly X, Lepilliez V, Gincul R, Valette PJ, Ponchon T. Pancreatic resection: drain or no drain?. Surgery 2013;154(5):1069‐77. [] [DOI] [PubMed] [Google Scholar]; 2864188
- Behrman SW, Zarzaur BL, Parmar A, Riall TS, Hall BL, Pitt HA. Routine drainage of the operative bed following elective distal pancreatectomy does not reduce the occurrence of complications. Journal of Gastrointestinal Surgery 2015;19(1):72‐9. [] [DOI] [PMC free article] [PubMed] [Google Scholar]; 4439022
- Correa‐Gallego C, Brennan MF, Dʼangelica M, Fong Y, Dematteo RP, Kingham TP, et al. Operative drainage following pancreatic resection: analysis of 1122 patients resected over 5 years at a single institution. Annals of Surgery 2013;258(6):1051‐8. [] [DOI] [PMC free article] [PubMed] [Google Scholar]; 2864190
- Fisher WE, Hodges SE, Silberfein EJ, Artinyan A, Ahern CH, Jo E, et al. Pancreatic resection without routine intraperitoneal drainage. International Hepato‐Pancreato‐Biliary Association 2011;13(7):503‐10. [; DOI: 10.1111/j.1477-2574.2011.00331.x] [DOI] [PMC free article] [PubMed] [Google Scholar]; 2864192
- Giovinazzo F, Butturini G, Salvia R, Mascetta G, Monsellato D, Marchegiani G, et al. Drain management after pancreatic resection: state of the art. Journal of Hepato‐Biliary‐Pancreatic Sciences 2011;18(6):779‐84. [] [DOI] [PubMed] [Google Scholar]; 2864194
- Heslin MJ, Harrison LE, Brooks AD, Hochwald SN, Coit DG, Brennan MF. Is intra‐abdominal drainage necessary after pancreaticoduodenectomy?. Journal of Gastrointestinal Surgery 1998;2(4):373‐8. [] [DOI] [PubMed] [Google Scholar]; 2864196
- Jeekel J. No abdominal drainage after Whipple's procedure. British Journal of Surgery 1992;79(2):182. [] [DOI] [PubMed] [Google Scholar]; 2864198
- Kawai M, Tani M, Terasawa H, Ina S, Hirono S, Nishioka R, et al. Early removal of prophylactic drains reduces the risk of intra‐abdominal infections in patients with pancreatic head resection: prospective study for 104 consecutive patients. Annals of Surgery 2006;244(1):1‐7. [] [DOI] [PMC free article] [PubMed] [Google Scholar]; 2864200
- Lee SE, Ahn YJ, Jang JY, Kim SW. Prospective randomized pilot trial comparing closed suction drainage and gravity drainage of the pancreatic duct in pancreaticojejunostomy. Journal of Hepato‐Biliary‐Pancreatic Surgery 2009;16(6):837‐43. [] [DOI] [PubMed] [Google Scholar]; 2864202
- Lim C, Dokmak S, Cauchy F, Aussilhou B, Belghiti J, Sauvanet A. Selective policy of no drain after pancreaticoduodenectomy is a valid option in patients at low risk of pancreatic fistula: a case‐control analysis. World Journal of Surgery 2013;37(5):1021‐7. [] [DOI] [PubMed] [Google Scholar]; 2864204
- Mehta VV, Fisher SB, Maithel SK, Sarmiento JM, Staley CA, Kooby DA. Is it time to abandon routine operative drain use? A single institution assessment of 709 consecutive pancreaticoduodenectomies. Journal of the American College of Surgeons 2013;216(4):635‐42. [] [DOI] [PubMed] [Google Scholar]; 2864206
- Paulus EM, Zarzaur BL, Behrman SW. Routine peritoneal drainage of the surgical bed after elective distal pancreatectomy: is it necessary?. American Journal of Surgery 2012;204(4):422‐7. [] [DOI] [PubMed] [Google Scholar]; 2864208
References to ongoing studies
- Čečka F, Loveček M, Jon B, Skalický P, Šubrt Z, Ferko A. DRAPA trial ‐ closed‐suction drains versus closed gravity drains in pancreatic surgery: study protocol for a randomized controlled trial. Trials 2015;16:207. [] [DOI] [PMC free article] [PubMed] [Google Scholar]; 4439024
Additional references
- Allen PJ. Operative drains after pancreatic resection ‐ the Titanic is sinking. International Hepato‐Pancreato‐Biliary Association 2011;13(9):595. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Allen PJ, Gönen M, Brennan MF, Bucknor AA, Robinson LM, Pappas MM, et al. Pasireotide for postoperative pancreatic fistula. New England Journal of Medicine 2014;370(21):2014‐22. [DOI] [PubMed] [Google Scholar]
- Anderson KE, Mack T, Silverman D. Cancer of the pancreas. In: Schottenfeld D, Fraumeni JF Jr editor(s). Cancer Epidemiology and Prevention. 3rd Edition. New York: Oxford University Press, 2006:1‐1416. [Google Scholar]
- Andrén‐Sandberg A. Complications of pancreatic surgery. North American Journal of Medical Sciences 2011;3(12):531‐5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bassi C, Dervenis C, Butturini G, Fingerhut A, Yeo C, Izbicki J, et al. Postoperative pancreatic fistula: an international study group (ISGPF) definition. Surgery 2005;138(1):8‐13. [DOI] [PubMed] [Google Scholar]
- Bornman PC, Beckingham IJ. ABC of diseases of liver, pancreas, and biliary system: chronic pancreatitis. BMJ 2001;322(7287):660‐3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Braganza JM, Lee SH, McCloy RF, McMahon MJ. Chronic pancreatitis. Lancet 2011;377(9772):1184‐97. [DOI] [PubMed] [Google Scholar]
- Cameron‐Strange A, Horner J. Haemorrhage following insertion of continuous suction drains at appendicectomy. Journal of the Royal College of Surgeons of Edinburgh 1985;30(4):271‐2. [PubMed] [Google Scholar]
- Charoenkwan K, Kietpeerakool C. Retroperitoneal drainage versus no drainage after pelvic lymphadenectomy for the prevention of lymphocyst formation in patients with gynaecological malignancies. Cochrane Database of Systematic Reviews 2010, Issue 1. [DOI: 10.1002/14651858.CD007387.pub2] [DOI] [PubMed] [Google Scholar]
- Cheng Y, Lu J, Xiong X, Wu S, Lin Y, Wu T, et al. Gases for establishing pneumoperitoneum during laparoscopic abdominal surgery. Cochrane Database of Systematic Reviews 2013, Issue 1. [DOI: 10.1002/14651858.CD009569.pub2] [DOI] [PubMed] [Google Scholar]
- Cheng Y, Jia Q, Xiong X, He D, Cheng NS. Hepatobiliary and pancreatic: traumatic neuroma of the ampulla of Vater. Journal of Gastroenterology and Hepatology 2014;29(7):1342. [DOI] [PubMed] [Google Scholar]
- Cheng Y, Zhou S, Zhou R, Lu J, Wu S, Xiong X, et al. Abdominal drainage to prevent intra‐peritoneal abscess after open appendectomy for complicated appendicitis. Cochrane Database of Systematic Reviews 2015, Issue 2. [DOI: 10.1002/14651858.CD010168.pub2] [DOI] [PubMed] [Google Scholar]
- Cheng Y, Ye M, Xiong X, Peng S, Wu HM, Cheng N, et al. Fibrin sealants for the prevention of postoperative pancreatic fistula following pancreatic surgery. Cochrane Database of Systematic Reviews 2016, Issue 2. [DOI: 10.1002/14651858.CD009621.pub2] [DOI] [PubMed] [Google Scholar]
- Clavien PA, Barkun J, Oliveira ML, Vauthey JN, Dindo D, Schulick RD, et al. The Clavien‐Dindo classification of surgical complications: five‐year experience. Annals of Surgery 2009;250(2):187‐96. [DOI] [PubMed] [Google Scholar]
- Connor S, Alexakis N, Garden OJ, Leandros E, Bramis J, Wigmore SJ. Meta‐analysis of the value of somatostatin and its analogues in reducing complications associated with pancreatic surgery. British Journal of Surgery 2005;92(9):1059‐67. [DOI] [PubMed] [Google Scholar]
- Jesus EC, Karliczek A, Matos D, Castro AA, Atallah ÁN. Prophylactic anastomotic drainage for colorectal surgery. Cochrane Database of Systematic Reviews 2004, Issue 2. [DOI: 10.1002/14651858.CD002100.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Diener MK, Tadjalli‐Mehr K, Wente MN, Kieser M, Büchler MW, Seiler CM. Risk‐benefit assessment of closed intra‐abdominal drains after pancreatic surgery: a systematic review and meta‐analysis assessing the current state of evidence. Langenbeck's Archives of Surgery 2011;396(1):41‐52. [DOI] [PubMed] [Google Scholar]
- Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Annals of Surgery 2004;240(2):205‐13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dragovich T, Erickson RA, Larson CR, Shabahang M. Pancreatic cancer, 2011. emedicine.medscape.com/article/280605‐overview (accessed 16 October 2016).
- Durai R, Mownah A, Ng PC. Use of drains in surgery: a review. Journal of Perioperative Practice 2009;19(6):180‐6. [DOI] [PubMed] [Google Scholar]
- Forman D, Delaney B, Kuipers E, Malthaner R, Moayyedi P, Gardener E, et al. Cochrane Upper GI and Pancreatic Diseases Group. About The Cochrane Collaboration (Cochrane Review Groups (CRGs)) 2011, Issue 12. Art. No.: COLOCA.
- Garg PK, Tandon RK. Survey on chronic pancreatitis in the Asia‐Pacific region. Journal of Gastroenterology and Hepatology 2004;19(9):998‐1004. [DOI] [PubMed] [Google Scholar]
- Gates S, Anderson ER. Wound drainage for caesarean section. Cochrane Database of Systematic Reviews 2005, Issue 1. [DOI: 10.1002/14651858.CD004549.pub2] [DOI] [PubMed] [Google Scholar]
- Brozek J, Oxman A, Schunemann H. GRADEprofiler (GRADEpro). Canada: Evidence Prime, 2015.
- Gurusamy KS, Samraj K, Davidson BR. Routine abdominal drainage for uncomplicated liver resection. Cochrane Database of Systematic Reviews 2007, Issue 3. [DOI: 10.1002/14651858.CD006232.pub2] [DOI] [PubMed] [Google Scholar]
- Gurusamy KS, Samraj K. Routine abdominal drainage for uncomplicated open cholecystectomy. Cochrane Database of Systematic Reviews 2007, Issue 2. [DOI: 10.1002/14651858.CD006003.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gurusamy KS, Samraj K, Mullerat P, Davidson BR. Routine abdominal drainage for uncomplicated laparoscopic cholecystectomy. Cochrane Database of Systematic Reviews 2007, Issue 4. [DOI: 10.1002/14651858.CD006004.pub3] [DOI] [PubMed] [Google Scholar]
- Gurusamy KS, Koti R, Fusai G, Davidson BR. Somatostatin analogues for pancreatic surgery. Cochrane Database of Systematic Reviews 2013, Issue 4. [DOI: 10.1002/14651858.CD008370.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hackert T, Werner J, Buchler MW. Postoperative pancreatic fistula. Surgeon2011; Vol. 9, issue 4:211‐7. [DOI] [PubMed]
- Halloran CM, Ghaneh P, Bosonnet L, Hartley MN, Sutton R, Neoptolemos JP. Complications of pancreatic cancer resection. Digestive Surgery 2002;19(2):138‐46. [DOI] [PubMed] [Google Scholar]
- Henkus HE. Complications of high‐vacuum suction drainage. European Journal of Surgery 1999;165(8):813‐4. [DOI] [PubMed] [Google Scholar]
- Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta‐analyses. BMJ 2003;327(7414):557‐60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Higgins JPT, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
- Inoue M, Uchida K, Otake K, Koike Y, Okugawa Y, Kobayashi M, et al. Placement of prophylactic drains after laparotomy may increase infectious complications in neonates. Pediatric Surgery International 2011;27(9):975‐9. [DOI] [PubMed] [Google Scholar]
- Lowenfels AB, Maisonneuve P. Epidemiology and risk factors for pancreatic cancer. Best Practice & Research. Clinical Gastroenterology 2006;20(2):197‐209. [DOI] [PubMed] [Google Scholar]
- Lévy P, Barthet M, Mollard BR, Amouretti M, Marion‐Audibert AM, Dyard F. Estimation of the prevalence and incidence of chronic pancreatitis and its complications. Gastroenterologie Clinique et Biologique 2006;30(6‐7):838‐44. [DOI] [PubMed] [Google Scholar]
- Makama JG, Ahmed A, Ukwenya Y, Mohammed I. Drain site hernia in an adult: a case report. West African Journal of Medicine 2010;29(6):429‐31. [DOI] [PubMed] [Google Scholar]
- Memon MA, Memon MI, Donohue JH. Abdominal drains: a brief historical review. Irish Medical Journal 2001;94(6):164‐6. [PubMed] [Google Scholar]
- Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMAG. Preferred Reporting Items for Systematic Reviews and Meta‐Analyses: the PRISMA statement. Open Medicine 2009;3(3):12‐130. [PMC free article] [PubMed] [Google Scholar]
- Nomura T, Shirai Y, Okamoto H, Hatakeyama K. Bowel perforation caused by silicone drains: a report of two cases. Surgery Today 1998;28(9):940‐2. [DOI] [PubMed] [Google Scholar]
- Parker MJ, Livingstone V, Clifton R, McKee A. Closed suction surgical wound drainage after orthopaedic surgery. Cochrane Database of Systematic Reviews 2007, Issue 3. [DOI: 10.1002/14651858.CD001825.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ramacciato G, Mercantini P, Petrucciani N, Nigri GR, Kazemi A, Muroni M, et al. Risk factors of pancreatic fistula after pancreaticoduodenectomy: a collective review. American Journal of Surgery 2011;77(3):257‐69. [PubMed] [Google Scholar]
- Reed MW, Wyman A, Thomas WE, Zeiderman MR. Perforation of the bowel by suction drains. British Journal of Surgery 1992;79(7):679. [DOI] [PubMed] [Google Scholar]
- Reeves BC, Deeks JJ, Higgins JPT, Wells GA. Chapter 13: Including non‐randomized studies. In: Higgins JPT, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
- Copenhagen, The Nordic Cochrane Centre: The Cochrane Collaboration. Review Manager (RevMan). Version 5.3. Copenhagen, The Nordic Cochrane Centre: The Cochrane Collaboration, 2014.
- Riall TS, Reddy DM, Nealon WH, Goodwin JS. The effect of age on short‐term outcomes after pancreatic resection: a population‐based study. Annals of Surgery 2008;248(3):459‐67. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sahu SK, Bahl DV, Husain M, Sachan PK. Drain erosion into bowel: an unusual complication. Internet Journal of Surgery2008; Vol. 16, issue 2.
- Samraj K, Gurusamy KS. Wound drains following thyroid surgery. Cochrane Database of Systematic Reviews 2007, Issue 4. [DOI: 10.1002/14651858.CD006099.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spanier BW, Dijkgraaf MG, Bruno MJ. Epidemiology, aetiology and outcome of acute and chronic pancreatitis: an update. Best Practice & Research. Clinical Gastroenterology 2008;22(1):45‐63. [DOI] [PubMed] [Google Scholar]
- Srivastava P, Srivastava S, Sahu M. Iatrogenic bowel perforation secondary to surgical drain after cholecystectomy: a case report with review of literature. Internet Journal of Surgery2007; Vol. 13, issue 1.
- Sterne JAC, Egger M, Moher D. Chapter 10: Addressing reporting biases. In: Higgins JPT, Green S, editors. Cochrane Handbook for Systematic Reviews of Intervention. Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
- Wilt AA, Coolsen MM, Hingh IH, Wilt GJ, Groenewoud H, Dejong CH, et al. To drain or not to drain: a cumulative meta‐analysis of the use of routine abdominal drains after pancreatic resection. International Hepato‐Pancreato‐Biliary Association 2013;15(5):337‐44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hee R. Complications of drainage. Acta Chirurgica Belgica 1983;83(5):340‐4. [PubMed] [Google Scholar]
- Wang Z, Chen J, Su K, Dong Z. Abdominal drainage versus no drainage post gastrectomy for gastric cancer. Cochrane Database of Systematic Reviews 2011, Issue 8. [DOI: 10.1002/14651858.CD008788.pub2] [DOI] [PubMed] [Google Scholar]
- Wente MN, Veit JA, Bassi C, Dervenis C, Fingerhut A, Gouma DJ, et al. Postpancreatectomy hemorrhage (PPH): an International Study Group of Pancreatic Surgery (ISGPS) definition. Surgery 2007;142(1):20‐5. [DOI] [PubMed] [Google Scholar]
- Wente MN, Bassi C, Dervenis C, Fingerhut A, Gouma DJ, Izbicki JR, et al. Delayed gastric emptying (DGE) after pancreatic surgery: a suggested definition by the International Study Group of Pancreatic Surgery (ISGPS). Surgery 2007;142(5):761‐8. [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
- Cheng Y, Yang C, Lin Y, Lu J, Wu S, Zhou R, et al. Prophylactic abdominal drainage for pancreatic surgery. Cochrane Database of Systematic Reviews 2013, Issue 6. [DOI: 10.1002/14651858.CD010583] [DOI] [PubMed] [Google Scholar]
- Peng S, Cheng Y, Yang C, Lu J, Wu S, Zhou R, et al. Prophylactic abdominal drainage for pancreatic surgery. Cochrane Database of Systematic Reviews 2015, Issue 8. [DOI: 10.1002/14651858.CD010583.pub2] [DOI] [PubMed] [Google Scholar]